The Role of Communities in Mental Health Care in Low- and Middle-Income Countries: A Meta-Review of Components and Competencies

 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Synthesis
- Domain 1. WHY was a community component or community platform selected for the intervention or an aspect of the intervention? What was the rationale for how the community component would facilitate achievement of the intervention objectives?
- Domain 2. WHERE was the community component conducted or delivered? What were the barriers or facilitators in that setting, i.e., platform?
- Domain 3. WHAT were the community components of the intervention? This could include specific strategies (e.g., community sensitization, awareness raising), or specific therapies (e.g., behavioral activation, cognitive behavioral therapy).
- Domain 4. WHO is the delivery agent for the community component? How were they recruited, trained, supervised, and certified, and how was their competency determined?
- Domain 5. HOW were the community components implemented? This refers to any descriptions of the process by which the actions are implemented, including roles of specialist mental health workers and other support staff, specific manuals, technologies, and tools.
2.4. Quality Assessment of Included Studies
3. Results
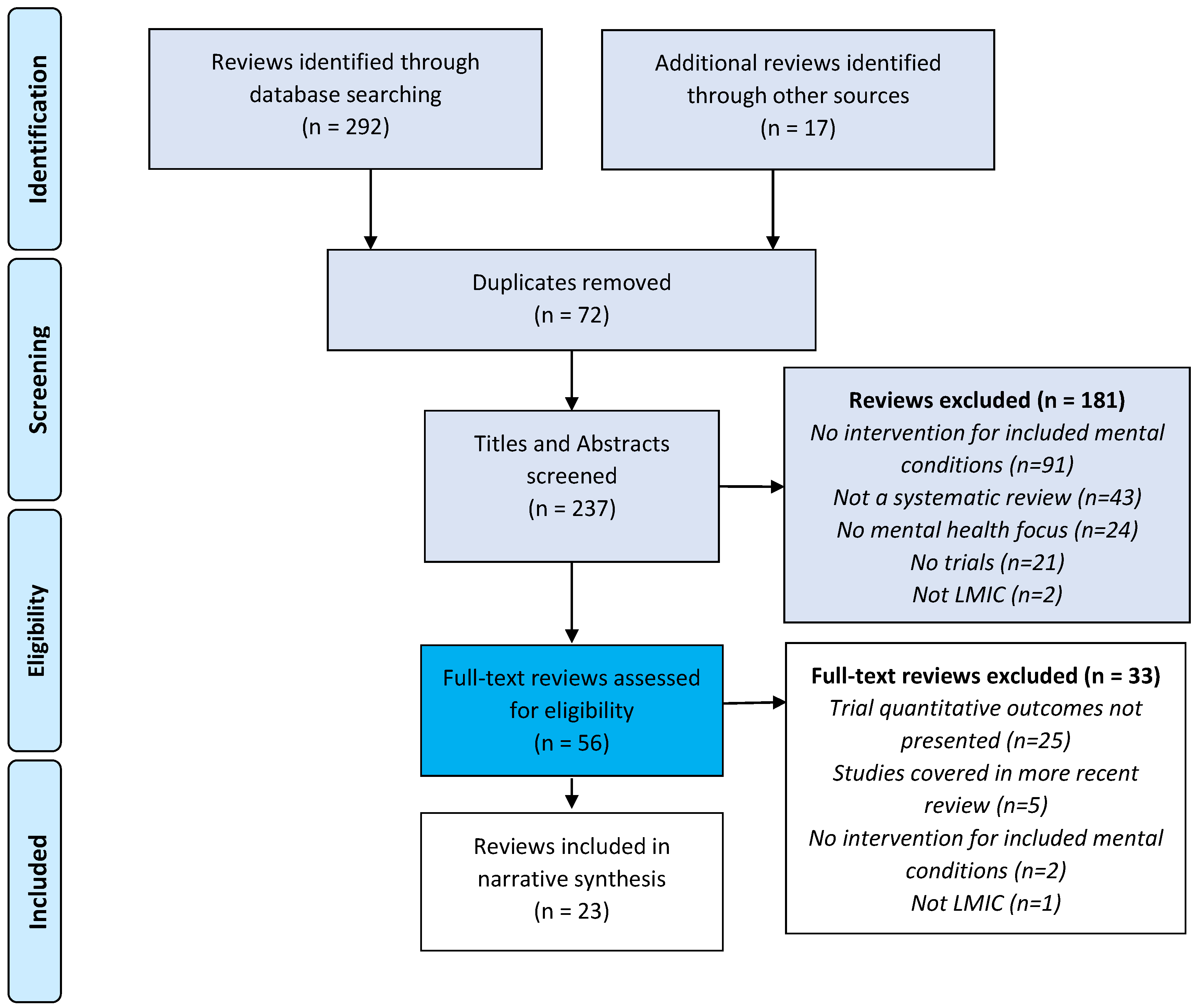
3.1. Search Results and Review Characteristics
3.2. Quality Assessment of the Included Reviews
3.3. Domain 1. Why Are Community Components Selected for Mental Health Interventions?
3.3.1. Community Platforms as an Alternative to Primary Care
3.3.2. Enhancing Quality of and Engagement with Clinical Care
3.3.3. Involvement of Family Members
3.3.4. Economic Productivity
3.3.5. Social Inclusion
3.4. Domain 2. Where Are Community Components Delivered?
3.4.1. Homes
3.4.2. Schools
3.4.3. Other Community Platforms
3.4.4. Technology and Digital Platforms
3.5. Domain 3. What Are the Community Components Delivered?
3.5.1. Population and Community-Wide Mental Health Awareness Programs
3.5.2. Psychoeducation
3.5.3. Skills Training and Community-Based Psychosocial Rehabilitation
3.5.4. Case Management
3.5.5. Psychological Treatments
3.6. Domain 4. Who Delivers the Community Components of Interventions?
3.6.1. Community Health Workers
3.6.2. Other Health Professionals
3.6.3. Formal Providers outside the Healthcare System
3.6.4. Non-Formal Providers
3.7. Domain 5. How Are Community Components Implemented?
3.7.1. Service User Involvement in Design of Community Programs
3.7.2. Identification of Intervention Beneficiaries
3.7.3. Recruitment
3.7.4. Training and Acquiring Competency
3.7.5. Assuring Quality
3.7.6. Sustaining Motivation
3.7.7. Delivery Formats
3.7.8. Integration into Other Platforms
3.7.9. Implementation Barriers
3.8. Domain 6. Harms and Risks
4. Discussion
4.1. Community Components in Mental Health Care from Reviewed Literature
4.2. Agenda for Future Research on Community Components in Mental Health Care
4.2.1. Recommendation 1. Develop Guidance on Standardized Reporting of Community Components for Mental Health Services
4.2.2. Recommendation 2. Employ Implementation Science to Evaluate Community Components of Mental Health Care
4.2.3. Recommendation 3. Study Approaches to Increase Service User and Family Involvement in Developing and Implementing Community Mental Health Services
4.2.4. Recommendation 4. Develop Tools to Study and Promote Competencies in Community Mental Health Care and use these for Research and Quality Improvement
4.2.5. Recommendation 5. Integrate and Evaluate Tools for Service Providers and Service Users to Enhance Reach and Effectiveness of Community Components
4.2.6. Recommendation 6. Use Technology to Expand the Scope and Improve the Quality of Community Mental Health Services
4.2.7. Recommendation 7. Better Integrate Community Platforms into Other Systems of Care
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Allen, J.; Balfour, R.; Bell, R.; Marmot, M. Social determinants of mental health. Int. Rev. Psychiatry 2014, 26, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Druss, B.G.; von Esenwein, S.A.; Compton, M.T.; Rask, K.J.; Zhao, L.; Parker, R.M. A Randomized Trial of Medical Care Management for Community Mental Health Settings: The Primary Care Access, Referral, and Evaluation (PCARE) Study. Am. J. Psychiatry 2010, 167, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.J.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Goldberg, D.; Huxley, P. Mental Illness in the Community: The Pathway to Psychiatric Care; Routledge: London, UK, 2012. [Google Scholar]
