A Community-Driven Approach to Generate Urban Policy Recommendations for Obesity Prevention

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Project Context
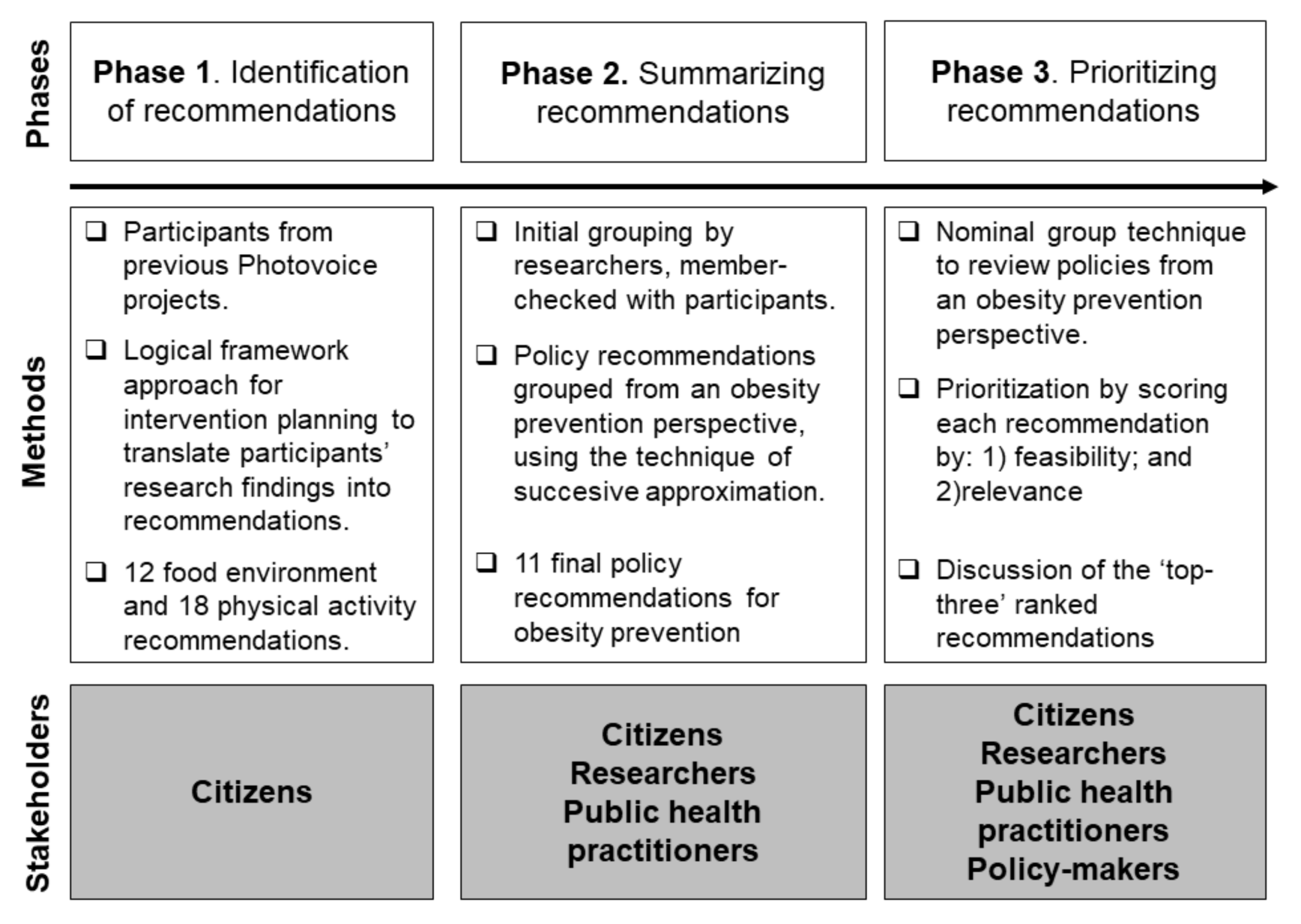
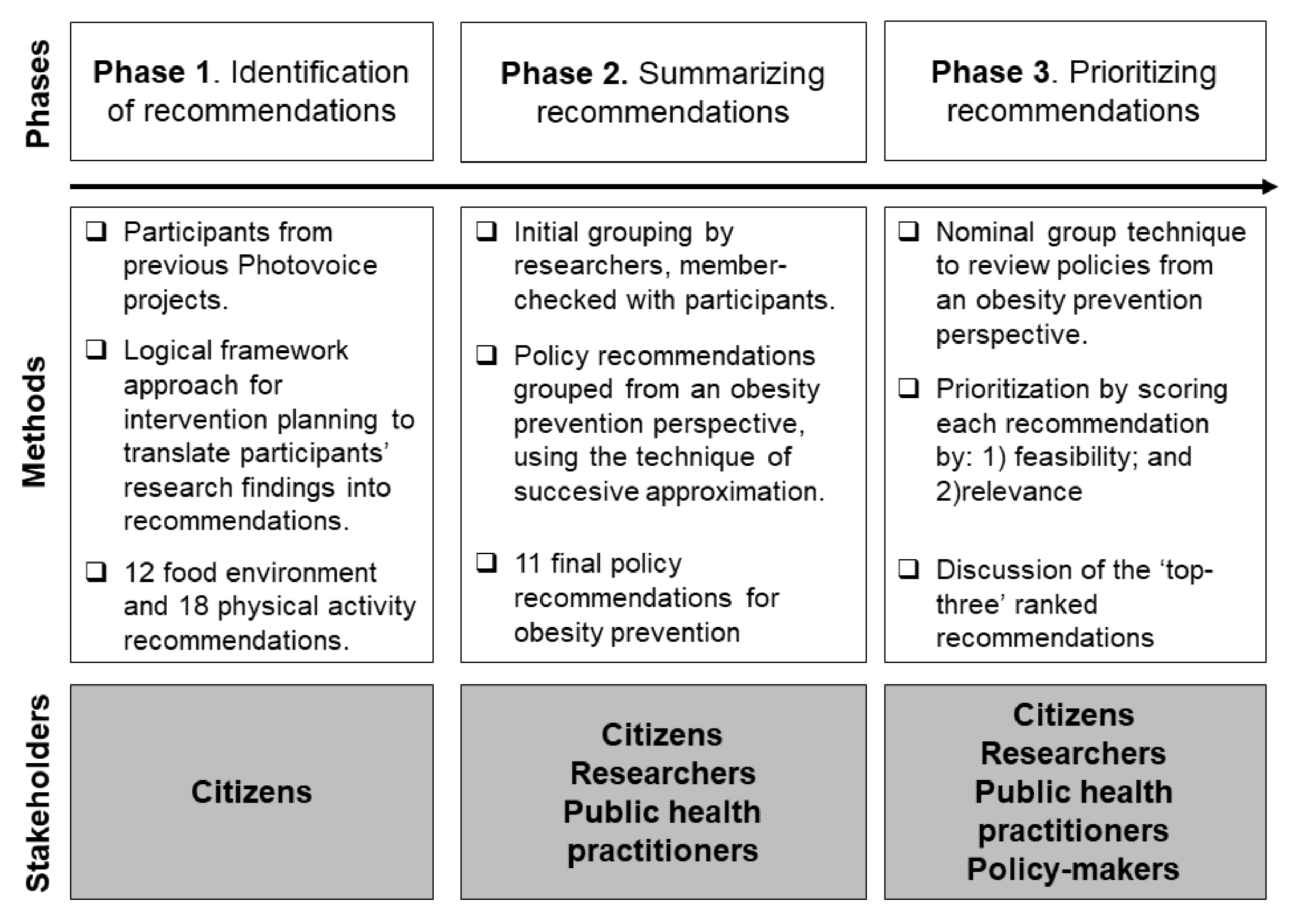
2.2. Study Design
2.3. Phase 1: Identification of Policy Recommendations
2.4. Phase 2: Summarizing Recommendations for Obesity Prevention
2.5. Phase 3: Prioritization Process
3. Results
3.1. Policy Recommendations to Promote Healthy Diet and Physical Activity
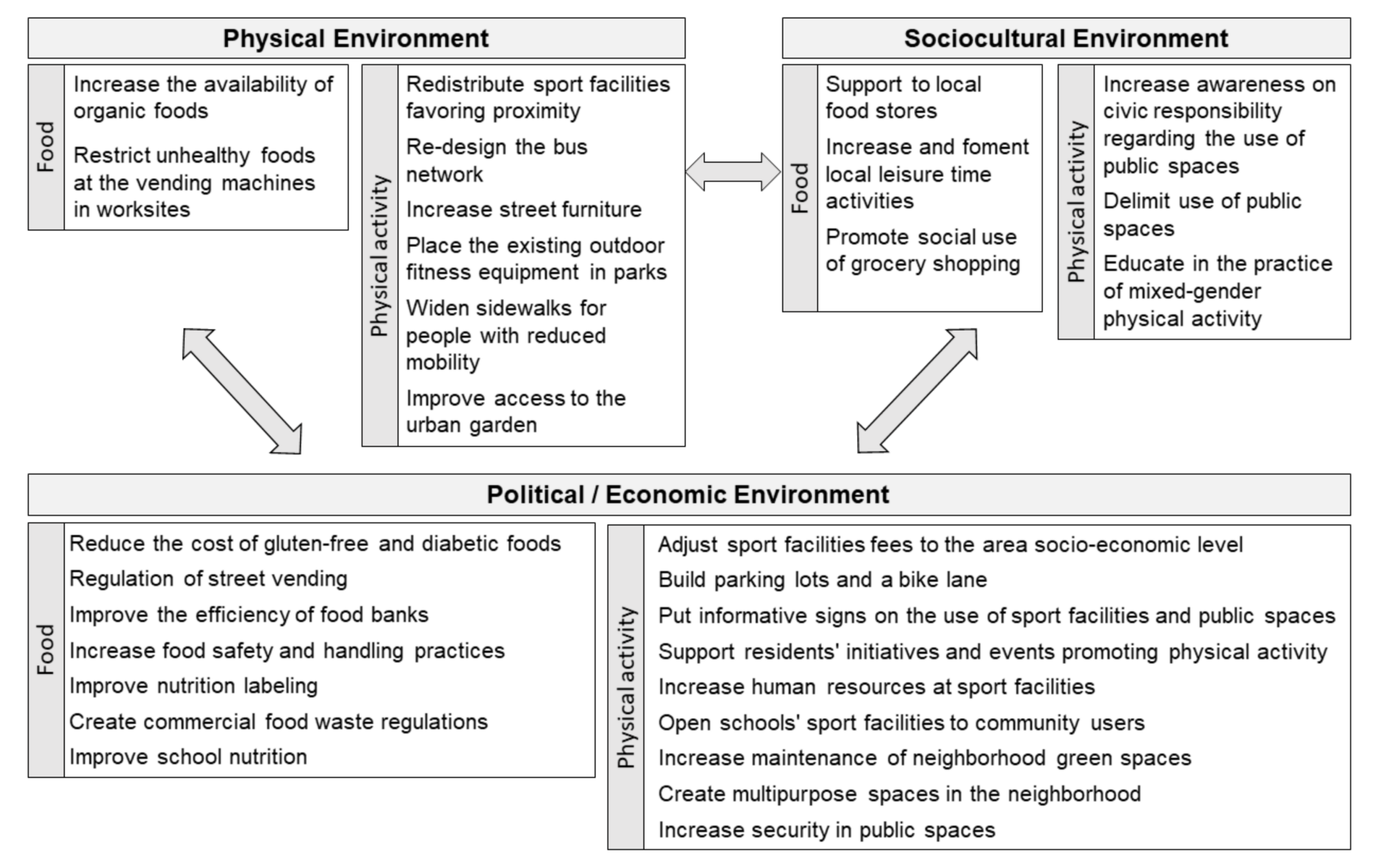
3.2. Urban Policy Recommendations for Obesity Prevention
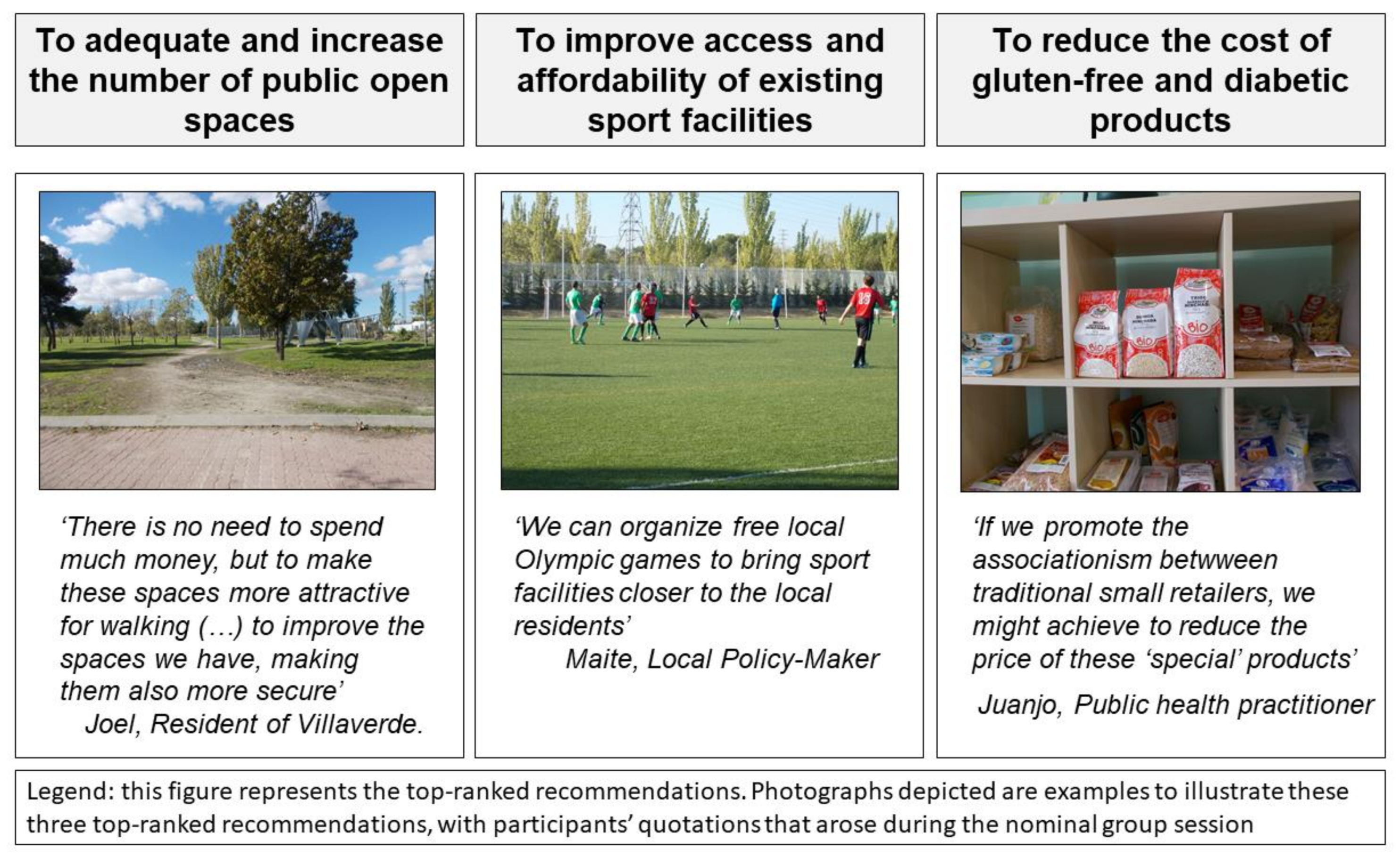
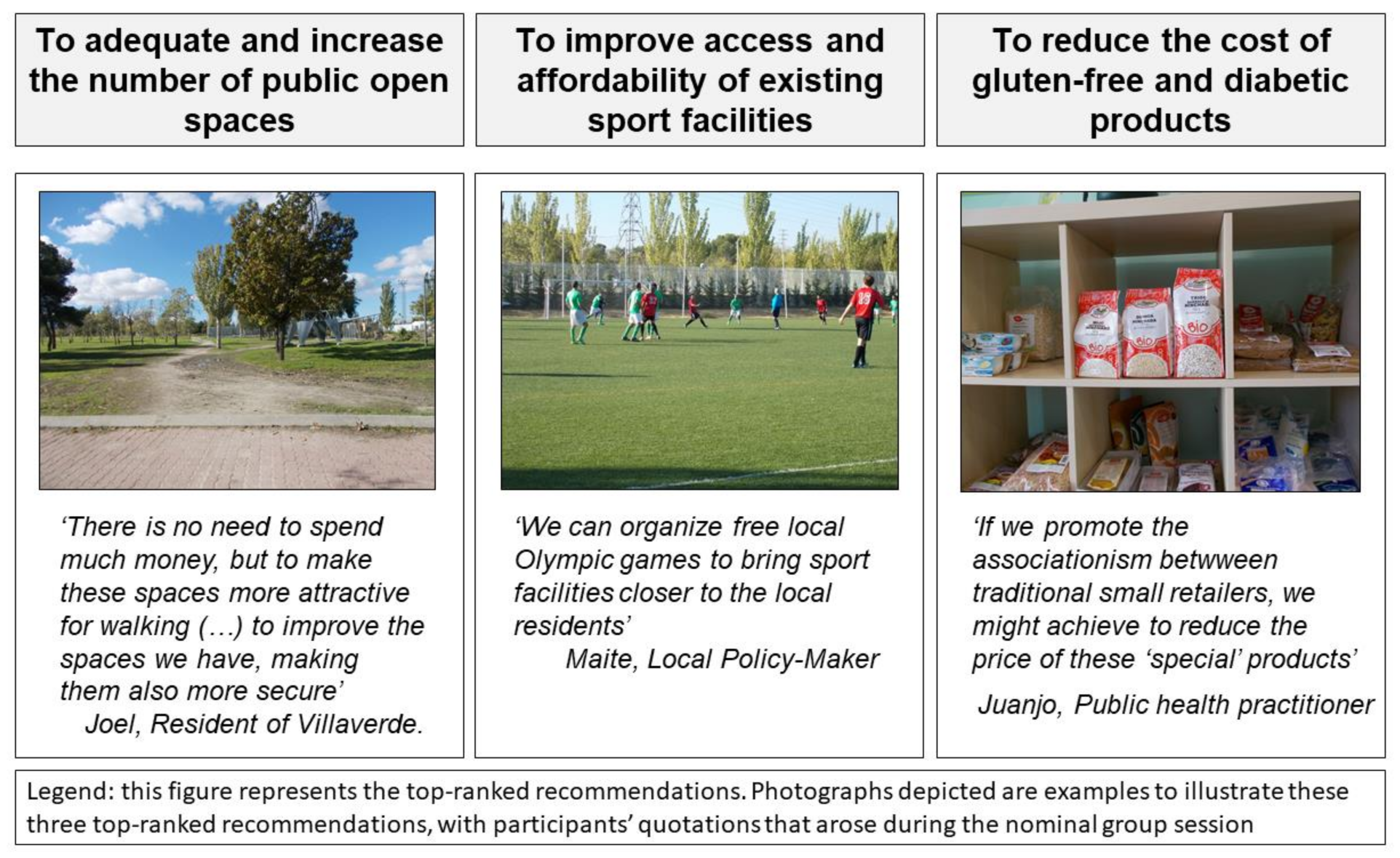
3.3. Ranked Set of Policy Recommendations
4. Discussion
Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. (Baltim.) 1999, 29, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N. Global, regional and national prevalence of overweight and obesity in children and adults 1980–2013: A systematic analysis. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Basterra-Gortari, F.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Gea, A.; Martinez-Gonzalez, M. Prevalence of obesity and diabetes in Spanish adults 1987–2012. Med. Clin. (Barc.) 2017, 148, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; De Vogli, R.; Gimeno, D.; Kivimaki, M. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Beydoun, M.A. The obesity epidemic in the United States—Gender, age, socioeconomic, racial/ethnic, and geographic characteristics: A systematic review and meta-regression analysis. Epidemiol. Rev. 2007, 29, 6–28. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Mourad, T.A.; Jildeh, C.; Abdeen, Z.; Philalithis, A.; Tzanakis, N. Obesity in Mediterranean region (1997–2007): A systematic review. Obes. Rev. 2008, 9, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Reques, L.; Giráldez-García, C.; Miqueleiz, E.; Belza, M.J.; Regidor, E. Educational differences in mortality and the relative importance of different causes of death: A 7-year follow-up study of Spanish