Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China


Abstract
:1. Introduction
2. Materials and Methods
2.1. PM2.5 Concentration and Socio-Economic Data
2.2. Health Impact Assessment
2.3. Economic Loss Evaluation
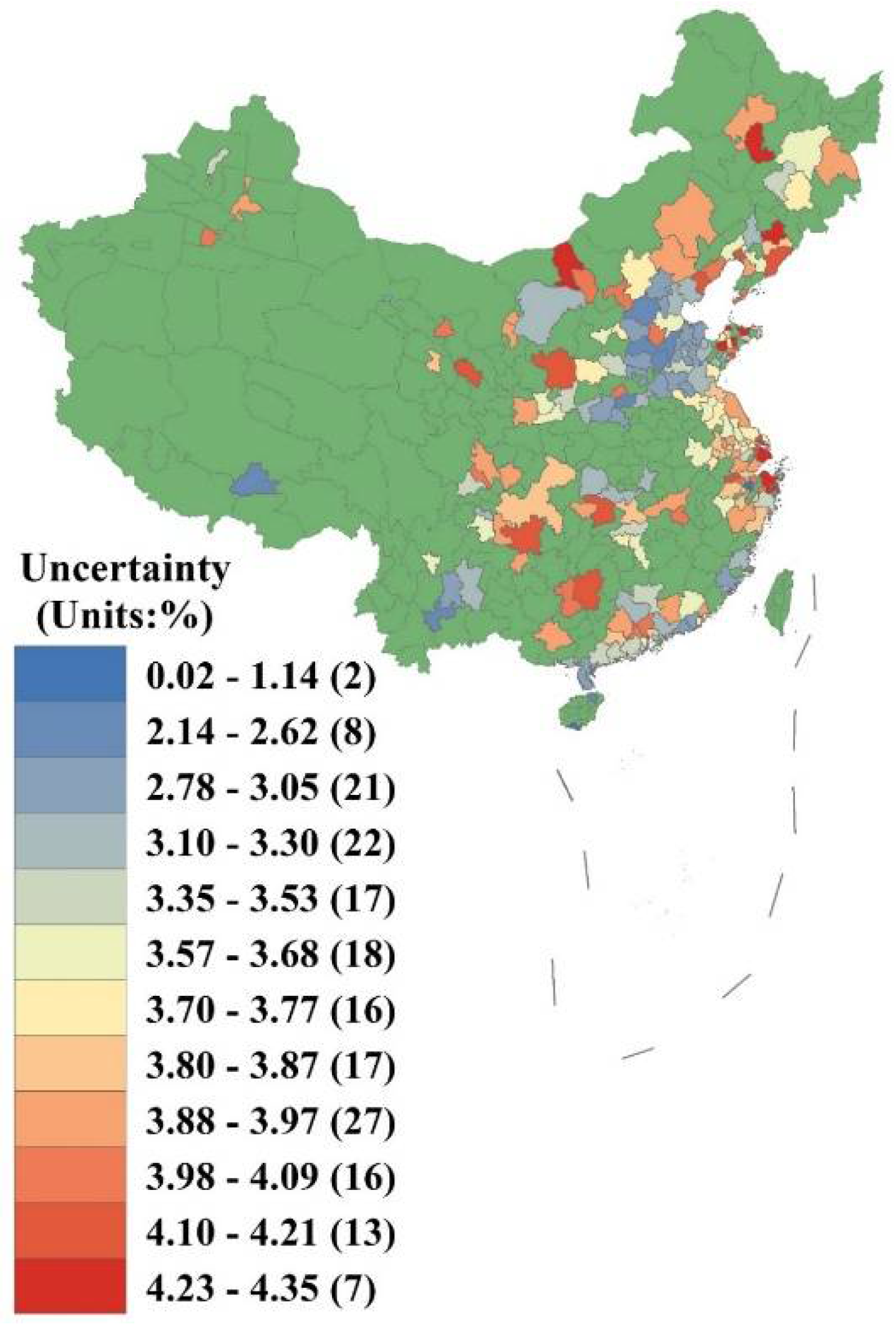
2.4. Uncertainty Analysis
3. Results
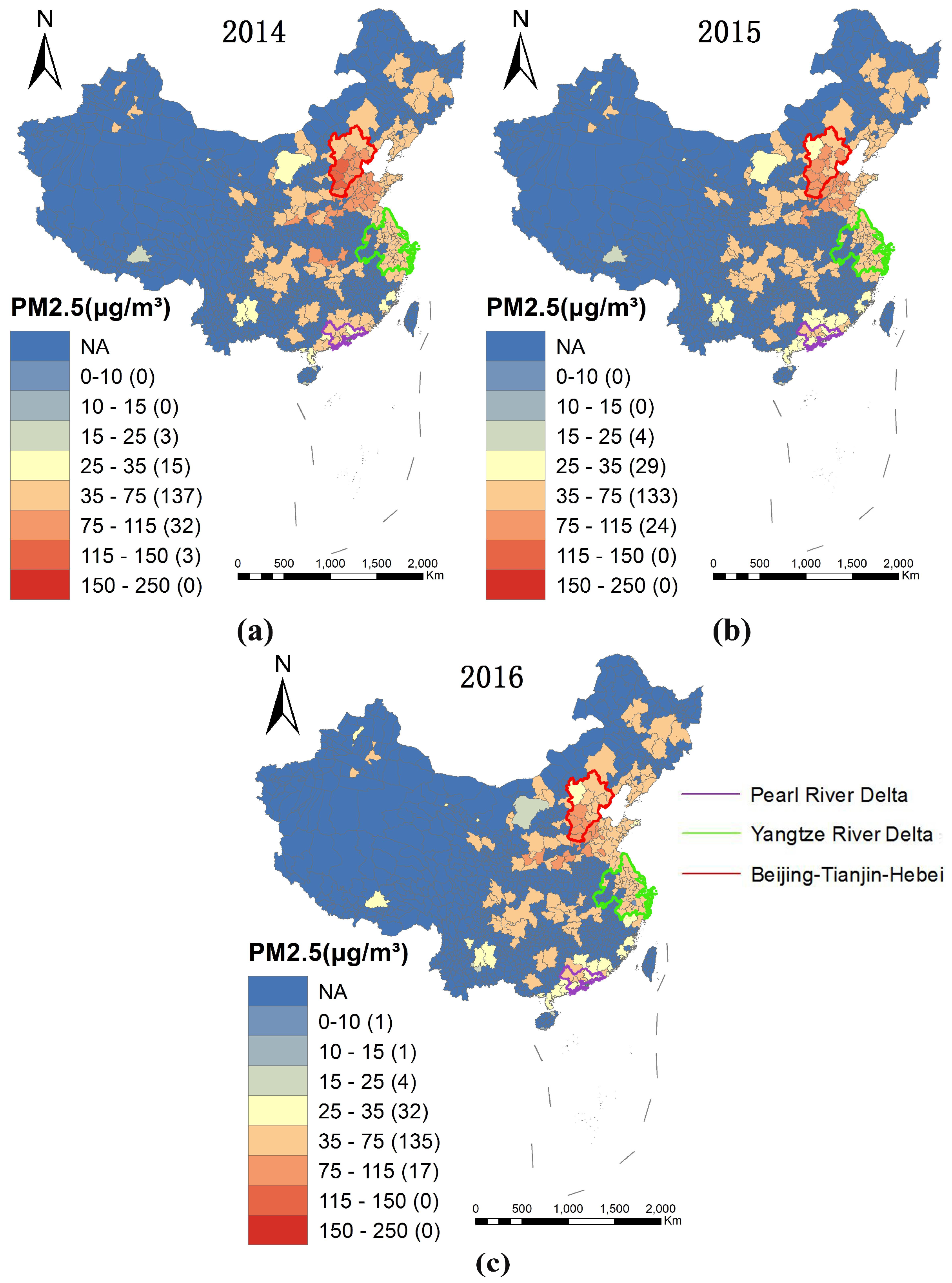
3.1. Spatial Distribution of PM2.5
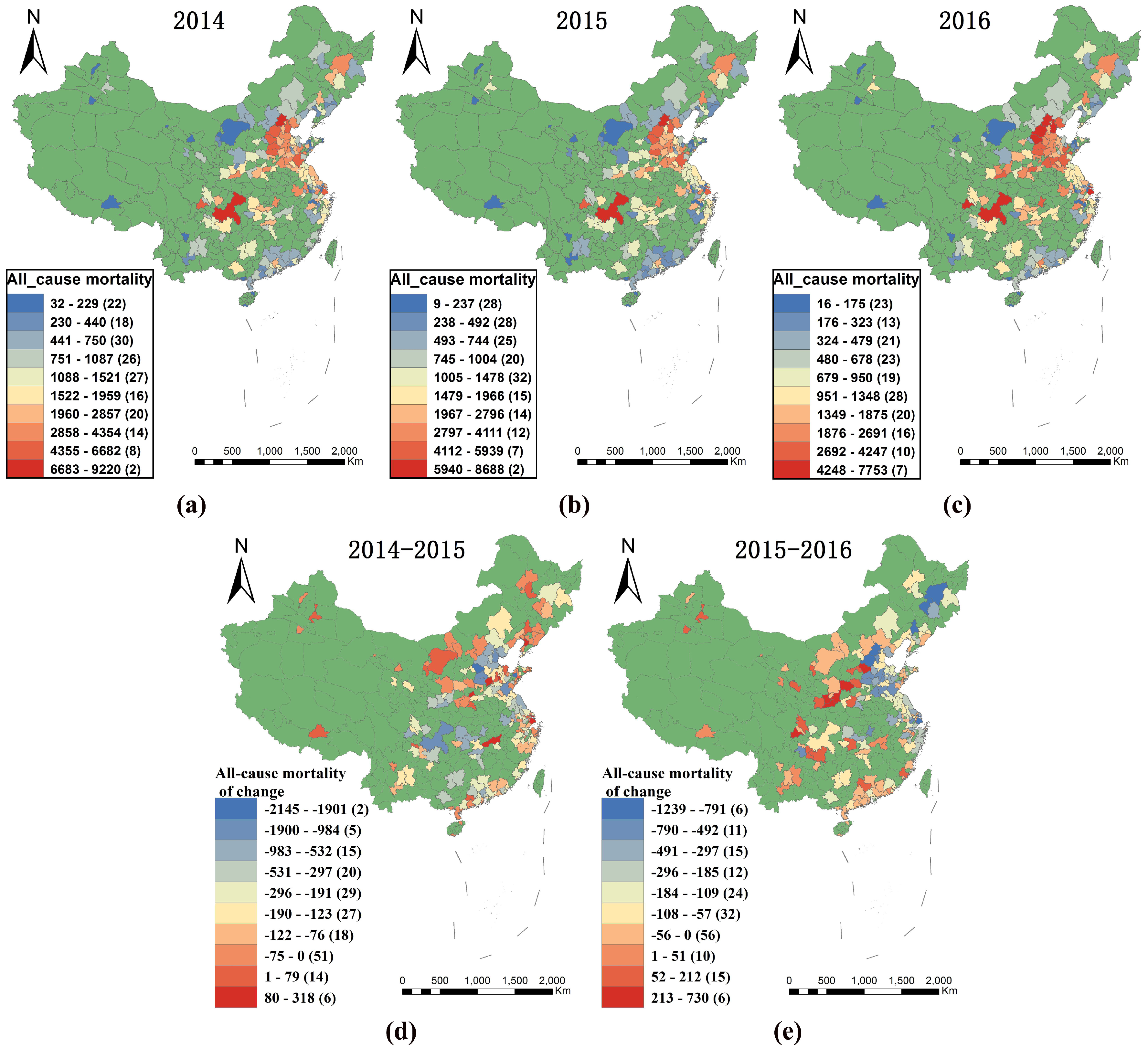
3.2. PM2.5 Health Impact
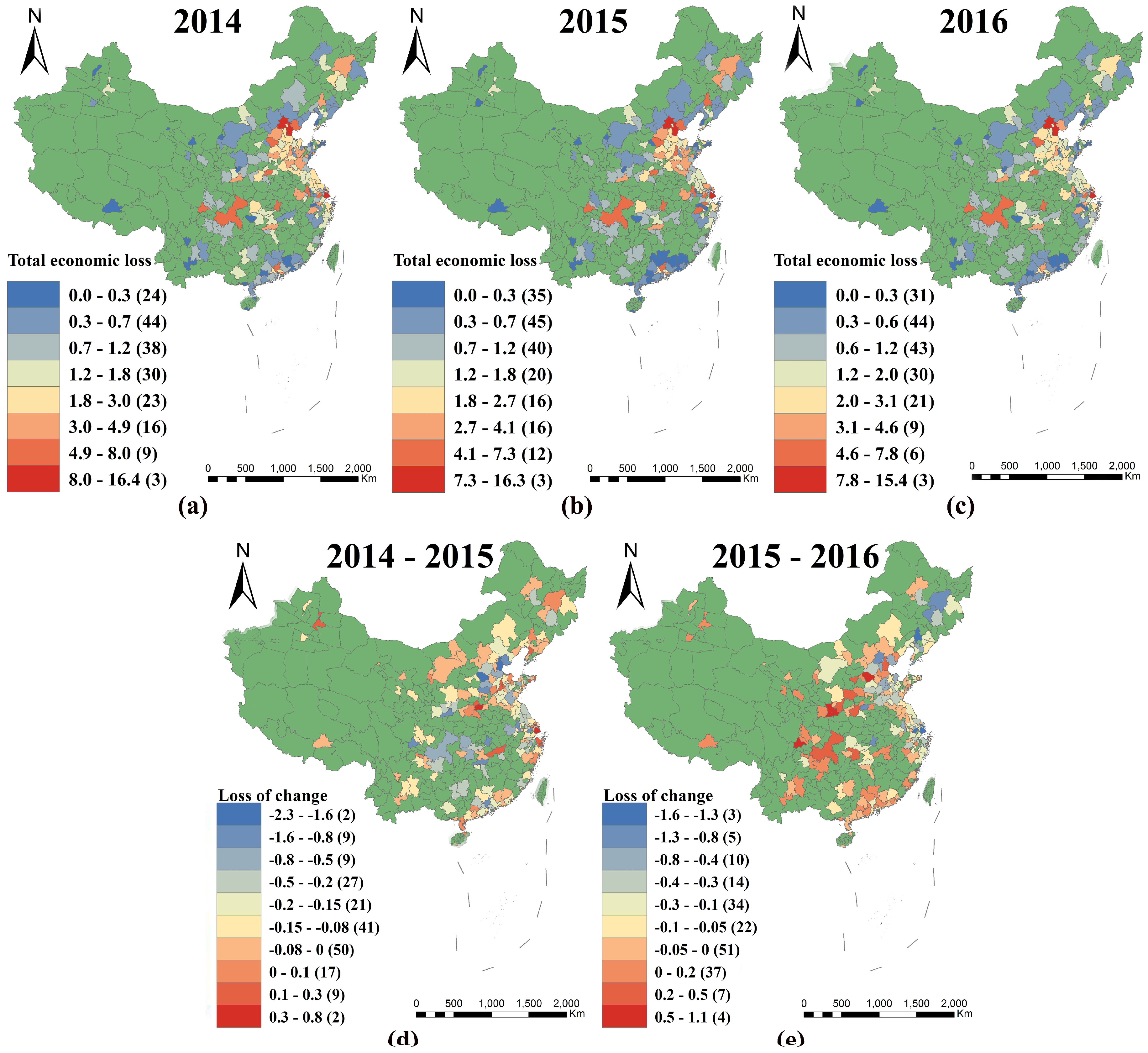
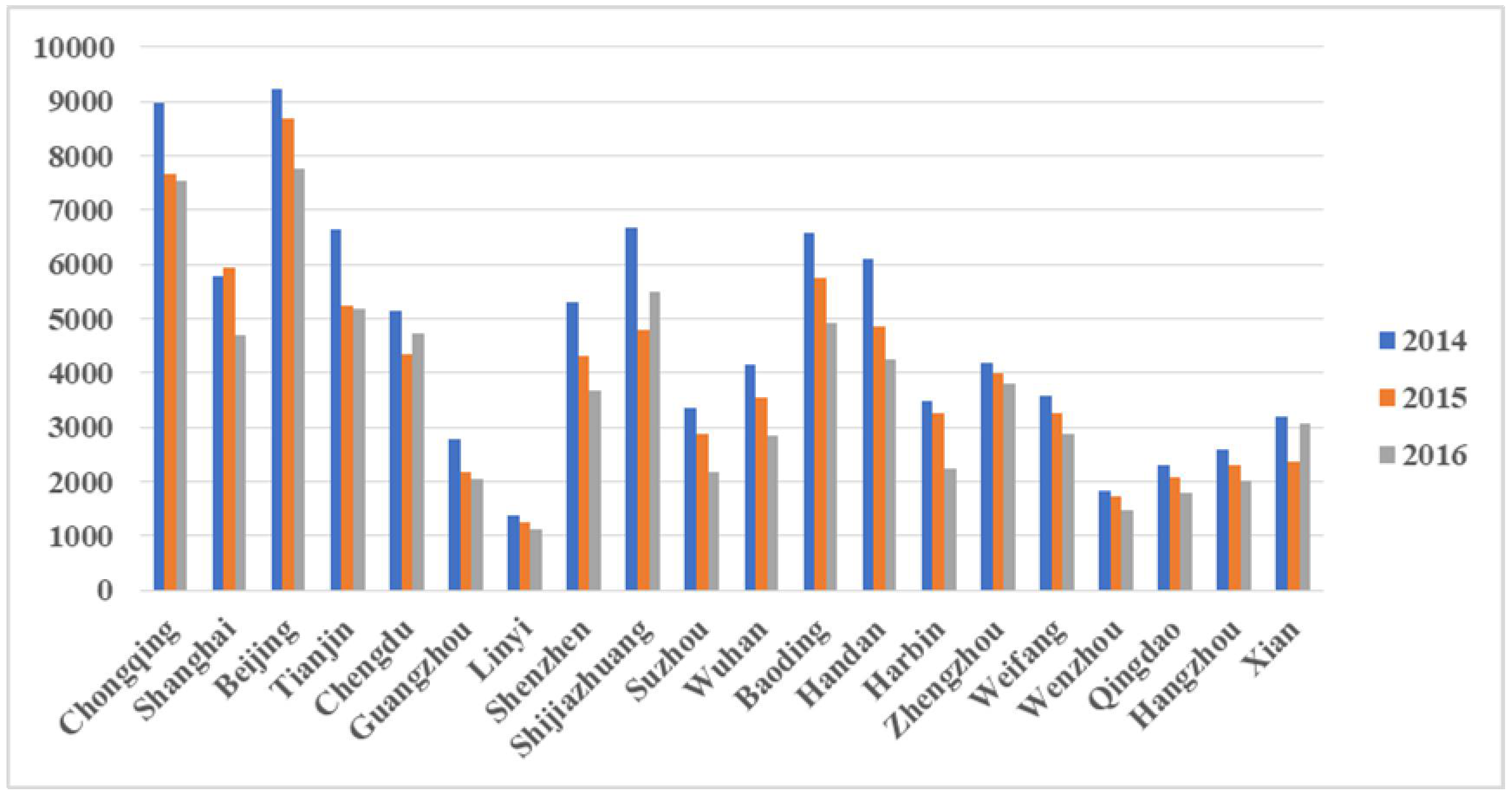
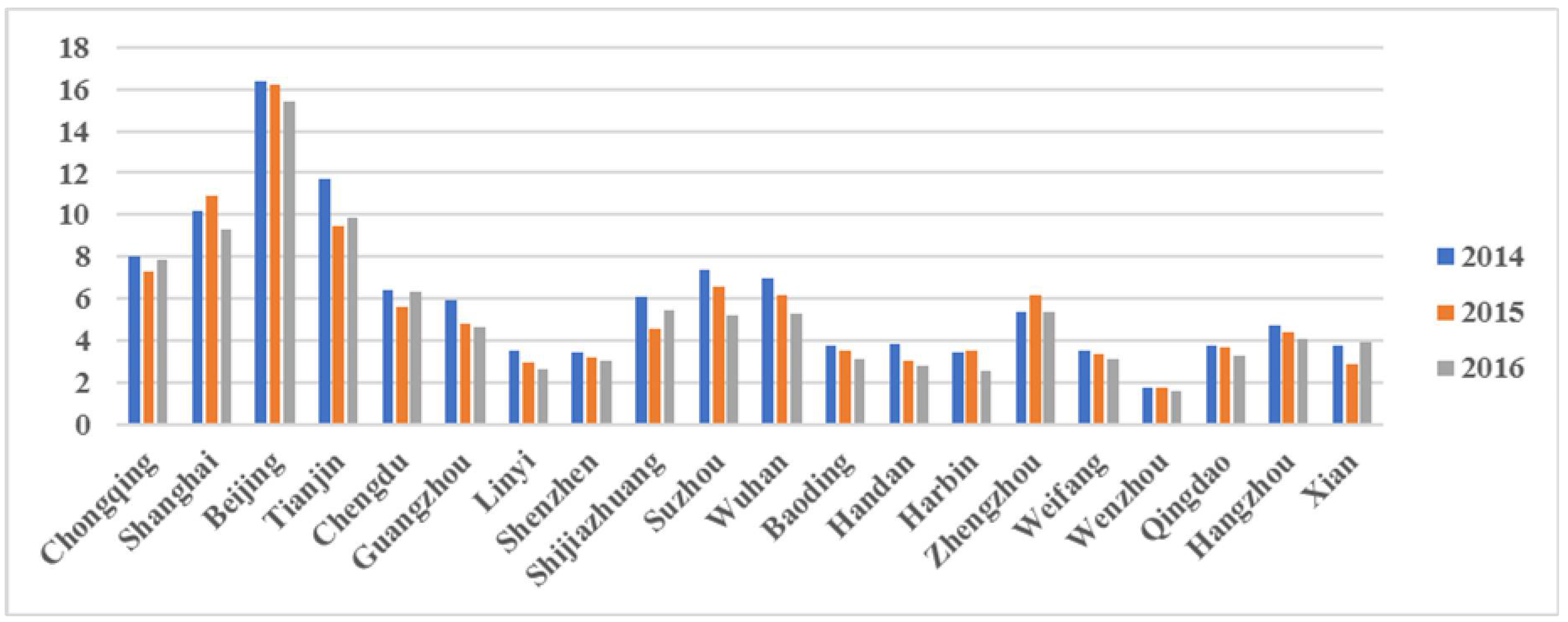
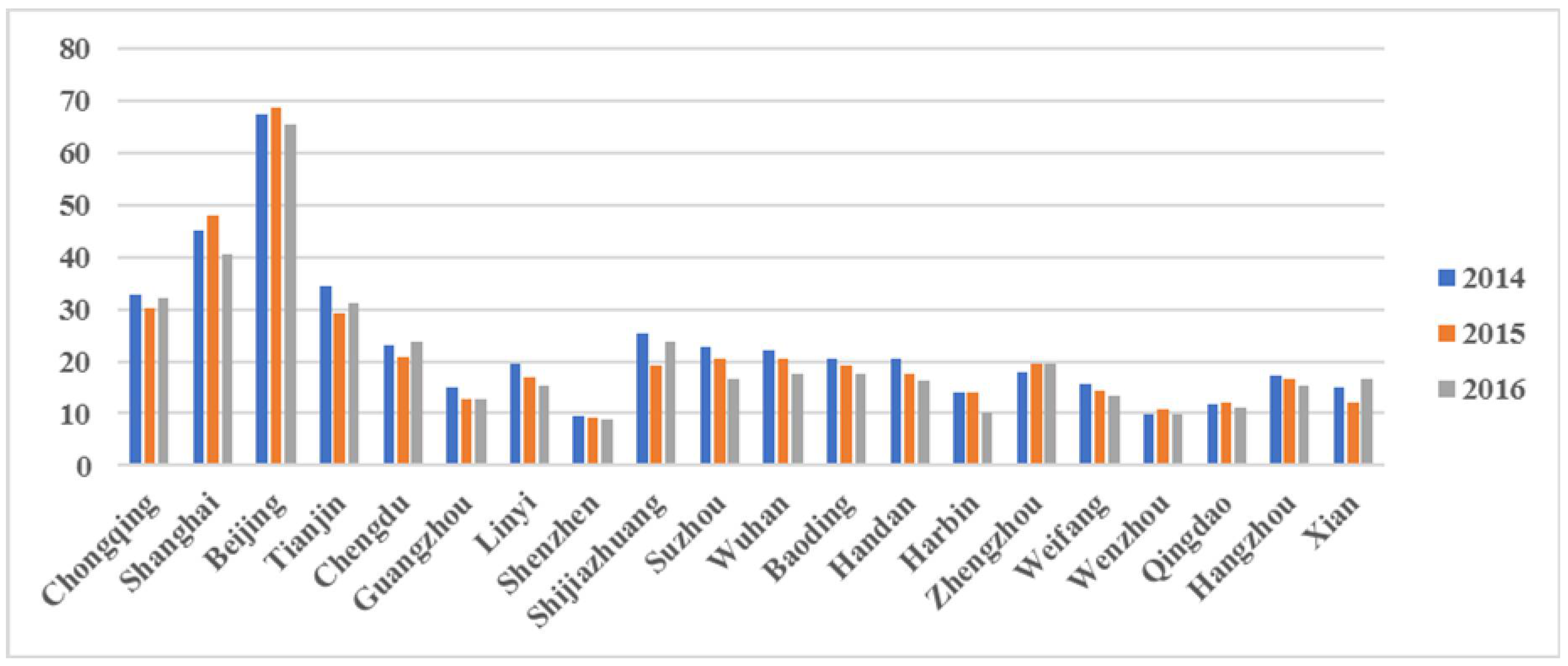
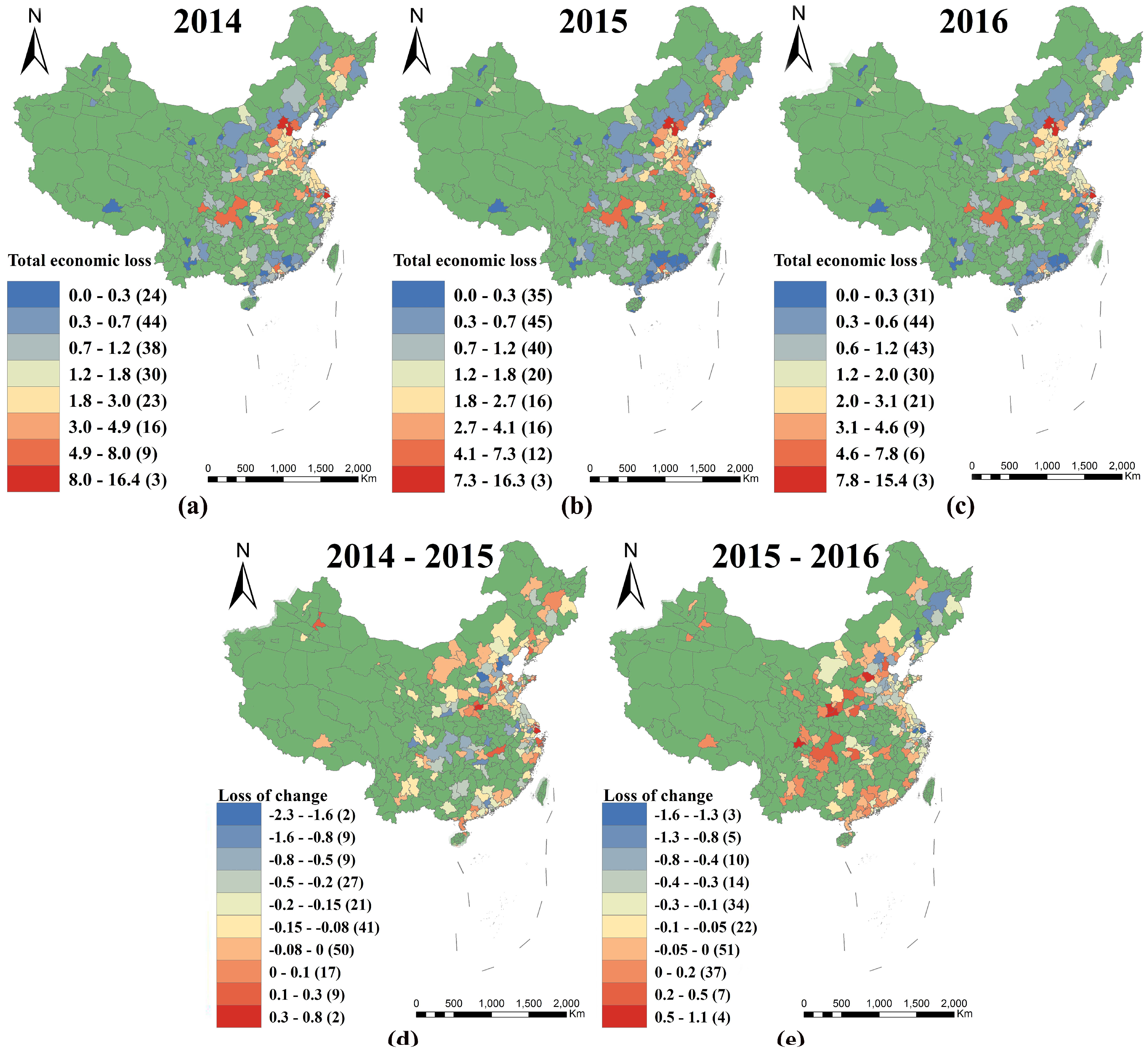
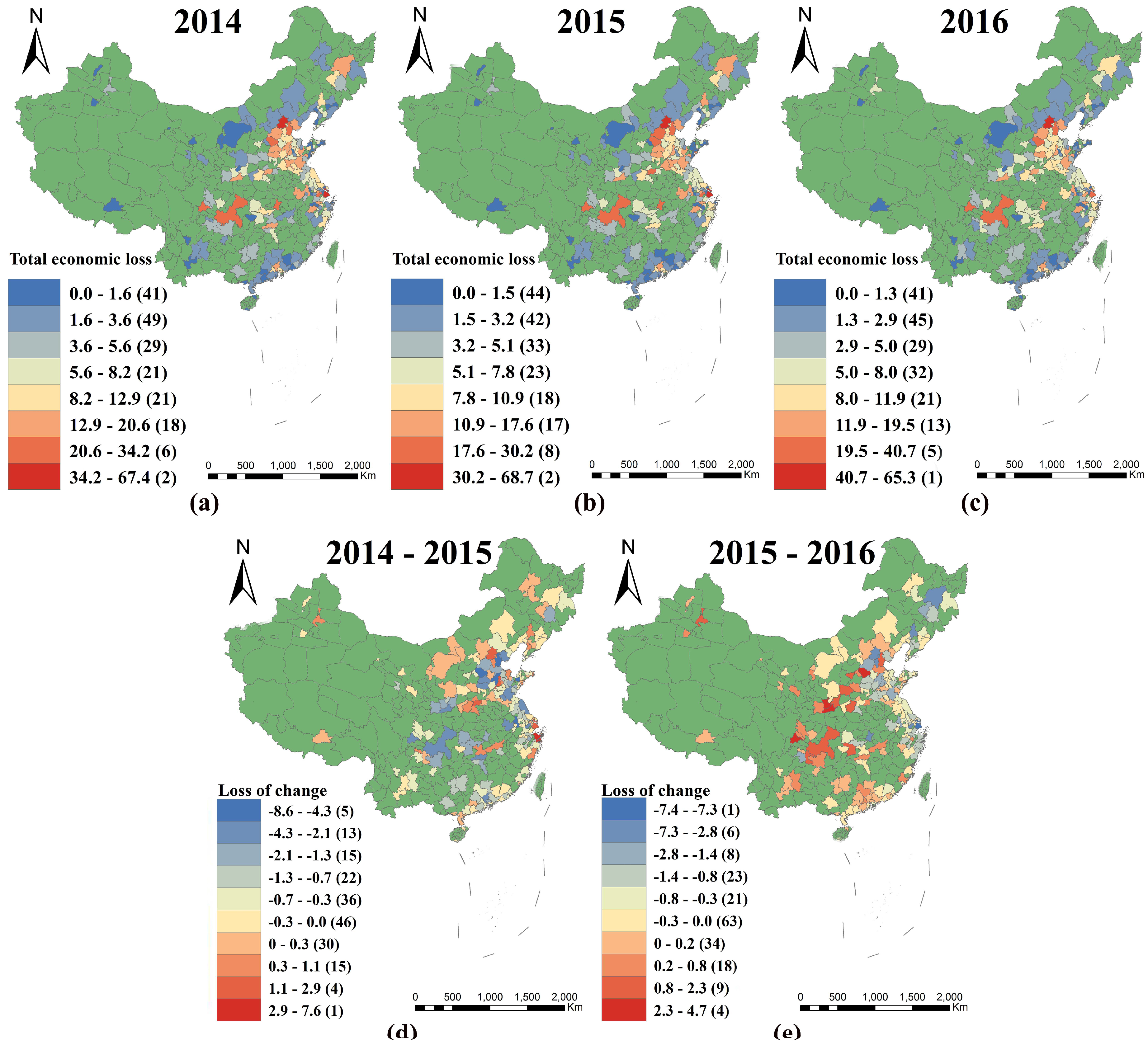
3.3. Economic Loss of Health Impacts
3.4. Uncertainty Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Monetary Fund (IMF). World Economic Outlook Databases. Available online: http://www.imf.org/external/ns/cs.aspx?id=28 (accessed on 4 October 2016).
- Cao, C.; Jiang, W.; Wang, B.; Fang, J.; Lang, J.; Tian, G.; Jiang, J.; Zhu, T.F. Inhalable microorganisms in Beijing’s PM2.5 and PM10 pollutants during a severe smog event. Environ. Sci. Technol. 2014, 48, 1499–1507. [Google Scholar] [CrossRef] [PubMed]
