Evaluation of the Waste Tire Resources Recovery Program and Environmental Health Policy in Taiwan

Abstract
:1. Introduction
2. Literature Review
3. Background
4. Method
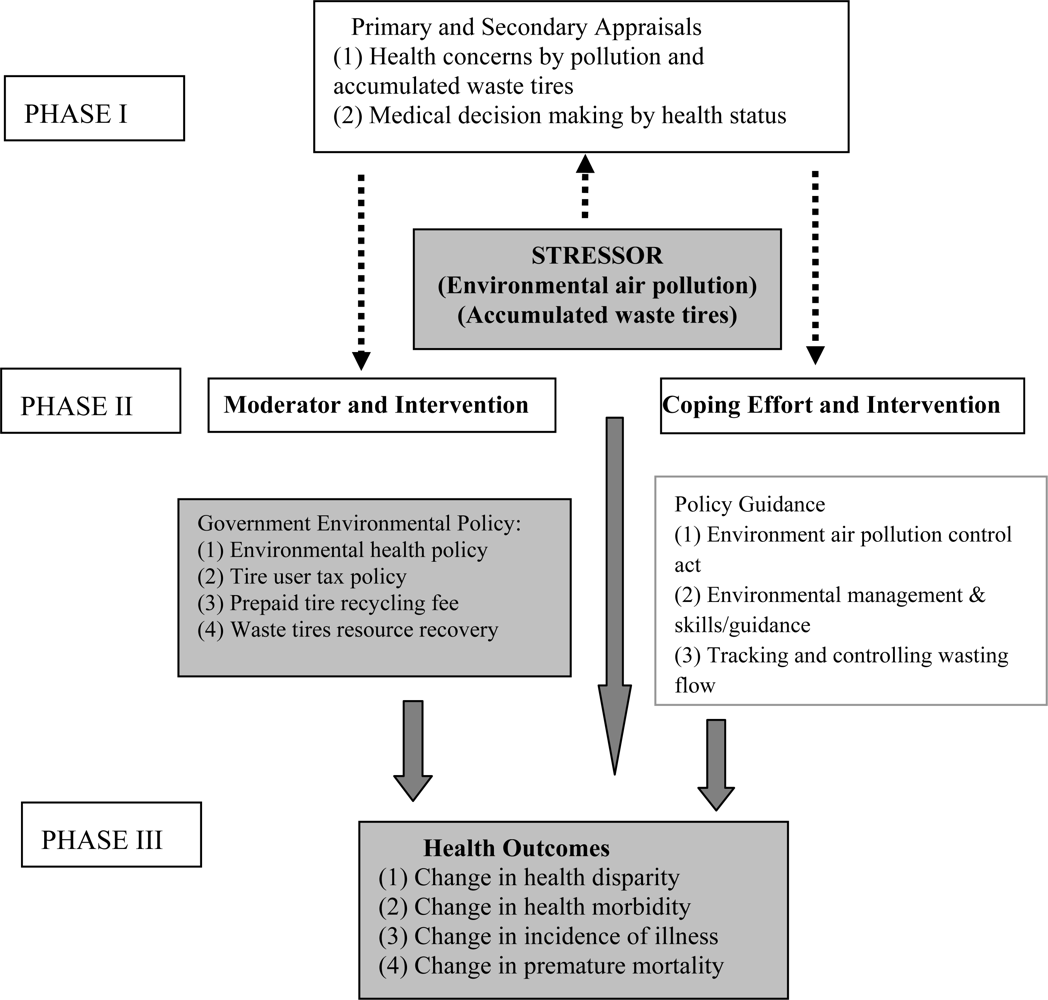
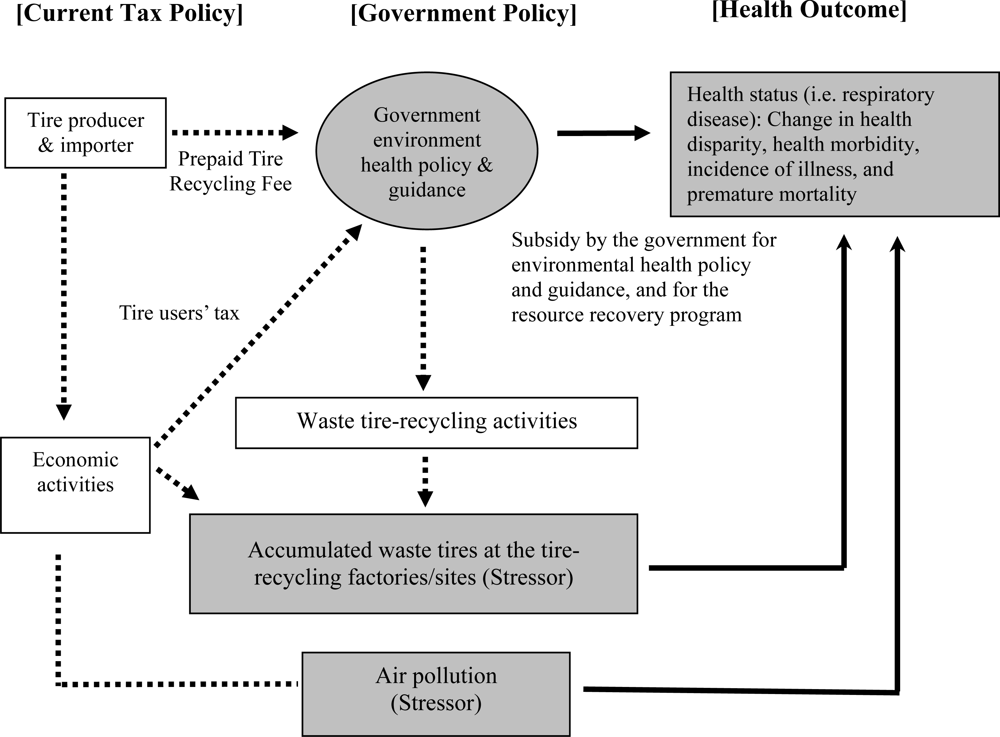
4.1. Analytical Framework: Application of the Transactional Model
4.2. Data
5. Empirical Results
6. Discussion
7. Conclusions
Acknowledgments
References
- EPA of Taiwanese Government. The Annual Assessment Report of the Air Pollution Control in Taiwan in 1992–2002: The Project Report for the Tire-recycling Management and Subsidy Costs; The Department and Bureau of Environmental Protection of Taiwanese Government: Taoyuan City, Taiwan, 2002. [Google Scholar]
- Horner, JM. Environmental health implications of heavy metal pollution from car tires. Rev. Environ. Health 1996, 11, 175–178. [Google Scholar]
- Wenzel, L; Glanz, K; Lerman, C. Theory, research, and practice in health behavior and health education. In Health Behavior and Health Education, 3rd Ed; Glanz, K, Rimer, BK, Lewis, FM, Eds.; Jossey-Bass: San Francisco, USA, 2002; pp. 210–239. [Google Scholar]
- Schwartz, J. Particulate air pollution and daily mortality in Detroit. Environ. Res 1991, 564, 204–213. [Google Scholar]
- Schwartz, J. What are people dying of on high air pollution days? Environ. Res 1994, 64, 26–35. [Google Scholar]
- Lee, JT; Kim, H; Hong, YC; Kwon, HJ; Schwartz, J; Christiani, DC. Air pollution and daily mortality in seven major cities of Korea, 1991–1997. Environ. Res 2000, 84, 247–254. [Google Scholar]
- O’Neill, MS; Loomis, D; Borja-Aburto, VH. Ozone, area social conditions, and mortality in Mexico City. Environ. Res 2004, 94, 234–242. [Google Scholar]
- Chang, CC; Tsai, SS; Ho, SC; Yang, CY. Air pollution and hospital admissions for cardiovascular disease in Taipei, Taiwan. Environ. Res 2005, 98, 114–119. [Google Scholar]
- Shaw, D; Hung, MF. Evolution and evaluation of air pollution control policy in Taiwan. Environ. Econ. Policy Stud 2001, 1, 141–166. [Google Scholar]
- Braun-Fahrlander, C; Ackermann-Liebrich, U; Schwartz, J; Gnehm, HP; Rutishauser, M; Wanner, HU. Air pollution and respiratory symptoms in preschool children. Am. Rev. Respir. Dis 1992, 145, 42–47. [Google Scholar]
- Pope, CA, III. Respiratory hospital admissions associated with PM10 pollution in Utah, Salt Lake, and Cache valleys. Arch. Environ. Health 1991, 46, 89–97. [Google Scholar]
- Gilliland, FD; Berhane, K; Rappaport, EB; Thomas, DC; Avol, E; Gauderman, WJ; London, SJ; Margolis, HG; McConnell, R; Islam, KT; Peters, JM. The effects of ambient air pollution on school absenteeism due to respiratory illnesses. Epidemiology 2001, 12, 43–54. [Google Scholar]
