A Helpline Telephone Service for Tobacco Related Issues: The Italian Experience

Abstract
:
1. Introduction
2. Results and Discussion
2.1. The Smoking Problem
2.2. Telephone Counsellingand t he Italian Antismoking Helpline’s Experience
2.3. The Italian Antismoking Helpline and Smoking Cessation Services
2.4. The Antismoking Italian Helpline and OssFAD Material
- The collection of educational material on addiction prevention developed in Italy;
- The identification of material that appraised the target of reference, the type of used language, the communication's effectiveness in comparison to the contents, the formative objectives;
- The production of educational materials;
- The set up of Italian schools database and the promotion of materials to schools;
- The evaluation of the educational materials diffused administering a questionnaire to the teachers.
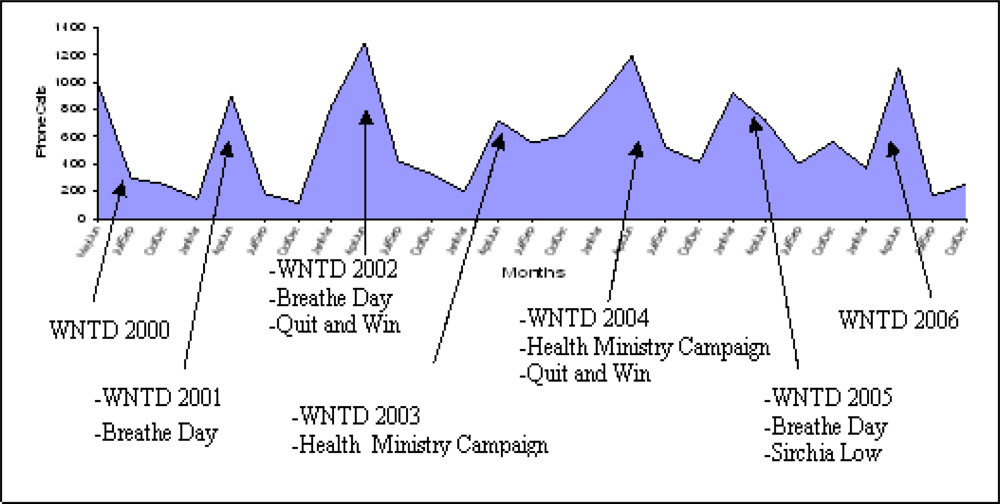
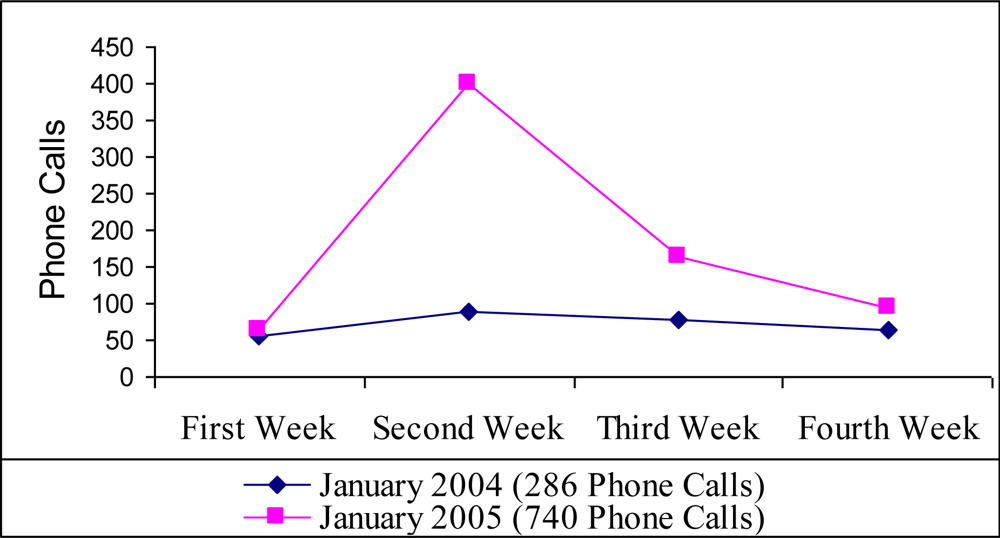
2.5. Italian Antismoking Helpline and Anti-tobacco Media Campaigns
3. Conclusions
Acknowledgments
References
- Cornuz, J; Zellweger, JP; Burnard, B. Smoking cessation: importance for the patient and role of the practitioner. Schweiz. Med. Wochenschr 1994, 124, 1315–1325. [Google Scholar]
- Franchini, M; Caruso, C; Perico, A; Pacifici, R; Monleon, T; Garcia-Algar, O; Rossi, S; Pichini, S. Assessment of foetal exposure to cigarette smoke after recent implementations of smoke-free policy in Italy. Acta Paediatr 2008, 97, 546–550. [Google Scholar]
- US Department of Health and Human Services. Reducing Tobacco Use: A Report of the Surgeon General. Department of Health and Human Services, Centers for Disease Control and Prevention; National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, Georgia, U.S. A., 2000; pp. 5–25.
