Delphi Method to Achieve Clinical Consensus for a BPMN Representation of the Central Venous Access Placement for Training Purposes

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
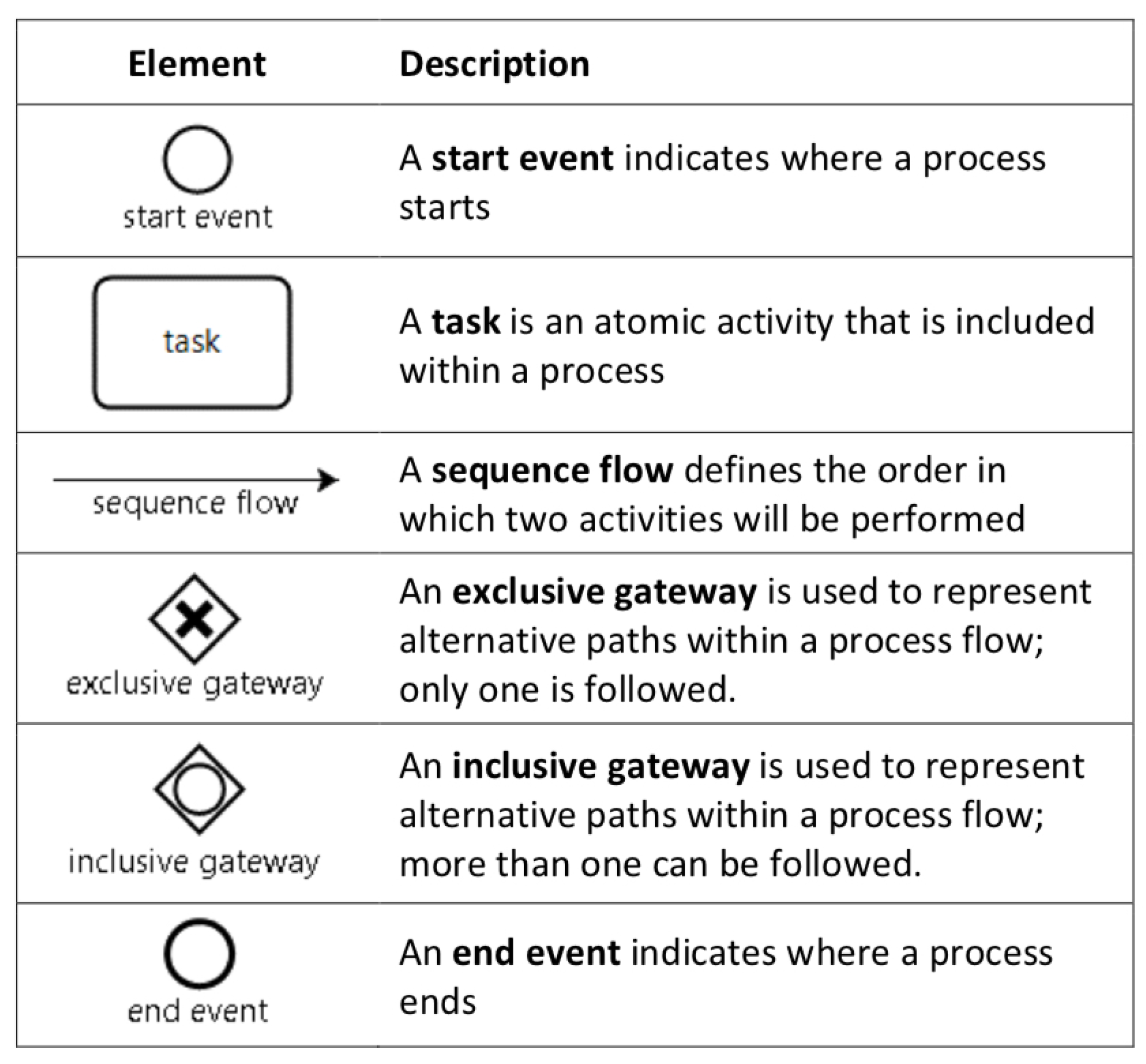
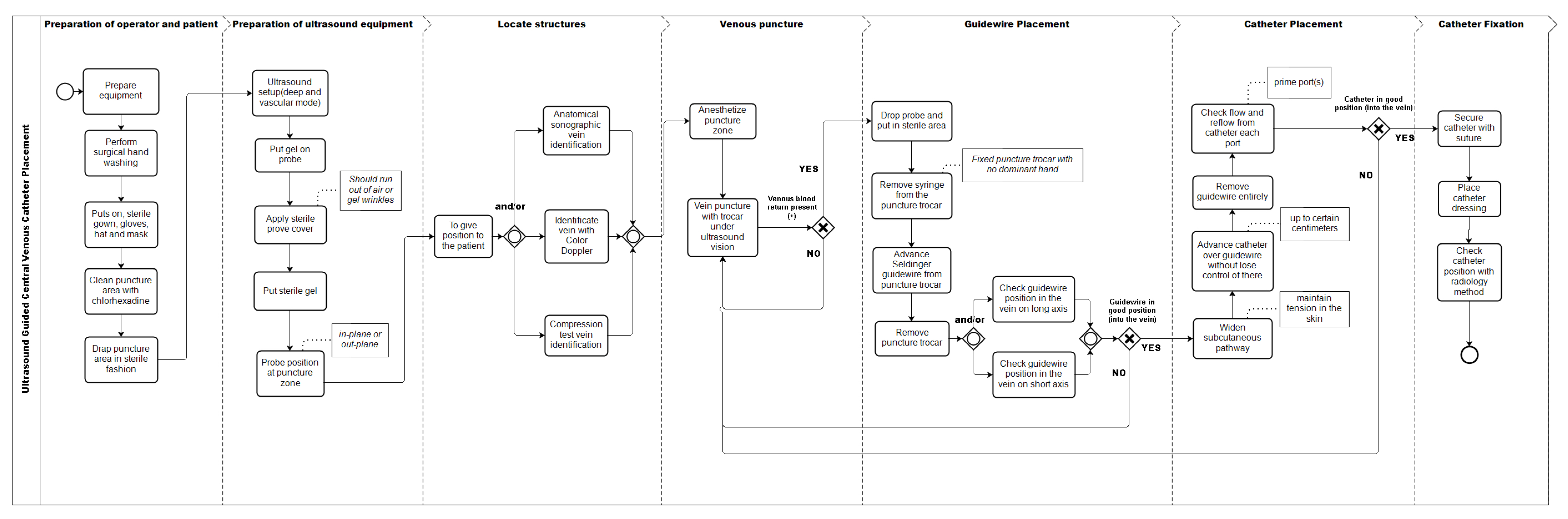
2.1. Development of an Initial Process Model of Ultrasound Guided CVC Placement
2.2. Consensus through the Delphi Method
- Display of the proposed BPMN model (Supplementary Figure S1).
- Personal data acquisition: specialty, work area, contact data.
- Set of structured questions, where all the activities of the previously defined BPMN model are listed sequentially. Each question describes the activity and asks each expert to weigh the appropriateness of its inclusion in the model, based on a 5-point Likert scale: 1. Under no circumstances should be included, 2. Should not be included, 3. May or may not be included, 4. Should be included, 5. Must be included.
- Addition of new activities not included in the proposed model, defining the place they should occupy in the model.
- Proposal of other experts in the ultrasound guided CVC placement, who could participate in the research.
3. Results
3.1. Experts
3.2. Model
- Five were included as new activities in the second survey.
- Five activities already considered were modified, either by redefining an activity or by adding some qualitative attribute.
- Four activities were not included because they escaped the scope of the model (e.g., catheter tunneling, or avoiding the patient taking deep breaths).
- Of the three alternatives proposed as activities to verify the position of the vein with ultrasonography before puncture (Anatomical identification, compression, or use of Doppler), none reached the inclusion threshold. When analyzed as a whole, 92% of respondents used at least one of these three alternatives, so it was decided to include all the possibilities in the graphic model.
- “Check catheter in the vein with ultrasound in short axis” inside the vein lumen, obtained 67% on the inclusion criterion; and “Check catheter in the vein with ultrasound in long axis”, obtained 75%. Therefore, it was decided to include both as variants of the same activity.
- The activity “Put sterile gel on covered transducer” did not reach the inclusion criterion. However, we considered that the way the item was worded was incorrect, given that the sterile gel is sometimes used on the puncture site to generate an interface that avoids the presence of air and not necessarily on the transducer. This could have caused confusion among the experts. Therefore, we modified its name to “Put sterile gel” and included it as such in the final model.
