Susceptibility to Alcohol Hangovers: The Association with Self-Reported Immune Status

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
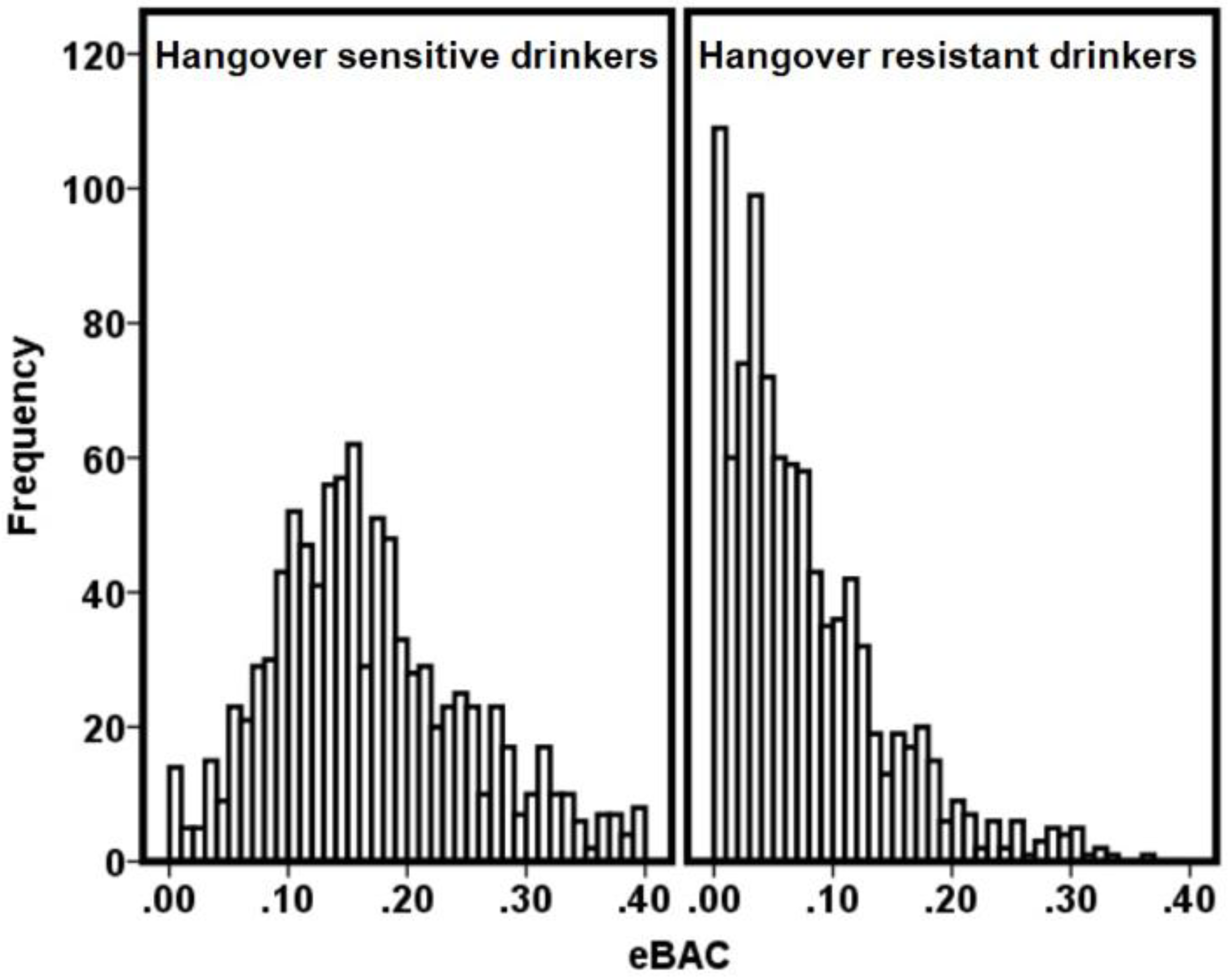
3.1. eBAC Cut-Off of at Least 0.18%
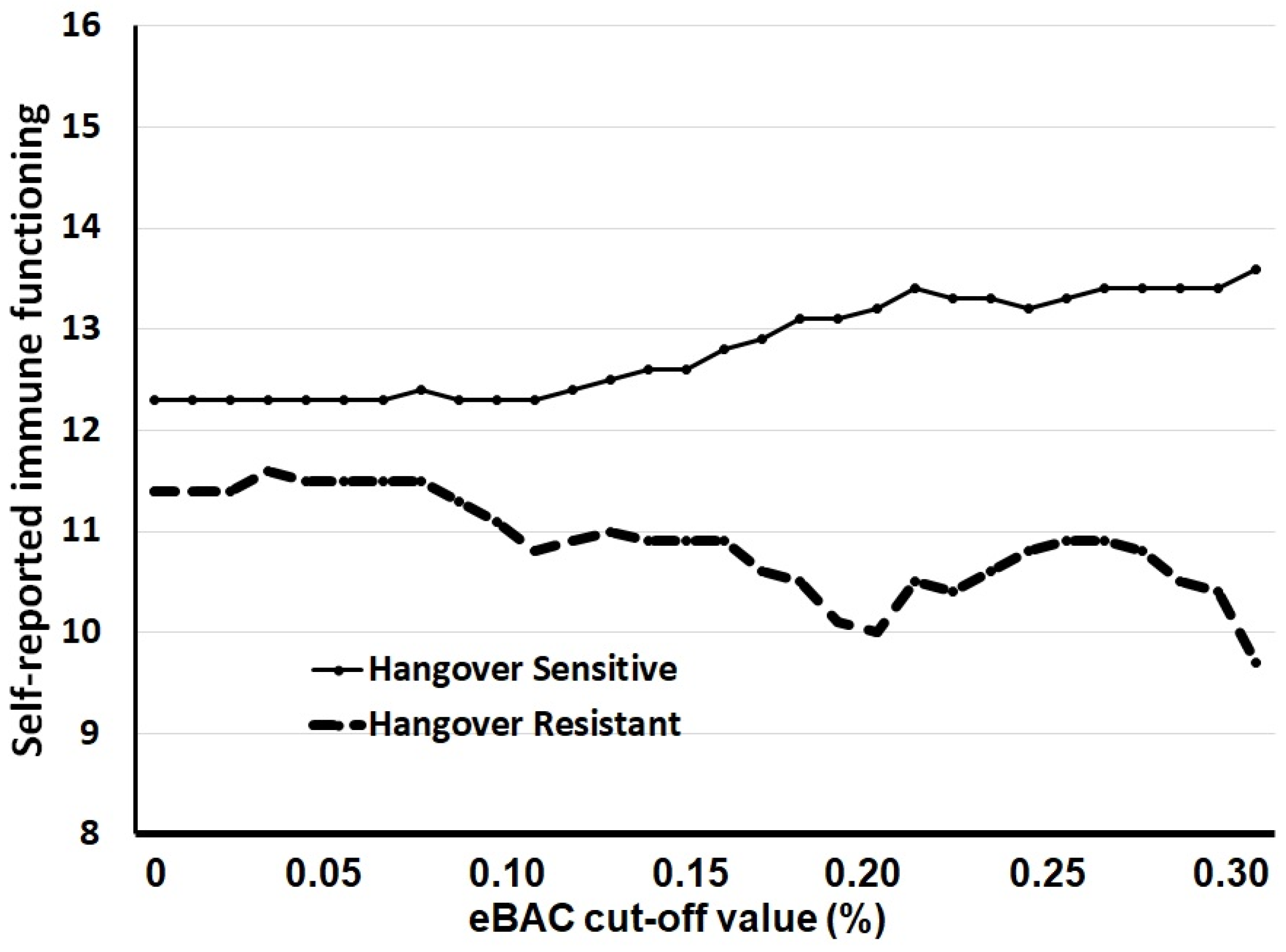
3.2. Other eBAC Cut-Off Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Van Schrojenstein Lantman, M.; Mackus, M.; Van de Loo, A.J.A.E.; Verster, J.C. Development of a definition for the alcohol hangover: Consumer descriptions and expert consensus. Curr. Drug Abuse Rev. 2016, 9, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Howland, J.; Rohsenow, D.J.; Edwards, E.M. Are some drinkers resistant to hangover? A literature review. Curr. Drug Abuse Rev. 2008, 1, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; de Klerk, S.; Bervoets, A.C.; Kruisselbrink, L.D. Can hangover immunity really be claimed? Curr. Drug Abuse Rev. 2013, 6, 253–254. [Google Scholar] [CrossRef] [PubMed]
- Kruisselbrink, L.D.; Bervoets, A.C.; de Klerk, S.; van de Loo, A.J.A.E.; Verster, J.C. Hangover resistance in a Canadian university student population. Addict. Behav. Rep. 2017, 5, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Hogewoning, A.; van de Loo, A.J.A.E.; Mackus, M.; Raasveld, S.J.; de Zeeuw, R.; Bosma, E.R.; Bouwmeester, N.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Characteristics of social drinkers with and without a hangover after heavy alcohol consumption. Subst. Abuse Rehab. 2016, 7, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Penning, R.; van Nuland, M.; Fliervoet, L.A.L.; Olivier, B.; Verster, J.C. The pathology of alcohol hangover. Curr. Drug Abuse Rev. 2010, 3, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Neupane, S.P.; Skulberg, A.; Skulberg, K.R.; Aass, H.C.; Bramness, J.G. Cytokine changes following acute ethanol intoxication in healthy men: A crossover study. Mediat. Inflamm. 