- Evans-Lacko, S.; Corker, E.; Williams, P.; Henderson, C.; Thornicroft, G. Effect of the Time to Change anti-stigma campaign on trends in mental-illness-related public stigma among the English population in 2003–13: An analysis of survey data. Lancet Psychiatry 2014, 1, 121–128. [Google Scholar] [CrossRef]
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Brekke, J.; Kay, D.D.; Lee, K.S.; Green, M.F. Biosocial pathways to functional outcome in schizophrenia. Schizophr. Res. 2005, 80, 213–225. [Google Scholar] [CrossRef] [PubMed]
- WHO. Mental Health Action Plan 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. WHO QualityRights Tool Kit; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Thornicroft, G.; Alem, A.; Antunes Dos Santos, R.; Barley, E.; Drake, R.E.; Gregorio, G.; Hanlon, C.; Ito, H.; Latimer, E.; Law, A.; et al. WPA guidance on steps, obstacles and mistakes to avoid in the implementation of community mental health care. World Psychiatry 2010, 9, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thornicroft, G.; Deb, T.; Henderson, C. Community mental health care worldwide: Current status and further developments. World Psychiatry 2016, 15, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Chisholm, D.; Parikh, R.; Charlson, F.J.; Degenhardt, L.; Dua, T.; Ferrari, A.J.; Hyman, S.; Laxminarayan, R.; Levin, C.; et al. Addressing the burden of mental, neurological, and substance use disorders: Key messages from Disease Control Priorities, 3rd edition. Lancet 2016, 387, 1672–1685. [Google Scholar] [CrossRef]
- Thornicroft, G.; Chatterji, S.; Evans-Lacko, S.; Gruber, M.; Sampson, N.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.; Borges, G.; et al. Undertreatment of people with major depressive disorder in 21 countries. Br.J. Psychiatry 2017, 210, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Thirthalli, J.; Channaveerachari, N.; Subbakrishna, D.; Cottler, L.; Varghese, M.; Gangadhar, B. Prospective study of duration of untreated psychosis and outcome of never-treated patients with schizophrenia in India. Indian J. Psychiatry 2011, 53, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Drew, N.; Funk, M.; Tang, S.; Lamichhane, J.; Chávez, E.; Katontoka, S. Human rights violations of people with mental and psychosocial disabilities: An unresolved global crisis. Lancet 2011, 378, 1664–1675. [Google Scholar] [CrossRef]
- Asher, L.; Fekadu, A.; Teferra, S.; De Silva, M.; Pathare, S.; Hanlon, C. “I cry every day and night, I have my son tied in chains”: Physical restraint of people with schizophrenia in community settings in Ethiopia. Glob. Health 2017, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Atta, A.; Attafuah, J.; Jack, H.; Baning, F.; Rosenheck, R. Joining psychiatric care and faith healing in a prayer camp in Ghana: Randomised trial. Br.J. Psychiatry 2018, 212, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Burns, J.K.; Dhingra, M.; Tarver, L.; Kohrt, B.A.; Lund, C. Income inequality and depression: A systematic review and meta-analysis of the association and a scoping review of mechanisms. World Psychiatry 2018, 17, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Lund, C.; Stansfeld, S.; De Silva, M. Social determinants of mental health. In Global Mental Health: Principles and Practice; Patel, V., Minas, H., Cohen, A., Prince, M.J., Eds.; Oxford University Press: New York, NY, USA, 2014; pp. 116–136. [Google Scholar]
- Semrau, M.; Evans-Lacko, S.; Koschorke, M.; Ashenafi, L.; Thornicroft, G. Stigma and discrimination related to mental illness in low- and middle-income countries. Epidemiol. Psychiatr. Sci. 2015, 24, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, C.; Luitel, N.P.; Kathree, T.; Murhar, V.; Shrivasta, S.; Medhin, G.; Ssebunnya, J.; Fekadu, A.; Shidhaye, R.; Petersen, I.; et al. Challenges and opportunities for implementing integrated mental health care: A district level situation analysis from five low- and middle-income countries. PLoS ONE 2014, 9, e88437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gwaikolo, W.S.; Kohrt, B.A.; Cooper, J.L. Health system preparedness for integration of mental health services in rural Liberia. BMC Health Serv. Res. 2017, 17, 508. [Google Scholar] [CrossRef] [PubMed]
- Angdembe, M.; Kohrt, B.A.; Jordans, M.; Rimal, D.; Luitel, N.P. Situational analysis to inform development of primary care and community-based mental health services for severe mental disorders in Nepal. Int. J. Ment. Health Syst. 2017, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. Word Bank Country and Lending Groups. Availabe online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 13 April 2018).
