Projection of Future Mortality Due to Temperature and Population Changes under Representative Concentration Pathways and Shared Socioeconomic Pathways


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Estimation of Temperature Increases above Pre-industrial Levels
2.3. Association between Temperature and Mortality
2.4. Temperature-Related Mortality Projection
3. Results
3.1. Maximum Temperature Increases and Population Changes
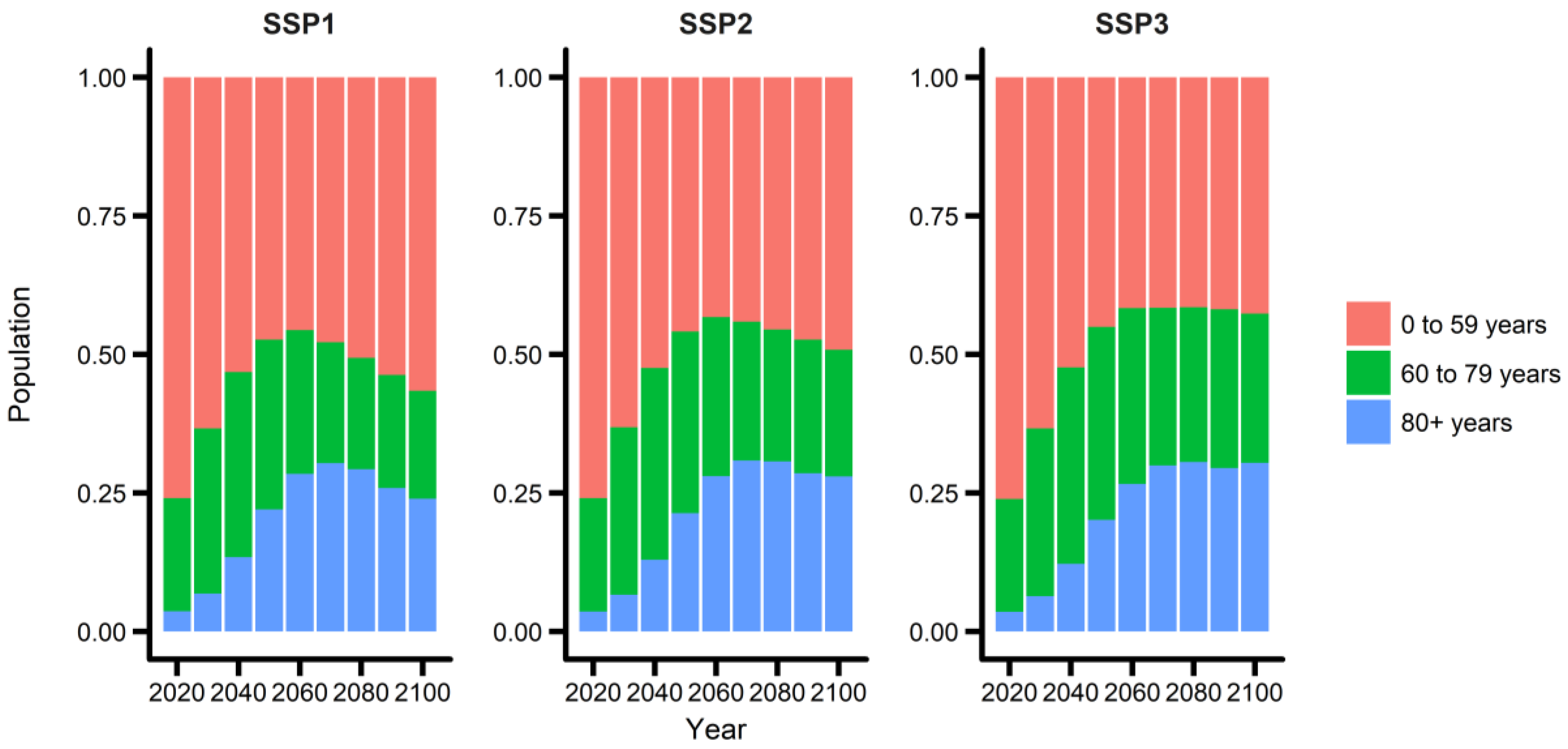
3.2. Population Changes
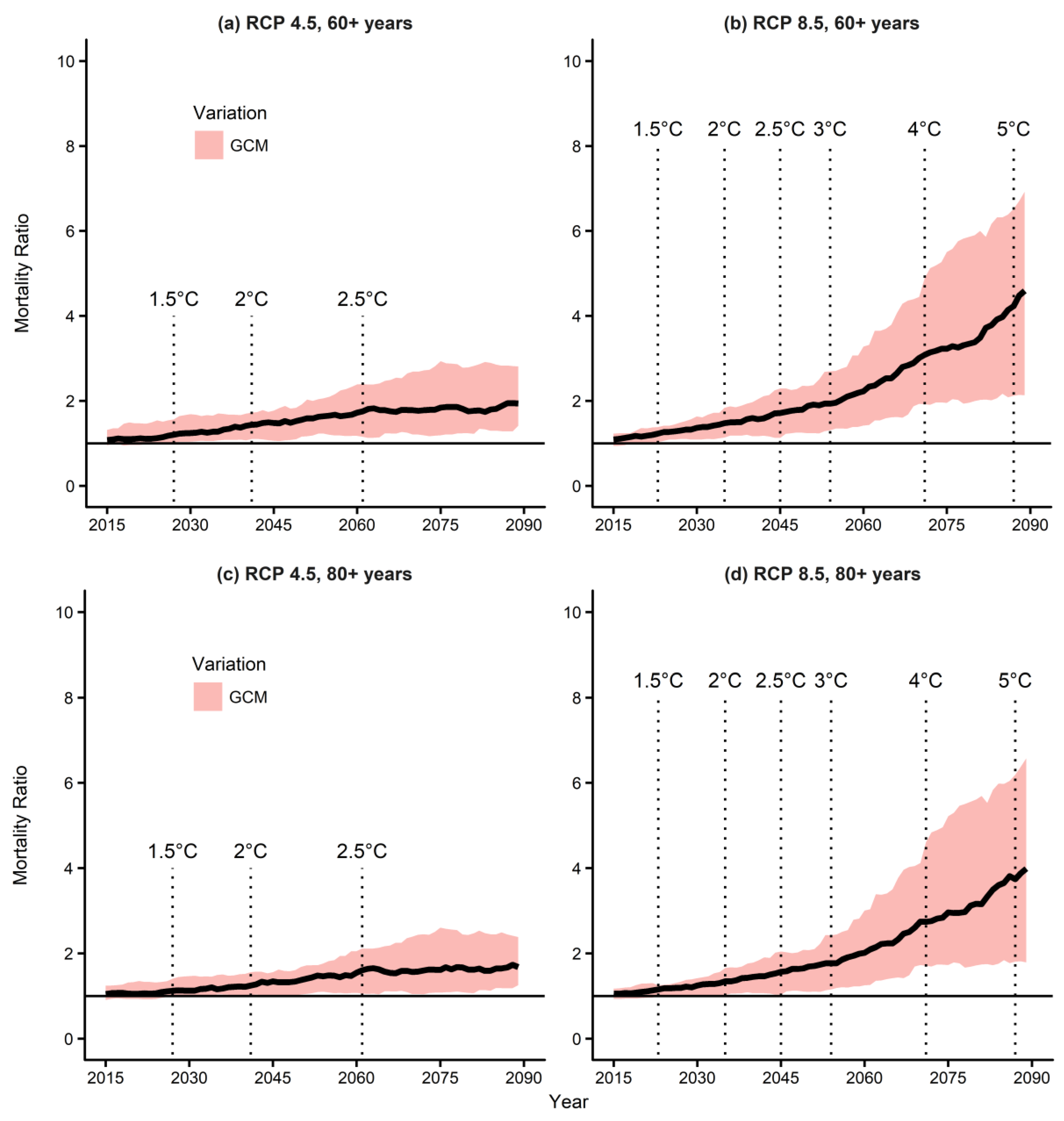
3.3. Mortality Prediction Due to Temperature Changes
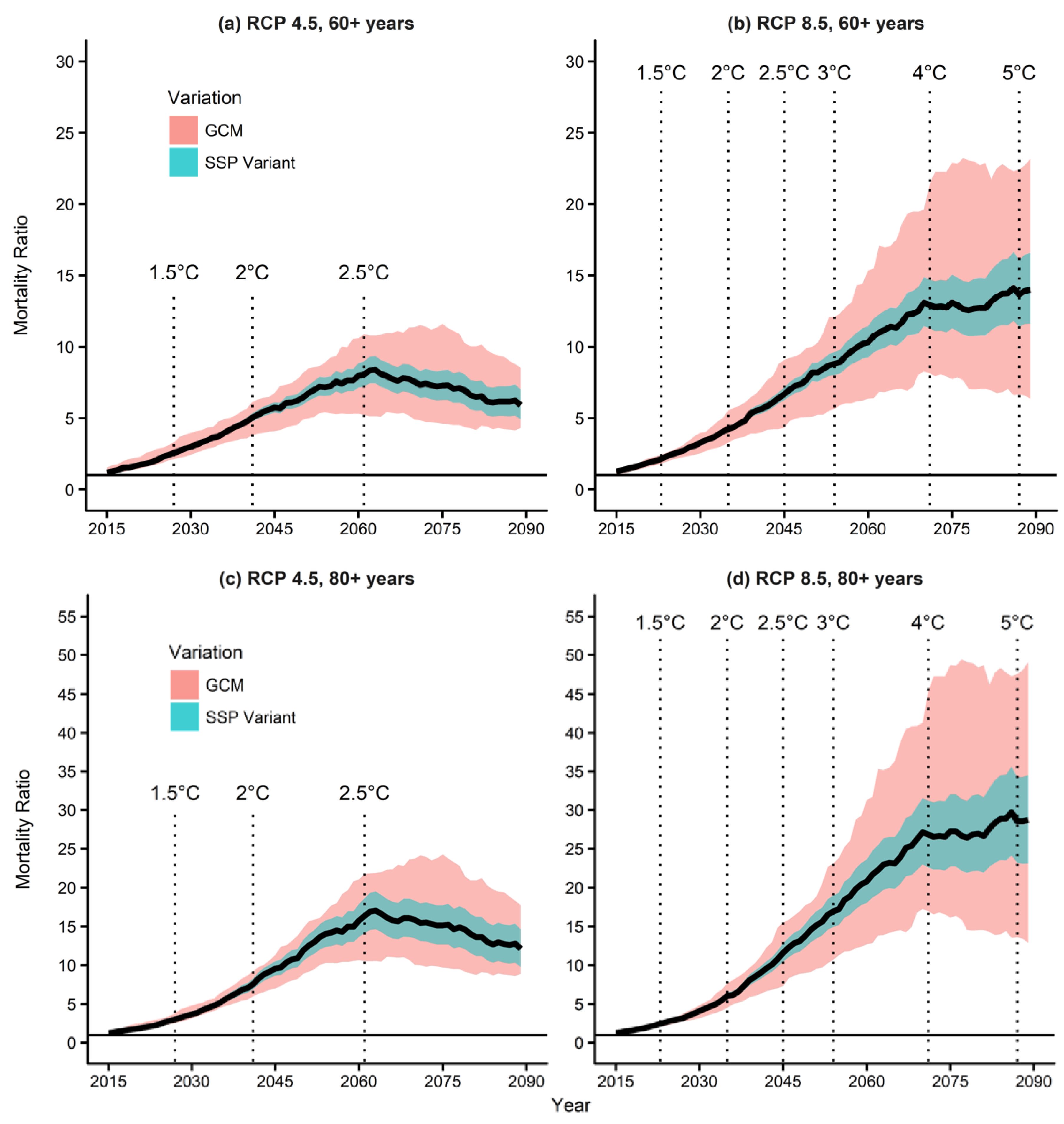
3.4. Mortality Prediction Due to Temperature and Population Changes
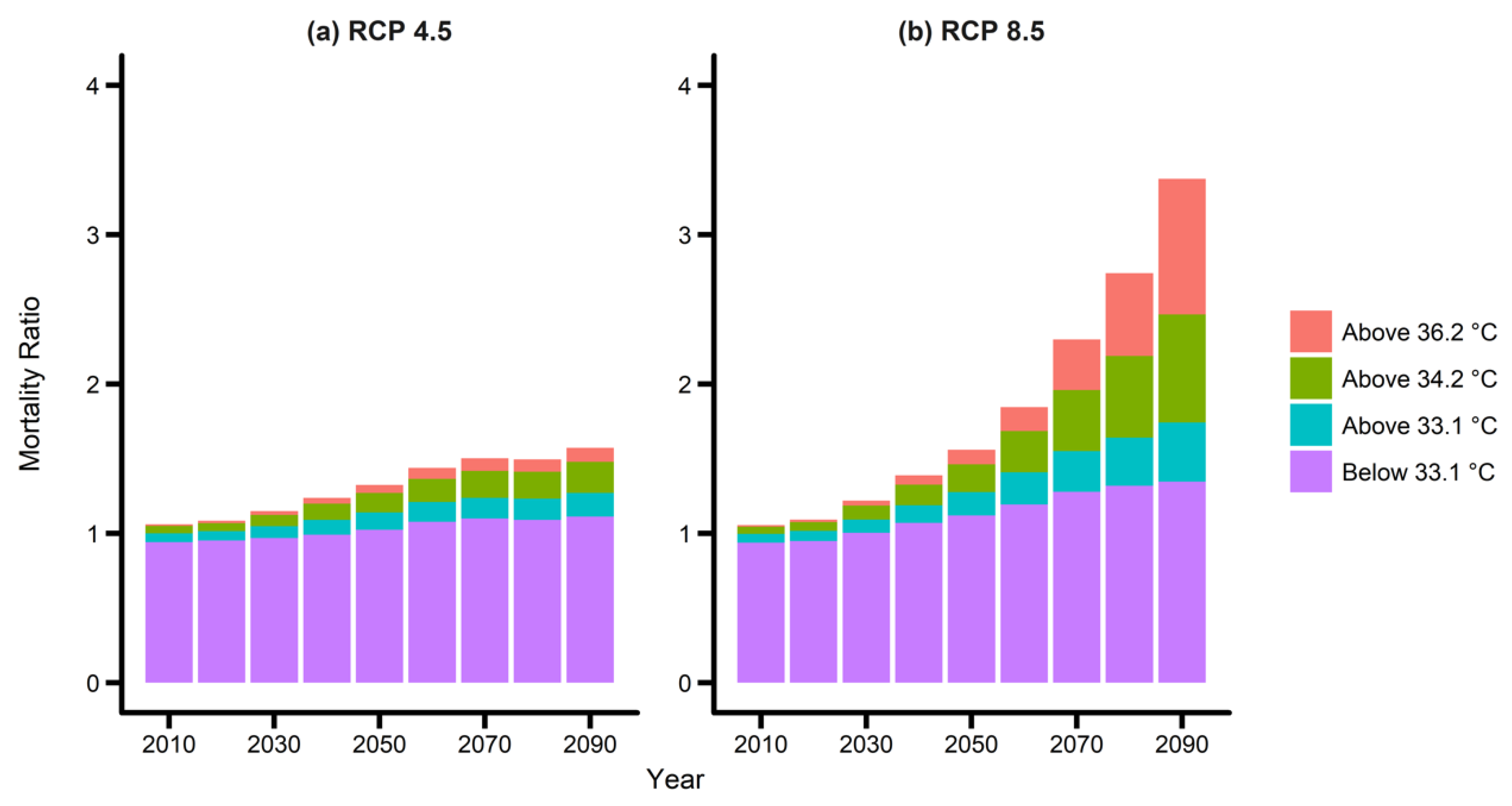
3.5. Mortality Prediction Due to Extreme Temperature Changes
4. Discussion
4.1. Impact of Global Temperature Increases by 1.5 °C and 2 °C on Mortality
4.2. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hayhoe, K.; Sheridan, S.; Kalkstein, L.; Greene, S. Climate change, heat waves, and mortality projections for Chicago. J. Gt. Lakes Res. 2010, 36, 65–73. [Google Scholar] [CrossRef]
