Characterization of Fine Particulate Matter and Associated Health Burden in Nanjing

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection: Meteorological Conditions, PM2.5 and Other Air Pollutants
2.2. Estimation of Premature Mortality Attributable to PM2.5
2.3. Calculation of YLL
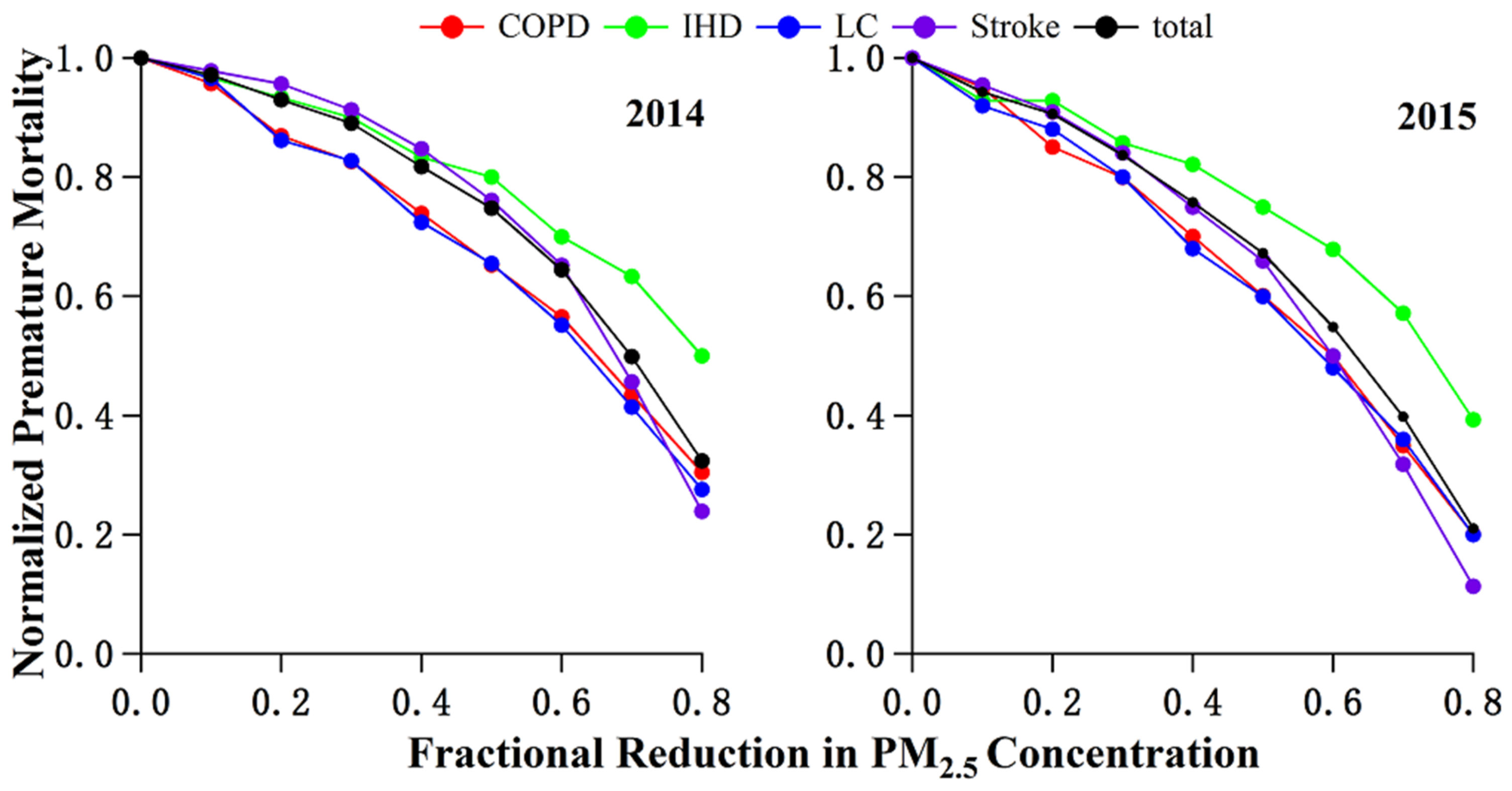
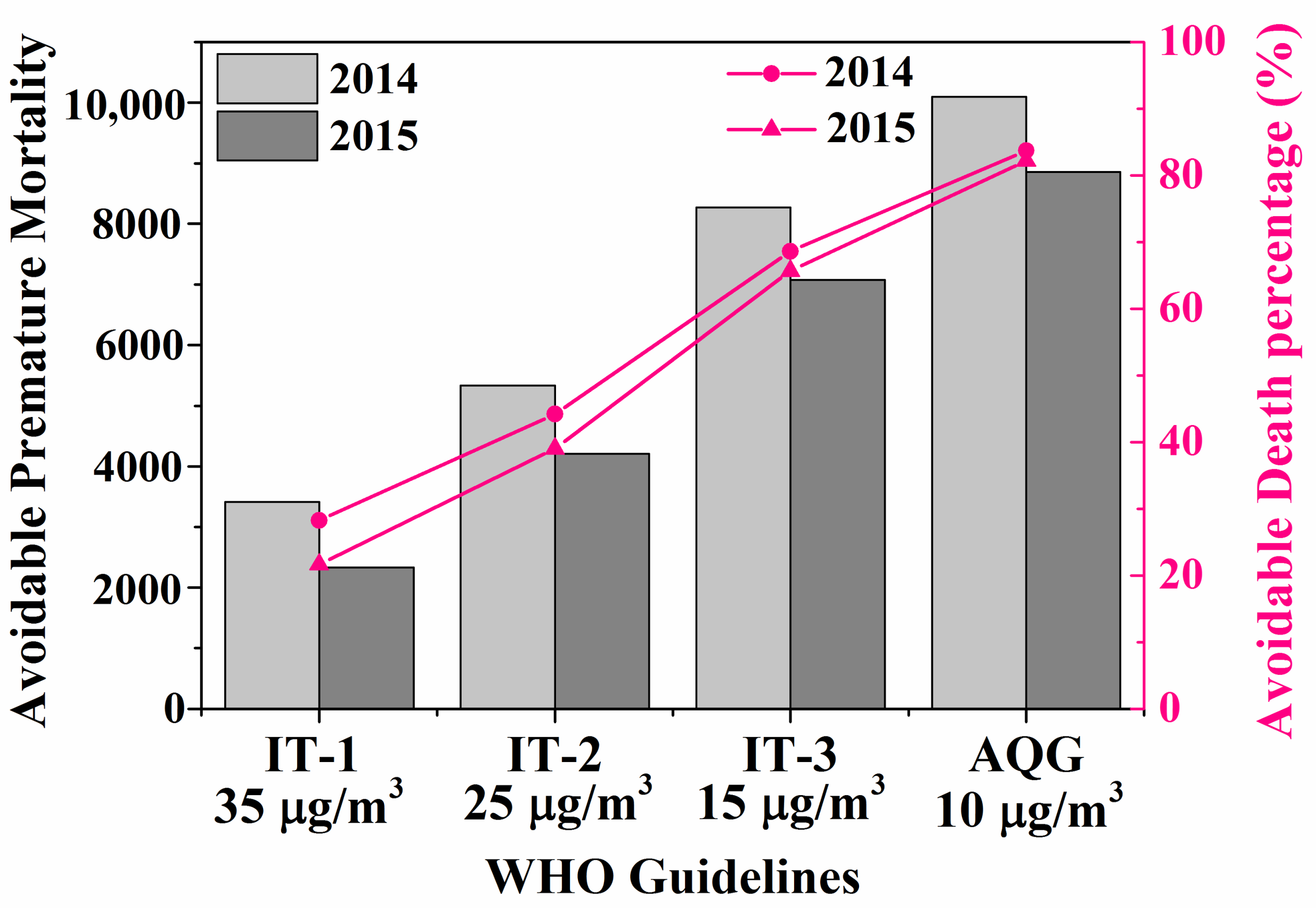
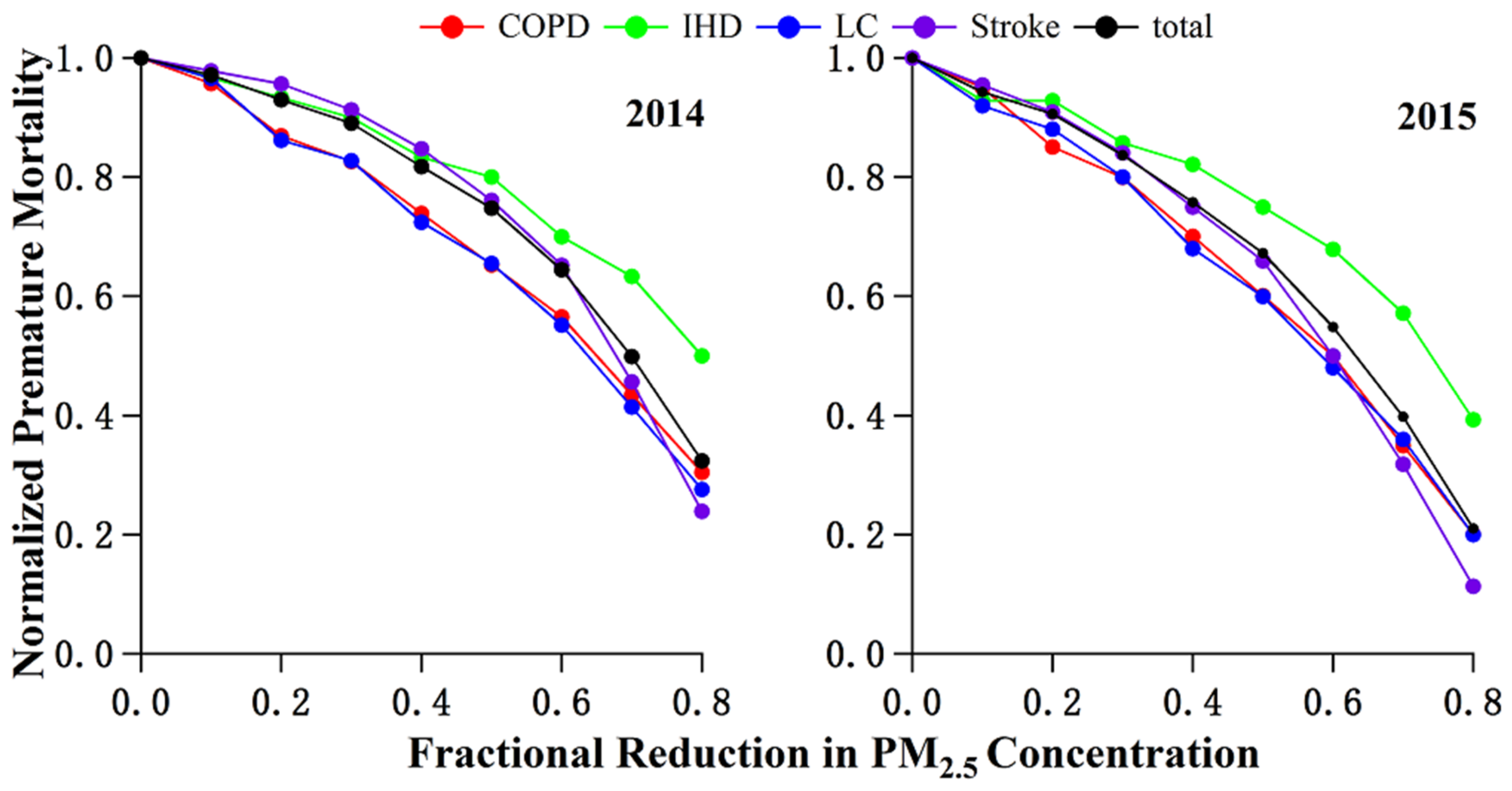
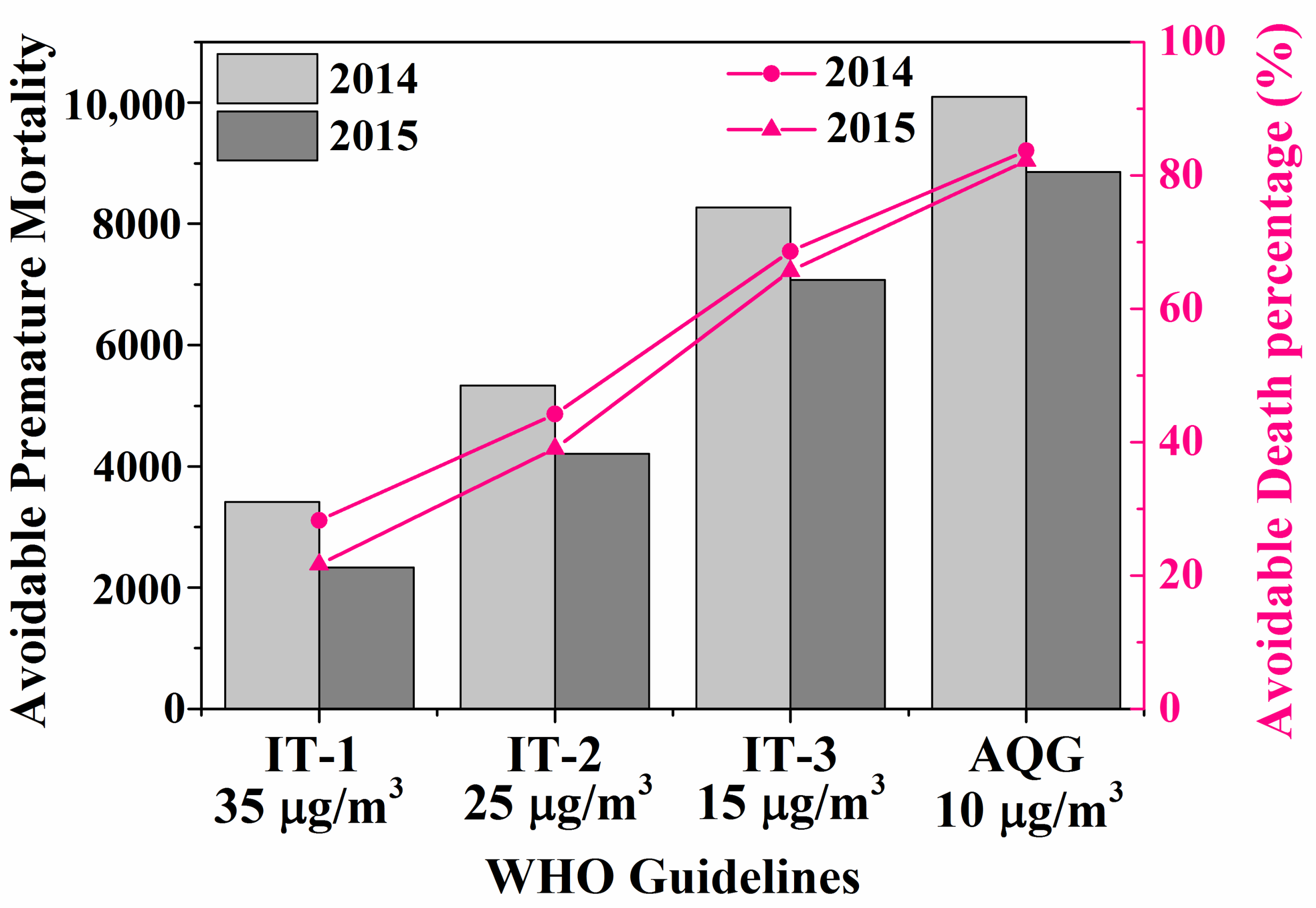
2.4. Evaluating the Effectiveness of PM2.5 Reduction
3. Results and Discussion
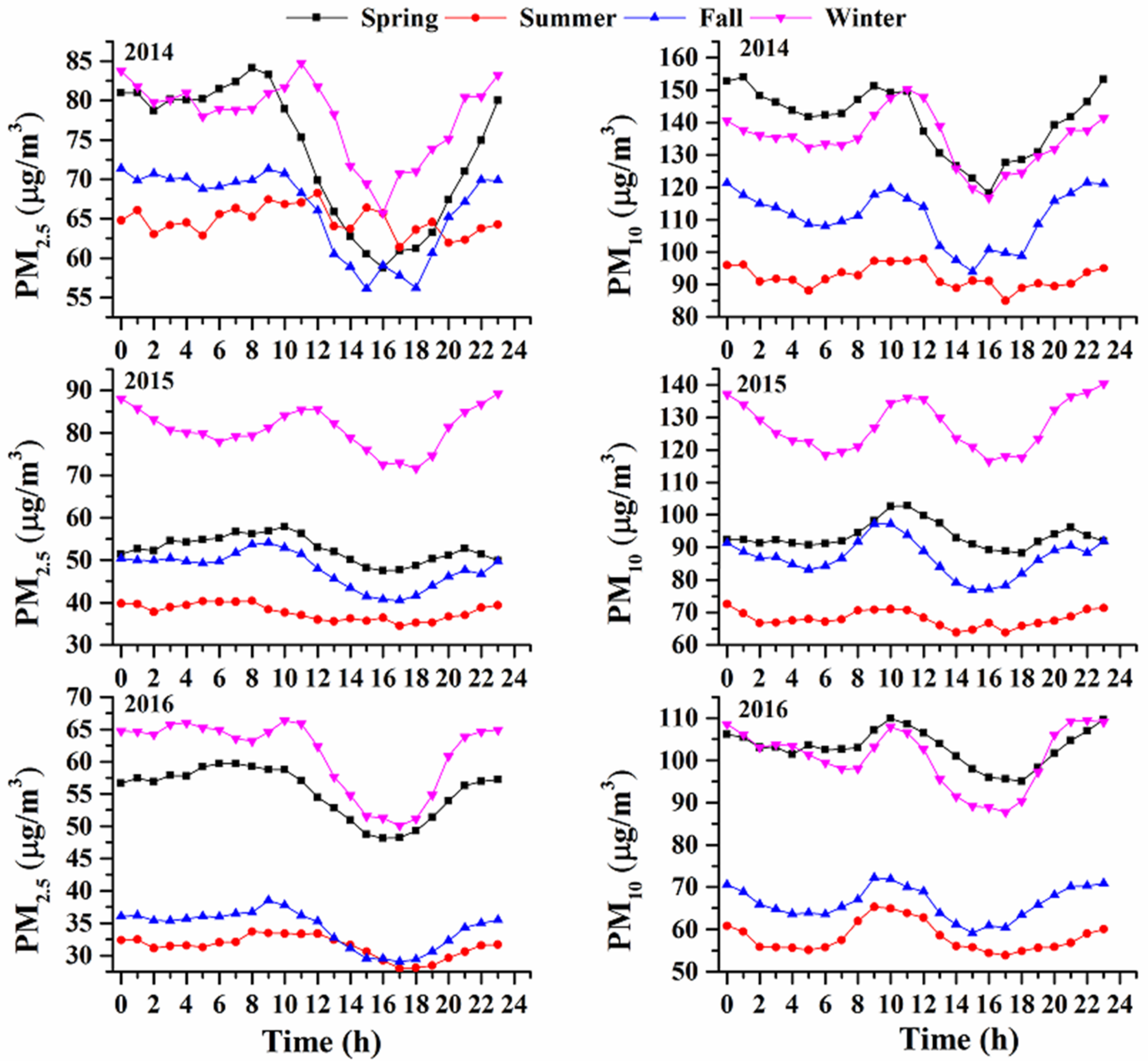
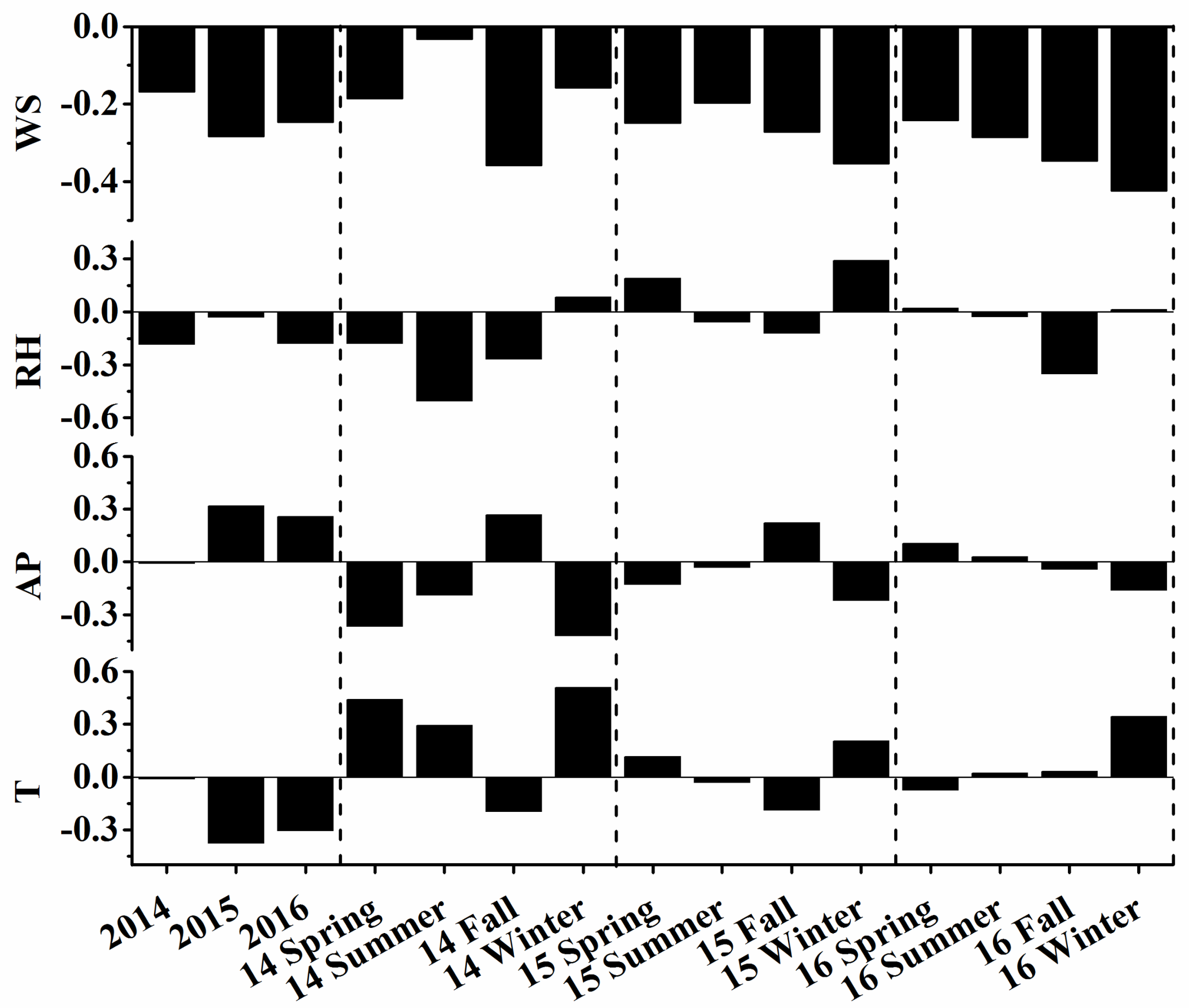
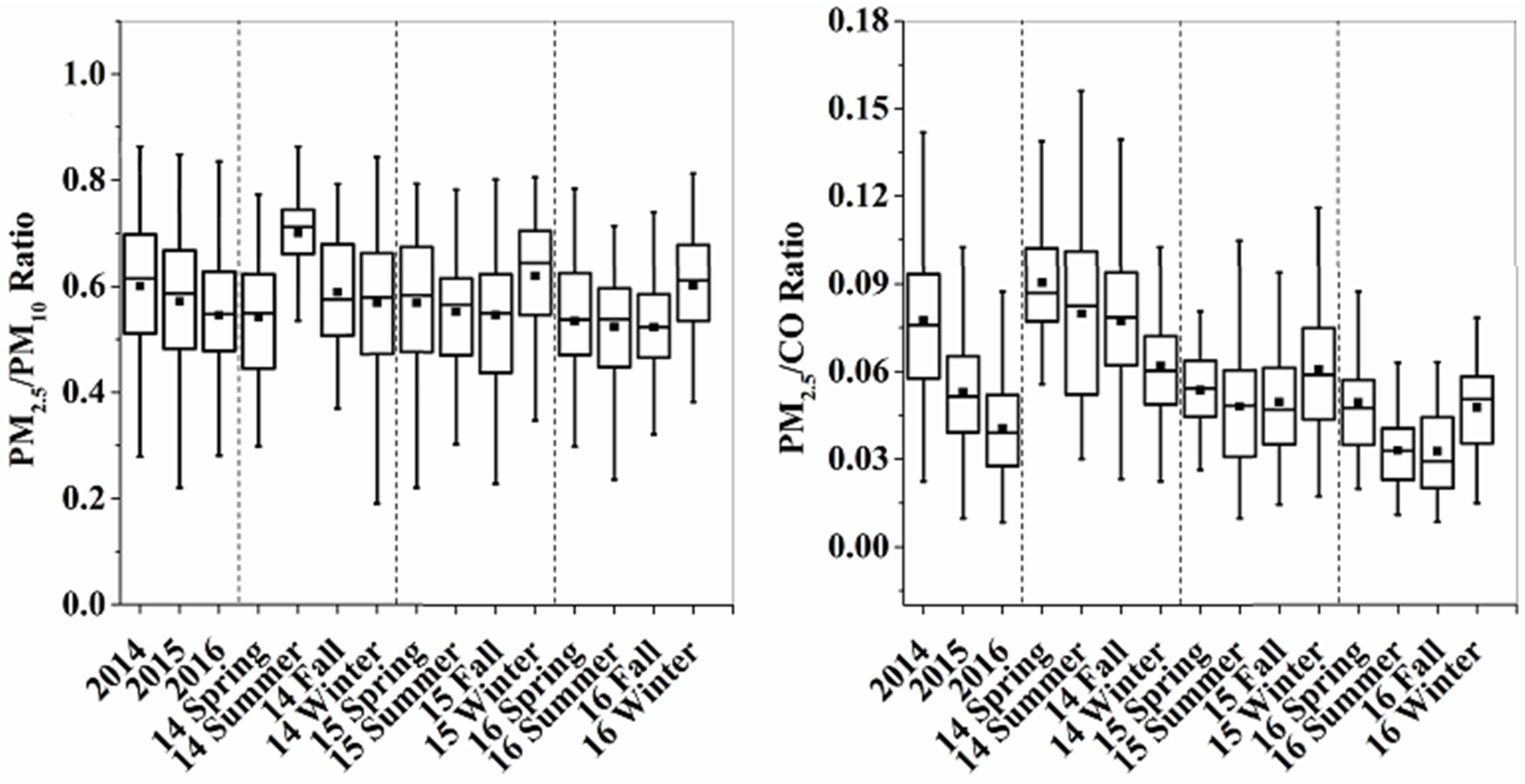
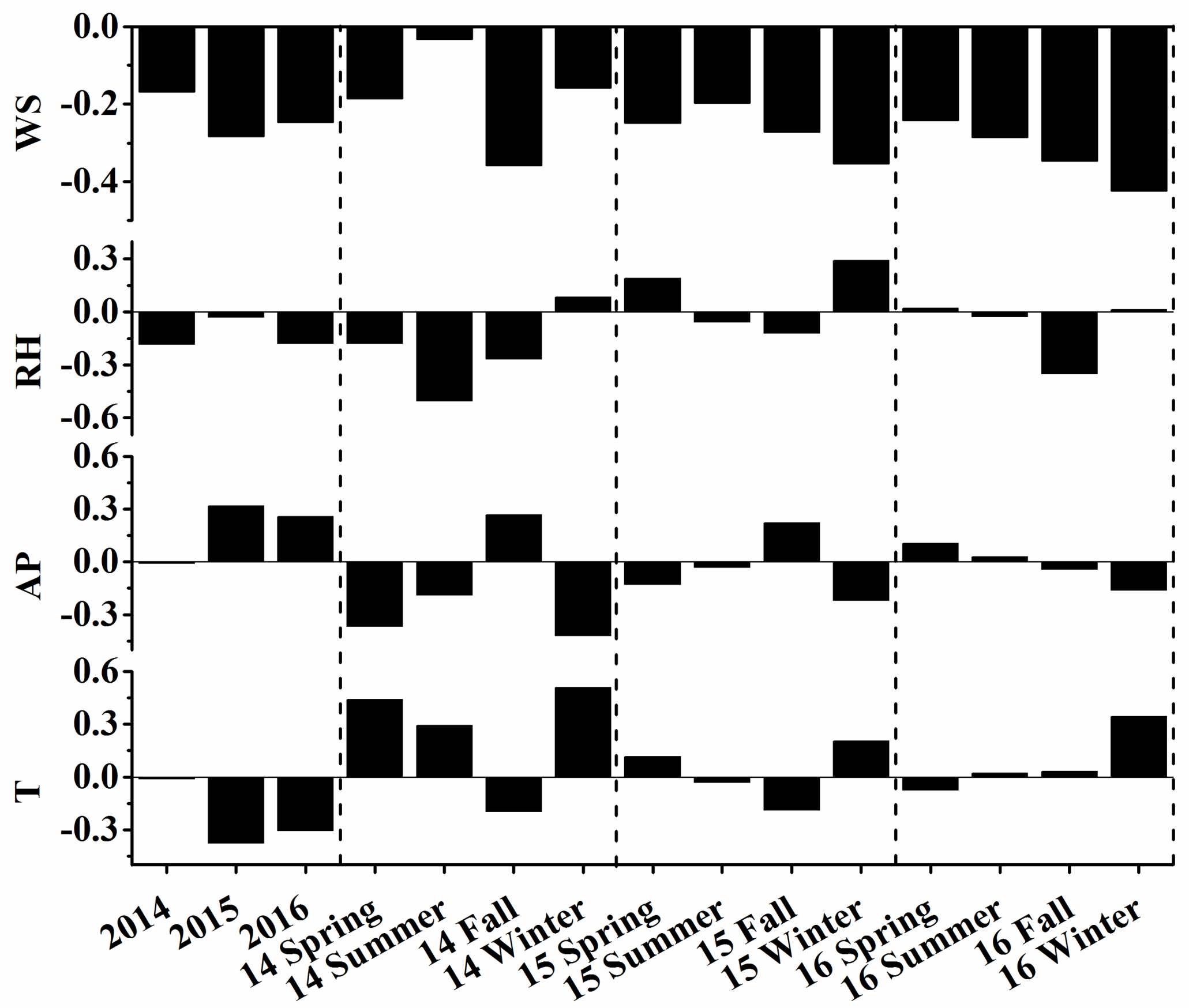
3.1. Characterization of PM2.5 Pollution in Nanjing
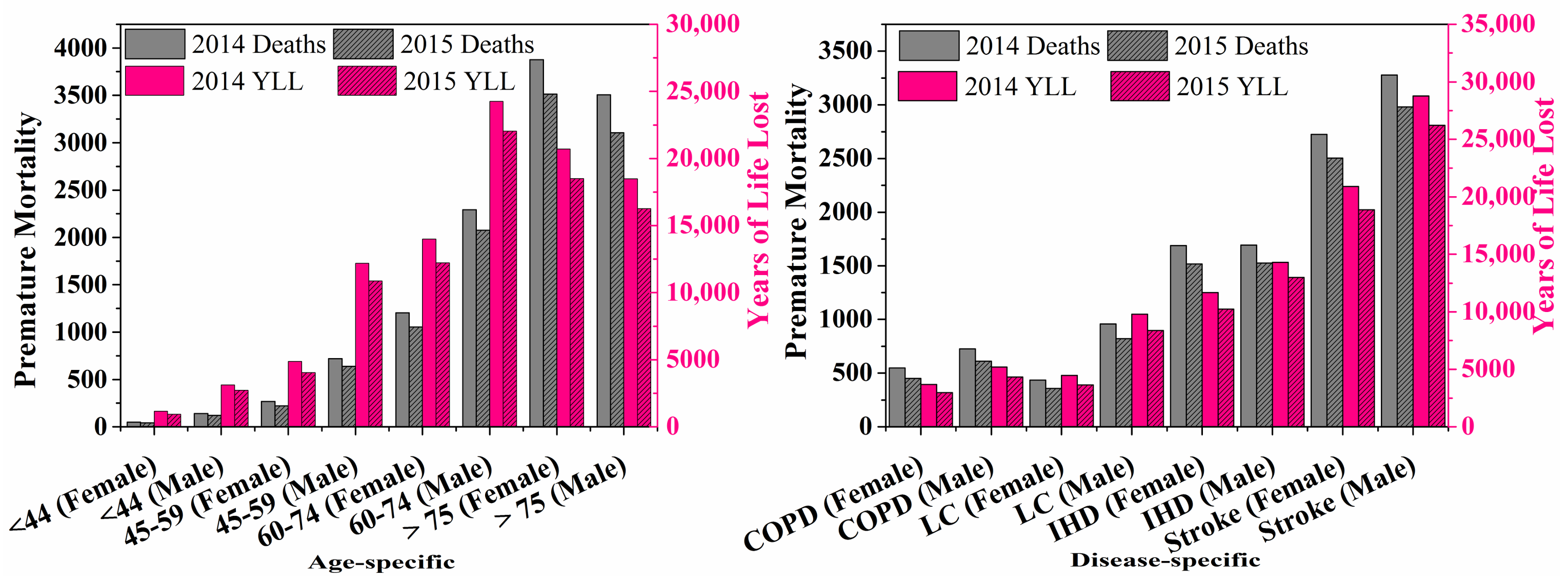
3.2. Health Burdens Attributable to PM2.5
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Li, X.; Ma, Y.; Wang, Y.; Liu, N.; Hong, Y. Temporal and spatial analyses of particulate matter (PM10 and PM2.5) and its relationship with meteorological parameters over an urban city in northeast China. Atmos. Res. 2017, 198, 185–193. [Google Scholar] [CrossRef]
- Xie, Y.; Zhao, B.; Zhang, L.; Luo, R. Spatiotemporal variations of PM2.5 and PM10 concentrations between 31 chinese cities and their relationships with SO2, NO2, CO and O3. Particuology 2015, 20, 141–149. [Google Scholar] [CrossRef]
- Chen, T.; He, J.; Lu, X.; She, J.; Guan, Z. Spatial and temporal variations of PM2.5 and its relation to meteorological factors in the urban area of Nanjing, China. Int. J. Environ. Res. Public Health 2016, 13, 921. [Google Scholar] [CrossRef] [PubMed]