- Ho, WC; Hartley, WR; Myers, L; Lin, MH; Lin, YS; Lien, CH; Lin, RS. Air pollution, weather, and associated risk factors related to asthma prevalence and attack rate. Environ. Res 2007, 104, 402–409. [Google Scholar]
- Mullahy, J; Portney, PR. Air pollution, cigarette smoking, and the production of respiratory health. J. Health Econ 1990, 9, 193–205. [Google Scholar]
- Archer, VE. Air pollution and fatal lung disease in three Utah counties. Arch. Environ. Health 1990, 45, 325–334. [Google Scholar]
- Schwartz, J. The distributed lag between air pollution and daily deaths. Epidemiology 2000, 11, 320–326. [Google Scholar]
- Braga, ALF; Zanobetti, A; Schwartz, J. The lag structure between particulate air pollution and respiratory and cardiovascular deaths in 10 US cities. J. Occup. Environ. Med 2001, 43, 927–933. [Google Scholar]
- Kim, SY; Lee, JT; Hong, YC; Ahn, KJ; Kim, H. Determining the threshold effect of ozone on daily mortality: an analysis of ozone and mortality in Seoul, Korea, 1995–1999. Environ. Res 2004, 94, 113–119. [Google Scholar]
- Choudhury, AH; Gordian, ME; Morris, SS. Associations between respiratory illness and PM10 air pollution. Arch. Environ. Health 1997, 52, 113–117. [Google Scholar]
- Peters, JM; Avol, E; Navidi, W; London, SJ; Gauderman, WJ; Lurmann, F; Linn, WS; Margolis, H; Rappaport, E; Gong, H, Jr; Thomas, DC. A study of twelve Southern California communities with differing levels and types of air pollution: I. Prevalence of respiratory morbidity. Am. J. Respir. Crit. Care Med 1999, 159, 760–767. [Google Scholar]
- Chay, KY; Greenstone, M. Air quality, infant mortality, and the Clean Air Act of 1970.
- Currie, J; Neidell, M. Air population and infant health: What can we learn from California’s recent experience? NBER Working Paper #10251, NBER: Cambridge, MA, USA, 2004. [Google Scholar]
- Evans, GW; Cohen, S. Environmental stress. In Handbook of Environmental Psychology; Stokols, D, Altman, I, Eds.; John Wiley & Sons: New York, USA, 1987; Volume 1, pp. 571–610. [Google Scholar]
- Glanz, K. Perspectives on group, organization, and community interventions. In Health Behavior and Health Education, 3rd Ed; Glanz, K, Rimer, BK, Lewis, FM, Eds.; Jossey-Bass: San Francisco, USA, 2002; pp. 389–403. [Google Scholar]
- Folkman, S; Lazarus, RS; Gruen, RJ; DeLongis, A. Appraisal, coping, health status, and psychological symptoms. J. Pers. Soc. Psychol 1986, 50, 571–579. [Google Scholar]
- Quah, E; Boon, TL. The economic cost of particulate air pollution on health in Singapore. J. Asian Econ 2003, 14, 73–90. [Google Scholar]