adults. J. Epidemiol. Community Health 2014, 68, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Larranaga, I.; Arteagoitia, J.M.; Rodriguez, J.L.; Gonzalez, F.; Esnaola, S.; Pinies, J.A.; The Sentinel Practice Network of the Basque Country. Socio-economic inequalities in the prevalence of Type 2 diabetes, cardiovascular risk factors and chronic diabetic complications in the Basque Country, Spain. Diabet. Med. 2005, 22, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Franco, M.; Bilal, U.; Diez-Roux, A.V. Preventing non-communicable diseases through structural changes in urban environments. J. Epidemiol. Community Health 2015, 69, 509–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, S.L.; Sallis, J.F.; Ritenbaugh, C.; Hill, J.O.; Birch, L.L.; Frank, L.D.; Glanz, K.; Himmelgreen, D.A.; Mudd, M.; Popkin, B.M.; et al. Environmental and societal factors affect food choice and physical activity: Rationale. Nutr. Rev. 2001, 59, S21–S39. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Lovasi, G.S.; Hutson, M.A.; Guerra, M.; Neckerman, K.M. Built environments and obesity in disadvantaged populations. Epidemiol. Rev. 2009, 31, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Kligerman, M.; Sallis, J.F.; Ryan, S.; Frank, L.D.; Nader, P.R. Association of neighborhood design and recreation environment variables with physical activity and body mass index in adolescents. Am. J. Health Promot. 2007, 21, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Glass, T.A.; Curriero, F.C.; Stewart, W.F.; Schwartz, B.S. The built environment and obesity: A systematic review of the epidemiologic evidence. Health Place 2010, 16, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Michimi, A.; Wimberly, M.C. Spatial patterns of obesity and associated risk factors in the conterminous U.S. Am. J. Prev. Med. 2010, 39, e1–e12. [Google Scholar] [CrossRef] [PubMed]
- Congdon, P. Variations in obesity rates between US counties: Impacts of activity access, food environments, and settlement patterns. Int. J. Environ. Res. Public Health 2017, 14, 1023. [Google Scholar] [CrossRef] [PubMed]
