The Role of Work-Related Factors in the Development of Psychological Distress and Associated Mental Disorders: Differential Views of Human Resource Managers, Occupational Physicians, Primary Care Physicians and Psychotherapists in Germany

 ,
,
Abstract
:1. Introduction
- (1)
- What are the most important factors potentially associated with mental disorders in employees from the views of HRMs of industrial Companies, OPs, PCPs and PTs?
- (2)
- What are the differential views of HRMs of Industrial Companies, OPs, PCPs and PTs concerning the relevance of specific work-related stressors in the development of (stress-associated) mental disorders?
- (3)
- What are the differential views of HRMs of Industrial Companies, OPs, PCPs, and PTs concerning the relevance of the individual risks of employees in the development of (stress-associated) mental disorders?
2. Study Population, Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Statistical Analyses
3. Results
3.1. Rankings of Importance of Potential Stress-Dimensions by Group of Profession
3.2. Sum-Score Group Differences of Perceived Relevance of Stress-Dimensions
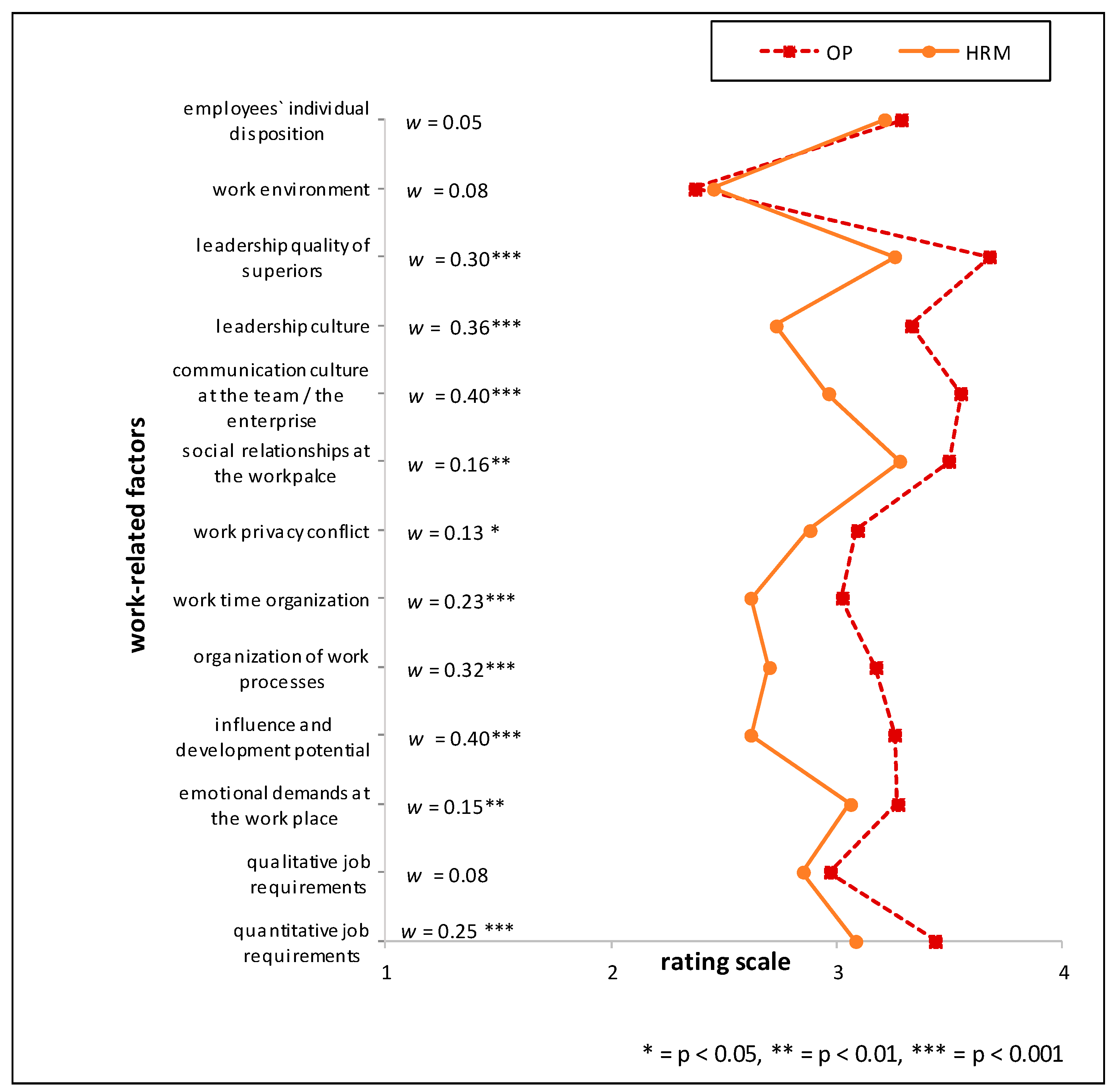
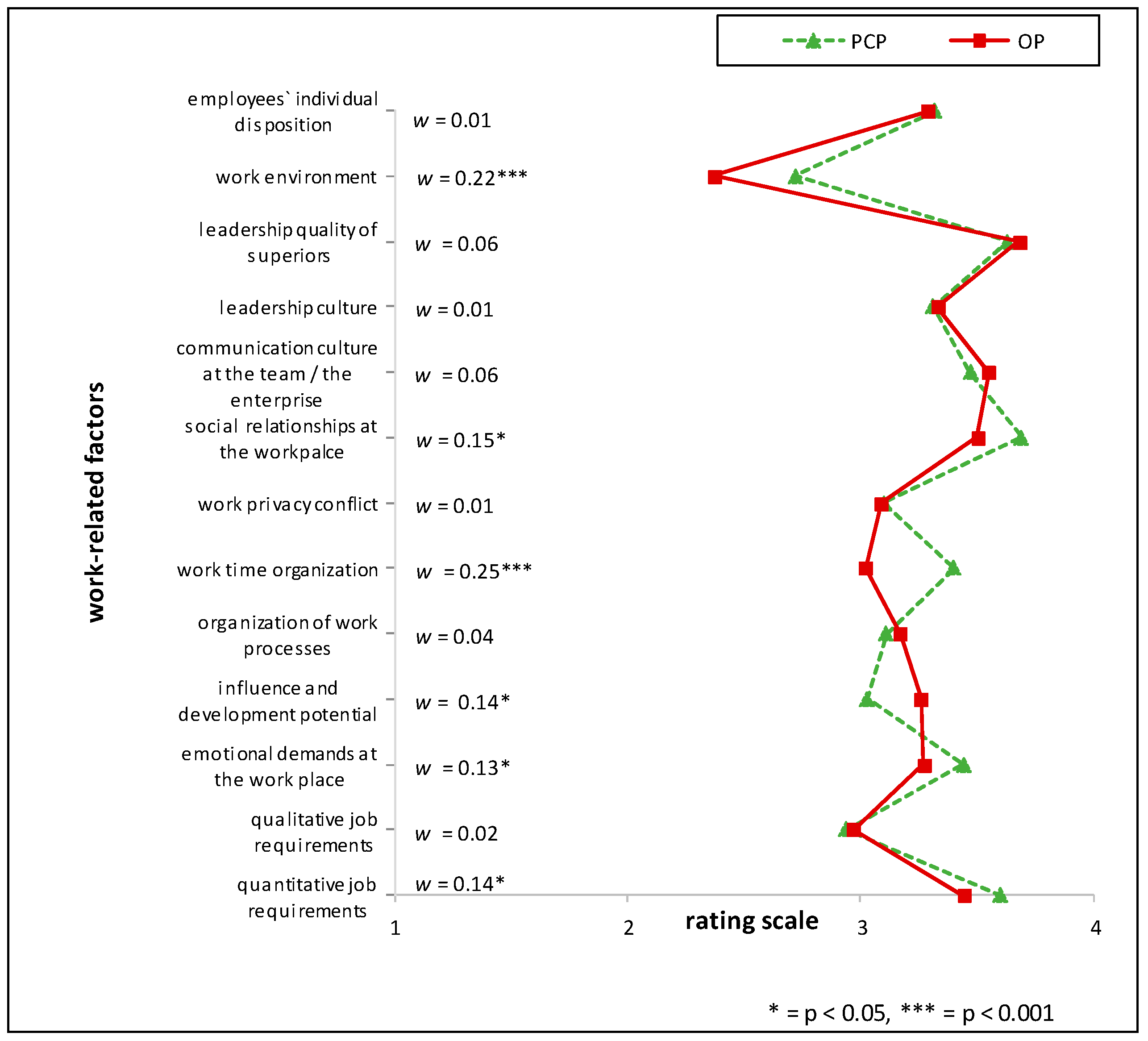
3.3. Relative Group Differences of Perceived Importance of Specific Stressors
3.4. Relative Group Differences of Importance of ‘Individual Risks’ of Employees
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Organization for Economic Co-operation and Development. Fit Mind, Fit Job: From Evidence to Practice in Mental Health and Work. Mental Health and Work; OECD Publishing: Paris, France, 2015. [Google Scholar]
- GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries: A systematic analysis for the global burden of disease study 2013. Lancert 2015, 386, 743–800. [Google Scholar]
- Organization for Economic Co-operation and Development. Sick on the Job? Myths and Realities About Mental Health and Work; OECD Publishing: Paris, France, 2012. [Google Scholar]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N. Global burden of disease attributable to mental and substance use disorders: Findings from the global burden of disease study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Kopin, I.J. Evolution of concepts of stress. Stress 2007, 10, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-J.; Mykletun, A.; Møyner, E.I.; Øverland, S.; Henderson, M.; Stansfeld, S.; Hotopf, M.; Harvey, S.B. Job