- Berger, SA; Jones, PA; White, MC. Exploratory analysis of respiratory illness among persons living near a landfill. J. Environ. Health 2000, 62, 19–23. [Google Scholar]
- Pope, CA, III; Dockery, DW; Spengler, JD; Raizenne, ME. Respiratory health and PM10 pollution. A daily time series analysis. Am. Rev. Respir. Dis 1991, 144, 668–674. [Google Scholar]
- Yang, CY; Wang, JD; Chan, CC; Chen, PC; Huang, JS; Cheng, MF. Respiratory and irritant health effects of a population living in a petrochemical-polluted area in Taiwan. Environ Res 1997, 74, 145–149. [Google Scholar]
- Vassanadumrongdee, S; Matsuoka, S; Shirakawa, H. Meta-analysis of contingent valuation studies on air pollution-related morbidity risks. Environ. Econ. Policy Stud 2004, 6, 11–47. [Google Scholar]
- Greene, WH. Econometric Analysis; Prentice Hall: New Jersey, USA, 2007; pp. 215–245. [Google Scholar]
- Kennedy, P. A Guide to Econometrics; MIT Press: Cambridge, USA, 2008; pp. 116–136. [Google Scholar]
- Wooldridge, JM. Introductory Econometrics: A Modern Approach; Thomson, South-Western: Ohio, USA, 2003; pp. 323–359. [Google Scholar]
- Grossman, M. The human capital model. In Handbooks in Economics; Elsevier: Amsterdam, Holland, 2003; pp. 347–408. [Google Scholar]
- Chang, NB. Economic and policy instrument analyses in support of the scrap tire recycling program in Taiwan. J. Environ. Manage 2008, 86, 435–450. [Google Scholar]
- Yamada, T; Chen, CC; Yamada, T. Economic evaluation of relapse prevention for substance users: Treatment settings and health care policy. Adv. Health Econ. Health Serv. Res 2005, 16, 431–450. [Google Scholar]
- Samet, JM; Pope, CA, III. Epidemiologic research needs for particulate air pollution. J. Toxicol. Environ. Health 2003, 66, 1873–1876. [Google Scholar]
- Pope, CA, III; Burnett, RT. Confounding in air pollution epidemiology: the broader context. Epidemiology 2007, 18, 424–426. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Mean** | Standard Deviation** |
|---|---|---|
| Dependent Variables: | ||
| ▪ RES & BRO as health status:
Number of deaths caused by bronchitis and other respiratory diseases in persons per county/city per year by ICD9 classification number of basic tabulation 460–466 | 576.85 | 341.66 |
| ▪ RESPIRATORY as health status:
Number of deaths caused by respiratory related disease in persons per county/city per year by ICD9 classification number of basic tabulation 460–466 | 487.99 | 293.51 |
| Independent Variables: | ||
| ▪ SUBSIDY:
The government subsidy to the environmental health policy for the resource recovery program in 10,000 Taiwan dollars per county/city per year* | 646.44 | 1159.14 |
| ▪ SUBSIDY2:
A quadratic term of the government subsidy* | 174.62E+4 | 581.02E+4 |
| ▪ Waste tires (STRESSOR):
Accumulated waste tires at tire recycling factories/sites based on collection of waste tires in tons per county/city per year | 202.01 | 362.23 |
| ▪ O3, t-1 (STRESSOR):
1-year-lag level of ozone pollutant concentration expressed in ppb in 3-year moving average of the 8th highest by county/city | 115.24 | 22.50 |
| ▪ O3, t-2 (STRESSOR):
2-year-lag level of ozone pollutant concentration expressed in ppb in 3-year moving average of the 8th highest by county/city | 114.34 | 22.41 |
| ▪ PM10, t-1 (STRESSOR):
1-year-lag level of respirable particle pollutant concentration expressed in μg/m3 in 3-year moving average of the 8th highest by county/city | 139.91 | 35.35 |
| ▪ PM10, t-2 (STRESSOR):
2-year-lag level of respirable particle pollutant concentration expressed in μg/m3 in 3-year moving average of the 8th highest by county/city | 143.05 | 36.57 |
| ▪ D. O3, t-1 (STRESSOR):
Interacting city dummy variable (D.CITY) with 1-year-lag level of ozone pollutant concentration expressed in ppb in 3-year moving average of the 8th highest by county/city | 55.06 | 61.01 |
| ▪ D. O3, t-2 (STRESSOR):
Interacting city dummy variable (D.CITY) with 2-year-lag level of ozone pollutant concentration expressed in ppb in 3-year moving average of the 8th highest by county/city | 54.31 | 60.27 |
| ▪ D. PM10, t-1 (STRESSOR):
Interacting city dummy variable (D.CITY) with 1-year-lag level of respirable particle pollutant concentration expressed in μg/m3 in 3-year moving average 8th highest by county/city | 65.18 | 73.65 |
| ▪ D. PM10, t-2 (STRESSOR):
Interacting city dummy variable (D.CITY) with 2-year-lag level of respirable particle pollutant concentration expressed in μg/m3 in 3-year moving average of the 8th highest by county/city | 66.89 | 75.66 |
| ▪ D. CITY:
A large city dummy variable, 1=if the population density is more than 1,000 per square km, otherwise 0. | 0.45 | 0.50 |
| ▪ TIME dummy 1999:
Year dummy variable, with a 1 assigned to the year of 1999 and a 0 to other year. Year of 1998 is excluded as an omitted year | 0.25 | 0.44 |
| ▪ TIME dummy 2000:
Year dummy variable, with a 1 assigned to the year of 2000 and a 0 to other year. Year of 1998 is excluded as an omitted year | 0.25 | 0.44 |
| ▪ TIME dummy 2001:
Year dummy variable, with a 1 assigned to the year of 2001 and a 0 to other year. Year of 1998 is excluded as an omitted year | 0.25 | 0.44 |
| ▪ POPULATION:
Population of county/city | 101.38E+4 | 799.00E+3 |
| Independent Variable | RES & BRO | RESPIRATORY | ||
|---|---|---|---|---|
| Estimate | t-statistics | Estimate | t-statistics | |