- Zhan, D.; Kwan, M.-P.; Zhang, W.; Wang, S.; Yu, J. Spatiotemporal variations and driving factors of air pollution in China. Int. J. Environ. Public Health 2017, 14, 1538. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, Y.; Hu, J.; Ying, Q.; Hu, X.M. Relationships between meteorological parameters and criteria air pollutants in three megacities in China. Environ. Res. 2015, 140, 242–254. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; Brimblecombe, P. Regulatory effects on particulate pollution in the early hours of Chinese new year, 2015. Environ. Monit. Assess. 2017, 189, 467. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.L.; Cao, F. Fine particulate matter (PM2.5) in China at a city level. Sci. Rep. 2015, 5, 14884. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, C.; Bi, J. Development of land use regression models for PM2.5, SO2, NO2 and O3 in Nanjing, China. Environ. Res. 2017, 158, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, C.H.; Fu, J.S.; Huang, C.; Streets, D.G.; Huang, H.Y.; Zhang, G.F.; Wang, Y.J.; Jang, C.J.; Wang, H.L.; et al. Air quality and emissions in the Yangtze river delta, China. Atmos. Chem. Phys. 2011, 11, 1621–1639. [Google Scholar] [CrossRef] [Green Version]
- Luo, K.; Li, R.; Wang, Z.; Zhang, R.; Xu, Q. Effect modification of the association between temperature variability and daily cardiovascular mortality by air pollutants in three Chinese cities. Environ. Pollut. 2017, 230, 989–999. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Lin, Z.; Chen, R.; Norback, D.; Liu, C.; Kan, H.; Deng, Q.; Huang, C.; Hu, Y.; Zou, Z.; et al. The effects of PM2.5 on asthmatic and allergic diseases or symptoms in preschool children of six Chinese cities, based on China, children, homes and health (CCHH) project. Environ. Pollut. 2018, 232, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Speakman, J.R. Ambient particulate air pollution (PM2.5) is associated with the ratio of type 2 diabetes to obesity. Sci. Rep. 2017, 7, 9144. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Wang, Y.; Feng, W.; Wu, J.; Fu, C.; Deng, H.; Huang, J.; Wang, L.; Zheng, M.; Liu, H. Ambient air pollution and risk for ischemic stroke: A short-term exposure assessment in south China. Int. J. Environ. Public Health 2017, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, Y.; Liu, S.; Chen, X.; Zou, W.; Zhao, D.; Li, X.; Pu, J.; Huang, L.; Chen, J.; et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: Results from a cross-sectional study in China. Thorax 2017, 72, 788–795. [Google Scholar] [CrossRef] [PubMed]
- Shao, D.; Du, Y.; Liu, S.; Brunekreef, B.; Meliefste, K.; Zhao, Q.; Chen, J.; Song, X.; Wang, M.; Wang, J.; et al. Cardiorespiratory responses of air filtration: A randomized crossover intervention trial in seniors living in Beijing: Beijing indoor air purifier study, biapsy. Sci. Total. Environ. 