- Townshend, T.; Lake, A. Obesogenic environments: Current evidence of the built and food environments. Perspect. Public Health 2016, 137, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Buscail, C.; Menai, M.; Salanave, B.; Daval, P.; Painsecq, M.; Lombrail, P.; Hercberg, S.; Julia, C. Promoting physical activity in a low-income neighborhood of the Paris suburb of Saint-Denis: Effects of a community-based intervention to increase physical activity. BMC Public Health 2016, 16, 667. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Sallis, J.F.; Sugiyama, T.; Frank, L.D.; Lowe, M.; Owen, N. Translating active living research into policy and practice: One important pathway to chronic disease prevention. J. Public Health Policy 2015, 36, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Kramer, L.; Schwartz, P.; Cheadle, A.; Borton, J.E.; Wright, M.; Chase, C.; Lindley, C. Promoting Policy and Environmental Change Using Photovoice in the Kaiser Permanente Community Health Initiative. Health Promot. Pract. 2010, 11, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Ministerio De Sanidad y consumo Estrategia NAOS. Invertir la Tend. la obesidad. Estrateg. para la Nutr. Act. Física y Prevención la Obesidad 2005, 40. (In Spanish) [Google Scholar] [CrossRef]
- Arnott, B.; Rehackova, L.; Errington, L.; Sniehotta, F.F.; Roberts, J.; Araujo-Soares, V. Efficacy of behavioural interventions for transport behaviour change: Systematic review, meta-analysis and intervention coding. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 133. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Kumar, M.B. Preventing childhood obesity and diabetes: Is it time to move out of the school? Pediatr. Diabetes 2007, 8, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Corburn, J. Bringing local knowledge into environmental decision making: Improving urban planning for communities at risk. J. Plan. Educ. Res. 2003, 22, 420–433. [Google Scholar] [CrossRef]
