Growth Charts for Height, Weight, and BMI (6–18 y) for the Tuscany Youth Sports Population

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Evaluation
2.3. Statistical Analysis
2.3.1. Study of the Prevalence of Overweight and Obesity
2.3.2. Tracing Growth Charts
3. Results
3.1. Prevalence of Overweight and Obesity
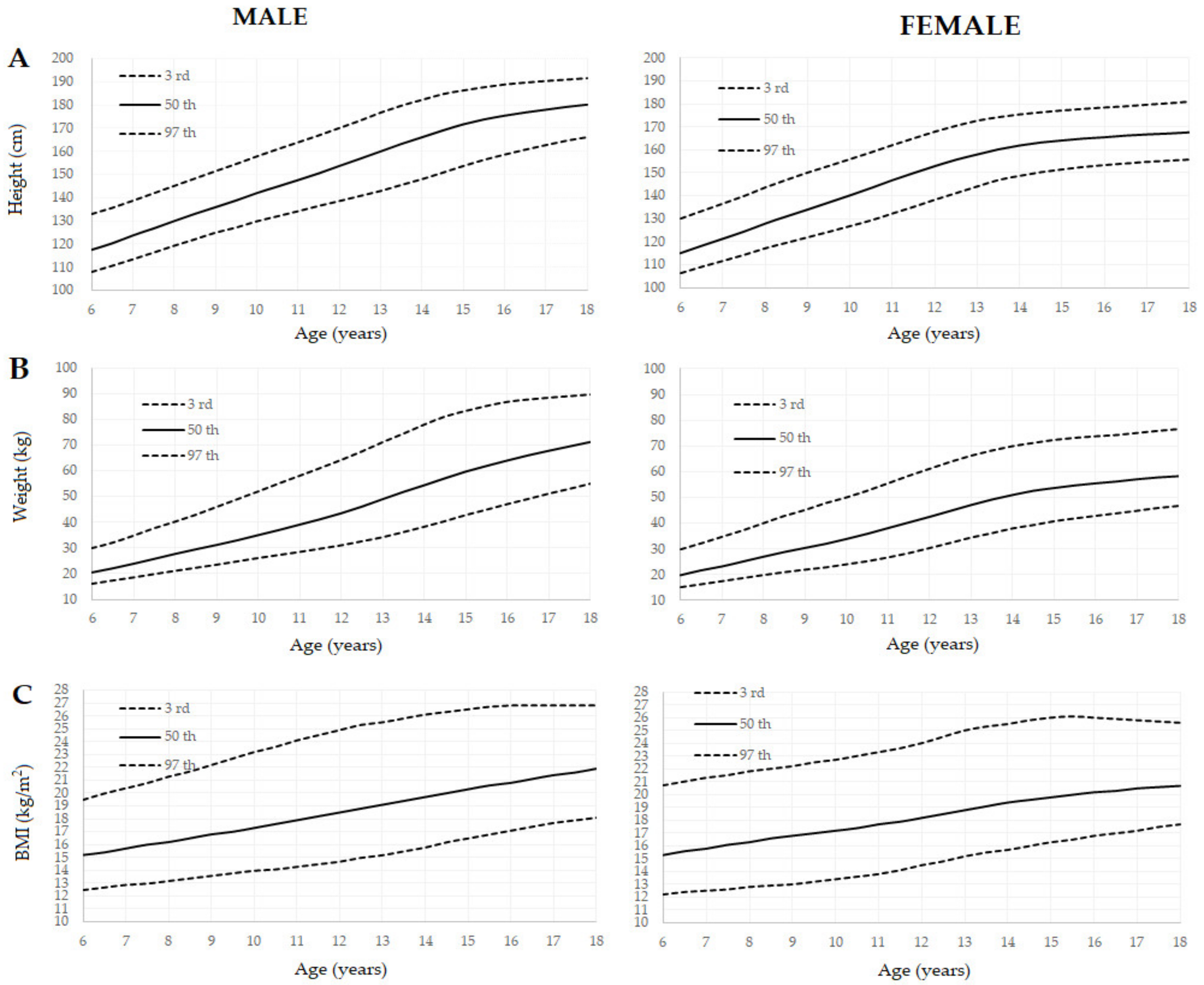
3.2. Growth Charts
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Consideration of the Evidence on Childhood Obesity for the Commission on Ending Childhood Obesity: Report of the ad hoc Working Group on Science and Evidence for Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 20 October 2019).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Abrignani, M.G.; Lucà, F.; Favilli, S.; Benvenuto, M.; Rao, C.M.; Di Fusco, S.A.; Gabrielli, D.; Gulizia, M.M.; Cardiovascular Prevention Area; Young Cardiologists Area; et al. Lifestyles and Cardiovascular Prevention in Childhood and Adolescence. Pediatr. Cardiol. 2019, 40, 1113–1125. [Google Scholar] [CrossRef] [PubMed]
- Stoner, L.; Rowlands, D.; Morrison, A.; Credeur, D.; Hamlin, M.; Gaffney, K.; Lambrick, D.; Matheson, A. Efficacy of Exercise Intervention for Weight Loss in Overweight and Obese Adolescents: Meta-Analysis and Implications. Sports Med. 2016, 46, 1737–1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019, 23, CD001871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicente-Rodríguez, G.; Benito, P.J.; Casajús, J.A.; Ara, I.; Aznar, S.; Castillo, M.J.; Dorado, C.; González-Agüero, A.; González-Gallego, J.; González-Gross, M.; et al. Physical activity, exercise and sport practice to fight against youth and childhood obesity. Nutr. Hosp. 2016, 33, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Weintraub, D.L.; Tirumalai, E.C.; Haydel, K.F.; Fujimoto, M.; Fulton, J.E.; Robinson, T.N. Team sports for overweight children: The Stanford Sports to Prevent Obesity Randomized Trial (SPORT). Arch. Pediatr. Adolesc. Med. 2008, 162, 232–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.E.; Pope, Z.; Gao, Z. The Role of Youth Sports in Promoting Children’s Physical Activity and Preventing Pediatric Obesity: A Systematic Review. Behav. Med. 2018, 44, 62–76. [Google Scholar] [CrossRef] [PubMed]