- Singla, D.R.; Kohrt, B.A.; Murray, L.K.; Anand, A.; Chorpita, B.F.; Patel, V. Psychological treatments for the world: Lessons from low- and middle-income countries. Annu. Rev. Clin. Psychol. 2017, 13, 149–181. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Asher, L.; Patel, V.; De Silva, M.J. Community-based psychosocial interventions for people with schizophrenia in low and middle-income countries: Systematic review and meta-analysis. BMC Psychiatry 2017, 17, 355. [Google Scholar] [CrossRef] [PubMed]
- Arjadi, R.; Nauta, M.H.; Chowdhary, N.; Bockting, C.L.H. A systematic review of online interventions for mental health in low and middle income countries: A neglected field. Glob. Ment. Health 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Barry, M.M.; Clarke, A.M.; Jenkins, R.; Patel, V. A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health 2013, 13, 835. [Google Scholar] [CrossRef] [PubMed]
- Chibanda, D.; Cowan, F.M.; Healy, J.L.; Abas, M.; Lund, C. Psychological interventions for Common Mental Disorders for People Living With HIV in Low- and Middle-Income Countries: Systematic review. Trop. Med. Int. Health 2015, 20, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, N.; Sikander, S.; Atif, N.; Singh, N.; Ahmad, I.; Fuhr, D.C.; Rahman, A.; Patel, V. The content and delivery of psychological interventions for perinatal depression by non-specialist health workers in low and middle income countries: A systematic review. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 113–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhary, N.; Jotheeswaran, A.; Nadkarni, A.; Hollon, S.; King, M.; Jordans, M.; Rahman, A.; Verdeli, H.; Araya, R.; Patel, V. The methods and outcomes of cultural adaptations of psychological treatments for depressive disorders: A systematic review. Psychol. Med. 2014, 44, 1131–1146. [Google Scholar] [CrossRef] [PubMed]
- Clarke, K.; King, M.; Prost, A. Psychosocial Interventions for Perinatal Common Mental Disorders Delivered by Providers Who Are Not Mental Health Specialists in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis. PLoS Med. 2013, 10, e1001541. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Reijnders, M.; Purgato, M.; Barbui, C. Psychotherapies for depression in low- and middle-income countries: A meta-analysis. World Psychiatry 2018, 17, 90–101. [Google Scholar] [CrossRef] [PubMed]
- De Silva, M.J.; Cooper, S.; Li, H.L.; Lund, C.; Patel, V. Effect of psychosocial interventions on social functioning in depression and schizophrenia: Meta-analysis. Br. J. Psychiatry 2013, 202, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Patel, V.; Thomas, S.; Tol, W. Mental health interventions in schools in low-income and middle-income countries. Lancet Psychiatry 2014, 1, 388–398. [Google Scholar] [CrossRef]
- Iemmi, V.; Blanchet, K.; Gibson, L.J.; Kumar, K.S.; Rath, S.; Hartley, S.; Murthy, G.V.S.; Patel, V.; Weber, J.; Kuper, H. Community-based rehabilitation for people with physical and mental disabilities in low- and middle-income countries: A systematic review and meta-analysis. J. Dev. Eff. 2016, 8, 368–387. [Google Scholar] [CrossRef]
- Jordans, M.J.D.; Tol, W.A.; Komproe, I.H.; De Jong, J.T.V.M. Systematic review of evidence and treatment approaches: Psychosocial and mental health care for children in war. Child Adolesc. Ment. Health 2009, 14, 2–14. [Google Scholar] [CrossRef]
- Jordans, M.J.; Pigott, H.; Tol, W.A. Interventions for Children Affected by Armed Conflict: A Systematic Review of Mental Health and Psychosocial Support in Low- and Middle-Income Countries. Curr. Psychiatry Rep. 2016, 18, 9. [Google Scholar] [CrossRef] [PubMed]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Klasen, H.; Crombag, A.C. What works where? A systematic review of child and adolescent mental health interventions for low and middle income countries. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 595–611. [Google Scholar] [CrossRef] [PubMed]
- Lund, C.; De Silva, M.; Plagerson, S.; Cooper, S.; Chisholm, D.; Das, J.; Knapp, M.; Patel, V. Poverty and mental disorders: Breaking the cycle in low-income and middle-income countries. Lancet 2011, 378, 1502–1514. [Google Scholar] [CrossRef]
- Mutamba, B.B.; van Ginneken, N.; Smith Paintain, L.; Wandiembe, S.; Schellenberg, D. Roles and effectiveness of lay community health workers in the prevention of mental, neurological and substance use disorders in low and middle income countries: A systematic review. BMC Health Serv. Res. 2013, 13, 412. [Google Scholar] [CrossRef] [PubMed]
- Naslund, J.A.; Aschbrenner, K.A.; Araya, R.; Marsch, L.A.; Unützer, J.; Patel, V.; Bartels, S.J. Digital technology for treating and preventing mental disorders in low-income and middle-income countries: A narrative review of the literature. Lancet Psychiatry 2017, 4, 486–500. [Google Scholar] [CrossRef]
- Rahman, A.; Fisher, J.; Bower, P.; Luchters, S.; Thach, T.; Yasamy, M.T.; Saxena, S.; Waheed, W. Interventions for common perinatal mental disorders in women in low- and middle-income countries: A systematic review and meta-analysis. Bull. World Health Org. 2013, 91, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Rane, A.; Church, S.; Bhatia, U.; Orford, J.; Velleman, R.; Nadkarni, A. Psychosocial interventions for addiction-affected families in Low and Middle Income Countries: A systematic review. Addict. Behav. 2017, 74, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, R.A.; Fazel, M. School and Community-Based Interventions for Refugee and Asylum Seeking Children: A Systematic Review. PLoS ONE 2014, 9, e89359. [Google Scholar] [CrossRef] [PubMed]
- van Ginneken, N.; Tharyan, P.; Lewin, S.; Rao, G.N.; Meera, S.M.; Pian, J.; Chandrashekar, S.; Patel, V. Non-specialist health worker interventions for the care of mental, neurological and substance-abuse disorders in low- and middle-income countries. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hungerbuehler, I.; Valiengo, L.; Loch, A.A.; Rössler, W.; Gattaz, W.F. Home-Based Psychiatric Outpatient Care Through Videoconferencing for Depression: A Randomized Controlled Follow-Up Trial. JMIR Ment Health 2016, 3, e36. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Wang, Y. Yi yu zheng zong he shi jia ting zhi liao: 76 li dan mang sui ji dui zhao (Synthetical family treatment for depression: A randomized-controlled single-blind study among 76 cases). J. Clin. Rehabil. Tissue Eng. Res. 2007, 11, 7787–7790. [Google Scholar]
- Barrera-Valencia, C.; Benito-Devia, A.V.; Vélez-Álvarez, C.; Figueroa-Barrera, M.; Franco-Idárraga, S.M. Cost-effectiveness of synchronous vs. asynchronous telepsychiatry in prison inmates with depression. Rev. Colomb. Psiquiatr. (Engl. Ed.) 2017, 46, 65–73. [Google Scholar] [CrossRef]