- Díez, J.; Valiente, R.; Ramos, C.; García, R.; Gittelsohn, J.; Franco, M. The mismatch between observational measures and residents’ perspectives on the retail food environment: A mixed-methods approach in the Heart Healthy Hoods study. Public Health Nutr. 2017, 20, 2970–2979. [Google Scholar] [CrossRef] [PubMed]
- Hergenrather, K.C.; Rhodes, S.D.; Cowan, C.A.; Bardhoshi, G.; Pula, S. Photovoice as community-based participatory research: A qualitative review. Am. J. Health Behav. 2009, 33, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Cash, J.L.; Powers, L.S. Who Knows the Streets as Well as the Homeless? Promoting Personal and Community Action through Photovoice. Health Promot. Pract. 2000, 1, 81–89. [Google Scholar] [CrossRef]
- Wang, C.; Burris, M.A. Photovoice: Concept, Methodology, and Use for Participatory Needs Assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [PubMed]
- Wang, C. Photovoice: A participatory action research strategy applied to women’s health. J. Women’s Health 1999, 8, 185–192. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. The conceptual, historical, and practice roots of community based participatory research and related participatory traditions. In Community-Based Participatory Research for Health; John Wiley & Sons, Inc.: New York, NY, USA, 2003; pp. 27–52. ISBN 1118045440. [Google Scholar]
- Israel, B.A.; Coombe, C.M.; Cheezum, R.R.; Schulz, A.J.; McGranaghan, R.J.; Lichtenstein, R.; Reyes, A.G.; Clement, J.; Burris, A. Community-based participatory research: A capacity-building approach for policy advocacy aimed at eliminating health disparities. Am. J. Public Health 2010, 100, 2094–2102. [Google Scholar] [CrossRef] [PubMed]
- Catalani, C.; Minkler, M. Photovoice: A Review of the Literature in Health and Public Health. Health Educ. Behav. 2010, 37, 424–451. [Google Scholar] [CrossRef] [PubMed]