- Vella, S.A.; Cliff, D.P. Organised sports participation and adiposity among a cohort of adolescents over a two year period. PLoS ONE 2018, 13, e0206500. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Basso, C.; Schiavon, M.; Pelliccia, A.; Thiene, G. Preparticipation screening of young competitive athletes for prevention of sudden cardiac death. J. Am. Coll. Cardiol. 2008, 52, 1981–1989. [Google Scholar] [CrossRef] [PubMed]
- Cacciari, E.; Milani, S.; Balsamo, A.; Dammacco, F.; De Luca, F.; Chiarelli, F.; Pasquino, A.M.; Tonini, G.; Vanelli, M. Italian cross-sectional growth charts for height, weight and BMI (6–20 y). Eur. J. Clin. Nutr. 2002, 56, 171–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biffi, A.; Delise, P.; Zeppilli, P.; Giada, F.; Pelliccia, A.; Penco, M.; Casasco, M.; Colonna, P.; D’Andrea, A.; D’Andrea, L.; et al. Italian cardiological guidelines for sports eligibility in athletes with heart disease: Part 1. J. Cardiovasc. Med. 2013, 14, 477–499. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Green, P.J. Smoothing reference centile curves: The LMS method and penalized likelihood. Stat. Med. 1992, 11, 1305–1319. [Google Scholar] [CrossRef] [PubMed]
- Rigby, R.A.; Stasinopoulos, D.M. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat. Med. 2004, 23, 3053–3076. [Google Scholar] [CrossRef] [PubMed]
- Indagine “Aspetti della vita quotidiana”—Anno 2016. Available online: https://www.istat.it/it/archivio/202040 (accessed on 11 October 2019).
- Nardone, P.; Spinelli, A.; Buoncristiano, M.; Lauria, L.; Pierannunzio, D.; Galeone, D. Il Sistema di sorveglianza OKkio alla SALUTE: Risultati 2016. Available online: https://www.epicentro.iss.it/okkioallasalute/pdf/ONLINE_OKKIO_ALLA_SALUTE.pdf (accessed on 20 October 2019).