strain, health and sickness absence: Results from the Hordaland Health Study. PLoS ONE 2014, 9, e96025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arends, I.; van der Klink, J.J.; Van Rhenen, W.; de Boer, M.R.; Bültmann, U. Predictors of recurrent sickness absence among workers having returned to work after sickness absence due to common mental disorders. Scand. J. Work Environ. Health 2014, 40, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Stenfors, C.; Magnusson Hanson, L.; Oxenstierna, G.; Theorell, T.; Nilsson, L.-G. Psychosocial working conditions and cognitive complaints among Swedish employees. PLoS ONE 2013, 8, e60637. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Stansfeld, S.A.; Fuhrer, R.; Ferrie, J.E.; Kivima, M. Overtime work as a predictor of major depressive episode: A 5-year follow-up of the Whitehall II study. PLoS ONE 2012, 7, e30719. [Google Scholar] [CrossRef] [PubMed]
- Malinauskienė, V.; Leišytė, P.; Malinauskas, P. Psychosocial job characteristics, social support, and sense of coherence as determinants of mental health among nurses. Medicina 2009, 45, 910–918. [Google Scholar] [PubMed]
- Lunau, T.; Siegrist, J.; Dragano, N.; Wahrendorf, M. The association between education and work stress: Does the policy context matter? PLoS ONE 2015, 10, e0121573. [Google Scholar] [CrossRef] [PubMed]
- Rugulies, R.; Madsen, I.E.H.; Nielsen, M.B.D.; Olsen, L.R.; Mortensen, E.L.; Bech, P. Occupational position and its relation to mental distress in a random sample of Danish residents. Int. Arch. Occup. Environ. Health 2010, 83, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Lopes, C.S.; Araya, R.; Werneck, G.L.; Chor, D.; Faerstein, E. Job strain and other work conditions: Relationships with psychological distress among civil servants in Rio De Janeiro, Brazil. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 43, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Marchand, A.; Demers, A.; Durand, P. Does work really cause distress? The contribution of occupational structure and work organization to the experience of psychological distress. Soc. Sci. Med. 2005, 61, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, B.; Milosevic, M.; Golubic, R.; Belosevic, L.; Russo, A.; Mustajbegovic, J. Work-related stress and workability among croatian university hospital midwives. Midwifery 2011, 27, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Shields, M. Shift work and health. Health Rep. 2002, 13, 11. [Google Scholar] [PubMed]