- Belon, A.P.; Nieuwendyk, L.M.; Vallianatos, H.; Nykiforuk, C.I.J. Perceived community environmental influences on eating behaviors: A Photovoice analysis. Soc. Sci. Med. 2016, 171, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Belon, A.P.; Nieuwendyk, L.M.; Vallianatos, H.; Nykiforuk, C.I.J. How community environment shapes physical activity: Perceptions revealed through the PhotoVoice method. Soc. Sci. Med. 2014, 116, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Díez, J.; Conde, P.; Sandin, M.; Urtasun, M.; López, R.; Carrero, J.L.; Gittelsohn, J.; Franco, M. Understanding the local food environment: A participatory photovoice project in a low-income area in Madrid, Spain. Health Place 2017, 43, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Evaluation and Research Methods; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2002; ISBN 0803937792. [Google Scholar]
- Sackett, C.R.; Newhart, S.; Jenkins, A.M.; Cory, L. Girls’ Perspectives of Barriers to Outdoor Physical Activity through Photovoice: A Call for Counselor Advocacy. J. Creat. Ment. Health 2017, 1–17. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- NORAD. The Logical Framework Approach (LFA)—Handbook for objectives-oriented planning. In Zhurnal Eksperimentalnoi I Teoreticheskoi Fiziki; NORAD: Oslo, Norway, 1999; Volume 107. [Google Scholar]
- Neuman, L.W. Social Research Methods: Quantitative and Qualitative Approaches; Allyn Barcon: Boston, MA, USA, 2005; Volume 13, pp. 1–6. [Google Scholar]
- Mahmood, A.; Chaudhury, H.; Michael, Y.L.; Campo, M.; Hay, K.; Sarte, A. A photovoice documentation of the role of neighborhood physical and social environments in older adults’ physical activity in two metropolitan areas in North America. Soc. Sci. Med. 2012, 74, 1180–1192. [Google Scholar] [CrossRef] [PubMed]
- Van de Ven, A.H.; Delbecq, A.L. The nominal group as a research instrument for exploratory health studies. Am. J. Public Health 1972, 62, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Shirk, J.L.; Ballard, H.L.; Wilderman, C.C.; Phillips, T.; Wiggins, A.; Jordan, R.; McCallie, E.; Minarchek, M.; Lewenstein, B.V.; Krasny, M.E.; et al. Public participation in scientific research: A framework for deliberate design. Ecol. Soc. 2012, 17. [Google Scholar] [CrossRef]