- Mo, Z.; Fu, Q.; Zhang, L.; Lyu, D.; Mao, G. Acute effects of air pollution on respiratory disease mortalities and outpatients in Southeastern China. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Dabass, A.; Talbott, E.O.; Venkat, A.; Rager, J.; Marsh, G.M. Association of exposure to particulate matter (PM2.5) air pollution and biomarkers of cardiovascular disease risk in adult NHANES participants (2001–2008). Int. J. Hyg. Environ. Health 2016, 3, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Zhou, Y.; Lu, Y.; Duan, Y.; Tang, X.; Deng, Q.; Yuan, H. A Case-Crossover Study between Fine Particulate Matter Elemental Composition and Emergency Admission with Cardiovascular Disease. Acta Cardiol. Sin. 2017, 1, 66–73. [Google Scholar] [CrossRef]
- Huang, F.; Bing, P.; Wu, J.; Chen, E.; Chen, L. Relationship between exposure to PM2.5 and lung cancer incidence and mortality: A meta-analysis. Oncotarget 2017, 26, 43322. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; Zhu, L.; Yuan, F.; Kong, X.; Huang, T.; Cai, Y.D. Analysis of the relationship between PM2.5 and lung cancer based on protein-protein interactions. Comb. Chem. High Throughput Screen. 2016, 2, 100–108. [Google Scholar] [CrossRef]
