German Public Support for Tobacco Control Policy Measures: Results from the German Study on Tobacco Use (DEBRA), a Representative National Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Participants
2.2. Measures
2.2.1. Policy Questions
- “The sale of cigarettes and tobacco in Germany should be banned completely within the next 10 years.”
- “The legal age of sale of cigarettes and tobacco in Germany should be raised from 18 to 21.”
- “Tobacco industry sales should be taxed in order to use the money to address problems caused by tobacco (e.g., health issues, environmental problems, etc.).”
- “It should be assessed whether e-cigarettes are safe and effective in assisting smokers to quit.”
- “When minor children are in the car, smoking inside the car should be banned and subjected to punishment.”
- “Strongly support”
- “Tend to support”
- “No opinion either way”
- “Tend to oppose”
- “Strongly oppose”
- “No answer”
2.2.2. Socio-Demographic Characteristics
2.2.3. Smoking Characteristics
2.3. Analyses
3. Results
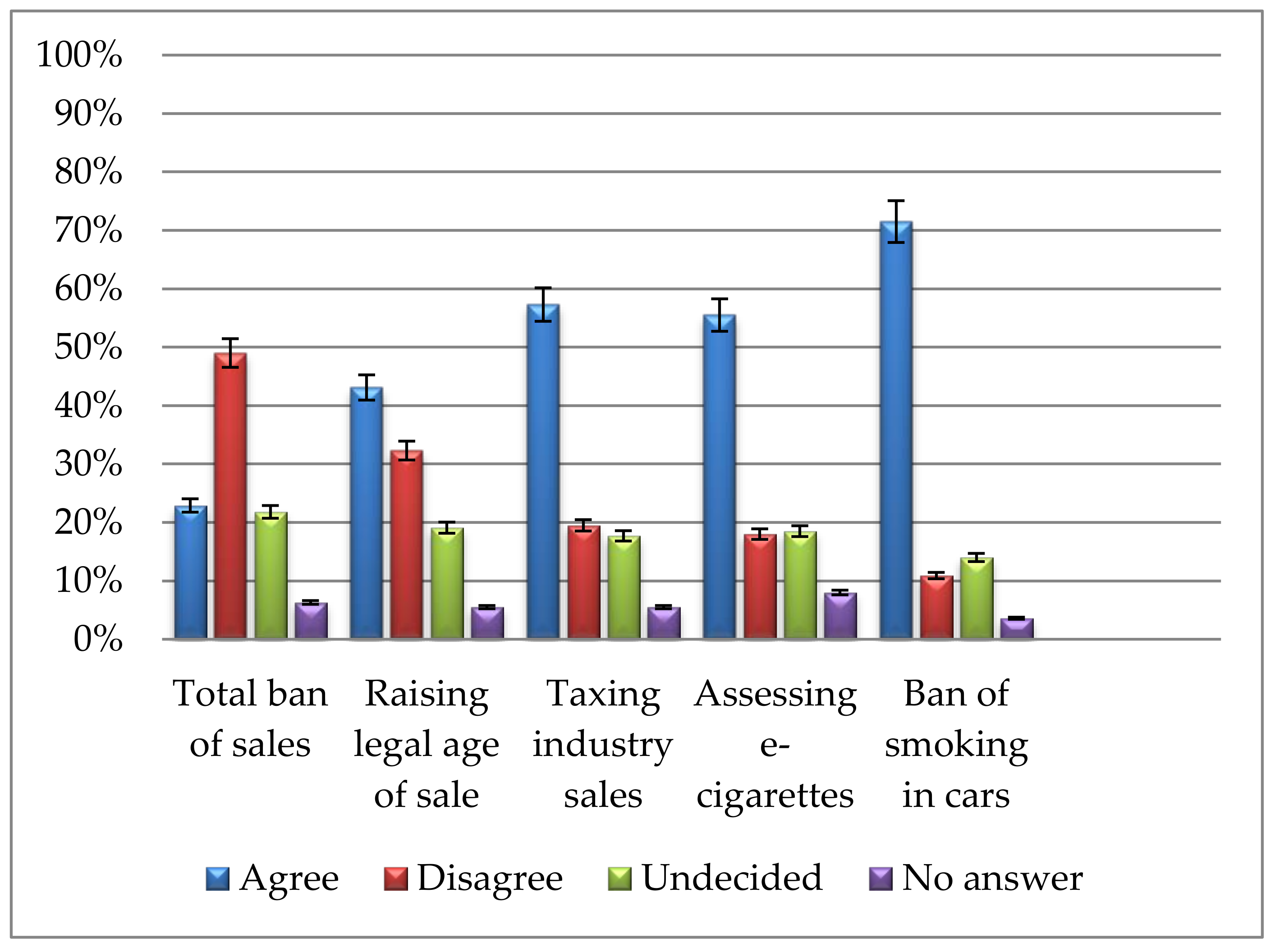
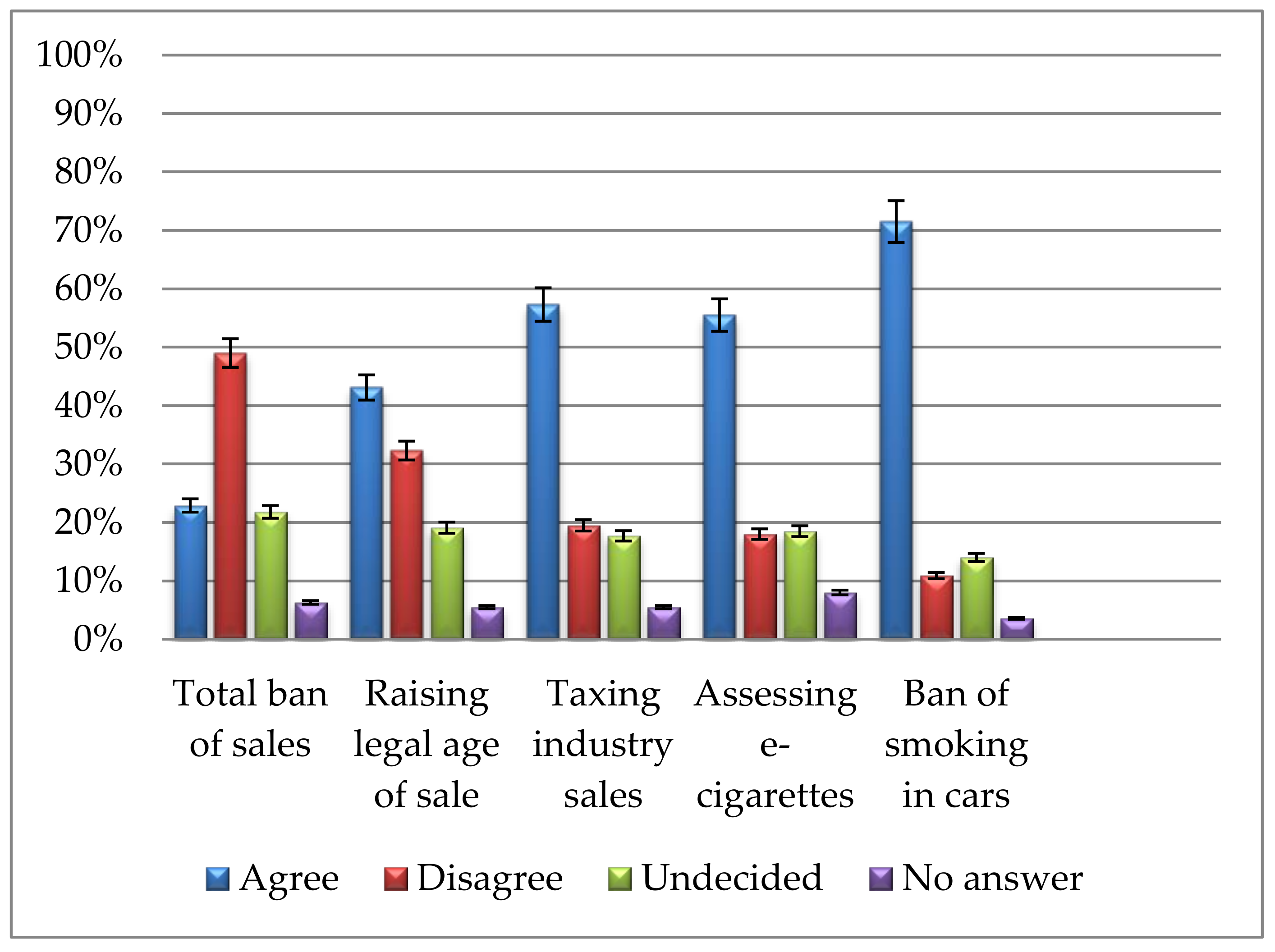
3.1. Public Support for Tobacco Policy Measures
3.2. Results from the Regression Analysis
3.2.1. Support for a Total Ban on Tobacco Sales
3.2.2. Support for Raising the Legal Age of Sale
3.2.3. Support for Special Taxation of Tobacco Industry Profits
3.2.4. Support for Assessing the Effectiveness and Safety of EC as Cessation Aids
3.2.5. Support for Ban on Smoking in Cars When Children Are Present
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kotz, D.; Boeckmann, M.; Kastaun, S. The use of tobacco, e-cigarettes, and methods to quit smoking in Germany—A representative study using 6 waves of data over 12 months (the DEBRA study). Dtsch. Ärzteblatt Int. 2018, 115, 235–242. [Google Scholar]