- Johannessen, H.A.; Tynes, T.; Sterud, T. Effects of occupational role conflict and emotional demands on subsequent psychological distress a 3-year follow-up study of the general working population in Norway. JOEM 2013, 55, 605–614. [Google Scholar] [PubMed]
- Roelen, C.A.M.; Weites, S.H.; Koopmans, P.C.; van der Klink, J.J.L.; Groothoff, J.W. Sickness absence and psychosocial work conditions: A multilevel study. Occup. Med. 2008, 58, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Bültmann, U.; Kant, I.J.; Schröer, C.A.P.; Kasl, S.V. The relationship between psychosocial work characteristics and fatigue and psychological distress. Int. Arch. Occup. Environ. Health 2006, 75, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.K.; Östergren, P.-O.; Canivet, C.; Moghadassi, M.; Lindeberg, S.; Karasek, R.; Isacsson, S.-O. Synergistic interaction effect between job control and social support at work on general psychological distress. Int. Arch. Occup. Environ. Health 2011, 84, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Lindblom, K.M.; Steven, J.L.; Fedeli, C.; Bryngelsson, I.-L. Burnout in the working population: Relations to psychosocial work factors. Int. J. Behav. Med. 2006, 13, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Moen, P.; Kaduk, A.; Kossek, E.E.; Hammer, L.; Buxton, O.M.; O’Donnell, E.; Almeida, D.; Fox, K.; Tranby, E.; Oakes, J.M.; et al. Is work-family conflict a multilevel stressor linking job conditions to mental health? Evidence from the work, family and health network. Res. Sociol. Work 2015, 26, 177–217. [Google Scholar] [CrossRef] [PubMed]
- Finne, L.B.; Christensen, J.O.; Knardahl, S. Psychological and social work factors as predictors of mental distress: A prospective study. PLoS ONE 2014, 9, e102514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuno, K.; Kawakami, K.; Inoue, A.; Ishizaki, M.; Tabata, M.; Tsuchiya, M.; Akiyama, M.; Kitazume, A.; Kuroda, M.; Shimazu, A. Intragroup and intergroup conflict at work, psychological distress, and work engagement in a sample of employees in Japan. Ind. Health 2009, 47, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Honda, A.; Date, Y.; Abe, Y.; Aoyagi, K.; Honda, S. Communication, support