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| CVC | Central Venous Catheter |
| BPMN | Business Process Model and Notation |
| CTA | Cognitive Task Analysis |
| ICSAD | Imperial College Surgical Assessment Device |
References
- Fecso, A.B.; Szasz, P.; Kerezov, G.; Grantcharov, T.P. The Effect of Technical Performance on Patient Outcomes in Surgery. Ann. Surg. 2017, 265, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Leape, L.L.; Brennan, T.A.; Laird, N.; Lawthers, A.G.; Localio, A.R.; Barnes, B.A.; Hebert, L.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N. Engl. J. Med. 1991, 324, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, D.A.; Brydges, R.; Zendejas, B.; Hamstra, S.J.; Hatala, R. Mastery Learning for Health Professionals Using Technology-enhanced Simulation: A Systematic Review and Meta-analysis. Acad. Med. 2013, 88, 1178–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barsuk, J.H.; Ahya, S.N.; Cohen, E.R.; McGaghie, W.C. Mastery learning of temporary hemodialysis catheter insertion by nephrology fellows using simulation technology and deliberate practice. Am. J. 2009, 54, 70–76. [Google Scholar] [CrossRef]
- Grantcharov, T.P.; Reznick, R.K. Teaching procedural skills. BMJ 2008, 336, 1129–1131. [Google Scholar] [CrossRef]
- Sullivan, M.E.; Yates, K.A.; Inaba, K.; Lam, L.; Clark, R.E. The Use of Cognitive Task Analysis to Reveal the Instructional Limitations of Experts in the Teaching of Procedural Skills. Acad. Med. 2014, 89, 811–816. [Google Scholar] [CrossRef]
- Clark, R.E.; Pugh, C.M.; Yates, K.A.; Inaba, K.; Green, D.J.; Sullivan, M.E. The Use of Cognitive Task Analysis to Improve Instructional Descriptions of Procedures. J. Surg. Res. 2012, 173, e37–e42. [Google Scholar] [CrossRef]
- Yates, K.A.; Feldon, D.F. Advancing the practice of cognitive task analysis: A call for taxonomic research. Theor. Issues Ergon. Sci. 2011, 12, 472–495. [Google Scholar] [CrossRef]
- Wingfield, L.R.; Kulendran, M.; Chow, A.; Nehme, J.; Purkayastha, S. Cognitive Task Analysis: Bringing Olympic Athlete Style Training to Surgical Education. Surg. Innov. 2015, 22, 406–417. [Google Scholar] [CrossRef]
- Boehler, M.L.; Roberts, N.; Sanfey, H.; Mellinger, J. Do Surgeons and Gastroenterologists Describe Endoscopic Retrograde Cholangiopancreatography Differently? A Qualitative Study. J. Surg. Educ. 2016, 73, 66–72. [Google Scholar] [CrossRef]
- Object Management Group. Business Process Model and Notation™ (Bpmn™) Version 2.0; Object Management Group: Needham, MA, USA, 2011; Available online: https://www.omg.org/spec/BPMN/2.0/PDF (accessed on 3 January 2020).
- Dumas, M.; La Rosa, M.; Mendling, J.; Reijers, H.A. Fundamentals of Business Process Management; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Scheuerlein, H.; Rauchfuss, F.; Dittmar, Y.; Molle, R.; Lehmann, T.; Pienkos, N.; Settmacher, U. New methods for clinical pathways-Business Process Modeling Notation (BPMN) and Tangible Business Process Modeling (t.BPM). Langenbeck’s Arch. Surg. 2012, 397, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Rolón, E.; Chavira, G.; Orozco, J.; Soto, J.P. Towards a Framework for Evaluating Usability of Business Process Models with BPMN in Health Sector. Procedia Manuf. 2015, 3, 5603–5610. [Google Scholar] [CrossRef] [Green Version]
- Lenz, R.; Blaser, R.; Beyer, M.; Heger, O.; Biber, C.; Bäumlein, M.; Schnabel, M. IT support for clinical pathways–lessons learned. Int. J. Med. Inform. 2007, 76 (Suppl. 3), S397–S402. [Google Scholar] [CrossRef] [PubMed]
- Shitkova, M.; Taratukhin, V.; Becker, J. Towards a Methodology and a Tool for Modeling Clinical Pathways. Procedia Comput. Sci. 2015, 63, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, F.; Garcia, F.; Calahorra, L.; Llorente, C. Business process modeling in healthcare. Stud. Health Technol. Inform. 2012, 179, 75–87. [Google Scholar]