- Pacifici, R; Pichini, S; Scafato, E; Zuccaro, P; Macchia, T; Bartoli, G; Di Pucchio, A; Martucci, L; Modigliani, G; Mortali, C; Pizzi, E; Russo, R. Osservatorio su Fumo, Alcol e Droga. Not Ist Sup Sanità 2001, 14, 3–10. [Google Scholar]
- WHO. Draft WHO Framework Convention on Tobacco Control; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Osservatorio Fumo, Alcol e Droga. Il fumo in Italia: Indagine DOXA 2008; Istituto Superiore di Sanità: Roma, Italy, 2008.
- Peto, R; Lopez, AD; Boreham, J; Thun, M. Mortality From Smoking In Developed Countries 1950–2000, 2nd Ed ed; Clinical Trial Service Unit & Epidemiological Studies Unit: Oxford, U.K., 1994; (Update June 2006 on www.ctsu.ox.ac.uk).
- Peto, R; Darby, S; Deo, H; Silcocks, P; Whitley, E; Doll, R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. Brit. Med. J 2000, 321, 323–329. [Google Scholar]
- Simonato, L; Agudo, A; Ahrens, W; Benhamou, E; Benhamou, S; Boffetta, P; Brennan, P; Darby, SC; Forastiere, F; Fortes, C; Gaborieau, V; Gerken, M; Gonzales, CA; Jöckel, KH; Kreuzer, M; Merletti, F; Nyberg, F; Pershagen, G; Pohlabeln, H; Rösch, F; Whitley, E; Wichmann, HE; Zambon, P. Lung cancer and sigarette smoking in Europe: an update of risk estimates and an assessment of inter-country heterogeneity. Int. J. Cancer 2001, 91, 876–887. [Google Scholar]
- Strachan, DP; Cook, DG. Health effects of passive smoking 1. Parental smoking and lower respiratory illness in infancy and early childhood. Thorax 1997, 52, 905–914. [Google Scholar]
- He, J; Vupputuri, S; Allen, K; Prerost, MR; Hughes, J; Whelton, PK. Passive smoking and the risk of coronary heart disease – A meta-analysis of epidemiologic studies. N. Engl. J. Med 1999, 340, 920–926. [Google Scholar]
- Hackshaw, AK; Law, MR; Wald, NJ. The accumulated evidence on lung cancer and environmental tobacco smoke. BMJ 1997, 315, 980–988. [Google Scholar]
- Windham, GC; Eaton, A; Hopkins, B. Evidence for association between environmental tobacco smoke exposure and birth weight: a metanalysis and new data. Paediatr Perinat. Epidemiol 1999, 13, 35–57. [Google Scholar]
- Anderson, HR; Cook, DG. Passive smoking and sudden infant death syndrome: review of the epidemiological evidence. Thorax 1997, 52, 1003–1009. [Google Scholar]
- Fiore, MC; Croyle, RT; Curry, SJ; Cutler, CM; Davis, RM; Gordon, C; Healton, C; Koh, HK; Orleans, CT; Richling, D; Satcher, D; Seffrin, J; Williams, C; Williams, LN; Keller, PA; Baker, TB. Preventing 3 million premature deaths and helping 5 millionsmokers quit: a national action plan for tobacco cessation. Am. J. Public Health 2004, 94, 205–210. [Google Scholar]
- Hopkins, DP; Briss, PA; Ricard, CJ; Husten, CG; Carande-Kulis, VG; Fielding, JE; Alao, MO; McKenna, JW; Sharp, DJ; Harris, JR; Woollery, TA; Harris, KW. Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke. Am. J. Prev. Med 2001, 20, 16–66. [Google Scholar]
- Lichtenstein, E; Glasgow, RE; Lando, HA; Ossip-Klein, DJ; Boles, SM. Telephone counseling for smoking cessation: rationales and meta-analytic review of evidence. Health Educ. Res 1996, 11, 243–257. [Google Scholar]
- Stead, LF; Lancaster, T; Perera, R. Telephone counselling for smoking cessation (Cochrane Review). In The Cochrane Library 2004; Issue 1, John Wiley & Sons, Ltd: Chichester, U.K., 2004. [Google Scholar]