2016, 3758590. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C. The alcohol hangover: A puzzling phenomenon. Alcohol Alcohol. 2008, 43, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Kim, W.; Yoon, S.J.; Choi, B.M.; Kim, J.S.; Go, H.J.; Kim, Y.K.; Jeong, J. Effects of alcohol hangover on cytokine production in healthy subjects. Alcohol 2003, 31, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Sobell, L.C.; Agrawal, S.; Sobell, M.B.; Leo, G.I.; Johnson-Young, L.; Cunningham, J.A. Comparison of a Quick Drinking Screen and Timeline Followback with alcohol abusers. J. Stud. Alcohol 2003, 64, 858–861. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.E.; Watson, I.D.; Batt, R.D. Prediction of blood alcohol concentrations in human subjects. Updating the Widmark Equation. J. Stud. Alcohol 1981, 42, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.; Vile, R.; Osborne, L.A.; Romano, M.; Truzoli, R. Problematic Internet Usage and Immune Function. PLoS ONE 2015, 10, e0134538. [Google Scholar] [CrossRef] [PubMed]
- Van Schrojenstein Lantman, M.; Otten, L.S.; Mackus, M.; de Kruijff, D.; Van de Loo, A.J.A.E.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Mental resilience, perceived immune functioning, and health. J. Multidiscip. Healthc. 2017, 10, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Mackus, M.; de Kruijff, D.; Otten, L.S.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Differential gender effects in the relationship between perceived immune functioning and autism spectrum disorder scores. Int. J. Environ. Res. Public Health 2017, 14, 409. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Stephens, R.; Penning, R.; Rohsenow, D.; McGeary, J.; Levy, D.; McKinney, A.; Finnigan, F.; Piasecki, T.M.; Adan, A.; et al. The Alcohol Hangover Research Group consensus statement on best practice in alcohol hangover research. Curr. Drug Abuse Rev. 2010, 3, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Brenner, P.S.; De Lamater, J. Lies, damned lies, and survey self-reports? Identity as a cause of measurement bias. Soc. Psychol. Q. 2016, 79, 333–354. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Hangover Sensitive | Hangover Resistant | ||
|---|---|---|---|
| n = 400 | n = 81 | ||
| Mean (SD) | Mean (SD) | p-Value | |
| Age (years) | 21.1 (1.9) | 20.7 (2.0) | 0.047 * |
| BMI (kg/m2) | 22.3 (2.8) | 22.3 (3.3) | 0.992 |
| Age of regular alcohol consumption | 16.3 (1.3) | 16.6 (1.7) | 0.045 * |
| Number of drinks per average occasion | 8.5 (4.5) | 7.0 (3.5) | 0.004 * |
| Number of drinking days in the past month | 11.5 (6.6) | 8.9 (7.0) | 0.001 * |
| Number of days drunk in the past month | 4.7 (3.6) | 2.3 (2.2) | 0.0001 * |
| Number of drinks consumed on the heaviest occasion | 15.6 (5.5) | 13.8 (4.4) | 0.006 * |
| Duration of alcohol consumption (h) | 6.8 (2.4) | 5.9 (2.1) | 0.001 * |
| eBAC (%) on heaviest occasion | 0.27 (0.1) | 0.26 (0.1) | 0.123 |
| Hangover Sensitive | Hangover Resistant | ||
|---|---|---|---|
| n = 400 | n = 81 | ||
| Mean (SD) | Mean (SD) | p-Value | |
| Overall score | 13.1 (4.9) | 10.5 (3.6) | 0.0001 * |
| Headache | 2.1 (0.9) | 1.7 (0.9) | 0.0001 * |
| Runny nose | 2.0 (1.0) | 1.8 (0.9) | 0.088 |
| Coughing | 2.0 (1.0) | 1.6 (0.9) | 0.002 * |
| Sore throat | 1.7 (0.9) | 1.3 (0.8) | 0.0001 * |
| Diarrhea | 1.4 (1.0) | 1.1 (0.9) | 0.008 * |