- Dobson, G.; Chong, M.; Chow, L.; Flexman, A.; Kurrek, M.; Laflamme, C.; Lagacé, A.; Stacey, S.; Thiessen, B. Guidelines to the Practice of Anesthesia—Revised Edition 2018. Can. J. Anaesth. 2018, 65, 76–104. [Google Scholar] [CrossRef] [Green Version]
- Madenci, A.L.; Solis, C.V.; de Moya, M.A. Central venous access by trainees: A systematic review and meta-analysis of the use of simulation to improve success rate on patients. Simul. Healthc. J. Soc. Simul. Healthc. 2014, 9, 7–14. [Google Scholar] [CrossRef]
- Barsuk, J.H.; Cohen, E.R.; Feinglass, J.; McGaghie, W.C.; Wayne, D.B. Use of Simulation-Based Education to Reduce Catheter-Related Bloodstream Infections. Arch. Intern. Med. 2009, 169, 1420–1423. [Google Scholar] [CrossRef] [Green Version]
- Ma, I.W.Y.; Brindle, M.E.; Ronksley, P.E.; Lorenzetti, D.L.; Sauve, R.S.; Ghali, W.A. Use of Simulation-based Education to Improve Outcomes of Central Venous Catheterization: A Systematic Review and Meta-analysis. Acad. Med. 2011, 86, 1137–1147. [Google Scholar] [CrossRef]
- Cohen, E.R.; Feinglass, J.; Barsuk, J.H.; Barnard, C.; O’Donnell, A.; McGaghie, W.C.; Wayne, D.B. Cost savings from reduced catheter-related bloodstream infection after simulation-based education for residents in a medical intensive care unit. Simul. Healthc. J. Soc. Simul. Healthc. 2010, 5, 98–102. [Google Scholar] [CrossRef]
- Nguyen, B.V.; Prat, G.; Vincent, J.L.; Nowak, E.; Bizien, N.; Tonnelier, J.M.; Renault, A.; Ould-Ahmed, M.; Boles, J.M.; L’Her, E. Determination of the learning curve for ultrasound-guided jugular central venous catheter placement. Intensive Care Med. 2013, 40, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Hind, D.; Calvert, N.; McWilliams, R.; Davidson, A.; Paisley, S.; Beverley, C.; Thomas, S. Ultrasonic locating devices for central venous cannulation: Meta-analysis. BMJ 2003, 327, 361–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brass, P.; Hellmich, M.; Kolodziej, L.; Schick, G.; Smith, A.F. Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization. Cochrane Database Syst. Rev. 2015, 1, CD006962. [Google Scholar] [CrossRef] [PubMed]
- American Society of Anesthesiologists Task Force on Central Venous Access; Rupp, S.M.; Apfelbaum, J.L.; Blitt, C.; Caplan, R.A.; Connis, R.T.; Domino, K.B.; Fleisher, L.A.; Grant, S.; Mark, J.B.; et al. Practice guidelines for central venous access: A report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology 2012, 116, 539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKinley, R.K.; Strand, J.; Ward, L.; Gray, T.; Alun-Jones, T.; Miller, H. Checklists for assessment and certification of clinical procedural skills omit essential competencies: A systematic review. Med. Educ. 2008, 42, 338–349. [Google Scholar] [CrossRef]
- Ma, I.W.Y.; Zalunardo, N.; Pachev, G.; Beran, T.; Brown, M.; Hatala, R.; McLaughlin, K. Comparing the use of global rating scale with checklists for the assessment of central venous catheterization skills using simulation. Adv. Health Sci. Educ. 2011, 17, 457–470. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [PubMed] [Green Version]
- Mead, D.; Moseley, L. The use of the Delphi as a research approach. Nurse Res. 2001, 8, 4–23. [Google Scholar] [CrossRef]
- Okoli, C.; Pawlowski, S.D. The Delphi method as a research tool: An example, design considerations and applications. Inf. Manag. 2004, 42, 15–29. [Google Scholar] [CrossRef] [Green Version]
- Braun, R.; Schlieter, H.; Burwitz, M. Bpmn4cp: Design and implementation of a bpmn extension for clinical pathways. In Proceedings of the 2014 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Belfast, UK, 2–5 November 2014; pp. 9–16. [Google Scholar]