- Zhu, SH; Anderson, CM; Johnson, CE; Tedeschi, G; Roeseler, A. A centralized telephone service for tobacco cessation: the California experience. Tob Control 2000, 9, II48–55. [Google Scholar]
- Centers for Disease Control and Prevention. Office on Smoking and Health. Unpublished quitline data.
- McAfee, T; Sofian, NS; Wilson, J; Hindmarsh, M. The role of tobacco intervention in population-based health care: a case study. Am. J. Prev. Med 1998, 14, 46–52. [Google Scholar]
- Zhu, SH; Anderson, CM. Bridging the clinical and public health approaches to smoking cessation: California Smokers’ Helpline. In Promoting Human Wellness: New Frontiers for Research, Practice, and Polic; Jamner, MS, Stokols, D, Eds.; University of California Press: Berkeley, CA, U.S.A., 2000; pp. 378–394. [Google Scholar]
- Zhu, SH; Rosbrook, B; Anderson, C; Gilpin, E; Sadler, G; Pierce, JP. The demographics of help-seeking for smoking cessation in California and the role of the California Smokers’ Helpline. Tob. Control 1995, 4, S9–15. [Google Scholar]
- Pacifici, R; Di Pucchio, A; Pizzi, E; Martucci, L; Mortali, C; Zuccaro, P. L’attivita di counselling del Telefono Verde contro il Fumo dell’Istituto Superiore di Sanita. 2001, 103–109. [Google Scholar]
- Di Pucchio, A; Pizzi, E; Solimini, R; Matrobattista, L; Rossi, S. Structural and operational characteristics of Italian Smoking Cessation Services: a National investigation. 10th Annual Conference of SRNT, Rome, Italy; September 2008; p. 173. [Google Scholar]
- Pizzi, E; Di Pucchio, A; Rossi, S; Carosi, G; Martucci, L; Mattioli, D; Mazzola, M; Mortali, C; Pacifici, R; Zuccaro, P. Guida ai servizi territoriali per la cessazione dal fumo di tabacco. (Update 2007). Istituto Superiore di Sanità: Roma, Italia, 2008; (Strumenti di Riferimento 08/S1). [Google Scholar]
- Belleudi, V; Bargagli, AM; Davoli, M; Di Pucchio, A; Pacifici, R; Pizzi, E; Zuccaro, P; Peducci, CA. “Servizi territoriali per la cessazione dal fumo”. Interventi per la cessazione dell’abitudine al fumo in Italia: offerta ed efficacia nella pratica. Risultati di uno studio longitudinale multicentrico. Epidemiol. Prev 2007, 31, 148–157. [Google Scholar]
- Zuccaro, P; Di Pucchio, A; Pizzi, E; Martucci, L; Carosi, G; Solimini, R; Rossi, S. Il fumo in Italia. Respiro 2008, 2, 23–24. [Google Scholar]
- Faggiano, F; Vigna-Taglianti, FD; Versino, E; Zambon, A; Borraccino, A; Lemma, P. School-based prevention for illicit drugs' use. Cochrane Database Syst Rev 2005, 18, CD003020. [Google Scholar]
- Thomas, R; Perera, R. School-based programmes for preventing smoking. Cochrane Database Syst Rev 2002, 4, CD001293. [Google Scholar]
- Botvin, GJ; Griffin, KW. Life Skills Training: empirical findings and future directions. J. Prim. Prev 2004, 25, 211–231. [Google Scholar]
- Zuccaro, P; Caraffa, G; Pizzi, E; Di Pucchio, A; Martucci, L; Modigliani, G; Rossi, S; Mazzola, M; Carosi, G; Pichini, S; Mattioli, D; Pacifici, R. Venditori di Fumo. Conoscere i meccanismi che inducono al fumo di tabacco e le sue conseguenze. Percorso multimediale interattivo; Istituto Superiore di Sanità: Roma, Italia, 2005. [Google Scholar]
- NIDA. Preventing Drug Use among Children and Adolescents. Available at Http:// www.drugabuse.gov/pdf/prevention/inBrief.pdf (accessed December 24, 2008).
