Does the Electronic Health Card for Asylum Seekers Lead to an Excessive Use of the Health System? Results of a Survey in Two Municipalities of the German Ruhr Area


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Asylum Seekers
3.2. Reference Population
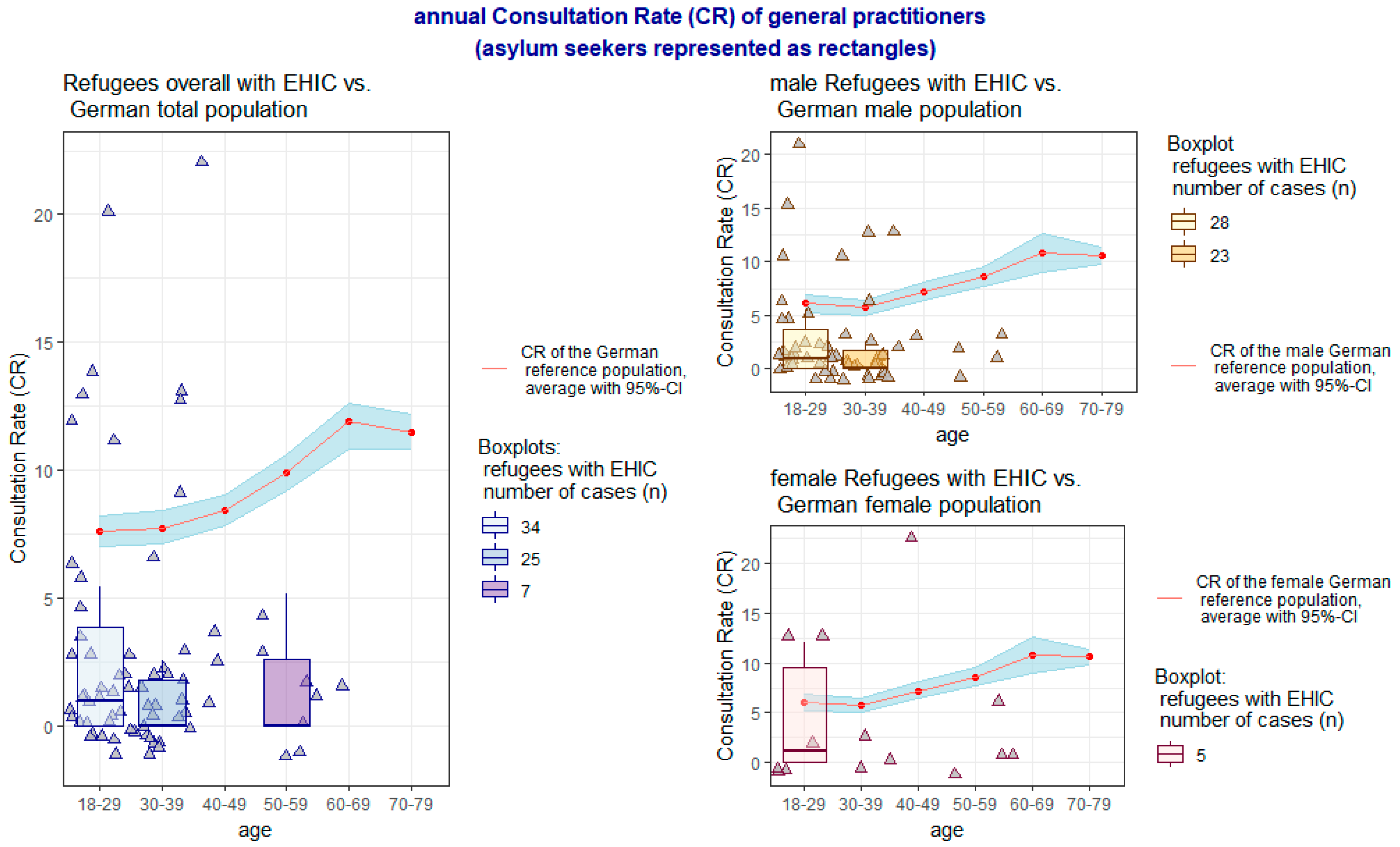
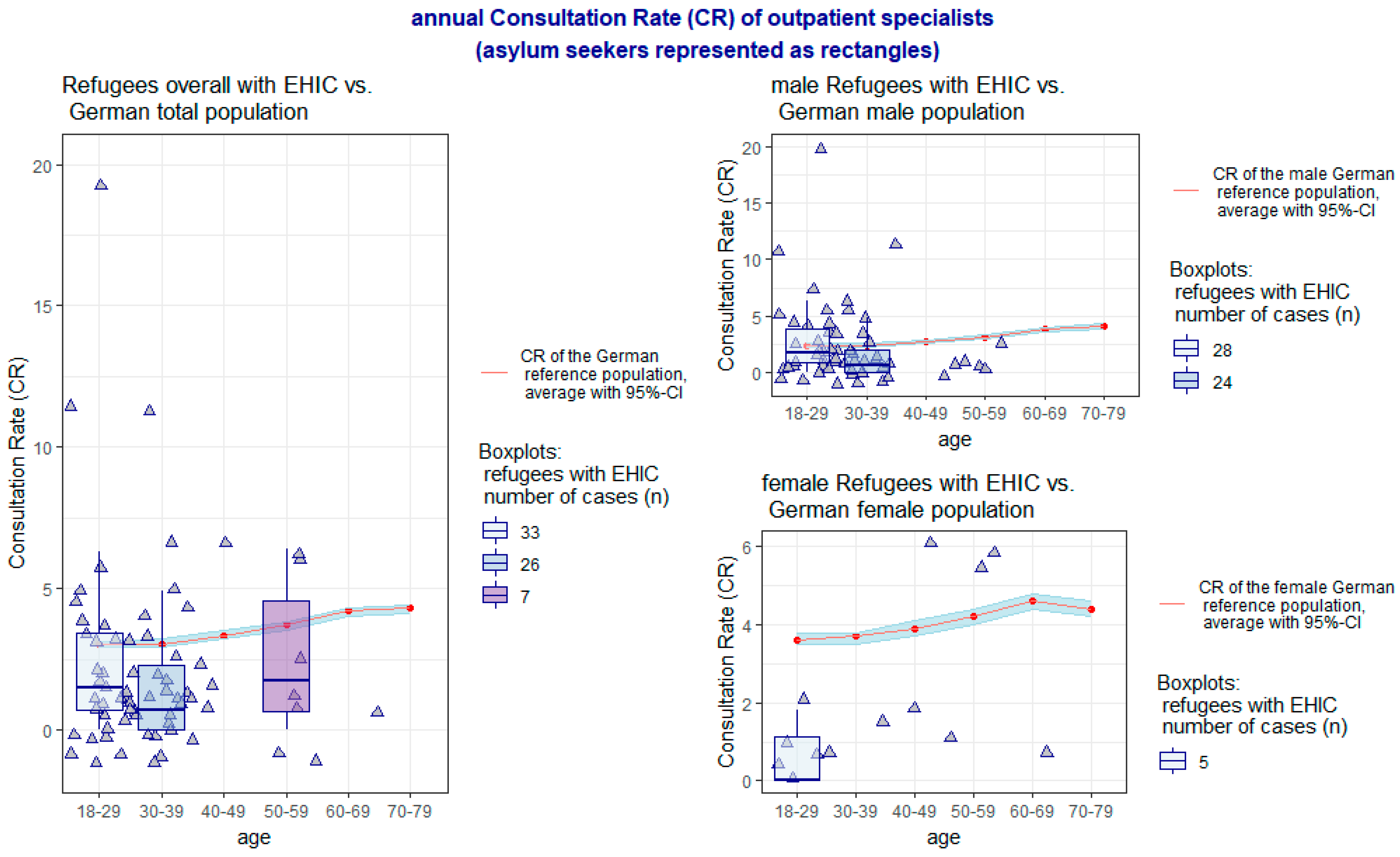
3.3. Comparison
4. Discussion
Scientific Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| EHIC | Electronic Health Insurance Card |
| CR | Consultation Rate of Ambulant Physicians |
| RKI | Robert-Koch-Institute |
| DEGS-1 | German Health Interview and Examination Survey for Adults |
| NA | Not available |
| CI | Confidence Interval |
References
- Bundeszentrale für Politische Bildung Zahlen zu Asyl in Deutschland | bpb. Available online: http://www.bpb.de/gesellschaft/migration/flucht/218788/zahlen-zu-asyl-in-deutschland (accessed on 7 December 2018).