- Sistema di Sorveglianza HBSC Health Behaviour in School-aged Children. RISULTATI DELLA RILEVAZIONE 2018. Available online: https://www.epicentro.iss.it/hbsc/pdf/sovrappeso%20e%20obesit%C3%A0.pdf (accessed on 10 November 2019).
- Vella, S.A.; Cliff, D.P.; Okely, A.D.; Scully, M.L.; Morley, B.C. Associations between sports participation, adiposity and obesity-related health behaviors in Australian adolescents. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khudairy, L.; Loveman, E.; Colquitt, J.L.; Mead, E.; Johnson, R.E.; Fraser, H.; Olajide, J.; Murphy, M.; Velho, R.M.; O’Malley, C.; et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 2017, 6, CD012691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lorenzo, A.; Gratteri, S.; Gualtieri, P.; Cammarano, A.; Bertucci, P.; Di Renzo, L. Why primary obesity is a disease? J. Transl. Med. 2019, 17, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carl, R.L.; Johnson, M.D.; Martin, T.J. Council on Sports Medicine and Fitness. Promotion of Healthy Weight-Control Practices in Young Athletes. Pediatrics 2017, 140, e20171871. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Sample | Normal Weight | Overweight | Obese | ||||
|---|---|---|---|---|---|---|---|
| Age | n. | % | n. | % | n. | % | n. |
| 6 | 189 | 88.9 | 168 | 8.5 | 16 | 2.6 | 5 |
| 7 | 135 | 83.7 | 113 | 13.3 | 18 | 2.9 | 4 |
| 8 | 166 | 80.7 | 134 | 16.7 | 28 | 2.4 | 4 |
| 9 | 242 | 82.6 | 200 | 14.9 | 36 | 2.5 | 6 |
| 10 | 436 | 84.6 | 369 | 14.4 | 63 | 0.9 | 4 |
| 11 | 675 | 83.3 | 562 | 15.1 | 102 | 1.6 | 11 |
| 12 | 1567 | 83.8 | 1313 | 14.5 | 227 | 1.7 | 27 |
| 13 | 1631 | 85.6 | 1396 | 12.8 | 208 | 1.7 | 27 |
| 14 | 1618 | 86.5 | 1399 | 12.1 | 195 | 1.5 | 24 |
| 15 | 1611 | 87.8 | 1415 | 10.8 | 174 | 1.4 | 22 |
| 16 | 1524 | 88.2 | 1344 | 10.7 | 163 | 1.1 | 17 |
| 17 | 675 | 91.4 | 617 | 7.7 | 52 | 0.9 | 6 |
| 10,469 | 86.3 | 9038 | 12.3 | 1274 | 1.5 | 157 | |
| Total Sample | Normal Weight | Overweight | Obese | ||||
|---|---|---|---|---|---|---|---|
| Age | n. | % | n. | % | n. | % | n. |
| 6 | 122 | 82.8 | 101 | 10.7 | 13 | 6.6 | 8 |
| 7 | 88 | 77.3 | 68 | 14.8 | 13 | 6.8 | 6 |
| 8 | 141 | 75.9 | 107 | 16.3 | 23 | 3.5 | 5 |
| 9 | 192 | 83.3 | 160 | 14.6 | 28 | 2.1 | 4 |
| 10 | 295 | 86.1 | 254 | 13.6 | 40 | 0.3 | 1 |
| 11 | 426 | 89.2 | 380 | 10.6 | 45 | 0.2 | 1 |
| 12 | 613 | 88.2 | 541 | 11.1 | 68 | 0.7 | 4 |
| 13 | 626 | 90.4 | 566 | 9.1 | 57 | 0.5 | 3 |
| 14 | 590 | 91.3 | 539 | 8.0 | 47 | 0.7 | 4 |