- Badyda, A.J.; Grellier, J.; Dąbrowiecki, P. Ambient PM2.5 exposure and mortality due to lung cancer and cardiopulmonary diseases in polish cities. Adv. Exp. Med. Biol. 2016, 344, 9–17. [Google Scholar] [CrossRef]
- Van Winkle, L.S.; Bein, K.; Anderson, D.; Pinkerton, K.E.; Tablin, F.; Wilson, D.; Wexler, A.S. Biological dose response to PM2.5: Effect of particle extraction method on platelet and lung responses. Toxicol. Sci. 2015, 143, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Liang, S.; Zhao, J.; Qian, Z.; Bassig, B.A.; Yang, R.; Zhang, Y.; Hu, K.; Xu, S.; Zheng, T.; et al. Maternal exposure to air pollutant PM2.5 and PM10 during pregnancy and risk of congenital heart defects. J. Expo. Sci. Environ. Epidemiol. 2016, 4, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Kjellstrom, T.; Holmer, I.; Lemke, B. Workplace heat stress, health and productivity—An increasing challenge for low and middle-income countries during climate change. Glob. Health Action 2009, 1, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lei, Y.; Wu, S.; Chen, J.; Yan, D. The health economic loss of fine particulate matter (PM2.5) in Beijing. J. Clean. Prod. 2017, 161. [Google Scholar] [CrossRef]
- Huang, D.; Zhang, S. Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China. China Environ. Sci. 2013, 1, 166–174. (In Chinese) [Google Scholar]
- Wang, J.; Wang, S.; Voorhees, A.S.; Zhao, B.; Jang, C.; Jiang, J.; Fu, J.S.; Ding, D.; Zhu, Y.; Hao, J. Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta, China. Atmos. Environ. 2015, 123, 440–448. [Google Scholar] [CrossRef]
- Mu, Q.; Zhang, S. Assessment of the Trend of Heavy PM2.5 Pollution Days and Economic Loss of Health Effect during 2001–2013. Acta Sci. Nat. Univ. Pekin. 2015, 4, 694–706. (In Chinese) [Google Scholar]
- Yin, H.; Pizzol, M.; Xu, L. External costs of PM2.5 pollution in Beijing, China: Uncertainty analysis of multiple health impacts and costs. Environ. Pollut. 2017, 356–369. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Dai, H.; Geng, Y.; Xie, Y.; Masui, T.; Liu, Z.; Qian, Y. Economic Impacts from PM2.5 Pollution-Related Health Effects: A Case Study in Shanghai. Environ. Sci. Technol. 2017, 51. [Google Scholar] [CrossRef] [PubMed]