- Mons, U.; Kahnert, S. Neuberechnung der tabakattributablen Mortalität—Nationale und regionale Daten für Deutschland (Recalculation of Tobacco-Attributable Mortality: National and Regional Data for Germany). Das Gesundheitswes. 2017. [Google Scholar] [CrossRef]
- Kuntz, B.; Lampert, T. Smoking and Passive Smoke Exposure Among Adolescents in Germany. Dtsch. Arztebl. Int. 2016, 113, 23–30. [Google Scholar] [PubMed]
- Bolte, G.; Fromme, H. Socioeconomic determinants of children’s environmental tobacco smoke exposure and family’s home smoking policy. Eur. J. Public Health 2008, 19, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Thyrian, J.R.; Hanke, M.; Hannöver, W.; Grempler, J.; Röske, K.; Fusch, C.; John, U. Tabakrauchexposition in der Wohnung und stationäre Behandlungen von Kindern unter 5 Jahren in Deutschland [Exposure to tobacco smoke (passive smoking) in the home and inpatient treatment of children under the age of 5 years in Germany]. DMW Dtsch. Medizinische Wochenschrift 2005, 130, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, M.B.; Fullman, N.; Ng, M.; Salama, J.S.; Abajobir, A.; Abate, K.H.; Abbafati, C.; Abera, S.F.; Abraham, B.; Abyu, G.Y. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef]
- Grüning, T.; Strünck, C.; Gilmore, A. Puffing Away? Explaining the Politics of Tobacco Control in Germany. Ger. Polit. 2008, 17, 140–164. [Google Scholar] [CrossRef]
- Grüning, T.; Gilmore, A. Germany: Tobacco industry still dictates policy. Tob. Control 2007, 16, 2. [Google Scholar] [PubMed]
- Joossens, L.; Raw, M. The Tobacco Control Scale 2016 in Europe; European Commission: Brussels, 2017. [Google Scholar]
- Framework Convention Alliance Parties to the WHO FCTC (Ratifications and Accessions). Available online: http://www.fctc.org/about-fca/tobacco-control-treaty/latest-ratifications/parties-ratifications-accessions (accessed on 14 December 2017).