| 15 | 495 | 90.3 | 447 | 8.3 | 41 | 1.4 | 7 |
| 16 | 436 | 95.1 | 415 | 6.0 | 25 | 0.5 | 2 |
| 17 | 207 | 93.7 | 194 | 5.8 | 12 | 0.5 | 1 |
| Total | 4231 | 89.1 | 3772 | 9.8 | 413 | 1.1 | 46 |
| Male | Female | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Height (cm) | Weight (kg) | BMI (kg/m2) | Height (cm) | Weight (kg) | BMI (kg/m2) | |||||||||||||
| Age (yrs) | 3rd | 50th | 97th | 3rd | 50th | 97th | 3rd | 50th | 97th | 3rd | 50th | 97th | 3rd | 50th | 97th | 3rd | 50th | 97th |
| 6 | 107.8 | 117.5 | 132.8 | 15.9 | 20.5 | 30.1 | 12.5 | 15.2 | 19.5 | 106.1 | 115 | 130.3 | 15.0 | 19.8 | 29.9 | 12.2 | 15.3 | 20.7 |
| 6.5 | 110.5 | 120.3 | 135.5 | 17.2 | 22.1 | 32.2 | 12.7 | 15.4 | 20.0 | 108.9 | 118.2 | 133.6 | 16.2 | 21.7 | 32.3 | 12.4 | 15.6 | 21.0 |
| 7 | 113.3 | 123.7 | 138.6 | 18.4 | 23.9 | 34.9 | 12.9 | 15.7 | 20.4 | 111.5 | 121.3 | 136.8 | 17.4 | 23.2 | 34.8 | 12.5 | 15.8 | 21.3 |
| 7.5 | 116.2 | 126.7 | 141.8 | 19.7 | 25.8 | 37.8 | 13.0 | 16.0 | 20.8 | 114.1 | 124.4 | 140.1 | 18.6 | 25.1 | 37.3 | 12.6 | 16.1 | 21.5 |
| 8 | 119.2 | 129.9 | 145.0 | 21.0 | 27.7 | 40.3 | 13.2 | 16.2 | 21.3 | 117.0 | 127.9 | 143.8 | 19.8 | 27.0 | 40.1 | 12.8 | 16.3 | 21.8 |
| 8.5 | 122.0 | 133.0 | 148.2 | 22.2 | 29.5 | 43.0 | 13.4 | 16.5 | 21.7 | 119.4 | 131.0 | 147.1 | 20.9 | 28.8 | 42.9 | 12.9 | 16.6 | 22.0 |
| 9 | 124.9 | 135.9 | 151.4 | 23.4 | 31.2 | 46.0 | 13.6 | 16.8 | 22.2 | 121.8 | 134.0 | 150.2 | 21.9 | 30.4 | 45.2 | 13.0 | 16.8 | 22.2 |
| 9.5 | 127.1 | 138.8 | 154.5 | 24.7 | 33.0 | 49.0 | 13.8 | 17.0 | 22.7 | 124.2 | 137.1 | 153.1 | 22.8 | 32.0 | 47.9 | 13.2 | 17.0 | 22.5 |
| 10 | 129.8 | 142.0 | 157.8 | 26.0 | 35.0 | 52.0 | 14.0 | 17.3 | 23.2 | 126.7 | 140.2 | 156.0 | 24.0 | 33.9 | 50.1 | 13.4 | 17.2 | 22.7 |
| 10.5 | 132.0 | 144.8 | 160.9 | 27.2 | 37.0 | 55.1 | 14.1 | 17.6 | 23.6 | 129.2 | 143.4 | 159.0 | 25.2 | 35.9 | 52.7 | 13.6 | 17.4 | 23.0 |
| 11 | 134.2 | 147.6 | 163.9 | 28.4 | 39.1 | 58.1 | 14.3 | 17.9 | 24.1 | 132.2 | 146.8 | 162.1 | 26.7 | 38.1 | 55.6 | 13.8 | 17.7 | 23.3 |
| 11.5 | 136.5 | 150.5 | 166.9 | 29.7 | 41.2 | 61.1 | 14.5 | 18.2 | 24.5 | 135.1 | 149.9 | 165.0 | 28.4 | 40.3 | 58.5 | 14.1 | 17.9 | 23.6 |
| 12 | 138.6 | 153.7 | 170.1 | 31.0 | 43.5 | 64.2 | 14.7 | 18.5 | 24.9 | 138.2 | 152.9 | 167.9 | 30.4 | 42.5 | 61.2 | 14.5 | 18.2 | 24.0 |
| 12.5 | 140.8 | 156.8 | 173.3 | 32.6 | 46.1 | 67.5 | 15.0 | 18.8 | 25.3 | 141.1 | 155.7 | 170.4 | 32.4 | 44.8 | 63.9 | 14.8 | 18.5 | 24.5 |