- Åström, D.O.; Forsberg, B.; Ebi, K.L.; Rocklöv, J. Attributing mortality from extreme temperatures to climate change in Stockholm, Sweden. Nat. Clim. Chang. 2013, 3, 1050. [Google Scholar] [CrossRef]
- Bobb, J.F.; Peng, R.D.; Bell, M.L.; Dominici, F. Heat-related mortality and adaptation to heat in the United States. Environ. Health Perspectives 2014, 122, 811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, C. (Ed.) Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation. Special Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: New York, NY, USA, 2012. [Google Scholar]
- Zuo, J.; Pullen, S.; Palmer, J.; Bennetts, H.; Chileshe, N.; Ma, T. Impacts of heat waves and corresponding measures: A review. J. Clean. Prod. 2015, 92, 1–12. [Google Scholar] [CrossRef]
- Petkova, E.P.; Horton, R.M.; Bader, D.A.; Kinney, P.L. Projected heat-related mortality in the US urban northeast. Int. J. Environ. Res. Public Health 2013, 10, 6734–6747. [Google Scholar] [CrossRef] [PubMed]
- Hajat, S.; Vardoulakis, S.; Heaviside, C.; Eggen, B. Climate change effects on human health: Projections of temperature-related mortality for the UK during the 2020s, 2050s and 2080s. J. Epid. Commun. Health 2014, 68, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Honda, Y.; Kondo, M.; McGregor, G.; Kim, H.; Guo, Y.L.; Hijioka, Y.; Yoshikawa, M.; Oka, K.; Takano, S.; Hales, S.; et al. Heat-related mortality risk model for climate change impact projection. Environ. Health Prev. Med. 2014, 19, 56. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Sinclair, V.A.; Räisänen, J.; Ruuhela, R. Heat waves in Finland: Present and projected summertime extreme temperatures and their associated circulation patterns. Int. J. Climatol. 2018, 38, 1393–1408. [Google Scholar] [CrossRef]
- Shaposhnikov, D.; Revich, B. Climate Change and Projections of Temperature-Related Mortality, in Climate Change and Air Pollution. Springer 2018. [Google Scholar] [CrossRef]
- Karmalkar, A.V.; Bradley, R.S. Consequences of global warming of 1.5 C and 2 C for regional temperature and precipitation changes in the contiguous United States. PLoS ONE 2017, 12, e0168697. [Google Scholar] [CrossRef] [PubMed]