- Bass, J.K.; Annan, J.; McIvor Murray, S.; Kaysen, D.; Griffiths, S.; Cetinoglu, T.; Wachter, K.; Murray, L.K.; Bolton, P.A. Controlled Trial of Psychotherapy for Congolese Survivors of Sexual Violence. New Engl. J. Med. 2013, 368, 2182–2191. [Google Scholar] [CrossRef] [PubMed]
- Ali, B.S.; Rahbar, M.H.; Naeem, S.; Gul, A.; Mubeen, S.; Iqbal, A. The effectiveness of counseling on anxiety and depression by minimally trained counselors: A randomized controlled trial. Am. J. Psychoth. 2003, 57, 324–336. [Google Scholar] [CrossRef]
- Marasinghe, R.B.; Edirippulige, S.; Kavanagh, D.; Smith, A.; Jiffry, M.T.M. Effect of mobile phone-based psychotherapy in suicide prevention: A randomized controlled trial in Sri Lanka. J. Telemed. Telecare 2012, 18, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Bolton, P.; Lee, C.; Haroz, E.E.; Murray, L.; Dorsey, S.; Robinson, C.; Ugueto, A.M.; Bass, J. A Transdiagnostic Community-Based Mental Health Treatment for Comorbid Disorders: Development and Outcomes of a Randomized Controlled Trial among Burmese Refugees in Thailand. PLoS Med. 2014, 11, e1001757. [Google Scholar] [CrossRef] [PubMed]
- Bolton, P.; Bass, J.; Neugebauer, R.; Verdeli, H.; Clougherty, K.F.; Wickramaratne, P.; Speelman, L.; Ndogoni, L.; Weissman, M. Group interpersonal psychotherapy for depression in rural Uganda: A randomized controlled trial. JAMA 2003, 289, 3117–3124. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.; Fong, D.Y.T.; Yuen, K.H.; Yuk, H.; Pang, P.; Humphreys, J.; Bullock, L. Effect of an Advocacy Intervention on Mental Health in Chinese Women Survivors of Intimate Partner Violence A Randomized Controlled Trial. JAMA 2010, 304, 536–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.-L.; Luo, S.-Y.; Chan, S.W.-C. Interpersonal psychotherapy-oriented program for Chinese pregnant women: Delivery, content, and personal impact. Nurs. Health Sci. 2012, 14, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.-l.; Chan, S.W.-c.; Li, X.; Chen, S.; Hao, Y. Evaluation of an interpersonal-psychotherapy-oriented childbirth education programme for Chinese first-time childbearing women: A randomised controlled trial. Int. J. Nurs. Stud. 2010, 47, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Wang, Z.-Z.; Qiu, L.-R.; Wan, G.-B.; Lin, Y.; Wei, Z. Psychological intervention for postpartum depression. J. Huazhong Univ. Sci. Technol. [Med. Sci.] 2014, 34, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Ngai, F.W.; Wong, P.W.C.; Leung, K.Y.; Chau, P.H.; Chung, K.F. The Effect of Telephone-Based Cognitive-Behavioral Therapy on Postnatal Depression: A Randomized Controlled Trial. Psychother. Psychosom. 2015, 84, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Petersen, I.; Hancock, J.H.; Bhana, A.; Govender, K. A group-based counselling intervention for depression comorbid with HIV/AIDS using a task shifting approach in South Africa: A randomized controlled pilot study. J. Affect. Disord. 2014, 158, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, I.M.; Tomlinson, M.; Harwood, J.M.; O’Connor, M.J.; Worthman, C.M.; Mbewu, N.; Stewart, J.; Hartley, M.; Swendeman, D.; Comulada, W.S. Outcomes of home visits for pregnant mothers and their infants: A cluster randomised controlled trial. AIDS (Lond. Engl.) 2013, 27, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Landman, M.; Tomlinson, M.; Molteno, C.; Swartz, L.; Murray, L. Impact of a mother—Infant intervention in an indigent peri-urban South African context. Br. J. Psychiatry 2002, 180, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Tomlinson, M.; Swartz, L.; Landman, M.; Molteno, C.; Stein, A.; McPherson, K.; Murray, L. Improving quality of mother-infant relationship and infant attachment in socioeconomically deprived community in South Africa: Randomised controlled trial. Br. Med. J. 2009, 338, b1858. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Malik, A.; Sikander, S.; Roberts, C.; Creed, F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: A cluster-randomised controlled trial. Lancet 2008, 372, 902–909. [Google Scholar] [CrossRef]
- Hughes, M. Randomised, Controlled Trial of a Perinatal Psycho-Social Intervention for Postnatal Depression in Goa, India; University of London King’s College London Institute of Psychiatry: London, UK, 2009. [Google Scholar]
- Hirani, S.S.; Karmaliani, R.; McFarlane, J.; Asad, N.; Madhani, F.; Shehzad, S.; Ali, N.A. Development of an economic skill building intervention to promote women's safety and child development in Karachi, Pakistan. Issues Ment. Health Nurs. 2010, 31, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Aracena, M.; Krause, M.; Pérez, C.; Méndez, M.J.; Salvatierra, L.; Soto, M.; Pantoja, T.; Navarro, S.; Salinas, A.; Farah, C.; et al. A cost-effectiveness evaluation of a home visit program for adolescent mothers. J. Health Psychol. 2009, 14, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Lara, M.A.; Navarro, C.; Navarrete, L. Outcome results of a psycho-educational intervention in pregnancy to prevent PPD: A randomized control trial. J. Affect. Disord. 2010, 122, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Langer, A.; Farnot, U.; Garcia, C.; Barros, F.; Victora, C.; Belizan, J.M.; Villar, J. The Latin American trial of psychosocial support during pregnancy: Effects on mother's wellbeing and satisfaction. Soc. Sci. Med. 1996, 42, 1589–1597. [Google Scholar] [CrossRef]
- Dybdahl, R. Children and mothers in war: An outcome study of a psychosocial intervention program. Child Dev. 2001, 72, 1214–1230. [Google Scholar] [CrossRef] [PubMed]
- Tezel, A.; Gözüm, S. Comparison of effects of nursing care to problem solving training on levels of depressive symptoms in post partum women. Patient Educa. Couns. 2006, 63, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Botha, U.A.; Koen, L.; Joska, J.A.; Hering, L.M.; Oosthuizen, P.P. Assessing the efficacy of a modified assertive community-based treatment programme in a developing country. BMC Psychiatry 2010, 10, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, J.; Zhu, Y.; Zhang, W.; Wang, Y.; Zhang, C. Comprehensive family therapy: An effective approach for cognitive rehabilitation in schizophrenia. Neuropsychiatr. Dis. Treat. 2015, 11, 1247–1253. [Google Scholar] [PubMed]
- Chatterjee, S.; Naik, S.; John, S.; Dabholkar, H.; Balaji, M.; Koschorke, M.; Varghese, M.; Thara, R.; Weiss, H.A.; Williams, P.; et al. Effectiveness of a community-based intervention for people with schizophrenia and their caregivers in India (COPSI): A randomised controlled trial. Lancet 2014, 383, 1385–1394. [Google Scholar] [CrossRef]