- Hefler, M. Germany: The tide to turn with graphic health warnings? Worldwide news and comment. Tob. Control 2016, 25, 263–266. [Google Scholar]
- Grüning, T.; Weishaar, H.; Collin, J.; Gilmore, A.B. Tobacco industry attempts to influence and use the German government to undermine the WHO Framework Convention on Tobacco Control. Tob. Control 2012, 21, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuters Staff Italy Cracks Down on Smokers as Tough Law Takes Effect. Available online: http://www.reuters.com/article/us-health-italy-smoking-idUSKCN0VB1I3 (accessed on 14 December 2017).
- Hofverberg, E. Finland: New Tobacco Law Adopted with Intent of Eliminating Tobacco Use. Available online: http://www.loc.gov/law/foreign-news/article/finland-new-tobacco-law-adopted-with-intent-of-eliminating-tobacco-use/ (accessed on 14 December 2017).
- Triggle, N. Car Smoking Ban Comes into Force. Available online: http://www.bbc.com/news/health-34402622 (accessed on 14 December 2017).
- Welsh Government Ban on Smoking in Cars Carrying Children Begins. Available online: http://gov.wales/newsroom/health-and-social-services/2015/151001ban/?lang=en (accessed on 14 December 2017).
- Ireland Department of Health Varadkar Announces Start Date for Smoking Ban in Cars Where Children Are Present. Available online: http://health.gov.ie/blog/press-release/varadkar-announces-start-date-for-smoking-ban-in-cars-where-children-are-present/ (accessed on 14 December 2017).
- Neue Kampagne Soll Kinder vor Passivrauchen im Auto Schützen (New Campaign Supposed to Protect Children from Smoke Exposure in Cars). Available online: https://www.aerzteblatt.de/nachrichten/69788/Neue-Kampagne-soll-Kinder-vor-Passivrauchen-im-Auto-schuetzen (accessed on 14 December 2017).