- Lehner, F.; Coats, S.; Stocker, T.F.; Pendergrass, A.G.; Sanderson, B.M.; Raible, C.C.; Smerdon, J.E. Projected drought risk in 1.5 C and 2 C warmer climates. Geophys. Res. Lett. 2017, 44, 7419–7428. [Google Scholar] [CrossRef]
- Wang, Z.; Lin, L.; Zhang, X.; Zhang, H.; Liu, L.; Xu, Y. Scenario dependence of future changes in climate extremes under 1.5 C and 2 C global warming. Sci. Rep. 2017, 7, 46432. [Google Scholar]
- Baiquan, Z.; Zhai, P.; Chen, Y.; Yu, R. Projected changes of thermal growing season over Northern Eurasia in a 1.5 °C and 2 °C warming world. Environ. Res. Lett. 2018, 13, 3. [Google Scholar]
- Wewerinke-Singh, M.; Doebbler, C. The Paris agreement: Some critical reflections on process and substance. UNSWLJ 2016, 39, 486. [Google Scholar]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- United Nations (UN). World Population Ageing 2015 Prepared by Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat; United Nations (UN): New York, NY, USA, 2006. [Google Scholar]





© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.Y.; Kim, E.; Lee, W.-S.; Chae, Y.; Kim, H. Projection of Future Mortality Due to Temperature and Population Changes under Representative Concentration Pathways and Shared Socioeconomic Pathways. Int. J. Environ. Res. Public Health 2018, 15, 822. https://doi.org/10.3390/ijerph15040822
Lee JY, Kim E, Lee W-S, Chae Y, Kim H. Projection of Future Mortality Due to Temperature and Population Changes under Representative Concentration Pathways and Shared Socioeconomic Pathways. International Journal of Environmental Research and Public Health. 2018; 15(4):822. https://doi.org/10.3390/ijerph15040822
Chicago/Turabian StyleLee, Jae Young, Ejin Kim, Woo-Seop Lee, Yeora Chae, and Ho Kim. 2018. "Projection of Future Mortality Due to Temperature and Population Changes under Representative Concentration Pathways and Shared Socioeconomic Pathways" International Journal of Environmental Research and Public Health 15, no. 4: 822. https://doi.org/10.3390/ijerph15040822