- Lv, L.; Li, H.; Yang, J. A health-based economic assessment of PM2.5 pollution in Chinese major cities. In Proceedings of the 2015 International Forum on Energy, Environment Science and Materials, Shenzhen, China, 25–26 September 2015. [Google Scholar]
- Xie, Y.; Dai, H.; Dong, H.; Hanaoka, T.; Masui, T. Economic Impacts from PM2.5 Pollution-Related Health Effects in China: A Provincial-Level Analysis. Environ. Sci. Technol. 2016, 9, 4836–4843. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhu, J.; Li, W.; Xu, D.; Liu, J. Estimation of the PM2.5 health effects in China during 2000–2011. Environ. Sci. Pollut. Res. 2017, 11, 10695–10707. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.; Shie, R.; Chan, C.; Lin, H. Burden of disease attributable to ambient fine particulate matter exposure in Taiwan. J. Formos. Med. Assoc. 2017, 1, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total Environ. 2016, 568, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, L.; Ye, B.; Feng, H.; Ren, F.; Huang, S. Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016. Int. J. Environ. Res. Public Health 2017, 11, 1321. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Xu, J.; Zhang, S. Valuing the health risks of particulate air pollution in the Pearl River Delta, China. Environ. Sci. Policy 2012, 1, 38–47. [Google Scholar] [CrossRef]
- WHO. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Available online: http://apps.who.int/iris/bitstream/10665/69477/1/WHO_SDE_PHE_OEH_06.02_eng.pdf (accessed on 28 April 2018).
- Ministry of Environmental Protection of the People’s Republic of China. Available online: http://www.zhb.gov.cn/hjzl/zghjzkgb/lnzghjzkgb/ (accessed on 5 June 2017).
- Hong, C.J.; Kan, H.D.; Chen, B.H. Quantitative evaluation of the atmosphere pollution about urban resident health hazard. J. Environ. Health 2005, 1, 62–64. (In Chinese) [Google Scholar]
- Hammitt, J.K. Valuing Mortality Risk: Theory and Practice. Environ. Sci. Technol. 2000, 8, 1396–1400. [Google Scholar] [CrossRef]