- BAMF (Bundesamt für Migration und Flüchtlinge) Initial Distribution of Asylum-Seekers. Available online: http://www.bamf.de/EN/Fluechtlingsschutz/AblaufAsylv/Erstverteilung/erstverteilung-node.html;jsessionid=9854D42FF92D33FEAB977159352F9F0E.2_cid286 (accessed on 7 December 2018).
- Kury, H.; Redo, S. Refugees and Migrants in Law and Policy: Challenges and Opportunities for Global Civic Education; Springer International Publishing: Berlin, Germany, 2018; ISBN 978-3-319-72158-3. [Google Scholar]
- Landeszentrale für Politische Bildung Baden-Württemberg Flüchtlinge in Deutschland. Available online: https://www.lpb-bw.de/fluechtlingsproblematik.html (accessed on 7 December 2018).
- Statista Europa: Flüchtlinge pro Einwohner in den Ländern der EU | Statistik. Available online: https://de.statista.com/statistik/daten/studie/156549/umfrage/asylbewerber-in-europa-2010/ (accessed on 7 December 2018).
- Statista • Chart: Lebanon Still Has the Highest Refugees Density. Available online: https://www.statista.com/chart/14323/countries-with-most-refugees-per-1000-inhabitants/ (accessed on 7 December 2018).