and psychosocial work environment affecting psychological distress among working women aged 20 to 39 years in Japan. Ind. Health 2016, 54, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.B.; Tvedt, S.D.; Matthiesen, S.B. Prevalence and occupational predictors of psychological distress in the offshore petroleum industry: A prospective study. Int. Arch. Occup. Environ. Health 2013, 86, 875–885. [Google Scholar] [CrossRef] [PubMed]
- Van der Wal, R.A.B.; Bucx, M.J.L.; Hendriks, J.C.M.; Scheffer, G.-J.; Prins, J.B. Psychological distress, burnout and personality traits in Dutch anaesthesiologists. Eur. J. Anaesthesiol. 2016, 33, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, Y.; Uchitomi, Y.; Fujimori, M.; Koyama, T.; Kataoka, H.; Kitamura, Y.; Sendo, T.; Inagaki, M. Exploring autistic-like traits relating to empathic attitude and psychological distress in hospital pharmacists. Int. J. Clin. Pharm. 2015, 37, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Dollard, M.F.; Winefield, A.H. Trait anxiety, work demand, social support and psychological distress in correctional officers. Anxiety Stress Coping 1995, 8, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Decker, F.H. Occupational and nonoccupational factors in job satisfaction and psychological distress among nurses. Res. Nurs. Health 1997, 20, 453–464. [Google Scholar] [CrossRef]
- Bronkhorst, B.; Tummers, L.; Steijn, B.; Vijverberg, D. Organizational climate and employee mental health outcomes: A systematic review of studies in health care organizations. Health Care Manag. Rev. 2015, 40, 254–271. [Google Scholar] [CrossRef] [PubMed]
- Happell, B.; Dwyer, T.; Reid-Searl, K.; Burke, K.J.; Caperchione, C.M.; Gaskin, C.J. Nurses and stress: Recognizing causes and seeking solutions. J. Nurs. Manag. 2013, 21, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.; Cooper, C.; Thomas, K. A model of work stress. Counsel. Work 2004, 2–5, 1–4. [Google Scholar]
- Preiser, C.; Rothermund, E.; Wittich, A.; Gündel, H.; Rieger, M.A. Psychosomatic consultation in the workplace: Opportunities and limitations of the services offered—Results of a qualitative study. Int. Arch. Occup. Environ. Health 2016, 89, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Moßhammer, D.; Michaelis, M.; Mehne, J.; Wilm, S.; Rieger, M.A. General practitioners’ and occupational health physicians’ views