2017, 603, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Girguis, M.S.; Strickland, M.J.; Hu, X.; Liu, Y.; Chang, H.H.; Belanoff, C.; Bartell, S.M.; Vieira, V.M. Chronic PM2.5 exposure and risk of infant bronchiolitis and otitis media clinical encounters. Int. J. Hyg. Environ. Health 2017, 220, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Stockfelt, L.; Andersson, E.M.; Molnar, P.; Gidhagen, L.; Segersson, D.; Rosengren, A.; Barregard, L.; Sallsten, G. Long-term effects of total and source-specific particulate air pollution on incident cardiovascular disease in Gothenburg, Sweden. Environ. Res. 2017, 158, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Mbelambela, E.P.; Hirota, R.; Eitoku, M.; Muchanga, S.M.J.; Kiyosawa, H.; Yasumitsu-Lovell, K.; Lawanga, O.L.; Suganuma, N. Occupation exposed to road-traffic emissions and respiratory health among Congolese transit workers, particularly bus conductors, in Kinshasa: A cross-sectional study. Environ. Health. Prev. Med. 2017, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Nenna, R.; Evangelisti, M.; Frassanito, A.; Scagnolari, C.; Pierangeli, A.; Antonelli, G.; Nicolai, A.; Arima, S.; Moretti, C.; Papoff, P.; et al. Respiratory syncytial virus bronchiolitis, weather conditions and air pollution in an Italian urban area: An observational study. Environ. Res. 2017, 158, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.T.; Iii, C.A.P.; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health. Perspect. 2014, 122, 397. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; He, J.; Wu, L.; Jin, T.; Chen, X.; Li, R.; Ren, P.; Zhang, L.; Mao, H. Health burden attributable to ambient PM2.5 in China. Environ. Pollut. 