- Batra, A. Treatment of tobacco dependence. Dtsch. Arztebl. Int. 2011, 108, 555–564. [Google Scholar] [PubMed]
- Twardella, D.; Brenner, H. Effects of practitioner education, practitioner payment and reimbursement of patients’ drug costs on smoking cessation in primary care: A cluster randomised trial. Tob. Control 2007, 16, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Reda, A.A.; Kaper, J.; Fikretler, H.; Severens, J.L.; van Schayck, C.P. Healthcare financing systems for increasing the use of tobacco dependence treatment. Cochrane Database Syst. Rev. 2009, CD004305. [Google Scholar]
- Kröger, C.; Gradl, S. Tabakentwöhnungsmaßnahmen in Deutschland. Bundesgesundheitsblatt Gesundheitsforsch. Gesundheitsschutz 2010, 53, 201–206. [Google Scholar] [CrossRef] [PubMed]
- DEBRA Study. Available online: www.debra-study.info (accessed on 22 August 2017).
- Shahab, L.; Goniewicz, M.L.; Blount, B.C.; Brown, J.; McNeill, A.; Alwis, K.U.; Feng, J.; Wang, L.; West, R. Nicotine, Carcinogen, and Toxin Exposure in Long-Term E-Cigarette and Nicotine Replacement Therapy Users. Ann. Intern. Med. 2017, 166, 390. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; Stratton, K., Kwan, L.Y., Eaton, D.L., Eds.; The National Academies Press: Washington, DC, USA, 2018; ISBN 978-0-309-46831-2. [Google Scholar]
- Public Health England. Evidence Review of E-Cigarettes and Heated Tobacco Products 2018: Executive Summary; Public Health England: London, UK, 2018.
- McRobbie, H.; Bullen, C.; Hartmann-Boyce, J.; Hajek, P. Electronic cigarettes for smoking cessation and reduction. Cochrane Database Syst. Rev. 2014, CD010216. [Google Scholar]
- Wilson, N.; Hoek, J.; Thomson, G.; Edwards, R. Should e-cigarette use be included in indoor smoking bans? Bull. World Health Organ. 2017, 95, 540–541. [Google Scholar] [CrossRef] [PubMed]
- Hess, I.; Lachireddy, K.; Capon, A. A systematic review of the health risks from passive exposure to electronic cigarette vapour. Public Heal. Res. Pract. 2016. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Electronic Nicotine Delivery Systems and Electronic Non-Nicotine Delivery Systems (ENDS/ENNDS); World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Hartmann-Boyce, J.; McRobbie, H.; Bullen, C.; Begh, R.; Stead, L.F.; Hajek, P. Electronic cigarettes for smoking cessation. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Villanti, A.C.; Feirman, S.P.; Niaura, R.S.; Pearson, J.L.; Glasser, A.M.; Collins, L.K.; Abrams, D.B. How do we determine the impact of e-cigarettes on cigarette smoking cessation or reduction? Review and recommendations for answering the research question with scientific rigor. Addiction 2018, 113, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Beard, E.; West, R.; Michie, S.; Brown, J. Association between electronic cigarette use and changes in quit attempts, success of quit attempts, use of smoking cessation pharmacotherapy, and use of stop smoking services in England: time series analysis of population trends. BMJ 2016, 354, i4645. [Google Scholar] [CrossRef] [PubMed]
- Coleman, B.N.; Apelberg, B.J.; Ambrose, B.K.; Green, K.M.; Choiniere, C.J.; Bunnell, R.; King, B.A. Association Between Electronic Cigarette Use and Openness to Cigarette Smoking Among US Young Adults. Nicotine Tob. Res. 2015, 17, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Persoskie, A.; O’Brien, E.K.; Nguyen, A.B.; Tworek, C. Measuring youth beliefs about the harms of e-cigarettes and smokeless tobacco compared to cigarettes. Addict. Behav. 2017, 70, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, L.T.; Warner, K.E. Adolescents and e-cigarettes: Objects of concern may appear larger than they are. Drug Alcohol Depend. 2017, 174, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Gallus, S.; Lugo, A.; La Vecchia, C.; Boffetta, P.; Chaloupka, F.J.; Colombo, P.; Currie, L.; Fernandez, E.; Fischbacher, C.; Gilmore, A.; et al. Pricing Policies And Control of Tobacco in Europe (PPACTE) project. Eur. J. Cancer Prev. 2014, 23, 177–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahab, L.; West, R. Public support in England for a total ban on the sale of tobacco products. Tob. Control 2010, 19, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Gardner, B.; West, R. Public support in England for raising the price of cigarettes to fund tobacco control activities. Tob. Control 2010, 19, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Kowitt, S.D.; Noar, S.M.; Ranney, L.M.; Goldstein, A.O.; Bach, L.; Brewer, N.; Holder-Hayes, E.; Day, H. Public attitudes toward larger cigarette pack warnings: Results from a nationally representative U.S. sample. PLoS One 2017, 12, e0171496. [Google Scholar] [CrossRef] [PubMed]
