Lack of Substantial Post-Cessation Weight Increase in Electronic Cigarettes Users

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Samples
2.2. Study Design and Study Assessments
2.3. Data Management
2.4. Study Outcomes
2.5. E-Cigarettes Users Phenotypes
2.6. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. Changes in Smoking Behaviour and Patterns of e-Cigarette Use
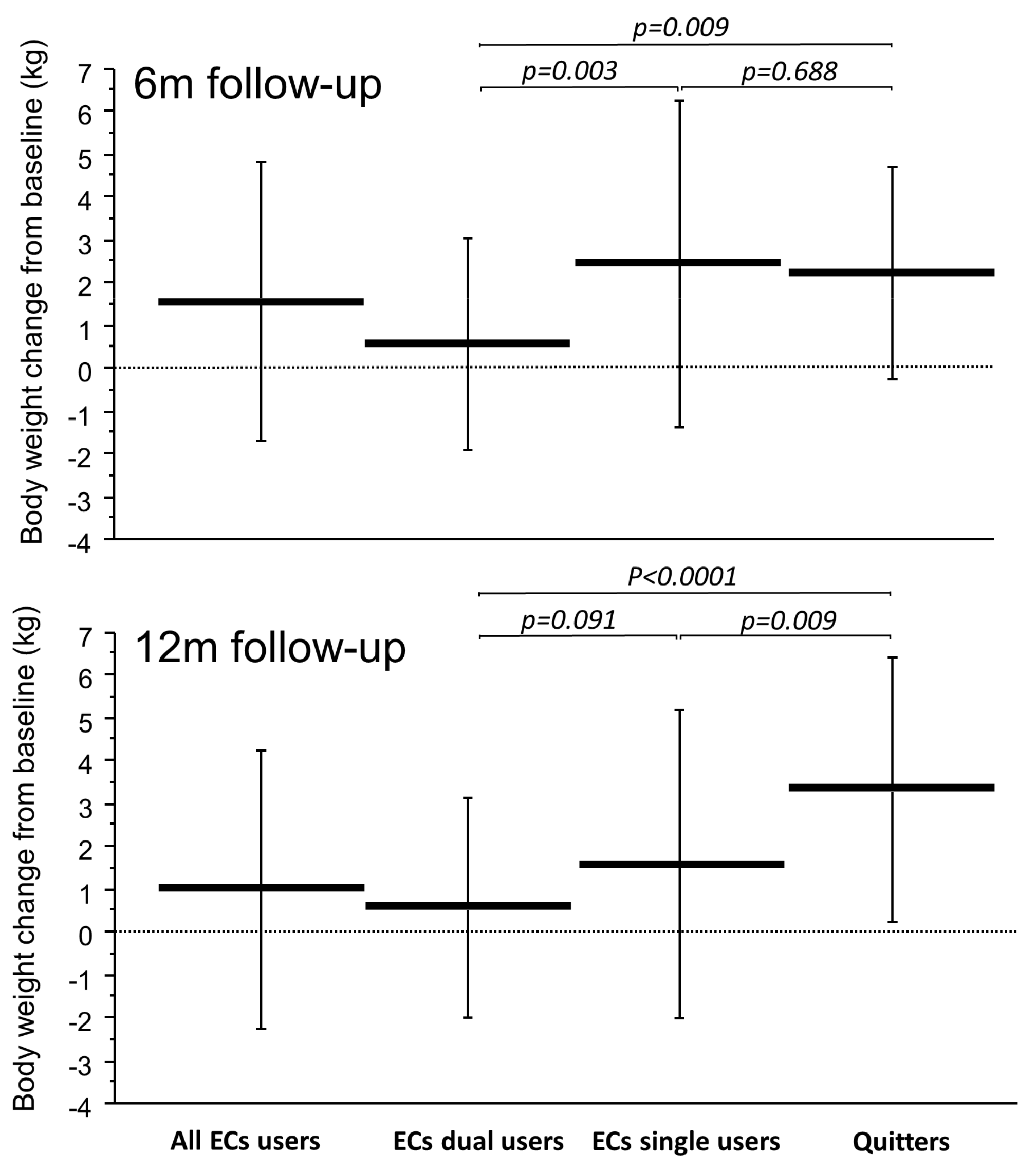
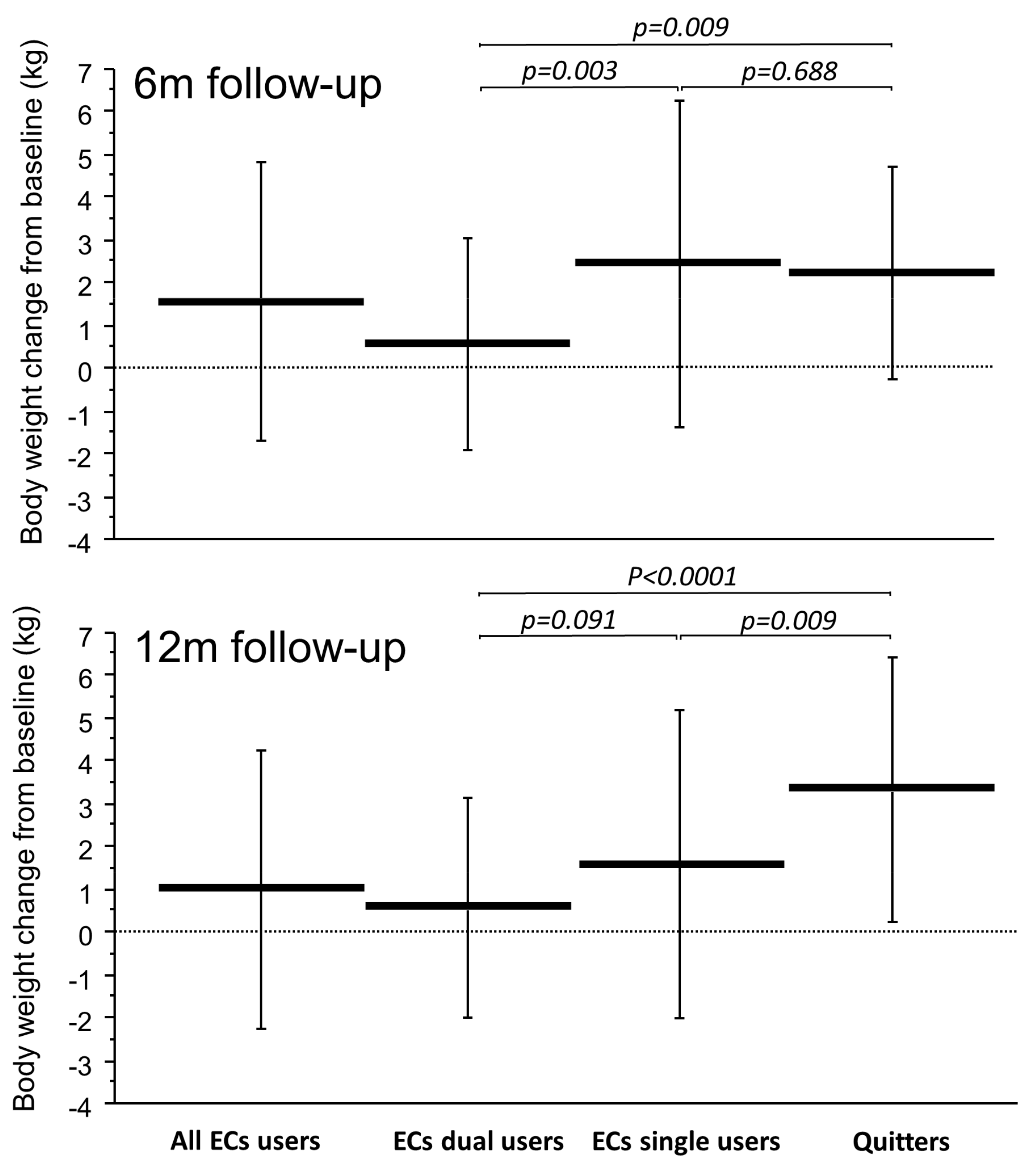
3.3. Changes in Body Weight
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; US Department of Health and Human Services: Atlanta, Georgia, 2014.
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2008—The MPOWER Package; World Health Organization: Geneva, Switzerland, 2008.
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004, 328, 1519. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. The Health Benefits of Smoking Cessation: A Report of the Surgeon General; U.S. Department of Health and Human Services: Rockville, MD, USA, 1990.