2017, 223, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Huang, L.; Chen, M.; Liao, H.; Zhang, H.; Wang, S.; Zhang, Q.; Ying, Q. Premature mortality attributable to particulate matter in China: Source contributions and responses to reductions. Environ. Sci. Technol. 2017, 51, 9950–9959. [Google Scholar] [CrossRef] [PubMed]
- Apte, J.S.; Marshall, J.D.; Cohen, A.J.; Brauer, M. Addressing global mortality from ambient PM2.5. Environ. Sci. Technol. 2015, 49, 8057–8066. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; van Donkelaar, A.; Martin, R.V.; Burnett, R.; Rainham, D.G.; Birkett, N.J.; Krewski, D. Estimates of global mortality attributable to particulate air pollution using satellite imagery. Environ. Res. 2013, 120, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Ge, X.; Hu, J.; Nie, D.; Tian, L.; Chen, M. Air pollution characteristics and health risks in Henan province, China. Environ. Res. 2017, 156, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Liu, T.; Xiao, J.; Zeng, W.; Li, X.; Guo, L.; Zhang, Y.; Xu, Y.; Tao, J.; Xian, H.; et al. Mortality burden of ambient fine particulate air pollution in six Chinese cities: Results from the pearl river delta study. Environ. Int. 2016, 96, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total. Environ. 2016, 568, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Anenberg, S.C.; Horowitz, L.W.; Tong, D.Q.; West, J.J. An estimate of the global burden of anthropogenic ozone and fine particulate matter on premature human mortality using atmospheric modeling. Environ. Health. Perspect. 2010, 118, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic impacts from PM2.5 pollution-related health effects in China: A provincial-level analysis. Environ. Sci. Technol. 2016, 50, 4836–4843. [Google Scholar] [CrossRef] [PubMed]