- Deutsches Krebsforschungszentrum (DKFZ). Nichtraucherschutz in Nordrhein-Westfalen: Akzeptanz in der Bevölkerung und Auswirkungen auf die Gastronomie [Protection from Second-Hand Smoke Exposure in Northrhine-Westphalia: Public Support and Effects on Gastronomy]; Deutsches Krebsforschungszentrum (DKFZ): Heidelberg, Germany, 2017. [Google Scholar]
- Schaller, K.; Braun, S.; Pötschke-Langer, M. Erfolgsgeschichte Nichtraucherschutz in Deutschland: Steigende Unterstützung in der Bevölkerung für gesetzliche Maßnahmen (Success story protection from second-hand smoke exposure in Germany: Increased public support for legislative measures). Gesundheitsmonitor Newsl. 2014, 4, 1–9. [Google Scholar]
- Kastaun, S.; Brown, J.; Brose, L.S.; Ratschen, E.; Raupach, T.; Nowak, D.; Cholmakow-Bodechtel, C.; Shahab, L.; West, R.; Kotz, D. Study protocol of the German Study on Tobacco Use (DEBRA): A national household survey of smoking behaviour and cessation. BMC Public Health 2017, 17, 378. [Google Scholar] [CrossRef] [PubMed]
- Kotz, D.; Brown, J.; West, R. Predictive validity of the Motivation To Stop Scale (MTSS): A single-item measure of motivation to stop smoking. Drug Alcohol Depend. 2013, 128, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Hitchman, S.C.; Fong, G.T.; Zanna, M.P.; Hyland, A.; Bansal-Travers, M. Support and correlates of support for banning smoking in cars with children: Findings from the ITC Four Country Survey. Eur. J. Public Health 2011, 21, 360–365. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Special Eurobarometer 458: Attitudes of Europeans towards Tobacco and Electronic Cigarettes; European Commission: Brussels, Belgium, 2017. [Google Scholar]
- European Commission. Special Eurobarometer 385: Attitudes of Europeans towards tobacco; European Commission: Brussels, Belgium, 2012. [Google Scholar]
- Patterson, C.; Semple, S.; Wood, K.; Duffy, S.; Hilton, S. A quantitative content analysis of UK newsprint coverage of proposed legislation to prohibit smoking in private vehicles carrying children. BMC Public Health 2015, 15, 760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippidis, F.T.; Agaku, I.T.; Vardavas, C.I.; Majeed, A. The association between economic recession and public support for increased tobacco taxation in 27 European countries. Scand. J. Public Health 2014, 42, 589–592. [Google Scholar] [CrossRef] [PubMed]
- Sureda, X.; Fernandez, E.; Martinez-Sanchez, J.M.; Fu, M.; Lopez, M.J.; Martinez, C.; Salto, E. Secondhand smoke in outdoor settings: Smokers’ consumption, non-smokers’ perceptions, and attitudes towards smoke-free legislation in Spain. BMJ Open 2015, 5, e007554. [Google Scholar] [CrossRef] [PubMed]
- Lykke, M.; Pisinger, C.; Glümer, C. Ready for a goodbye to tobacco?—Assessment of support for endgame strategies on smoking among adults in a Danish regional health survey. Prev. Med. (Baltim). 2016, 83, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Filippidis, F.T.; Girvalaki, C.; Mechili, E.-A.; Vardavas, C.I. Are political views related to smoking and support for tobacco control policies? A survey across 28 European countries. Tob. Induc. Dis. 2017, 15, 45. [Google Scholar] [CrossRef] [PubMed]
- Currie, L.M.; Blackman, K.; Clancy, L.; Levy, D.T. The effect of tobacco control policies on smoking prevalence and smoking-attributable deaths in Ireland using the IrelandSS simulation model. Tob. Control 2013, 22, e25–e32. [Google Scholar] [CrossRef] [PubMed]
- White, V.M.; Durkin, S.J.; Coomber, K.; Wakefield, M.A. What is the role of tobacco control advertising intensity and duration in reducing adolescent smoking prevalence? Findings from 16 years of tobacco control mass media advertising in Australia. Tob. Control 2015, 24, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Blackman, K.; Currie, L.M.; Mons, U. Germany SimSmoke: The Effect of Tobacco Control Policies on Future Smoking Prevalence and Smoking-Attributable Deaths in Germany. Nicotine Tob. Res. 2013, 15, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Department of Housing and Urban Development. Instituting Smoke-Free Public Housing: Final rule; Federal Register: Washington, DC, USA, 2016; Vol. 81, pp. 87430–87444.