- Chatterjee, S.; Patel, V.; Chatterjee, A.; Weiss, H.A. Evaluation of a community-based rehabilitation model for chronic schizophrenia in rural India. Br.J. Psychiatry J. Ment. Sci. 2003, 182, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Ghadiri Vasfi, M.; Moradi-Lakeh, M.; Esmaeili, N.; Soleimani, N.; Hajebi, A. Efficacy of aftercare services for people with severe mental disorders in Iran: A randomized controlled trial. Psychiatr. Serv. 2015, 66, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Hegde, S.; Rao, S.L.; Raguram, A.; Gangadhar, B.N. Addition of home-based cognitive retraining to treatment as usual in first episode schizophrenia patients: A randomized controlled study. Indian J. Psychiatry 2012, 54, 15–22. [Google Scholar] [PubMed]
- Li, Z.; Arthur, D. Family education for people with schizophrenia in Beijing, China: Randomised controlled trial. Br.J. Psychiatry 2005, 187, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Ran, M.-S.; Xiang, M.-Z.; Chan, C.L.-W.; Leff, J.; Simpson, P.; Huang, M.-S.; Shan, Y.-H.; Li, S.-G. Effectiveness of psychoeducational intervention for rural Chinese families experiencing schizophrenia. A randomised controlled trial. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, V.; Tehranidoost, M.; Yunesian, M.; Amini, H.; Mohammadi, M.; Jalali Roudsari, M. Effectiveness of a low-intensity home-based aftercare for patients with severe mental disorders: A 12-month randomized controlled study. Commun. Ment. Health J. 2012, 48, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Sungur, M.B.; Soygur, H.; Guner, P.; Ustun, B.; Cetin, I.; Falloon, I.R. Identifying an optimal treatment for schizophrenia: A 2-year randomized controlled trial comparing integrated care to a high-quality routine treatment. Int. J. Psychiatry Clin. Pract. 2011, 15, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; Ran, M.; Li, S. A controlled evaluation of psychoeducational family intervention in a rural Chinese community. Br. J. Psychiatry 1994, 165, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Xiong, W.; Phillips, M.R.; Hu, X.; Wang, R.; Dai, Q.; Kleinman, J.; Kleinman, A. Family-based intervention for schizophrenic patients in China: A randomised controlled trial. Br.J. Psychiatry 1994, 165, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, M.; Li, J.; Phillips, M.R. Randomised-control trial of family intervention for 78 first-episode male schizophrenic patients: An 18-month study in Suzhou, Jiangsu. Br. J. Psychiatry 1994, 164, 96–102. [Google Scholar]
- Cruz Almanza, M.D.L.A.; Gaona Márquez, L.; Sánchez Sosa, J.J. Empowering women abused by their problem drinker spouses: Effects of a cognitive-behavioral intervention. Salud Ment. 2006, 29, 25–31. [Google Scholar]
- Tiburcio, M.; Natera, G. Evaluación de un modelo de intervención breve para familiares de usuarios de alcohol y drogas. Un estudio piloto. Salud Ment. 2003, 26, 33–42. [Google Scholar]
- Li, L.; Hien, N.T.; Lin, C.; Tuan, N.A.; Tuan, L.A.; Farmer, S.C.; Detels, R. An intervention to improve mental health and family well-being of injecting drug users and family members in Vietnam. Psychol. Addict. Behav. 2014, 28, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Baharudin, D.F.; Mohd Hussin, A.H.; Sumari, M.; Mohamed, S.; Zakaria, M.Z.; Sawai, R.P. Family intervention for the treatment and rehabilitation of drug addiction: An exploratory study. J. Subst. Use 2014, 19, 301–306. [Google Scholar] [CrossRef]
- Jordans, M.J.; Tol, W.A.; Komproe, I.H.; Susanty, D.; Vallipuram, A.; Ntamatumba, P.; Lasuba, A.C.; de Jong, J.T. Development of a multi-layered psychosocial care system for children in areas of political violence. Int. J. Ment. Health Syst. 2010, 4, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordans, M.J.D.; Komproe, I.H.; Tol, W.A.; Kohrt, B.A.; Luitel, N.P.; Macy, R.D.; de Jong, J.T.V.M. Evaluation of a classroom-based psychosocial intervention in conflict-affected Nepal: A cluster randomized controlled trial. J. Child Psychol. Psychiatry Allied Discip. 2010, 51, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.; Komproe, I.; Jordans, M.; Ndayisaba, A.; Ntamutumba, P.; Sipsma, H.; Smallegange, E.; Macy, R.; de Jong, J. School-based mental health intervention for children in war-affected Burundi: A cluster randomized trial. BMC Med. 2014, 12, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tol, W.A.; Komproe, I.H.; Jordans, M.J.D.; Vallipuram, A.; Sipsma, H.; Sivayokan, S.; Macy, R.D.; De Jong, J.T. Outcomes and moderators of a preventive school-based mental health intervention for children affected by war in Sri Lanka: A cluster randomized trial. World Psychiatry 2012, 11, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Komproe, I.H.; Susanty, D.; Jordans, M.J.D.; Macy, R.D.; De Jong, J. School-based mental health intervention for children affected by political violence in Indonesia—A cluster randomized trial. JAMA 2008, 300, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Tol, W.A.; Komproe, I.H.; Jordans, M.J.D.; Gross, A.L.; Susanty, D.; Macy, R.D.; de Jong, J.T.V.M. Mediators and moderators of a psychosocial intervention for children affected by political violence. J. Consul. Clin. Psychol. 2010, 78, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.D.; Komproe, I.H.; Tol, W.A.; Susanty, D.; Vallipuram, A.; Ntamatumba, P.; Lasuba, A.C.; De Jong, J.T.V.M. Practice-Driven Evaluation of a Multi-Layered Psychosocial Care Package for Children in Areas of Armed Conflict. Community Ment. Health Journal 2011, 47, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.D.; Tol, W.A.; Komproe, I.H. Mental health interventions for children in adversity: Pilot-testing a research strategy for treatment selection in low-income settings. Soc. Sci. Med. 2011, 73, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.; Tol, W.A.; Susanty, D.; Ntamatumba, P.; Luitel, N.P.; Komproe, I.H.; de Jong, J.T. Implementation of a mental health care package for children in areas of armed conflict: A case study from Burundi, Indonesia, Nepal, Sri Lanka, and Sudan. PLoS Med 2013, 10, e1001371. [Google Scholar] [CrossRef] [PubMed]
- Layne, C.M.; Saltzman, W.R.; Poppleton, L.; Burlingame, G.M.; Pašalić, A.; Duraković, E.; Mušić, M.; Ćampara, N.; Dapo, N.; Arslanagić, B. Effectiveness of a school-based group psychotherapy program for war-exposed adolescents: A randomized controlled trial. J. Am. Acad.f Child Adolesc. Psychiatry 2008, 47, 1048–1062. [Google Scholar] [CrossRef] [PubMed]