- Hammitt, J.K.; Robinson, L.A. The income elasticity of the value per statistical life: Transferring estimates between high and low income populations. J. Benefit-Cost Anal. 2011, 2, 1–29. [Google Scholar] [CrossRef]
- Xie, X. The Value of Health: Environmental Benefit Assessment Method and Urban Air Pollution Control Strategy. Master’s Thesis, Peaking University, Beijing, China, 2010. (In Chinese). [Google Scholar]
- China 2012 Statistical Yearbook. Available online: http://www.stats.gov.cn/tjsj/ndsj/2012/indexeh.htm (accessed on 22 February 2013).
- OECD. Mortality Risk Valuation in Environment, Health and Transport Policies; OECD: Paris, French, 2012; pp. 137–139. ISBN 978-92-64-13080-7. [Google Scholar]
- Hou, Q.; An, X.; Wang, Y.; Tao, Y.; Sun, Z. An assessment of China’s PM10-related health economic losses in 2009. Sci. Total Environ. 2012, 7, 1184–1358. [Google Scholar] [CrossRef] [PubMed]
- China 2016 Statistical Yearbook. Available online: http://www.stats.gov.cn/tjsj/ndsj/2016/indexeh.htm (accessed on 28 February 2017).
- China Health and Family Planning Commission Statistical Yearbook. Available online: http://www.tjcn.org/e/search/result/?searchid=3173 (accessed on 16 June 2017).