{kind=link}
| Total Sample (n = 2062; 100%) | Current Smoker (n = 586; 28.4%) | Ex-Smoker (n = 369; 17.9%) | Never Smoker (n = 1107; 53.7%) | |
|---|---|---|---|---|
| Age, years (mean ± SD) | 51.8 ± 19.8 | 47.1 ± 17.2 | 58.4 ± 17.5 | 52.1 ± 21.1 |
| Sex | ||||
| Female | 1070 (51.9%) | 271 (46.2%) | 143 (38.8%) | 656 (59.3%) |
| Male | 992 (48.1%) | 315 (53.8%) | 226 (61.2%) | 451 (40.7%) |
| Education † | ||||
| High school equiv. | 479 (23.2%) | 110 (19.2%) | 85 (23.2%) | 284 (27.4%) |
| Adv. tech. college equiv. | 133 (6.5%) | 28 (4.9%) | 30 (8.2%) | 75 (7.2%) |
| Secondary school equiv. | 686 (33.3%) | 230 (40.1%) | 116 (31.7%) | 340 (32.8%) |
| Junior high school equiv. | 646 (31.3%) | 193 (33.6%) | 130 (35.5%) | 323 (31.1%) |
| No qualification | 33 (1.6%) | 13 (2.3%) | 5 (1.4%) | 15 (1.4.5%) |
| Household income | ||||
| >€5000/per month | 134 (6.5%) | 26 (4.4%) | 27 (7.3%) | 81 (7.3%) |
| €4000–5000/per month | 128 (6.2%) | 31 (5.3%) | 24 (6.5%) | 73 (6.6%) |
| €3000–4000/per month | 369 (17.9%) | 96 (16.4%) | 67 (18.2%) | 206 (18.6%) |
| €2000–3000/per month | 557 (27.0%) | 164 (28.0%) | 106 (28.7%) | 287 (25.9%) |
| €1000–2000/per month | 638 (30.9%) | 173 (29.5%) | 117 (31.7%) | 348 (31.4%) |
| <€1000/per month | 236 (11.4%) | 96 (16.4%) | 28 (7.6%) | 112 (10.1%) |
| Current Smokers Only (n = 586) | |
|---|---|
| Cigarettes smoked per day (mean ± SD) | 15.3 ± 9.0 |
| Made at least one quit attempt last year | 140 (23.9%) |
| Motivation to stop smoking (MRS) [43] | |
| Do not want to stop smoking | 268 (45.7%) |
| Should stop but do not really want to | 139 (23.7%) |
| Want to stop but have not thought about when | 52 (8.9%) |
| Want to stop but have not decided when | 51 (8.7%) |
| Really want to stop and hope to soon | 43 (7.3%) |
| Really want to stop and intend to in the next 3 months | 7 (1.2%) |
| Really want to stop and intend to in the next month | 6 (1.0%) |
| Banning Sale of Tobacco | Raising Legal Age of Sale from 18 to 21 | Taxing Tobacco Industry Sales, to Address Tobacco-Related Problems | Assessing Effectiveness and Safety of E-Cigarettes | Banning Smoking in Cars When Minors Are Present | |
|---|---|---|---|---|---|
| Smoking status | |||||
| Current smoker (ref.) | 1 | 1 | 1 | 1 | 1 |
| Ex-smoker | 3.48 (2.37–5.11) *** | 1.75 (1.31–2.36) *** | 3.48 (2.59–4.66) *** | 1.39 (1.04–1.85) * | 1.29 (0.95–1.74) |
| Never-smoker | 5.26 (3.80–7.28) *** | 2.73 (2.17–3.46) *** | 4.16 (3.30–5.24) *** | 1.50 (1.20) *** | 1.81 (1.42–2.31) *** |
| Age, 10-year units a | 0.98 (0.92–1.04) | 0.95 (0.89–1.00) * | 1.02 (0.96–1.08) * | 0.94 (0.89–0.99) * | 0.94 (0.89–1.00) * |
| Sex | |||||
| Female (reference) | 1 | 1 | 1 | 1 | 1 |
| Male | 0.83 (0.66–1.03) | 0.84 (0.69–1.02) | 0.81 (0.66–0.99) * | 0.88 (0.72–1.07) | 0.89 (0.72–1.10) |
| Education † | |||||
| High school equiv. (ref.) | 1 | 1 | 1 | 1 | 1 |
| Adv. tech. college equiv. | 1.59 (1.00–2.51) | 1.19 (0.79–1.801) | 0.86 (0.56–1.33) | 1.15 (0.75–1.75) | 1.28 (0.79–2.07) |