- Stevens, C. Designing an effective counteradvertising campaign—California. Cancer 1998, 83, 2736–2741. [Google Scholar]
- CDHHS/TCS. A model for change: the California Experience in tobacco control. California Department of Health Services, Tobacco Control Section: Sacramento, CA, U.S.A., 1998. [Google Scholar]
- Bandura, A. Social Cognitive Theory of Mass Communication. Media Psychol 2001, 3, 265–299. [Google Scholar]
- Wakefield, M; Borland, R. Saved by the bell: the role of telephone helpline services in the context of mass-media anti-smoking campaigns. Tob. Control 2000, 9, 117–119. [Google Scholar]
- Weinreich, NK. Hands-On Social Marketing: A Step-by-Step Guide; Sage Publications: Thousand Oaks, CA, U.S.A., 1999. [Google Scholar]
- Ossip-Klein, DJ; Giovino, GA; Megahed, N; Black, PM; Emont, SL; Stiggins, J; Shulman, E; Moore, L. Effects of a smokers’ hotline: results of a 10-county self-help trial. J. Consult. Clin. Psychol 1991, 59, 325–332. [Google Scholar]
- Centers for Disease Control and Prevention. Telephone quitlines: a resource for development, implementation, and evaluation; Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, U.S.A., 2004. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AIMS | TARGETS |
|---|---|
|
|
| Callers’ Characteristics | |
|---|---|
| Gender | % |
| Female | 45.7 |
| Male | 54.3 |
| Groups of Callers | % |
| Smokers | 61.4 |
| Non smokers | 7.2 |
| Ex-smokers | 4.9 |
| Family or friends | 9.8 |
| Other callers | 17.9 |
| Geographic range of callers | % |
| North | 34.4 |
| Center | 23.2 |
| South | 17.9 |
| Islands | 9.2 |
| Not found | 13.9 |
| Main Areas of Interest | % |
| Cessation Services | 55.2 |
| Psychological support | 23.6 |
| Anti-smoking therapies | 10.1 |
| Effects produced by tobacco smoke | 2.4 |
| Effects produced by second-hand smoke | 2.6 |
| Current legislation | 6.6 |
| Cooperation | 5 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pizzi, E.; Di Pucchio, A.; Mastrobattista, L.; Solimini, R.; Pacifici, R.; Pichini, S. A Helpline Telephone Service for Tobacco Related Issues: The Italian Experience. Int. J. Environ. Res. Public Health 2009, 6, 900-914. https://doi.org/10.3390/ijerph6030900
Pizzi E, Di Pucchio A, Mastrobattista L, Solimini R, Pacifici R, Pichini S. A Helpline Telephone Service for Tobacco Related Issues: The Italian Experience. International Journal of Environmental Research and Public Health. 2009; 6(3):900-914. https://doi.org/10.3390/ijerph6030900
Chicago/Turabian StylePizzi, Enrica, Alessandra Di Pucchio, Luisa Mastrobattista, Renata Solimini, Roberta Pacifici, and Simona Pichini. 2009. "A Helpline Telephone Service for Tobacco Related Issues: The Italian Experience" International Journal of Environmental Research and Public Health 6, no. 3: 900-914. https://doi.org/10.3390/ijerph6030900