| 13 | 143.0 | 160.0 | 176.8 | 34.2 | 49.0 | 71.1 | 15.2 | 19.1 | 25.5 | 144.0 | 158.0 | 172.6 | 34.5 | 47.1 | 66.3 | 15.2 | 18.8 | 25.0 |
| 13.5 | 145.6 | 163.2 | 179.8 | 36.2 | 51.8 | 74.4 | 15.5 | 19.4 | 25.8 | 146.8 | 160.2 | 174.1 | 36.2 | 49.2 | 68.3 | 15.5 | 19.1 | 25.3 |
| 14 | 148.1 | 166.1 | 182.3 | 38.3 | 54.4 | 77.9 | 15.8 | 19.7 | 26.1 | 148.6 | 161.9 | 175.3 | 38.1 | 51.0 | 70.0 | 15.7 | 19.4 | 25.5 |
| 14.5 | 150.9 | 169.0 | 184.8 | 40.5 | 57.1 | 81.0 | 16.2 | 20.0 | 26.3 | 150.2 | 163.2 | 176.2 | 39.4 | 52.6 | 71.2 | 16.0 | 19.6 | 25.8 |
| 15 | 153.8 | 171.7 | 186.4 | 42.9 | 59.7 | 83.2 | 16.5 | 20.3 | 26.5 | 151.4 | 164.1 | 177.0 | 40.9 | 53.7 | 72.4 | 16.3 | 19.8 | 26.0 |
| 15.5 | 156.5 | 173.8 | 187.8 | 45.0 | 61.9 | 85.1 | 16.8 | 20.6 | 26.7 | 152.5 | 164.9 | 177.7 | 42.0 | 54.7 | 73.2 | 16.5 | 20.0 | 26.1 |
| 16 | 158.8 | 175.4 | 189.0 | 47.2 | 64.0 | 86.7 | 17.1 | 20.8 | 26.8 | 153.3 | 165.5 | 178.3 | 43.0 | 55.5 | 73.8 | 16.8 | 20.2 | 26.0 |
| 16.5 | 160.9 | 176.8 | 189.8 | 49.2 | 66.0 | 87.6 | 17.4 | 21.1 | 26.8 | 154.0 | 166.2 | 178.8 | 44.0 | 56.2 | 74.3 | 17.0 | 20.3 | 25.9 |
| 17 | 162.9 | 178.0 | 190.5 | 51.3 | 67.8 | 88.3 | 17.7 | 21.4 | 26.8 | 154.7 | 166.7 | 179.5 | 45.0 | 57.1 | 75.1 | 17.2 | 20.5 | 25.8 |
| 17.5 | 164.8 | 179.2 | 191.1 | 53.2 | 69.5 | 88.9 | 17.9 | 21.6 | 26.8 | 155.2 | 167.1 | 180.1 | 46.1 | 57.8 | 75.9 | 17.5 | 20.6 | 25.7 |
| 18 | 166.3 | 180.2 | 191.7 | 55.2 | 71.2 | 89.5 | 18.1 | 21.9 | 26.8 | 155.7 | 167.6 | 180.8 | 46.9 | 58.3 | 76.6 | 17.7 | 20.7 | 25.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mascherini, G.; Galanti, G.; Massetti, L.; Calà, P.; Modesti, P.A. Growth Charts for Height, Weight, and BMI (6–18 y) for the Tuscany Youth Sports Population. Int. J. Environ. Res. Public Health 2019, 16, 4975. https://doi.org/10.3390/ijerph16244975
Mascherini G, Galanti G, Massetti L, Calà P, Modesti PA. Growth Charts for Height, Weight, and BMI (6–18 y) for the Tuscany Youth Sports Population. International Journal of Environmental Research and Public Health. 2019; 16(24):4975. https://doi.org/10.3390/ijerph16244975
Chicago/Turabian StyleMascherini, Gabriele, Giorgio Galanti, Luciano Massetti, Piergiuseppe Calà, and Pietro Amedeo Modesti. 2019. "Growth Charts for Height, Weight, and BMI (6–18 y) for the Tuscany Youth Sports Population" International Journal of Environmental Research and Public Health 16, no. 24: 4975. https://doi.org/10.3390/ijerph16244975