| Constant | 3.592a | 5.733 | 3.272a | 5.159 |
| SUBSIDY | –2.800E-04b | –2.353 | –0.306E-03b | –2.507 |
| SUBSIDY2 | 4.401E-08b | 2.315 | 4.745E-08b | 2.465 |
| Waste tires (STRESSOR) (ln) | 0.050c | 1.815 | 0.061b | 2.221 |
| O3, t-1 (STRESSOR) (ln) | –0.316 | –0.520 | –0.360 | –0.586 |
| O3, t-2 (STRESSOR) (ln) | –0.119 | –0.194 | –0.150 | –0.243 |
| PM10, t-1 (STRESSOR) (ln) | 1.158c | 1.903 | 1.422b | 2.308 |
| PM10, t-2 (STRESSOR) (ln) | –0.225 | –0.388 | –0.391 | –0.666 |
| D. O3 t-1 (STRESSOR) | 0.034a | 2.939 | 0.034a | 2.856 |
| D. O3, t-2 (STRESSOR) | 0.019c | 1.823 | 0.019c | 1.782 |
| D. PM10, t-1 (STRESSOR) | –0.026b | –2.051 | –0.029b | –2.246 |
| D. PM10, t-2 (STRESSOR) | 0.018 | 1.556 | 0.021c | 1.770 |
| D. CITY | –5.796a | –5.023 | –5.687a | –4.868 |
| TIME dummy 1999 | –0.112 | –1.051 | –0.127 | –1.178 |
| TIME dummy 2000 | –0.141 | –1.276 | –0.143 | –1.282 |
| TIME dummy 2001 | –0.128 | –1.021 | –0.158 | –1.249 |
| Number of observations 88 | 88 | |||
| Log-likelihood | –34.588 | –35.670 | ||
| Multiple R | 0.857 | 0.852 | ||
| R Square | 0.734 | 0.725 | ||
| Adjusted R Square | 0.678 | 0.668 | ||
| F statistics | 13.238a | 12.670a | ||
- Independent variables of (ln) denote the natural logarithm.
- Dependent variables, RES&BRO and RESPIRATORY, are the natural logarithm.
- Significance of t-statistics is indicated by the following: “a” at the 1% level, “b” at the 5% level, and “c” at the 10% level.
- TIME dummy 1998 is an omitted variable to evaluate the implementation of the new tire recycling regulation since 1999.
- Another regression included the variable of population density that was not statistically significant and showed similar results with lower F statistics. The results are available from the author on request.
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chen, C.-C.; Yamada, T.; Chiu, I.-M.; Liu, Y.-K. Evaluation of the Waste Tire Resources Recovery Program and Environmental Health Policy in Taiwan. Int. J. Environ. Res. Public Health 2009, 6, 1075-1094. https://doi.org/10.3390/ijerph6031075
Chen C-C, Yamada T, Chiu I-M, Liu Y-K. Evaluation of the Waste Tire Resources Recovery Program and Environmental Health Policy in Taiwan. International Journal of Environmental Research and Public Health. 2009; 6(3):1075-1094. https://doi.org/10.3390/ijerph6031075
Chicago/Turabian StyleChen, Chia-Ching, Tetsuji Yamada, I-Ming Chiu, and Yi-Kuen Liu. 2009. "Evaluation of the Waste Tire Resources Recovery Program and Environmental Health Policy in Taiwan" International Journal of Environmental Research and Public Health 6, no. 3: 1075-1094. https://doi.org/10.3390/ijerph6031075