- Polosa, R.; Benowitz, N.L. Treatment of nicotine addiction: Present therapeutic options and pipeline developments. Trends. Pharmacol. Sci. 2011, 32, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Koilpillai, P.; Fanshawe, T.R.; Lancaster, T. Combined pharmacotherapy and behavioural interventions for smoking cessation. In Cochrane Database of Systematic Reviews; Stead, L.F., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2016; Volume 3, p. CD008286. [Google Scholar]
- Klesges, R.C.; Meyers, A.W.; Klesges, L.M.; La Vasque, M.E. Smoking, body weight, and their effects on smoking behavior: A comprehensive review of the literature. Psychol. Bull. 1989, 106, 204. [Google Scholar] [CrossRef] [PubMed]
- Lycett, D.; Munafò, M.; Johnstone, E.; Murphy, M.; Aveyard, P. Associations between weight change over 8 years and baseline body mass index in a cohort of continuing and quitting smokers. Addiction 2011, 106, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.; Quinn, B.C. Estimating the effect of smoking cessation on weight gain: An instrumental variable approach. Health Serv. Res. 2006, 41, 2255–2266. [Google Scholar] [CrossRef] [PubMed]
- Zoli, M.; Picciotto, M.R. Nicotinic Regulation of Energy Homeostasis. Nicot. Tob. Res. 2012, 14, 1270–1290. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, R.J.N.; Pomerleau, C.S. “Prequit attrition” among weight-concerned women smokers. Eat. Behav. 2000, 1, 145–151. [Google Scholar] [CrossRef]
- Rosenthal, L.; Carroll-Scott, A.; Earnshaw, V.A.; Sackey, N.; O’Malley, S.S.; Santilli, A.; Ickovics, J.R. Targeting cessation: Understanding barriers and motivations to quitting among urban adult daily tobacco smokers. Addict. Behav. 2013, 38, 1639–1642. [Google Scholar] [CrossRef] [PubMed]
- Courtemanche, C.; Tchernis, R.; Ukert, B. The Effect of Smoking on Obesity: Evidence from a Randomized Trial. J. Health Econ. 2018, 57, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Davey Smith, G.; Bracha, Y.; Svendsen, K.H.; Neaton, J.D.; Haffner, S.M.; Kuller, L.H. Multiple Risk Factor Intervention Trial Research Group Incidence of type 2 diabetes in the randomized multiple risk factor intervention trial. Ann. Intern. Med. 2005, 142, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Yeh, H.C.; Duncan, B.B.; Schmidt, M.I.; Wang, N.Y.; Brancati, F.L. Smoking, Smoking Cessation, and Risk for Type 2 Diabetes Mellitus. Ann. Intern. Med. 2010, 152, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Farley, A.C.; Hajek, P.; Lycett, D.; Aveyard, P. Interventions for preventing weight gain after smoking cessation. In Cochrane Database of Systematic Reviews; Aveyard, P., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2016; Volume 1, p. CD006219. [Google Scholar]
- Caponnetto, P.; Russo, C.; Bruno, C.M.; Alamo, A.; Amaradio, M.D.; Polosa, R. Electronic cigarette: A possible substitute for cigarette dependence. Monaldi Arch. Chest Dis. 2015, 79, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Characteristics, perceived side effects and benefits of electronic cigarette use: A worldwide survey of more than 19,000 consumers. Int. J. Environ. Res. Public Health 2014, 11, 4356–4373. [Google Scholar] [CrossRef] [PubMed]
- Gallus, S.; Lugo, A.; Pacifici, R.; Pichini, S.; Colombo, P.; Garattini, S.; La Vecchia, C. E-Cigarette Awareness, Use, and Harm Perceptions in Italy: A National Representative Survey. Nicot. Tob. Res. 2014, 16, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Pechacek, T.F.; Nayak, P.; Gregory, K.R.; Weaver, S.R.; Eriksen, M.P. The Potential That Electronic Nicotine Delivery Systems Can be a Disruptive Technology: Results from a National Survey. Nicot. Tob. Res. 2016, 18, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Dawkins, L.; Kimber, C.; Puwanesarasa, Y.; Soar, K. First-versus second-generation electronic cigarettes: Predictors of choice and effects on urge to smoke and withdrawal symptoms. Addiction 2015, 110, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. Gateway effects and electronic cigarettes. Addiction 2017. [Google Scholar] [CrossRef] [PubMed]