- Botha, U.A.; Koen, L.; Galal, U.; Jordaan, E.; Niehaus, D.J.H. The rise of assertive community interventions in South Africa: A randomized control trial assessing the impact of a modified assertive intervention on readmission rates; a three year follow-up. BMC Psychiatry 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Fayyad, J.A.; Farah, L.; Cassir, Y.; Salamoun, M.M.; Karam, E.G. Dissemination of an evidence-based intervention to parents of children with behavioral problems in a developing country. Eur. Child Adolesc. Psychiatry 2010, 19, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.R.; Kumbakumba, E.; Aboud, F.E. Effects of a parenting intervention to address maternal psychological wellbeing and child development and growth in rural Uganda: A community-based, cluster-randomised trial. Lancet Glob.Health 2015, 3, e458–e469. [Google Scholar] [CrossRef]
- Singla, D.R.; Kumbakumba, E. The development and implementation of a theory-informed, integrated mother-child intervention in rural Uganda. Soc. Sci. Med. 2015, 147, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Chowdhary, N.; Pednekar, S.; Cohen, A.; Andrew, G.; Araya, R.; Simon, G.; King, M.; Telles, S.; Verdeli, H.; et al. Integrating evidence-based treatments for common mental disorders in routine primary care: Feasibility and acceptability of the MANAS intervention in Goa, India. World Psychiatry 2008, 7, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Detels, R.; Zhang, J.; Li, V.; Li, J. Community-Based Trial to Prevent Drug Use Among Youths in Yunnan, China. Am. J. Public Health 2002, 92, 1952–1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonhauser, M.; Fernandez, G.; Püschel, K.; Yañez, F.; Montero, J.; Thompson, B.; Coronado, G. Improving physical fitness and emotional well-being in adolescents of low socioeconomic status in Chile: Results of a school-based controlled trial. Health Promot. Int. 2005, 20, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Hu, P.; Zhang, Y.; Lu, Q.; Wang, D.; Yin, L.; Chen, Y.; Zou, X. Cognitive behavioral therapy in combination with systemic family therapy improves mild to moderate postpartum depression. Rev. Bras. Psiquiatr. 2014, 36, 47–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, P.; Bass, J.; Betancourt, T.; Speelman, L.; Onyango, G.; Clougherty, K.F.; Neugebauer, R.; Murray, L.; Verdeli, H. Interventions for depression symptoms among adolescent survivors of war and displacement in northern Uganda: A randomized controlled trial. JAMA 2007, 298, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Leese, M.; Koschorke, M.; McCrone, P.; Naik, S.; John, S.; Dabholkar, H.; Goldsmith, K.; Balaji, M.; Varghese, M.; et al. Collaborative community based care for people and their families living with schizophrenia in India: Protocol for a randomised controlled trial. Trials 2011, 12, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutamba, B.B.; Kane, J.C.; De Jong, J.; Okello, J.; Musisi, S.; Kohrt, B.A. Psychological treatments delivered by community health workers in low-resource government health systems: Effectiveness of group interpersonal psychotherapy for caregivers of children affected by Nodding Syndrome in Uganda. Psychol. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lay, B.; Salize, H.J.; Dressing, H.; Rüsch, N.; Schönenberger, T.; Bühlmann, M.; Bleiker, M.; Lengler, S.; Korinth, L.; Rössler, W. Preventing compulsory admission to psychiatric inpatient care through psycho-education and crisis focused monitoring. BMC Psychiatry 2012, 12, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shidhaye, R.; Murhar, V.; Gangale, S.; Aldridge, L.; Shastri, R.; Parikh, R.; Shrivastava, R.; Damle, S.; Raja, T.; Nadkarni, A.; et al. The effect of VISHRAM, a grass-roots community-based mental health programme, on the treatment gap for depression in rural communities in India: A population-based study. Lancet Psychiatry 2017, 4, 128–135. [Google Scholar] [CrossRef]
- Maes, K. The Lives of Community Health Workers: Local Labor and Globbal Health in Urban Ethiopia; Taylor & Francis: London, UK, 2016. [Google Scholar]
- Maes, K.; Kalofonos, I. Becoming and remaining community health workers: Perspectives from Ethiopia and Mozambique. Soc. Sci. Med. 2013, 87, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maes, K.; Closser, S.; Vorel, E.; Tesfaye, Y. Using community health workers. Ann. Anthropol.Pract. 2015, 39, 42–57. [Google Scholar] [CrossRef]
- Hanlon, C.; Tesfaye, M.; Wondimagegn, D.; Shibre, T. Ethical and professional challenges in mental health care in low- and middle-income countries. Int. Rev. Psychiatry 2010, 22, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Compton, M.T.; Bakeman, R.; Broussard, B.; Hankerson-Dyson, D.; Husbands, L.; Krishan, S.; Stewart-Hutto, T.; D’Orio, B.M.; Oliva, J.R.; Thompson, N.J. The police-based crisis intervention team (CIT) model: II. effects on level of force and resolution, referral, and arrest. Psychiatr. Serv. 2013. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Blasingame, E.; Compton, M.T.; Dakana, S.F.; Dossen, B.; Lang, F.; Strode, P.; Cooper, J. Adapting the Crisis Intervention Team (CIT) Model of Police–Mental Health Collaboration in a Low-Income, Post-Conflict Country: Curriculum Development in Liberia, West Africa. Am. J. Public Health 2015, 105, e73–e80. [Google Scholar] [CrossRef] [PubMed]
- Zafar, S.; Sikander, S.; Hamdani, S.U.; Atif, N.; Akhtar, P.; Nazir, H.; Maselko, J.; Rahman, A. The effectiveness of Technology-assisted Cascade Training and Supervision of community health workers in delivering the Thinking Healthy Program for perinatal depression in a post-conflict area of Pakistan – study protocol for a randomized controlled trial. Trials 2016, 17, 188. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.J.D.; Aldridge, L.; Luitel, N.P.; Baingana, F.; Kohrt, B.A. Evaluation of outcomes for psychosis and epilepsy treatment delivered by primary health care workers in Nepal: A cohort study. Int. J. Ment. Health Syst. 2017, 11, 70. [Google Scholar] [CrossRef] [PubMed]
- WHO. Mental Health Atlas; Department of Mental Health and Substance Abuse, World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Thornicroft, G. Evidence-based mental health care and implementation science in low- and middle-income countries. Epidemiol. Psychiatr. Sci. 2012, 21, 241–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIMH. Collaborative Hubs for International Research on Mental Health (U19). Availabe online: http://www.nimh.nih.gov/about/organization/gmh/globalhubs/index.shtml (accessed on 16 June 2017).