| Flu | 0.7 (0.7) | 0.5 (0.6) | 0.254 |
| Mild fever | 0.7 (0.7) | 0.6 (0.6) | 0.953 |
| Sinusitis | 0.3 (0.6) | 0.1 (0.3) | 0.008 * |
| Cold sores | 0.3 (0.7) | 0.3 (0.6) | 0.626 |
| Long-healing injuries | 0.3 (0.7) | 0.3 (0.6) | 0.475 |
| Ear infection | 0.2 (0.6) | 0.1 (0.3) | 0.194 |
| Warts | 0.2 (0.6) | 0.1 (0.4) | 0.092 |
| Eye infection | 0.2 (0.5) | 0.1 (0.4) | 0.482 |
| Bronchitis | 0.1 (0.4) | 0.1 (0.3) | 0.680 |
| Sudden high fever | 0.1 (0.3) | 0.1 (0.3) | 0.204 |
| Sepsis | 0.1 (0.5) | 0.1 (0.3) | 0.088 |
| Pneumonia | 0.0 (0.2) | 0.1 (0.2) | 0.396 |
| Meningitis | 0.0 (0.0) | 0.0 (0.0) | 1.000 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van de Loo, A.J.A.E.; Mackus, M.; Van Schrojenstein Lantman, M.; Kraneveld, A.D.; Brookhuis, K.A.; Garssen, J.; Scholey, A.; Verster, J.C. Susceptibility to Alcohol Hangovers: The Association with Self-Reported Immune Status. Int. J. Environ. Res. Public Health 2018, 15, 1286. https://doi.org/10.3390/ijerph15061286
Van de Loo AJAE, Mackus M, Van Schrojenstein Lantman M, Kraneveld AD, Brookhuis KA, Garssen J, Scholey A, Verster JC. Susceptibility to Alcohol Hangovers: The Association with Self-Reported Immune Status. International Journal of Environmental Research and Public Health. 2018; 15(6):1286. https://doi.org/10.3390/ijerph15061286
Chicago/Turabian StyleVan de Loo, Aurora J. A. E., Marlou Mackus, Marith Van Schrojenstein Lantman, Aletta D. Kraneveld, Karel A. Brookhuis, Johan Garssen, Andrew Scholey, and Joris C. Verster. 2018. "Susceptibility to Alcohol Hangovers: The Association with Self-Reported Immune Status" International Journal of Environmental Research and Public Health 15, no. 6: 1286. https://doi.org/10.3390/ijerph15061286