- Sola, A. The 2015 Refugee Crisis in Germany: Concerns about Immigration and Populism; The German Socio-Economic Panel Study; DIW: Berlin, Germany, 2018. [Google Scholar]
- Claassen, K.; Jäger, P. Impact of the Introduction of the Electronic Health Insurance Card on the Use of Medical Services by Asylum Seekers in Germany. Int. J. Environ. Res. Public Health 2018, 15, 856. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.; Yesil-Jürgens, R.; Razum, O.; Bozorgmehr, K.; Schenk, L.; Gilsdorf, A.; Rommel, A.; Lampert, T. Health and healthcare provision to asylum seekers and refugees in Germany. Zeitschriftenartikel 2017. [Google Scholar] [CrossRef]
- Hyde, R. Refugees need health cards, say German doctors. Lancet 2016, 388, 646–648. [Google Scholar] [CrossRef]
- Mehr Flüchtlinge Erhalten Gesundheitskarte. Available online: https://www.aerzteblatt.de/nachrichten/72619/Mehr-Fluechtlinge-erhalten-Gesundheitskarte (accessed on 7 December 2018).
- Bozorgmehr, K.; Razum, O. Effect of Restricting Access to Health Care on Health Expenditures among Asylum-Seekers and Refugees: A Quasi-Experimental Study in Germany, 1994–2013. PLoS ONE 2015, 10, e0131483. [Google Scholar] [CrossRef]
- Frisch, J. Angst vor Missbrauch: Kommunen Blockieren Gesundheitskarte. Available online: https://www.aerztezeitung.de/politik_gesellschaft/gp_specials/fluechtlinge/article/913018/angst-missbrauch-kommunen-blockieren-gesundheitskarte.html (accessed on 7 December 2018).
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Rattay, P.; Butschalowsky, H.; Rommel, A.; Prütz, F.; Jordan, S.; Nowossadeck, E.; Domanska, O. Utilisation of outpatient and inpatient health services in Germany. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013, 56, 832–844. [Google Scholar] [CrossRef] [PubMed]
- Braun, C.T.; Gnägi, C.R.; Klingberg, K.; Srivastava, D.; Ricklin, M.E.; Exadaktylos, A.K. Migrationsspezifische Aspekte des Patientengutes einer grossen europäischen universitären Notaufnahme über einen Zeitraum von zehn Jahren. Praxis 2017, 106, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Robert-Koch-Institut (RKI). Migration und Gesundheit; RKI: Berlin, Germnay, 2008. [Google Scholar]
- Schneider, C.; Joos, S.; Bozorgmehr, K. Disparities in health and access to healthcare between asylum seekers and residents in Germany: A population-based cross-sectional feasibility study. BMJ Open 2015, 5, e008784. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Groups | 18–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 |
|---|---|---|---|---|---|---|
| Absolute number | 60 | 45 | 13 | 9 | 1 | 0 |
| Hereof men absolute, (%) | 52, (86.67%) | 39, (86.67%) | 9, (69.23%) | 6, (66.67%) | 0 | 0 |
| Presence of chronic diseases (any) | 19, (32.20%), (1 NA) | 14, (31.11%) | 8, (61.54%) | 6, (66.67%) | 1, (100%) | NA |
| Mean CR/year of general practitioners (95% CI), (number of NA) | 3.18, (1.44–4.91), n = 34, (26 NA) | 2.06, (0.48–3.65), n = 26, (19 NA) | 7.29, (−9.39–23.97), n = 4, (9 NA), (1 outlier) | 1.48, (−0.40–3.35), n = 7 (2 NA) | 1.8, n = 1, (0 NA) | NA |
| Mean CR/year of outpatient specialists (95% CI), (number of NA) | 2.63, (1.24–4.01), n = 33, (27 NA) | 1.78, (0.69–2.86), n = 26 (19 NA) | 2.66, (−1.0–6.31), n = 4, (9 NA), (1 outlier) | 2.65, (0.23–5.10), n = 7, (2 NA) | 0, n = 1, (0 NA) | NA |
| Use of inpatient services at least one/year in %, n, (NA) | 26.92, n = 34, (26 NA) | 26.81, n = 26, (19 NA) | 24.63, n = 4, (9 NA) | 36.73, n = 7, (2 NA) | 60.0, n = 1, (0 NA) | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jäger, P.; Claassen, K.; Ott, N.; Brand, A. Does the Electronic Health Card for Asylum Seekers Lead to an Excessive Use of the Health System? Results of a Survey in Two Municipalities of the German Ruhr Area. Int. J. Environ. Res. Public Health 2019, 16, 1178. https://doi.org/10.3390/ijerph16071178
Jäger P, Claassen K, Ott N, Brand A. Does the Electronic Health Card for Asylum Seekers Lead to an Excessive Use of the Health System? Results of a Survey in Two Municipalities of the German Ruhr Area. International Journal of Environmental Research and Public Health. 2019; 16(7):1178. https://doi.org/10.3390/ijerph16071178
Chicago/Turabian StyleJäger, Pia, Kevin Claassen, Notburga Ott, and Angela Brand. 2019. "Does the Electronic Health Card for Asylum Seekers Lead to an Excessive Use of the Health System? Results of a Survey in Two Municipalities of the German Ruhr Area" International Journal of Environmental Research and Public Health 16, no. 7: 1178. https://doi.org/10.3390/ijerph16071178