- Government of Canada. Grand Challenges Canada: Global Mental Health. Availabe online: http://www.grandchallenges.ca/grand-challenges/global-mental-health/ (accessed on 16 June 2017).
- Murray, L.K.P.; Skavenski, S.M.S.W.M.P.H.; Bass, J.P.; Wilcox, H.P.; Bolton, P.M.M.P.H.; Imasiku, M.P.; Mayeya, J.M.P.H. Implementing Evidence-Based Mental Health Care in Low-Resource Settings: A Focus on Safety Planning Procedures. J. Cogn. Psychother. 2014, 28, 168–185. [Google Scholar] [CrossRef]
- Murray, L.K.; Tol, W.; Jordans, M.; Sabir, G.; Amin, A.M.; Bolton, P.; Bass, J.; Bonilla-Escobar, F.J.; Thornicroft, G. Dissemination and implementation of evidence based, mental health interventions in post conflict, low resource settings. Intervention 2014, 12, 94–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semrau, M.; Lempp, H.; Keynejad, R.; Evans-Lacko, S.; Mugisha, J.; Raja, S.; Lamichhane, J.; Alem, A.; Thornicroft, G.; Hanlon, C. Service user and caregiver involvement in mental health system strengthening in low- and middle-income countries: Systematic review. BMC Health Serv. Res. 2016, 16, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempp, H.; Abayneh, S.; Gurung, D.; Kola, L.; Abdulmalik, J.; Evans-Lacko, S.; Semrau, M.; Alem, A.; Thornicroft, G.; Hanlon, C. Service user and caregiver involvement in mental health system strengthening in low- and middle-income countries: A cross-country qualitative study. Epidemiol. Psychiatr. Sci. 2018, 27, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Abayneh, S.; Lempp, H.; Alem, A.; Alemayehu, D.; Eshetu, T.; Lund, C.; Semrau, M.; Thornicroft, G.; Hanlon, C. Service user involvement in mental health system strengthening in a rural African setting: Qualitative study. BMC Psychiatry 2017, 17, 187. [Google Scholar] [CrossRef] [PubMed]
- Gurung, D.; Upadhyaya, N.; Magar, J.; Giri, N.P.; Hanlon, C.; Jordans, M.J.D. Service user and care giver involvement in mental health system strengthening in Nepal: A qualitative study on barriers and facilitating factors. Int. J. Ment. Health Syst. 2017, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.; Gurung, D.; Kaiser, B.N.; Sikkema, K.J.; Dhakal, M.; Bhardwaj, A.; Tergesen, C.; Kohrt, B.A. A service user co-facilitated intervention to reduce mental illness stigma among primary healthcare workers: Utilizing perspectives of family members and caregivers. Fam. Syst. Health 2018. accepted. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Jordans, M.J.D.; Turner, E.L.; Sikkema, K.J.; Luitel, N.P.; Rai, S.; Singla, D.R.; Lamichhane, J.; Lund, C.; Patel, V. Reducing stigma among healthcare providers to improve mental health services (RESHAPE): Protocol for a pilot cluster randomized controlled trial of a stigma reduction intervention for training primary healthcare workers in Nepal. Pilot Feasibil. Stud. 2018, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Collins, P.Y.; Musisi, S.; Frehywot, S.; Patel, V. The core competencies for mental, neurological, and substance use disorder care in sub-Saharan Africa. Glob. Health Action 2015, 8, 26682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmavati, R. Community mental health services for the mentally ill: Practices and ethics. Int. Rev. Psychiatry 2012, 24, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Ramaiya, M.K.; Rai, S.; Bhardwaj, A.; Jordans, M.J.D. Development of a scoring system for non-specialist ratings of clinical competence in global mental health: A qualitative process evaluation of the Enhancing Assessment of Common Therapeutic Factors (ENACT) scale. Glob. Ment. Health 2015, 2, e23. [Google Scholar] [CrossRef] [PubMed]
- Kohrt, B.A.; Jordans, M.J.D.; Rai, S.; Shrestha, P.; Luitel, N.P.; Ramaiya, M.; Singla, D.; Patel, V. Therapist Competence in Global Mental Health: Development of the Enhancing Assessment of Common Therapeutic Factors (ENACT) Rating Scale. Behav. Res. Ther. 2015, 69, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.R.; Weobong, B.; Nadkarni, A.; Chowdhary, N.; Shinde, S.; Anand, A.; Fairburn, C.G.; Dimijdan, S.; Velleman, R.; Weiss, H.; et al. Improving the scalability of psychological treatments in developing countries: An evaluation of peer-led therapy quality assessment in Goa, India. Behav. Res. Ther. 2014, 60, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subba, P.; Luitel, N.P.; Kohrt, B.A.; Jordans, M.J.D. Improving detection of mental health problems in community settings in Nepal: Development and pilot testing of the community informant detection tool. Conf. Health 2017, 11, 28. [Google Scholar] [CrossRef] [PubMed]
- Epping-Jordan, J.E.; Harris, R.; Brown, F.L.; Carswell, K.; Foley, C.; García-Moreno, C.; Kogan, C.; van Ommeren, M. Self-Help Plus (SH+): A new WHO stress management package. World Psychiatry 2016, 15, 295–296. [Google Scholar] [CrossRef] [PubMed]
- van Ginneken, N.; Maheedhariah, M.S.; Ghani, S.; Ramakrishna, J.; Raja, A.; Patel, V. Human resources and models of mental healthcare integration into primary and community care in India: Case studies of 72 programmes. PLoS ONE 2017, 12, e0178954. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Author, Year | Categories of Mental Disorders |
|---|---|
| Asher et al., 2017 [28] | Psychoses |
| Arjadi et al., 2015 [29] | Common mental disorders |
| Barry et al., 2013 [30] | Child and adolescent disorders |
| Chibanda et al., 2015 [31] | Common mental disorders |
| Chowdhary et al., 2014 [32] | Perinatal mental disorders |
| Chowdhary et al., 2014 [33] | Common mental disorders, Perinatal mental disorders |
| Clarke et al., 2013 [34] | Perinatal mental disorders |
| Cuijpers et al., 2017 [35] | Common mental disorders, Perinatal mental disorders |
| De Silva et al., 2013 [36] | Common mental disorders, Psychoses |
| Fazel et al., 2014 [37] | Child and adolescent disorders |
| Iemmi et al., 2016 [38] | Psychoses |
| Jordans et al., 2009 [39] | Child and adolescent disorders |
| Jordans et al., 2016 [40] | Child and adolescent disorders |
| Kieling et al., 2011 [41] | Child and adolescent disorders |
| Klasen et al., 2013 [42] | Child and adolescent disorders |
| Lund et al., 2011 [43] | Common mental disorders |
| Mutamba et al., 2013 [44] | Common mental disorders, Child and adolescent disorders |
| Naslund et al., 2017 [45] | Common mental disorders, Psychoses |
| Rahman et al., 2013 [46] | Perinatal mental disorders |
| Rane et al., 2017 [47] | Substance use disorders |
| Singla et al., 2017 [26] | Common mental disorders, Perinatal mental disorders |
| Tyrer et al., 2014 [48] | Child and adolescent disorders |
| van Ginneken et al., 2013 [49] | Common mental disorders, Perinatal mental disorders, Psychoses, Substance use disorders, Child and adolescent disorders |