- Hales, B.; Terblanche, M.; Fowler, R.; Sibbald, W. Development of medical checklists for improved quality of patient care. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2008, 20, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Ma, I.W.; Sharma, N.; Brindle, M.E.; Caird, J.; McLaughlin, K. Measuring competence in central venous catheterization: A systematic-review. SpringerPlus 2014, 3, 33. [Google Scholar] [CrossRef] [Green Version]
- Neumuth, D.; Loebe, F.; Herre, H.; Neumuth, T. Modeling surgical processes: A four-level translational approach. Artif. Intell. Med. 2011, 51, 147–161. [Google Scholar] [CrossRef]
- Müller, R.; Rogge-Solti, A. BPMN for healthcare processes. In Proceedings of the 3rd Central-European Workshop on Services and their Composition (ZEUS 2011), Karlsruhe, Germany, 21–22 February 2011. [Google Scholar]
- Yeo, H.; Viola, K.; Berg, D.; Lin, Z.; Nunez-Smith, M.; Cammann, C.; Bell, R.H.; Sosa, J.A.; Krumholz, H.M.; Curry, L.A. Attitudes, Training Experiences, and Professional Expectations of US General Surgery Residents: A National Survey. JAMA 2009, 302, 1301–1308. [Google Scholar] [CrossRef]
- McKenna, D.T.; Mattar, S.G. What is wrong with the training of general surgery? Adv. Surg. 2014, 48, 201–210. [Google Scholar] [CrossRef]
- Huang, G.C.; McSparron, J.I.; Balk, E.M.; Richards, J.B.; Smith, C.C.; Whelan, J.S.; Newman, L.R.; Smetana, G.W. Procedural instruction in invasive bedside procedures: A systematic review and meta-analysis of effective teaching approaches. BMJ Qual. Saf. 2016, 25, 281–294. [Google Scholar] [CrossRef]
- Riggle, J.D.; Wadman, M.C.; McCrory, B.; Lowndes, B.R.; Heald, E.A.; Carstens, P.K.; Hallbeck, M.S. Task analysis method for procedural training curriculum development. Perspect. Med. Educ. 2014, 3, 204–218. [Google Scholar] [CrossRef] [Green Version]
- Yates, K.; Sullivan, M.; Clark, R. Integrated studies on the use of cognitive task analysis to capture surgical expertise for central venous catheter placement and open cricothyrotomy. Am. J. Surg. 2012, 203, 76–80. [Google Scholar] [CrossRef]
- Lalys, F.; Jannin, P. Surgical process modelling: A review. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 495–511. [Google Scholar] [CrossRef] [Green Version]
- Mincarone, P.; Leo, C.G.; Trujillo-Martín, M.D.M.; Manson, J.; Guarino, R.; Ponzini, G.; Sabina, S. Standardized languages and notations for graphical modelling of patient care processes: A systematic review. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2018, 30, 169–177. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Description | Number |
|---|---|---|
| Experts by Specialty | Anesthesiology | 8 |
| Anesthesiology and Intensive Medicine | 4 | |
| Nephrology | 1 | |
| Experts by unit of work of work | Operating Room | 7 |
| Operating Room and ICU | 4 | |
| ICU | 1 | |
| Dialysis Unit | 1 | |
| Experts by type of hospital | Private Hospital | 4 |
| Public Hospital | 3 | |
| University Hospital | 4 | |
| Military Hospital | 2 | |
| Expert by geographic location | Capital City | 10 |
| Regional Cities | 3 |
| Proposed Activity | First, Survey | Second Survey | Change | ||||
|---|---|---|---|---|---|---|---|
| Not Include % | Neutral % | Include % | Not Include % | Neutral % | Include % | % | |
| Prepare implements | 0.0 | 8.3 | 91.7 | 0 | 0 | 100 | 4.25 |
| Perform surgical hand washing | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | 0.00 |
| Get in sterile gown. gloves. hat and mask | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | −2.08 |
| Clean puncture area with chlorhexidine | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | 2.00 |
| Drape puncture area in sterile fashion | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | 0.00 |