on their cooperation: A cross-sectional postal survey. Int. Arch. Occup. Environ. Health 2016, 89, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Moßhammer, D.; Natanzon, I.; Manske, I.; Grutschkowski, P.; Rieger, M. Deficiencies and barriers of the cooperation between German general practitioners and occupational health physicians? A qualitative content analysis of focus groups. Zeitschrift fur Evidenz, Fortbildung und Qualitat im Gesundheitswesen 2011, 106, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Nubling, M.; Stossel, U.; Hasselhorn, H.M.; Michaelis, M.; Hofmann, F. Measuring psychological stress and strain at work—Evaluation of the COPSOQ questionnaire in Germany. Psychosom. Med. 2006, 3, 5. [Google Scholar]
- Beck, D.; Berger, S.; Breutmann, N.; Fergen, A.; Gregersen, S.; Morschhäuser, M.; Reddehase, B.; Ruck, Y.R.; Sandrock, S.; Splittgerber, B.; et al. Empfehlungen Zur Umsetzung Der Gefährdungsbeurteilung Psychischer Belastung; Bundesministerium für Arbeit und Soziales: Berlin, Germany, 2016.
- Nubling, M.; Vomstein, M.; Schmidt, S.G.; Gregersen, S.; Dulon, M.; Nienhaus, A. Psychosocial work load and stress in the geriatric care. BMC Public Health 2010, 10, 428. [Google Scholar] [CrossRef] [PubMed]
- Pejtersen, J.H.; Kristensen, T.S.; Borg, V.; Bjorner, J.B. The second version of the Copenhagen psychosocial questionnaire. Scand. J. Public Health 2010, 38 (Suppl. 3), 8–24. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E. The job demands-resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef]
- Michaelis, M.; Lange, R.; Junne, F.; Rothermund, E.; Zipfel, S.; Gündel, H.; Rieger, M. Prevention of common mental disorders in employees—Conception, study design and sample characteristics of a multi-target survey. Ment. Health Prev. 2016, 4, 88–95. [Google Scholar] [CrossRef]
- Bühner, M.; Ziegler, M. Statistik Für Psychologen Und Sozialwissenschaftler; Paerson Studium: Munich, Germany, 2009. [Google Scholar]
- BAuA. Gefaehrdungsbeurteilung Psychischer Belastung—Erfahrungen Und Empfehlungen; Erich Schmidt Verlag: Berlin, Germany, 2014. [Google Scholar]
- Bundesministerium für Arbeit und Soziales (Ed.) Gewünschte Und Erlebte Arbeitsqualitaet. Abschlussbericht Der Repraesentativen Befragung Im Auftrag Des Bundesministeriums Fuer Arbeit Und Soziales (Bmas); Bundesministerium für Arbeit und Soziales: Berlin, Germany, 2015.