- Hammitt, J.K.; Zhou, Y. The economic value of air-pollution-related health risks in China: A contingent valuation study. Environ. Resour. Econ. 2006, 33, 399–423. [Google Scholar] [CrossRef]
- Abhishek, B.; Ashok, K. Application of the crystal ball software for uncertainty and sensitivity analyses for predicted concentration and risk levels. Environ. Prog. Sustain. 2010, 3, 289–294. [Google Scholar] [CrossRef]
- Jiang, X.; Hong, C.; Zheng, Y.; Zheng, B.; Guan, D.; Zhang, Q.; Gouldson, A.; He, K. To what extent can China’s near-term air pollution control policy protect air quality and human health? A case study of the Pearl River Delta region. Environ. Res. Lett. 2015, 10, 104006–104018. [Google Scholar] [CrossRef]
- Apte, J.S.; Marshall, J.D.; Cohen, A.J.; Brauer, M. Addressing Global Mortality from Ambient PM2.5. Environ. Sci. Technol. 2015, 13, 8057–8066. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.; Dey, S.; Chowdhury, S. Ambient PM2.5 exposure and premature mortality burden in the holy city Varanasi, India. Environ. Pollut. 2017, 226, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Etchie, T.O.; Sivanesan, S.; Adewuyi, G.O.; Krishnamurthi, K.; Rao, P.S.; Etchie, A.T.; Pillarisetti, A.; Arora, N.K.; Smith, K.R. The health burden and economic costs averted by ambient PM2.5, pollution reductions in Nagpur, India. Environ. Int. 2017, 102, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Bae, S.; Kashima, S.; Tsuda, T.; Doi, H.; Honda, Y.; Kim, H.; Hong, Y.C. Health Impact Assessment of PM10 and PM2.5 in 27 Southeast and East Asian Cities. J. Occup. Environ. Med. 2015, 7, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Fann, N.; Lamson, A.D.; Anenberg, S.C.; Wesson, K.; Risley, D. Estimating the National Public Health Burden Associated with Exposure to Ambient PM2.5 and Ozone. Risk Anal. 2012, 1, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Åström, S.; Gustafsson, M.; Tekie, H.; Sjöberg, K. Quantification of population exposure to NO2, PM2.5 and PM10 and estimated health impacts in sweden 2010. Hum. Exp. Toxicol. 2015, 11, 1213–1227. [Google Scholar] [CrossRef]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 10082, 1907–1918. [Google Scholar] [CrossRef]
- Maji, K.J.; Arora, M.; Dikshit, A.K. Burden of disease attributed to ambient PM2.5 and PM10 exposure in 190 cities in China. Environ. Sci. Pollut. Res. 2017, 12, 11559–11572. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Shi, M.; Gao, S.; Li, S.; Mao, J. Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on BenMAP. Environ. Pollut. 2017, 211, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Song, Y.; Cai, X.; Zhou, J. Economic assessment of the health effects related to particulate matter pollution in 111 Chinese cities by using economic burden of disease analysis. Environ. Manag. 2008, 4, 947–954. [Google Scholar] [CrossRef] [PubMed]
- OECD. Reviewing the Evidence on and Calculating the Cost of the Health Impacts of Air Pollution, in the Cost of Air Pollution: Health Impacts of Road Transport. Available online: http://www.oecd-ilibrary.org/environment/the-cost-of-air-pollution_9789264210448–en accessed31.01.17 (accessed on 16 June 2017).
- Guo, H.; Cheng, T.; Gu, X.; Wang, Y.; Chen, H. Assessment of PM2.5 concentrations and exposure throughout China using ground observations. Sci. Total Environ. 2017, 301, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Beckx, C.; Int Panis, L.; Arentze, T.; Janssens, D.; Torfs, R.; Broekx, S.; Wets, G. A dynamic activity-based population modelling approach to evaluate exposure to air pollution: Methods and application to a Dutch urban area. Environ. Impact Assess. Rev. 2009, 29, 179–185. [Google Scholar] [CrossRef]
- Beverland, I.J.; Cohen, G.R.; Heal, M.R.; Carder, M.; Yap, C.; Robertson, C.; Hart, C.L.; Agius, R.M. A Comparison of Short-term and Long-term Air Pollution Exposure Associations with Mortality in Two Cohorts in Scotland. Environ. Health Perspect. 2012, 120, 1280–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | 2014 | 2015 | 2016 |
|---|---|---|---|
| All-cause mortality | 278,444 | 238,622 | 216,164 |
| Cardiovascular mortality | 71,058 | 60,991 | 55,321 |
| Respiratory mortality | 42,590 | 36,431 | 32,959 |
| Lung cancer mortality | 92,512 | 78,444 | 70,557 |
| Cardiovascular hospitalization | 1,001,233 | 851,497 | 767,387 |
| Chronic bronchitis | 185,798 | 159,366 | 144,459 |
| Acute bronchitis | 1,034,080 | 881,692 | 795,978 |
| Asthma attack | 19,197,994 | 15,935,983 | 14,130,036 |
| Affected population | 21,697,549 | 18,067,160 | 16,054,024 |
| Category | The Health Economic Loss (100 Million Dollar) | |||||
|---|---|---|---|---|---|---|
| 2014 AHC | 2014 VSL | 2015 AHC | 2015 VSL | 2016 AHC | 2016 VSL | |
| All-cause mortality | 256.32 | 1157.59 | 230.89 | 1061.69 | 214.16 | 1018.62 |
| Cardiovascular mortality | 65.46 | 295.48 | 59.03 | 271.44 | 54.84 | 260.75 |
| Respiratory mortality | 39.19 | 177 | 35.23 | 162.02 | 32.63 | 155.24 |
| Lung cancer mortality | 84.84 | 383.9 | 75.7 | 348.39 | 69.68 | 331.86 |
| Cardiovascular hospitalization | 12.2 | 12.2 | 10.95 | 10.95 | 10.28 | 10.28 |
| Chronic bronchitis | 42.48 | 42.48 | 39 | 39 | 37.44 | 37.44 |
| Acute bronchitis | 0.35 | 0.35 | 0.31 | 0.31 | 0.29 | 0.29 |
| Asthma attack | 6.57 | 6.57 | 5.8 | 5.8 | 5.4 | 5.4 |
| Total economic loss (TEL) | 317.93 | 1219.19 | 286.97 | 1117.76 | 267.38 | 1072.02 |
| TEL/GDP | 0.36% | 1.36% | 0.30% | 1.18% | 0.26% | 1.06% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Luo, L.; Song, C.; Yin, H.; Yang, J. Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China. Int. J. Environ. Res. Public Health 2018, 15, 1278. https://doi.org/10.3390/ijerph15061278
Yang Y, Luo L, Song C, Yin H, Yang J. Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China. International Journal of Environmental Research and Public Health. 2018; 15(6):1278. https://doi.org/10.3390/ijerph15061278
Chicago/Turabian StyleYang, Yang, Liwen Luo, Chao Song, Hao Yin, and Jintao Yang. 2018. "Spatiotemporal Assessment of PM2.5-Related Economic Losses from Health Impacts during 2014–2016 in China" International Journal of Environmental Research and Public Health 15, no. 6: 1278. https://doi.org/10.3390/ijerph15061278