| Secondary school equiv. | 1.15 (0.85–1.56) | 1.14 (0.88–1.48) | 0.81 (0.62–1.07) | 0.79 (0.61–1.02) | 0.97 (0.73–1.29) |
| Junior high school equiv. | 1.31 (0.94–1.83) | 1.31 (0.99–1.74) | 0.65 (0.49–0.88) ** | 0.80 (0.60–1.06) | 1.10 (0.81–1.51) |
| No qualification | 0.89 (0.33–2.39) | 2.00 (0.91–4.40) | 0.99 (0.42–2.32) | 0.37 (0.16–0.85) * | 0.86 (0.37–2.00) |
| Household income | |||||
| €>5000/per month (ref.) | 1 | 1 | 1 | 1 | 1 |
| €4000–5000/per month | 1.13 (0.62–2.05) | 1.08 (0.64–1.82) | 0.68 (0.39–1.19) | 1.18 (0.71–1.97) | 0.78 (0.43–1.42) |
| €3000–4000/per month | 0.81 (0.49–1.35) | 1.10 (0.71–1.69) | 0.72 (0.45–1.16) | 1.13 (0.74–1.73) | 0.75 (0.45–1.23) |
| €2000–3000/per month | 1.14 (0.71–1.83) | 1.11 (0.73–1.68) | 0.56 (0.35–0.87) ** | 1.31 (0.87–1.97) | 0.71 (0.44–1.15) |
| €1000–2000/per month | 1.28 (0.80–2.07) | 1.25 (0.83–1.90) | 0.77 (0.49–1.21) | 1.63 (1.08–2.47) * | 0.75 (0.47–1.22) |
| <€1000/per month | 1.48 (0.86–2.53) | 1.56 (0.98–2.50) | 0.86 (0.52–1.43) | 1.65 (1.03–2.65) * | 1.15 (0.66–2.01) |
| Banning Sale of Tobacco | Raising Legal Age of Sale from 18 to 21 | Taxing Tobacco Industry Sales | Assessing Effectiveness and Safety of E-Cigarettes | Banning Smoking in Cars When Minors Are Present | |
|---|---|---|---|---|---|
| Cigarettes smoked/day, number a | 0.99 (0.95–1.03) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) | 1.00 (1.00–1.00) |
| Quit attempt last year (yes/no) | |||||
| Yes, attempt to quit (reference) | 1 | 1 | 1 | 1 | 1 |
| No, attempt to quit | 0.20 (0.10–0.40) *** | 0.94 (0.59–1.50) | 0.71 (0.45–1.11) | 1.07 (0.69–1.65) | 0.96 (0.61–1.52) |
| Motivation to stop smoking (MRS) b | 1.06 (0.95–1.18) | 1.11 (1.02–1.20) * | 1.00 (0.92–1.08) | 1.01 (0.93–1.10) | 1.02 (0.94–1.12) |
| Age, 10-year units a | 0.89 (0.73–1.10) | 0.85 (0.75–0.96) ** | 0.92 (0.82–1.04) | 0.98 (0.87–1.09) | 1.01 (0.90–1.14) |
| Sex | |||||
| Female (ref.) | 1 | 1 | 1 | 1 | 1 |
| Male | 0.58 (0.28–1.17) | 0.84 (0.56–1.28) | 0.93 (0.62–1.39) | 0.76 (0.52–1.11) | 0.56 (0.37–0.84) ** |
| Education † | |||||
| High school equiv. (ref.) | 1 | 1 | 1 | 1 | 1 |
| Advanced technical college equiv. | 0.60 (0.07–5.36) | 1.95 (0.69–5.52) | 0.61 (0.21–1.76) | 1.62 (0.52–5.02) | 1.33 (0.43–4.15) |
| Secondary school equiv. | 0.50 (0.19–1.35) | 1.11 (0.60–2.05) | 0.63 (0.37–1.09) | 0.67 (0.39–1.15) | 1.14 (0.65–2.00) |
| Junior high school equiv. | 1.05 (0.39–2.80) | 1.79 (0.95–3.36) | 0.50 (0.28–0.89) * | 0.63 (0.35–1.11) | 1.44 (0.79–2.62) |
| No qualification | 2.97 (0.45–19.82) | 4.82 (1.31–17.79) * | 0.73 (0.19–2.79) | 0.47 (0.13–1.71) | 1.88 (0.45–7.86) |
| Household income | |||||
| €>5000/per month (ref.) | 1 | 1 | 1 | 1 | 1 |
| €4000–5000/per month | 1.37 (0.19–10.12) | 0.97 (0.23–4.01) | 0.22 (0.07–0.88) * | 0.48 (0.14–1.69) | 0.84 (0.19–3.81) |
| €3000–4000/per month | 0.78 (0.14–4.40) | 1.23 (0.41–3.72) | 0.71 (0.25–1.98) | 0.77 (0.28–2.11) | 0.70 (0.21–2.39) |
| €2000–3000/per month | 0.46 (0.09–2.53) | 0.84 (0.29–2.50) | 0.31 (0.11–0.85) * | 0.92 (0.35–2.45) | 0.48 (0.15–1.55) |