- Shiraiwa, M.; Ueda, K.; Pozzer, A.; Lammel, G.; Kampf, C.J.; Fushimi, A.; Enami, S.; Arangio, A.M.; Frohlich-Nowoisky, J.; Fujitani, Y.; et al. Aerosol health effects from molecular to global scales. Environ. Sci. Technol. 2017, 51, 13545–13567. [Google Scholar] [CrossRef] [PubMed]
- Lelieveld, J.; Barlas, C.; Giannadaki, D.; Pozzer, A. Model calculated global, regional and megacity premature mortality due to air pollution. Atmos. Chem. Phys. 2013, 13, 7023–7037. [Google Scholar] [CrossRef]
- Zheng, Y.; Xue, T.; Zhang, Q.; Geng, G.; Tong, D.; Li, X.; He, K. Air quality improvements and health benefits from china’s clean air action since 2013. Environ. Res. Lett. 2017, 12, 114020. [Google Scholar] [CrossRef]
- Wang, Y.; Ying, Q.; Hu, J.; Zhang, H. Spatial and temporal variations of six criteria air pollutants in 31 provincial capital cities in china during 2013–2014. Environ. Int. 2014, 73, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Yu, Y.; Yin, D.; He, J.; Liu, N.; Qu, J.; Xiao, J. Annual and diurnal variations of gaseous and particulate pollutants in 31 provincial capital cities based on in situ air quality monitoring data from china national environmental monitoring center. Environ. Int. 2016, 86, 92–106. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Chen, H.; Lin, Y.; Su, Q.; Cheng, L. Spatial variation of multiple air pollutants and their potential contributions to all-cause, respiratory, and cardiovascular mortality across China in 2015–2016. Atmos. Environ. 2017, 168, 23–35. [Google Scholar] [CrossRef]