- Kistler, C.; Crutchfield, T.; Sutfin, E.; Ranney, L.; Berman, M.; Zarkin, G.; Goldstein, A. Consumers’ Preferences for Electronic Nicotine Delivery System Product Features: A Structured Content Analysis. Int. J. Environ. Res. Public Health 2017, 14, 613. [Google Scholar] [CrossRef] [PubMed]
- Soule, E.K.; Maloney, S.F.; Guy, M.C.; Eissenberg, T.; Fagan, P. User identified positive outcome expectancies of electronic cigarette use: A concept mapping study. Psychol. Addict. Behav. 2017, 31, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Polosa, R. Safety evaluation and risk assessment of electronic cigarettes as tobacco cigarette substitutes: A systematic review. Ther. Adv. Drug Saf. 2014, 5, 67–86. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Campagna, D.; Cibella, F.; Morjaria, J.B.; Caruso, M.; Russo, C.; Polosa, R. EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as tobacco cigarettes substitute: A prospective 12-month randomized control design study. PLoS ONE 2013, 8, e66317. [Google Scholar] [CrossRef] [PubMed]
- Polosa, R.; Caponnetto, P.; Maglia, M.; Morjaria, J.B.; Russo, C. Success rates with nicotine personal vaporizers: A prospective 6-month pilot study of smokers not intending to quit. BMC Public Health 2014, 14, 1159. [Google Scholar] [CrossRef] [PubMed]
- Adriaens, K.; Van Gucht, D.; Declerk, P.; Baeyens, F. Effectiveness of the Electronic Cigarette: An Eight-Week Flemish Study with Six-Month Follow-up on Smoking Reduction, Craving and Experienced Benefits and Complaints. Int. J. Environ. Res. Public Health 2014, 11, 11220–11248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, S.H.; Zhuang, Y.L.; Wong, S.; Cummins, S.E.; Tedeschi, G.J. E-cigarette use and associated changes in population smoking cessation: Evidence from US current population surveys. BMJ 2017, 358, j3262. [Google Scholar] [CrossRef] [PubMed]
- Doran, N.; Brikmanis, K.; Petersen, A.; Delucchi, K.; Al-Delaimy, W.K.; Luczak, S.; Myers, M.; Strong, D. Does e-cigarette use predict cigarette escalation? A longitudinal study of young adult non-daily smokers. Prev. Med. 2017, 100, 279–284. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Clark, M.M.; Hurt, R.D.; Croghan, I.T.; Patten, C.A.; Novotny, P.; Sloan, J.A.; Dakhil, S.R.; Croghan, G.A.; Wos, E.J.; Rowland, K.M.; et al. The prevalence of weight concerns in a smoking abstinence clinical trial. Addict. Behav. 2006, 31, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Tuovinen, E.-L.; Saarni, S.E.; Kinnunen, T.H.; Haukkala, A.; Jousilahti, P.; Patja, K.; Kaprio, J.; Korhonen, T. Associations of Weight Concerns With Self-Efficacy and Motivation to Quit Smoking: A Population-Based Study Among Finnish Daily Smokers. Nicot. Tob. Res. 2015, 17, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Shimokata, H.; Muller, D.C.; Andres, R. Studies in the Distribution of Body Fat. JAMA 1989, 261, 1169. [Google Scholar] [CrossRef] [PubMed]
- Klesges, R.C.; Ward, K.D.; Ray, J.W.; Cutter, G.; Jacobs, D.R.; Wagenknecht, L.E. The prospective relationships between smoking and weight in a young, biracial cohort: The Coronary Artery Risk Development in Young Adults Study. J. Consult. Clin. Psychol. 1998, 66, 987–993. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, P.; Connett, J.E.; Lee, W.W.; Nides, M.; Murray, R.; Wise, R. Early and late weight gain following smoking cessation in the Lung Health Study. Am. J. Epidemiol. 1998, 148, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Pistelli, F.; Aquilini, F.; Carrozzi, L. Weight Gain after Smoking Cessation. Monaldi Arch. Chest Dis. 2016, 71, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Aubin, H.-J.; Farley, A.; Lycett, D.; Lahmek, P.; Aveyard, P. Weight gain in smokers after quitting cigarettes: Meta-analysis. BMJ 2012, 345, e4439. [Google Scholar] [CrossRef] [PubMed]