| €1000–2000/per month | 0.57 (0.11–3.10) | 1.22 (0.42–3.56) | 0.47 (0.17–1.26) | 1.30 (0.49–3.47) | 0.44 (0.14–1.43) |
| <€1000/per month | 0.53 (0.09–3.14) | 1.17 (0.39–3.57) | 0.34 (0.12–0.97) * | 0.80 (0.29–2.20) | 0.59 (0.17–1.98) |
| Banning Sale of Tobacco | Raising Legal Age of Sale from 18 to 21 | Taxing Tobacco Industry Sales | Assessing Effectiveness and Safety of E-Cigarettes | Banning Smoking in Cars When Minors Are Present | |
|---|---|---|---|---|---|
| Age, 10-year units a | 0.98 (0.92–1.05) | 0.97 (0.91–1.03) | 1.04 (0.98–1.12) | 0.93 (0.87–0.99) * | 0.92 (0.85–0.98) * |
| Sex | |||||
| Female (ref.) | 1 | 1 | 1 | 1 | 1 |
| Male | 0.83 (0.65–1.10) | 0.82 (0.66–1.02) | 0.79 (0.62–1.00) | 0.95 (0.75–1.20) | 1.02 (0.79–1.31) |
| Education † | |||||
| High school equiv. (ref.) | 1 | 1 | 1 | 1 | 1 |
| Advanced technical college equiv. | 1.55 (0.95–2.53) | 1.14 (0.72–1.81) | 0.93 (0.56–1.53) | 1.13 (0.70–1.84) | 1.30 (0.74–2.29) |
| Secondary school equiv. | 1.20 (0.86–1.66) | 1.20 (0.88–1.60) | 0.82 (0.59–1.13) | 0.84 (0.61–1.14) | 0.90 (0.64–1.27) |
| Junior high school equiv. | 1.25 (0.87–1.79) | 1.21 (0.87–1.68) | 0.66 (0.46–0.94) * | 0.87 (0.61–1.23) | 0.97 (0.66–1.42) |
| No qualification | 0.61 (0.19–1.98) | 1.18 (0.43–3.25) | 0.84 (0.26–2.74) | 0.20 (0.10–0.68) * | 0.64 (0.21–1.96) |
| Household income | |||||
| €>5000/per month (ref.) | 1 | 1 | 1 | 1 | 1 |
| €4000–5000/per month | 1.00 (0.53–1.88) | 1.16 (0.65–2.07) | 0.88 (0.46–1.69) | 1.44 (0.80–2.61) | 0.81 (0.41–1.60) |
| €3000–4000/per month | 0.72 (0.42–1.23) | 1.00 (0.61–1.57) | 0.66 (0.39–1.12) | 1.24 (0.77–2.01) | 0.75 (0.43–1.31) |
| €2000–3000/per month | 1.17 (0.71–1.93) | 1.15 (0.72–1.82) | 0.62 (0.37–1.04) | 1.35 (0.85–2.16) | 0.82 (0.48–1.41) |
| €1000–2000/per month | 1.34 (0.82–2.21) | 1.23 (0.77–1.94) | 0.84 (0.50–1.41) | 1.60 (1.00–2.56) | 0.96 (0.56–1.67) |
| <€1000/per month | 1.64 (0.91–2.94) | 1.84 (1.10–3.18) | 1.23 (0.65–2.33) | 2.38 (1.31–4.32) ** | 1.76 (0.86–3.60) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boeckmann, M.; Kotz, D.; Shahab, L.; Brown, J.; Kastaun, S. German Public Support for Tobacco Control Policy Measures: Results from the German Study on Tobacco Use (DEBRA), a Representative National Survey. Int. J. Environ. Res. Public Health 2018, 15, 696. https://doi.org/10.3390/ijerph15040696
Boeckmann M, Kotz D, Shahab L, Brown J, Kastaun S. German Public Support for Tobacco Control Policy Measures: Results from the German Study on Tobacco Use (DEBRA), a Representative National Survey. International Journal of Environmental Research and Public Health. 2018; 15(4):696. https://doi.org/10.3390/ijerph15040696
Chicago/Turabian StyleBoeckmann, Melanie, Daniel Kotz, Lion Shahab, Jamie Brown, and Sabrina Kastaun. 2018. "German Public Support for Tobacco Control Policy Measures: Results from the German Study on Tobacco Use (DEBRA), a Representative National Survey" International Journal of Environmental Research and Public Health 15, no. 4: 696. https://doi.org/10.3390/ijerph15040696