- Pyrri, I.; Kapsanaki-Gotsi, E. Functional relations of airborne fungi to meteorological and pollution factors in a mediterranean urban environment. Fungal. Ecol. 2017, 30, 48–54. [Google Scholar] [CrossRef]
- Zu, Y.; Huang, L.; Hu, J.; Zhao, Z.; Liu, H.; Zhang, H.; Ying, Q.; Chen, M. Investigation of relationships between meteorological conditions and high PM10 pollution in a megacity in the western Yangtze river delta, china. Air Qual. Atmos. Health 2017, 10, 713–724. [Google Scholar] [CrossRef]
- Liang, P.; Zhu, T.; Fang, Y.; Li, Y.; Han, Y.; Wu, Y.; Hu, M.; Wang, J. The role of meteorological conditions and pollution control strategies in reducing air pollution in Beijing during APEC 2014 and victory parade 2015. Atmos. Chem. Phys. 2017, 17, 1–62. [Google Scholar] [CrossRef]
- Hu, X.-M.; Zhang, Y.; Jacobson, M.Z.; Chan, C.K. Coupling and evaluating gas/particle mass transfer treatments for aerosol simulation and forecast. J. Geophys. Res. Atmos. 2008, 113. [Google Scholar] [CrossRef]
- Sandeep, A.; Rao, T.N.; Ramkiran, C.N.; Rao, S.V.B. Differences in atmospheric boundary-layer characteristics between wet and dry episodes of the Indian summer monsoon. Bound. Layer Meteorol. 2014, 153, 217–236. [Google Scholar] [CrossRef]
- Archer, V.E.; Coons, T.; Saccomanno, G.; Hong, D.-Y. Latency and the lung cancer epidemic among United States uranium miners. Health Phys. 2004, 87, 480–489. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Annual Mean | Spring | Summer | Fall | Winter | |