- Wang, C.C.; Redwood-Jones, Y.A. Photovoice ethics: Perspectives from flint photovoice. Health Educ. Behav. 2001, 28, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Rose, G. Sick individuals and sick populations. Int. J. Epidemiol. 1985, 14, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Recommended Community Strategies and Measurements to Prevent Obesity in the United States. Surveillance Summaries. MMWR 2009, 58, 1–26. [Google Scholar]
- Monterrosa, E.C.; Campirano, F.; Mayo, L.T.; Frongillo, E.A.; Cordero, S.H.; Kaufer-Horwitz, M.; Rivera, J.A. Stakeholder perspectives on national policy for regulating the school food environment in Mexico. Health Policy Plan. 2015, 30, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Besson, H.; Brage, S.; Jakes, R.W.; Ekelund, U.; Wareham, N.J. Estimating physical activity energy expenditure, sedentary time, and physical activity intensity by self-report in adults. Am. J. Clin. Nutr. 2010, 91, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Courtemanche, C.; Carden, A. Supersizing supercenters? The impact of Walmart Supercenters on body mass index and obesity. J. Urban Econ. 2011, 69, 165–181. [Google Scholar] [CrossRef]
- Asfaw, A. Does consumption of processed foods explain disparities in the body weight of individuals? The case of Guatemala. Health Econ. 2011, 20, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Diez, J.; Bilal, U.; Cebrecos, A.; Buczynski, A.; Lawrence, R.S.; Glass, T.; Escobar, F.; Gittelsohn, J.; Franco, M. Understanding differences in the local food environment across countries: A case study in Madrid (Spain) and Baltimore (USA). Prev. Med. (Baltim.) 2016, 89, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Pettinger, C.; Holdsworth, M.; Gerber, M. “All under one roof?” Differences in food availability and shopping patterns in Southern France and Central England. Eur. J. Public Health 2008, 18, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Flavián, C.; Haberberg, A.; Polo, Y. Food retailing strategies in the European union. A comparative analysis in the UK and Spain. J. Retail. Consum. Serv. 2002, 9, 125–138. [Google Scholar] [CrossRef]