- Theorell, T.; Hammarström, A.; Aronsson, G.; Träskman Bendz, L.; Grape, T.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Hall, C. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health 2015, 15, 738. [Google Scholar] [CrossRef] [PubMed]
- Seidler, A.; Thinschmidt, M.; Deckert, S.; Then, F.; Hegewald, J.; Nieuwenhuijsen, K.; Riedel-Heller, S.G. The role of psychosocial working conditions on burnout and its core component emotional exhaustion—A systematic review. J. Occup. Med. Toxicol. 2014, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Bass, B.M. Two decades of research and development in transformational leadership. Eur. J. Work Organ. Psychol. 1999, 8, 9–32. [Google Scholar] [CrossRef]
- Felfe, J. Transformationale Und Charismatische Führung—Stand Der Forschung Und Aktuelle Entwicklungen. Z. Personalpsychol. 2006, 5, 163–176. [Google Scholar] [CrossRef]
- Franke, F.; Felfe, J. How does transformational leadership impact employees’ psychological strain? Examining differentiated effects and the moderating role of affective organizational commitment. Leadership 2011, 7, 295–316. [Google Scholar] [CrossRef]
- Burgess, L.; Irvine, F.; Wallymahmed, A. Personality, stress and coping in intensive care nurses: A descriptive exploratory study. Nurs. Crit. Care 2010, 15, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Applebaum, D.; Fowler, S.; Fiedler, N.; Osinubi, O.; Robson, M. The impact of environmental factors on nursing stress, job satisfaction, and turnover intention. J. Nurs. Adm. 2010, 40, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Shackelton, R.; Siegrist, J.; Link, C.; Marceau, L.; von dem Knesebeck, O.; McKinlay, J. Work stress of primary care physicians in the US, UK and German health care systems. Soc. Sci. Med. 2010, 71, 298–304. [Google Scholar] [CrossRef]
- Mache, S. Coping with job stress by Hospital doctors: A comparative study. Wien Medizinsche Wochenschrift 2012, 162, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Salavecz, G.; Chandola, T.; Pikhart, H.; Dragano, N.; Siegrist, J.; Jöckel, K.H.; Erbel, R.; Pajak, A.; Malyutina, S.; Kubinova, R.; et al. Work stress and health in Western European and post-communist countries: An East–West comparison study. J. Epidemiol. Community Health 2010, 64, 57–62. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | HRM | OP | PCP | PT | ||||
|---|---|---|---|---|---|---|---|---|
| % | Total | % | Total | % | Total | % | Total | |
| Sex | ||||||||
| Male | 58.2 | 96/165 | 52.6 | 70/133 | 59.6 | 81/136 | 30.1 | 56/186 |
| Qualification of the PCP group | ||||||||
| Specialist title | - | - | 54.9 | 73/133 | 76.1 | 102/134 | 35.5 | 66/186 |
| Status of the investigated OP | ||||||||
| Employed in the enterprise | - | - | 46.0 | 54/128 | - | - | - | - |
| Employed in an external occupational health service | - | - | 24.2 | 31/128 | - | - | - | - |
| Own practice | - | - | 28.9 | 37/128 | - | - | - | - |
| Freelance without own practice | - | - | 4.7 | 6/128 | - | - | - | - |
| Size of enterprise | ||||||||
| Large (≥250 employees) | 53.6 | 89/166 | 93.9 | 108/115 | - | - | - | - |
| Medium-sized (50≥ and <250) | 38.0 | 63/166 | 4.3 | 5/115 | - | - | - | - |
| Small (<50) | 8.4 | 14/166 | 1.7 | 2/115 | - | - | - | - |
| Location of the OP/PCP practice | ||||||||
| City | - | - | 57.0 | 73/128 | 30.9 | 42/136 | - | - |
| City periphery | - | - | 27.3 | 35/128 | 37.5 | 51/136 | - | - |
| Countryside | - | - | 15.6 | 20/128 | 31.6 | 43/136 | - | - |