- Russo, C.; Cibella, F.; Caponnetto, P.; Campagna, D.; Maglia, M.; Frazzetto, E.; Mondati, E.; Caruso, M.; Polosa, R. Evaluation of Post Cessation Weight Gain in a 1-Year Randomized Smoking Cessation Trial of Electronic Cigarettes. Sci. Rep. 2016, 6, 18763. [Google Scholar] [CrossRef] [PubMed]
- Cravo, A.S.; Bush, J.; Sharma, G.; Savioz, R.; Martin, C.; Craige, S.; Walele, T. A randomised, parallel group study to evaluate the safety profile of an electronic vapour product over 12 weeks. Regul. Toxicol. Pharmacol. 2016, 81, S1–S14. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.F.; Madans, J.; Anda, R.F.; Kleinman, J.C.; Giovino, G.A.; Byers, T. Smoking Cessation and Severity of Weight Gain in a National Cohort. N. Engl. J. Med. 1991, 324, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Troiano, R.P.; Pamuk, E.R.; Kuczmarski, R.J.; Campbell, S.M. The Influence of Smoking Cessation on the Prevalence of Overweight in the United States. N. Engl. J. Med. 1995, 333, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Yanovski, J.A.; Yanovski, S.Z.; Sovik, K.N.; Nguyen, T.T.; O’Neil, P.M.; Sebring, N.G. A prospective study of holiday weight gain. N. Engl. J. Med. 2000, 342, 861–867. [Google Scholar] [CrossRef] [PubMed]
- Hull, H.R.; Radley, D.; Dinger, M.K.; Fields, D.A. The effect of the Thanksgiving holiday on weight gain. Nutr. J. 2006, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Cibella, F.; Mancuso, S.; Campagna, D.; Arcidiacono, G.; Polosa, R. Effect of a nicotine-free inhalator as part of a 605 smoking-cessation programme. Eur. Respir. J. 2011, 38, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Wills, T.A.; Sargent, J.D.; Gibbons, F.X.; Pagano, I.; Schweitzer, R. E-cigarette use is differentially related to smoking onset among lower risk adolescents. Tob. Control 2016, 26. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Spyrou, A.; Tsimopoulou, K.; Stefopoulos, C.; Romagna, G.; Voudris, V. Nicotine absorption from electronic cigarette use: Comparison between first and new-generation devices. Sci. Rep. 2014, 4, 4133. [Google Scholar] [CrossRef] [PubMed]
- Fearon, I.M.; Eldridge, A.; Gale, N.; Shepperd, C.J.; McEwan, M.; Camacho, O.M.; Nides, M.; McAdam, K.; Proctor, C.J. E-cigarette Nicotine Delivery: Data and Learnings from Pharmacokinetic Studies. Am. J. Health Behav. 2017, 41, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Pomerleau, C.S.; Ehrlich, E.; Tate, J.C.; Marks, J.L.; Flessland, K.A.; Pomerleau, O.F. The female weight-control smoker: A profile. J. Subst. Abuse 1993, 5, 391–400. [Google Scholar] [CrossRef]
- Wong, S.L.; Shields, M.; Leatherdale, S.; Malaison, E.; Hammond, D. Assessment of validity of self-reported smoking status. Health Rep. 2012, 23, 47–53. [Google Scholar] [PubMed]
- Nides, M.; Rand, C.; Dolce, J.; Murray, R.; O’hara, P.; Voelker, H.; Connett, J. Weight gain as a function of smoking cessation and 2-mg nicotine gum use among middle-aged smokers with mild lung impairment in the first 2 years of the Lung Health Study. Health Psychol. 1994, 13, 354–361. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; The National Academies Press: Washington, DC, USA, 2018. [Google Scholar]
- Evidence Review of E-Cigarettes and Heated Tobacco Products 2018: Executive Summary. Available online: https://www.gov.uk/government/publications/e-cigarettes-and-heated-tobacco-products-evidence-review/evidence-review-of-e-cigarettes-and-heated-tobacco-products-2018-executive-summary (accessed on 2 March 2018).