- Dankwa-Mullan, I.; Pérez-Stable, E.J. Addressing health disparities is a place-based issue. Am. J. Public Health 2016, 106, 637–639. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Population-Based Prevention Strategies for Childhood Obesity; Report of the WHO Forum Technical Meeting; World Health Organization: Geneva, Switzerland, 2010; Volume 40. [Google Scholar]
- Teti, M.; Pichon, L.; Kabel, A.; Farnan, R.; Binson, D. Taking pictures to take control: Photovoice as a tool to facilitate empowerment among poor and racial/ethnic minority women with HIV. J. Assoc. Nurses AIDS Care 2013, 24, 539–553. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, S.D.; Kelley, C.; Simán, F.; Cashman, R.; Alonzo, J.; McGuire, J.; Wellendorf, T.; Hinshaw, K.; Allen, A.B.; Downs, M.; Brown, M.; Martínez, O.; et al. Using Community-Based Participatory Research (CBPR) to Develop a Community-Level HIV Prevention Intervention for Latinas: A Local Response to a Global Challenge. Women’s Health Issues 2012, 22, e293–e301. [Google Scholar] [CrossRef] [PubMed]
- Budig, K.; Diez, J.; Conde, P.; Sastre, M.; Hernan, M.; Franco, M. Photovoice and empowerment: Evaluating the transformative potential of a Participatory Action Research project. BMC Public Health 2018. [Google Scholar] [CrossRef]
- World Health Organization—WHO. WHO|The Ottawa Charter for Health Promotion; First International Conference on Health Promotion, Ottawa, 21 November 1986; World Health Organization: Geneva, Switzerland, 2013; pp. 3–5. [Google Scholar] [CrossRef]
- Johnston, G. Champions for social change: Photovoice ethics in practice and “false hopes” for policy and social change. Glob. Public Health 2016, 11, 799–811. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D.; Bowman, K. Still learning: A critical reflection on three years of measuring women’s empowerment in Oxfam. Gend. Dev. 2014, 22, 253–269. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of community-based research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Wallerstein, N. Power between evaluator and community: Research relationships within New Mexico’s healthier communities. Soc. Sci. Med. 1999, 49, 39–53. [Google Scholar] [CrossRef]