| Status of HRM in the enterprise | ||||||||
| Executive director /owner | 17.5 | 28/160 | - | - | - | - | - | - |
| Human resource managers | 75.0 | 120/160 | - | - | - | - | - | - |
| Other | 7.5 | 12/160 | - | - | - | - | - | - |
| Variable | n | M | SD | Min–Max Score |
|---|---|---|---|---|
| Occupational physician (OP) | 133 | 54.9 | 8.0 | 36–77 |
| Primary care physicians a (PCP) | 130 | 53.7 | 8.6 | 37–75 |
| Psychotherapist (PT) | 183 | 53.9 | 8.6 | 31–71 |
| Human resource managers (HRM) | 159 | 48.8 | 8.1 | 25–66 |
| Dimensions | Individual Factor Items | Examples Given in the Questionnaire | Source |
|---|---|---|---|
| Work contents (4 items) | |||
| 1a | Quantitative job demands | Quantitative amount of the employee’s tasks | [37] |
| 1b | Qualitative job demands | Content of the employee’s work and the level of expertise/competencies/education/intellectual capacity required | [37] |
| 1c | Emotional demands in the workplace | Exposure to emotionally stressful events/work phases or emotional dimension of accountability/responsibility (e.g., during management of entrepreneurial crises) | [37] |
| 1d | Influence and development potential on the job | How work processes can be influenced/shaped by the executing employee and how the employee has the opportunity for personal growth/development within his work setting/processes. | [37] |
| Organization of work processes (3 items) | |||
| 2a | Organization of work processes | Description of work processes and definitions e.g., in terms of who is involved. transparency of duties within the team along the work processes etc. | [44] |
| 2b | Working time organization | Shift work, duration of daily working time | [39] |
| 2c | Work-privacy conflict | Structural dimension of compatibility of family and working life e.g., in terms of child care offerings, forecast reliability of absence from work etc. | [37] |
| Interpersonal relations and leadership (4 items) | |||
| 3a | Social relationships in the workplace | Working atmosphere in a team/ in the enterprise | [37] |
| 3b | Communication culture in the team/in the enterprise | Formal and informal ways and styles of communication among team members and within the enterprise at whole (transparency, timeliness, implicit/explicit ways of communication) etc. | a |
| 3c | Leadership culture | Hierarchies (flat/steep), accountabilities, accessibility etc. | [40] |
| 3d | Leadership quality of superiors | Leadership quality including interpersonal competencies of superiors | [37] |
| Physical work environment | |||
| 4a | Physical work environment | Structural dimension including e.g., noise exposure, lighting conditions, cleanliness, workplace ergonomics | [45] |
| (Individual level) | |||
| Individual disposition | |||
| 5a | Individual disposition of employee | The individual disposition of an employee in terms of e.g., stress-resilience, individual resources, prehistory of common mental disorders etc. | a |
| Stress-Dimensions | HRM | OP | PCP | PT | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |
| 1. Work content | 2.91 | 0.49 | 3.23 | 0.45 | 3.25 | 0.46 | 3.28 | 0.39 |
| 2. Work organization | 2.73 | 0.58 | 3.09 | 0.53 | 3.21 | 0.50 | 3.25 | 0.49 |
| 3. Interpersonal relations and leadership at work | 3.06 | 0.61 | 3.51 | 0.49 | 3.53 | 0.45 | 3.57 | 0.43 |
| Factors with Highest Rankings | Factors with Lowest Rankings | |||||||
|---|---|---|---|---|---|---|---|---|
| Position | Item | M | SD | Position | Item | M | SD | n |
| Human Resource Managers | ||||||||