| Ultrasound setup (deep and vascular mode) | 0.0 | 16.7 | 83.3 | 0 | 17 | 83 | −2.08 |
| Put gel in probe | 8.3 | 8.3 | 83.3 | 8 | 17 | 75 | −4.08 |
| Cover sterile probe | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | 4.17 |
| Put sterile gel in covered transducer | 16.7 | 33.3 | 50.0 | 17 | 42 | 42 | −2.17 |
| Probe position at puncture zone | 0.0 | 8.3 | 91.7 | 0 | 17 | 83 | 0.00 |
| To give position to the patient ⋆ | 0 | 17 | 83 | ||||
| Forced contralateral head rotation | 16.7 | 58.3 | 25.0 | 25 | 58 | 17 | −2.17 |
| Do Valsalva maneuver | 25.0 | 58.3 | 16.7 | 33 | 67 | 0 | −8.42 |
| Anatomical vein identification | 8.3 | 33.3 | 58.3 | 17 | 25 | 58 | −2.00 |
| Identify vein with color Doppler | 0.0 | 50.0 | 50.0 | 0 | 83 | 17 | −14.58 |
| Compression test identification | 0.0 | 33.3 | 66.7 | 0 | 33 | 67 | 2.17 |
| Anesthetize puncture zone | 0.0 | 25.0 | 75.0 | 0 | 25 | 75 | −2.00 |
| Puncture with fine needle | 41.7 | 33.3 | 25.0 | 42 | 50 | 8 | −8.25 |
| Vein puncture with trocar under ultrasound vision | 0.0 | 8.3 | 91.7 | 0 | 0 | 100 | 2.08 |
| Venous blood return + | 0.0 | 16.7 | 83.3 | 0 | 17 | 83 | −2.00 |
| Set probe in sterile area ⋆ | 0 | 17 | 83 | ||||
| Remove syringe from the puncture trocar | 0.0 | 25.0 | 75.0 | 0 | 17 | 83 | −2.17 |
| Advance Seldinger guidewire through puncture trocar | 0.0 | 8.3 | 91.7 | 0 | 0 | 100 | 2.08 |
| Remove puncture trocar ⋆ | 0 | 17 | 83 | ||||
| Verification of the guide with ultrasound in long axis | 0.0 | 16.7 | 83.3 | 0 | 25 | 75 | −10.33 |
| Verification of the guide with ultrasonography in short axis | 0.0 | 33.3 | 66.7 | 0 | 33 | 67 | −4.25 |
| Guidewire in good position (in the vein) | 0.0 | 0.0 | 100.0 | 0 | 8 | 92 | −4.08 |
| Cut skin | 25.0 | 58.3 | 16.7 | 33 | 58 | 8 | −4.25 |
| Widen subcutaneous pathway | 0.0 | 8.3 | 91.7 | 0 | 0 | 100 | −4.08 |
| Advance catheter over guidewire without losing control | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | 2.17 |
| Remove guidewire entirely | 0.0 | 0.0 | 100.0 | 0 | 0 | 100 | −0.08 |
| Check flow and reflow in each catheter port | 0.0 | 8.3 | 91.7 | 0 | 17 | 83 | −2.17 |
| Check catheter in the vein with ultrasound in long axis | 0.0 | 41.7 | 58.3 | 8 | 50 | 42 | −8.42 |
| Check catheter in the vein with ultrasound in short axis | 8.3 | 41.7 | 50.0 | 17 | 50 | 33 | −8.42 |
| Catheter in good position (in the vein) | 0.0 | 8.3 | 91.7 | 0 | 8 | 92 | −2.17 |
| Secure catheter with knots | 8.3 | 0.0 | 91.7 | 0 | 17 | 83 | −0.08 |
| Secure catheter with other systems ⋆ | 8 | 58 | 33 | ||||
| Place catheter patches | 0.0 | 8.3 | 91.7 | 0 | 8 | 92 | −0.08 |
| Check catheter position with radiology method ⋆ | 0 | 17 | 83 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de la Fuente, R.; Fuentes, R.; Munoz-Gama, J.; Dagnino, J.; Sepúlveda, M. Delphi Method to Achieve Clinical Consensus for a BPMN Representation of the Central Venous Access Placement for Training Purposes. Int. J. Environ. Res. Public Health 2020, 17, 3889. https://doi.org/10.3390/ijerph17113889
de la Fuente R, Fuentes R, Munoz-Gama J, Dagnino J, Sepúlveda M. Delphi Method to Achieve Clinical Consensus for a BPMN Representation of the Central Venous Access Placement for Training Purposes. International Journal of Environmental Research and Public Health. 2020; 17(11):3889. https://doi.org/10.3390/ijerph17113889
Chicago/Turabian Stylede la Fuente, Rene, Ricardo Fuentes, Jorge Munoz-Gama, Jorge Dagnino, and Marcos Sepúlveda. 2020. "Delphi Method to Achieve Clinical Consensus for a BPMN Representation of the Central Venous Access Placement for Training Purposes" International Journal of Environmental Research and Public Health 17, no. 11: 3889. https://doi.org/10.3390/ijerph17113889