- Freudenberg, N. Health promotion in the city: A review of current practice and future prospects in the United States. Annu. Rev. Public Health 2000, 21, 473–503. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Morrel-Samuels, S.; Hutchison, P.M.; Bell, L.; Pestronk, R.M. Flint photovoice: Community building among youths, adults, and policymakers. Am. J. Public Health 2004, 94, 911–913. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Action Area | Environmental Recommendation |
|---|---|
| Physical activity |
|
| Physical activity |
|
| Food environment |
|
| Physical activity/Food environment |
|
| Food environment |
|
| Physical activity/Food environment |
|
| Physical activity |
|
| Physical activity |
|
| Physical activity |
|
| Food environment |
|
| Food environment |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Díez, J.; Gullón, P.; Sandín Vázquez, M.; Álvarez, B.; Martín, M.D.P.; Urtasun, M.; Gamarra, M.; Gittelsohn, J.; Franco, M. A Community-Driven Approach to Generate Urban Policy Recommendations for Obesity Prevention. Int. J. Environ. Res. Public Health 2018, 15, 635. https://doi.org/10.3390/ijerph15040635
Díez J, Gullón P, Sandín Vázquez M, Álvarez B, Martín MDP, Urtasun M, Gamarra M, Gittelsohn J, Franco M. A Community-Driven Approach to Generate Urban Policy Recommendations for Obesity Prevention. International Journal of Environmental Research and Public Health. 2018; 15(4):635. https://doi.org/10.3390/ijerph15040635
Chicago/Turabian StyleDíez, Julia, Pedro Gullón, María Sandín Vázquez, Belén Álvarez, María Del Prado Martín, María Urtasun, Maite Gamarra, Joel Gittelsohn, and Manuel Franco. 2018. "A Community-Driven Approach to Generate Urban Policy Recommendations for Obesity Prevention" International Journal of Environmental Research and Public Health 15, no. 4: 635. https://doi.org/10.3390/ijerph15040635