| 1 | Social relationships in the workplace | 3.28 | 0.73 | 12 | Physical work environment | 2.45 | 0.68 | 170 |
| 2 | Leadership quality of superiors | 3.26 | 0.75 | 11 | Working time organization | 2.62 | 0.84 | 168 |
| 3 | Quantitative job demands | 3.08 | 0.72 | 10 | Influence and development potential on the job | 2.62 | 0.78 | 169 |
| Occupational Physicians | ||||||||
| 1 | Leadership quality of superiors | 3.68 | 0.55 | 12 | Qualitative job demands | 2.97 | 0.76 | 127 |
| 2 | Communication culture in the team/in the enterprise | 3.55 | 0.60 | 11 | Physical work environment | 2.37 | 0.73 | 133 |
| 3 | Social relationships in the workplace | 3.50 | 0.64 | 10 | Working time organization | 3.02 | 0.78 | 132 |
| Primary Care Physicians | ||||||||
| 1 | Social relationships in the workplace | 3.69 | 0.49 | 12 | Physical work environment | 2.72 | 0.82 | 136 |
| 2 | Leadership quality of superiors | 3.63 | 0.54 | 11 | Qualitative job demands | 2.94 | 0.80 | 135 |
| 3 | Quantitative job demands | 3.60 | 0.55 | 10 | Work-privacy conflict | 3.10 | 0.75 | 136 |
| Psychotherapists | ||||||||
| 1 | Social relationships in the workplace | 3.74 | 0.48 | 12 | Qualitative job demands | 2.77 | 0.73 | 184 |
| 2 | Leadership quality of superiors | 3.65 | 0.56 | 11 | Physical work environment | 2.77 | 0.75 | 181 |
| 3 | Communication culture in the team/in the enterprise | 3.58 | 0.54 | 10 | Organization of work processes | 3.13 | 0.66 | 184 |
| Factors with the Largest Group Differences between HRM and Medical Groups | ||
|---|---|---|
| Ranking Position | Items | w |
| HRM vs. OP | ||
| 1 | communication culture at the team/the enterprise | 0.40 |
| 2 | influence and development potential | 0.40 |
| 3 | leadership culture | 0.36 |
| HRM vs. PCP | ||
| 1 | work time organization | 0.46 |
| 2 | quantitative job requirements | 0.37 |
| 3 | communication culture of the team/the enterprise | 0.35 |
| HRM vs. PT | ||
| 1 | work time organization | 0.45 |
| 2 | influence and development potential | 0.43 |
| 3 | communication culture of the team/ the enterprise | 0.43 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Junne, F.; Michaelis, M.; Rothermund, E.; Stuber, F.; Gündel, H.; Zipfel, S.; Rieger, M.A. The Role of Work-Related Factors in the Development of Psychological Distress and Associated Mental Disorders: Differential Views of Human Resource Managers, Occupational Physicians, Primary Care Physicians and Psychotherapists in Germany. Int. J. Environ. Res. Public Health 2018, 15, 559. https://doi.org/10.3390/ijerph15030559
Junne F, Michaelis M, Rothermund E, Stuber F, Gündel H, Zipfel S, Rieger MA. The Role of Work-Related Factors in the Development of Psychological Distress and Associated Mental Disorders: Differential Views of Human Resource Managers, Occupational Physicians, Primary Care Physicians and Psychotherapists in Germany. International Journal of Environmental Research and Public Health. 2018; 15(3):559. https://doi.org/10.3390/ijerph15030559
Chicago/Turabian StyleJunne, Florian, Martina Michaelis, Eva Rothermund, Felicitas Stuber, Harald Gündel, Stephan Zipfel, and Monika A. Rieger. 2018. "The Role of Work-Related Factors in the Development of Psychological Distress and Associated Mental Disorders: Differential Views of Human Resource Managers, Occupational Physicians, Primary Care Physicians and Psychotherapists in Germany" International Journal of Environmental Research and Public Health 15, no. 3: 559. https://doi.org/10.3390/ijerph15030559