- Chinn, S.; Jarvis, D.; Melotti, R.; Luczynska, C.; Ackermann-Liebrich, U.; Antó, J.M.; Cerveri, I.; de Marco, R.; Gislason, T.; Heinrich, J.; et al. Smoking cessation, lung function, and weight gain: A follow-up study. Lancet 1998, 365, 1629–1635. [Google Scholar] [CrossRef]
- Stewart, S.T.; Cutler, D.M.; Rosen, A.B. Forecasting the Effects of Obesity and Smoking on U.S. Life Expectancy. N. Engl. J. Med. 2009, 361, 2252–2260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, C.; Goh, E.; Park, S.M.; Cho, B. Effects of smoking cessation and weight gain on cardiovascular disease risk factors in Asian male population. Atherosclerosis 2010, 208, 275–279. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | EC Users Study Group N = 86 | Cigarette Smokers Study Group N = 93 | Quitters Study Group N = 44 |
|---|---|---|---|
| Sex (No., M/F) | 58/28 | 59/34 | 29/15 |
| Age (Years, mean ± SD) | 54.2 ± 12.6 | 54.3 ± 11.7 | 53.3 ± 12.7 |
| Body weight (kg, mean ± SD) | 72.7 ± 11.9 | 72.5 ± 12.0 | 74.5 ± 8.9 |
| BMI (kg/m2, mean ± SD) | 26.0 ± 3.0 | 26.3 ± 3.3 | 26.7 ± 2.6 |
| Cig/day (cig/day, mean ± SD) | 21.1 ± 5.0 | 20.5 ± 4.7 | 20.2 ± 3.9 |
| BW T0 (kg, Mean ± SD) | BW 6m (kg, Mean ± SD) | BW 6m * (%T0, Mean ± SD) | BW 6m ** (diff T0, kg, Mean ± SD) | BW 12m (kg, Mean ± SD) | BW 12m * (%T0, Mean ± SD) | BW 12m ** (diff T0, kg, Mean ± SD) | |
|---|---|---|---|---|---|---|---|
| Cigarette smokers study group N = 93 | 72.5 ± 12.0 | 72.7 ± 11.8 | 0.5 ± 2.6 | 0.3 ± 1.8 | 72.9 ± 11.9 | 0.7 ± 2.9 | 0.5 ± 2.1 |
| EC users study group N = 86 | 72.7 ± 11.9 | 74.2 ± 12.6 | 2.2 ± 4.4 (p = 0.387) † | 1.6 ± 3.3 | 73.8 ± 12.4 | 1.5 ± 4.1 (p = 0.627) † | 1.1 ± 3.2 |
| Exclusive EC users § Dual users | 72.1 ± 11.7 73.2 ± 12.2 | 74.7 ± 12.8 73.8 ± 12.4 | 3.5 ± 4.9 0.9 ± 3.4 | 2.5 ± 3.7 0.6 ± 2.5 | 72.6 ± 13.2 75.0 ± 11.5 | 2.2 ± 4.6 0.7 ± 3.5 | 1.6 ± 3.6 0.8 ± 2.9 |
| Quitters study group N = 44 | 74.5 ± 8.9 | 76.8 ± 8.6 | 3.2 ± 3.6 (p = 0.048) † | 2.3 ± 2.5 | 77.9 ± 8.4 | 4.8 ± 4.5 (p = 0.019) † | 3.4 ± 3.0 |
| Variables | Weight Change at 6 Months | Weight Change at 12 Months | ||||
|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |
| Quitters study group * | 2.794 | 1.549/4.039 | <0.0001 | 4.127 | 2.780/5.474 | <0.0001 |
| EC users study group-exclusive EC users * | 2.908 | 1.639/4.176 | <0.0001 | 1.274 | −0.034/2.714 | 0.054 |
| EC users study group-dual users * | 0.419 | −0.830/1.669 | 0.509 | 0.076 | −1.309/1.460 | 0.914 |
| Sex ** | 0.630 | −0.339/1.599 | 0.201 | 0.983 | −0.066/2.031 | 0.066 |
| Age (years) | −0.024 | −0.062/0.014 | 0.212 | −0.019 | −0.060/0.0122 | 0.357 |
| BMI at T0 (kg/m2) | −0.088 | −0.239/0.063 | 0.252 | −0.126 | −0.289/0.038 | 0.131 |
| Cig/day at T0 (No.) | 0.054 | −0.045/0.152 | 0.287 | 0.043 | −0.064/0.149 | 0.434 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, C.; Cibella, F.; Mondati, E.; Caponnetto, P.; Frazzetto, E.; Caruso, M.; Caci, G.; Polosa, R. Lack of Substantial Post-Cessation Weight Increase in Electronic Cigarettes Users. Int. J. Environ. Res. Public Health 2018, 15, 581. https://doi.org/10.3390/ijerph15040581
Russo C, Cibella F, Mondati E, Caponnetto P, Frazzetto E, Caruso M, Caci G, Polosa R. Lack of Substantial Post-Cessation Weight Increase in Electronic Cigarettes Users. International Journal of Environmental Research and Public Health. 2018; 15(4):581. https://doi.org/10.3390/ijerph15040581
Chicago/Turabian StyleRusso, Cristina, Fabio Cibella, Enrico Mondati, Pasquale Caponnetto, Evelise Frazzetto, Massimo Caruso, Grazia Caci, and Riccardo Polosa. 2018. "Lack of Substantial Post-Cessation Weight Increase in Electronic Cigarettes Users" International Journal of Environmental Research and Public Health 15, no. 4: 581. https://doi.org/10.3390/ijerph15040581