| (1) Question and Inclusion | (2) Protocol | (3) Study Design | (4) Comprehensive Search | (5) Study Selection | (6) Data Extraction | (7) Excluded Studies Justification | (8) Included Studies Details | (9) Risk of Bias (RoB) | (10) Funding Sources | (11) Statistical Methods | (12) RoB on meta-analysis | (13) RoB in individual Studies | (14) Explanation for Heterogeneity | (15) Publication Bias | (16) Conflict of Interest | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asher et al., 2017 [28] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Arjadi et al., 2015 [29] | Yes | Yes | Yes | Yes | No | No | No | Yes | Partial Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Barry et al., 2013 [30] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Chibanda et al., 2015 [31] | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Chowdhary et al., 2014 [32] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Chowdhary et al., 2014 [33] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Clarke et al., 2013 [34] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Cuijpers et al., 2017 [35] | Yes | Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| De Silva et al., 2013 [36] | Yes | Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Fazel et al., 2014 [37] | Yes | Partial Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Partial Yes | No | N/A | N/A | No | Yes | Yes | Yes |
| Iemmi et al., 2016 [38] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Jordans et al., 2009 [39] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Partial Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Jordans et al., 2016 [40] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Kieling et al., 2011 [41] | Yes | Partial Yes | No | Partial Yes | No | No | No | Partial Yes | No | No | N/A | N/A | No | Yes | No | Yes |
| Klasen et al., 2013 [42] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | No | N/A | N/A | No | Yes | Yes | Yes |
| Lund et al., 2011 [43] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Partial Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| Mutamba et al., 2013 [44] | Yes | Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Naslund et al., 2017 [45] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Partial Yes | No | N/A | N/A | No | Yes | Yes | Yes |
| Rahman et al., 2013 [46] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Rane et al., 2017 [47] | Yes | Yes | Yes | Partial Yes | Yes | Yes | No | Yes | Partial Yes | No | N/A | N/A | No | Yes | Yes | Yes |
| Singla et al., 2017 [26] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | Yes |
| Tyrer et al., 2014 [48] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | N/A | N/A | Yes | Yes | Yes | Yes |
| van Ginneken et al., 2013 [49] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Total, N (%) * | 23 (100%) | 21 (91%) | 22 (96%) | 17 (74%) | 20 (87%) | 19 (83%) | 6 (26%) | 22 (96%) | 16 (70%) | 1 (4%) | 10 (100%) | 10 (100%) | 17 (74%) | 23 (100%) | 22 (96%) | 23 (100%) |
| Domain | Information |
|---|---|
| How are service users and family members engaged in selection, design, implementation, and evaluation of community components? |
| In addition to service users and caregivers, how were other stakeholders in the community engaged in the design, implementation, and evaluation? This may include potential cadres responsible for delivery and supervision of the program. |
| Why was a community approach selected, and what specific community component was chosen? Include formative research, literature reviews, theory of change workshops and other approaches employed; report the evidence base (e.g., GRADE scoring) for selected approach when available. |
| How do services equitably account for gender, ethnicity, socioeconomic status, and other social factors? What mechanisms are in place to monitor and promote human rights, e.g., QualityRights; (understanding informed consent before patients decide about treatment without feeling coerced)? How are stigma and discrimination monitored and addressed? |
| What activities are included in the community component to address the multiple tiers of comprehensive services, including how is mental health literacy increased? What is done to address universal, targeted, or indicated prevention? |
| What treatments are included in the community component; and how are livelihood and quality of life addressed with psychosocial rehabilitation services? |
| Where are the platforms for the community component; how was it selected and what are the facilitators and barriers? |
| Who is delivering the intervention; how were they selected, trained, and supervised; how is competency evaluated and promoted; how is the mental health and quality of life of service providers monitored? |
| How is the community program integrated into existing healthcare system; what are referral processes in stepped-care approaches? |
| How was the intervention adapted for the specific context; how are fidelity and quality monitored; how is the intervention adapted over time to adjust to community needs and resources; how much do the activities cost; what are the policies, manuals, and material resources needed for initiation, sustaining, and scaling up the community component? |
| What technologies are used for delivery, monitoring fidelity and quality, promoting adherence, etc. (e.g., person-to-person contact through phone; apps on mobile devices; internet-based services)? |
| What adverse events were experienced by participants; did community providers experience adverse outcomes; were there unintended consequences? |
| Domains | Competencies | Examples |
|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohrt, B.A.; Asher, L.; Bhardwaj, A.; Fazel, M.; Jordans, M.J.D.; Mutamba, B.B.; Nadkarni, A.; Pedersen, G.A.; Singla, D.R.; Patel, V. The Role of Communities in Mental Health Care in Low- and Middle-Income Countries: A Meta-Review of Components and Competencies. Int. J. Environ. Res. Public Health 2018, 15, 1279. https://doi.org/10.3390/ijerph15061279
Kohrt BA, Asher L, Bhardwaj A, Fazel M, Jordans MJD, Mutamba BB, Nadkarni A, Pedersen GA, Singla DR, Patel V. The Role of Communities in Mental Health Care in Low- and Middle-Income Countries: A Meta-Review of Components and Competencies. International Journal of Environmental Research and Public Health. 2018; 15(6):1279. https://doi.org/10.3390/ijerph15061279
Chicago/Turabian StyleKohrt, Brandon A., Laura Asher, Anvita Bhardwaj, Mina Fazel, Mark J. D. Jordans, Byamah B. Mutamba, Abhijit Nadkarni, Gloria A. Pedersen, Daisy R. Singla, and Vikram Patel. 2018. "The Role of Communities in Mental Health Care in Low- and Middle-Income Countries: A Meta-Review of Components and Competencies" International Journal of Environmental Research and Public Health 15, no. 6: 1279. https://doi.org/10.3390/ijerph15061279