|---|---|---|---|---|---|
| 2014 | 71 ± 35 | 74 ± 29 | 65 ± 34 | 67 ± 34 | 78 ± 42 |
| 2015 | 55 ± 33 | 53 ± 21 | 38 ± 21 | 47 ± 28 | 81 ± 42 |
| 2016 | 45 ± 29 | 55 ± 32 | 31 ± 16 | 34 ± 19 | 61 ± 32 |
| Average | 57 ± 34 | 60 ± 29 | 45 ± 29 | 49 ± 31 | 74 ± 40 |
| PM2.5 (μg/m3) | Attributable Fractions (AFs) (%) | ||||
|---|---|---|---|---|---|
| COPD | IHD | LC | Stroke | ||
| 2014 | 71 | 23 | 30 | 29 | 46 |
| 2015 | 55 | 20 | 28 | 25 | 44 |
| 2016 | 45 | 18 | 26 | 22 | 41 |
| IT-1 | 35 | 15 | 23 | 18 | 34 |
| IT-2 | 25 | 11 | 20 | 14 | 25 |
| IT-3 | 15 | 7 | 15 | 8 | 11 |
| AQG | 10 | 3 | 10 | 4 | 4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nie, D.; Chen, M.; Wu, Y.; Ge, X.; Hu, J.; Zhang, K.; Ge, P. Characterization of Fine Particulate Matter and Associated Health Burden in Nanjing. Int. J. Environ. Res. Public Health 2018, 15, 602. https://doi.org/10.3390/ijerph15040602
Nie D, Chen M, Wu Y, Ge X, Hu J, Zhang K, Ge P. Characterization of Fine Particulate Matter and Associated Health Burden in Nanjing. International Journal of Environmental Research and Public Health. 2018; 15(4):602. https://doi.org/10.3390/ijerph15040602
Chicago/Turabian StyleNie, Dongyang, Mindong Chen, Yun Wu, Xinlei Ge, Jianlin Hu, Kai Zhang, and Pengxiang Ge. 2018. "Characterization of Fine Particulate Matter and Associated Health Burden in Nanjing" International Journal of Environmental Research and Public Health 15, no. 4: 602. https://doi.org/10.3390/ijerph15040602