Successful Smoking Cessation and Duration of Abstinence—An Analysis of Socioeconomic Determinants

Abstract
:1. Introduction
2. Method
2.1. Data
2.2. Variables
2.2.1. Outcome Variables
2.2.2. Independent Variables
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Descriptive Analysis
3.2.1. Successful Cessation Analysis
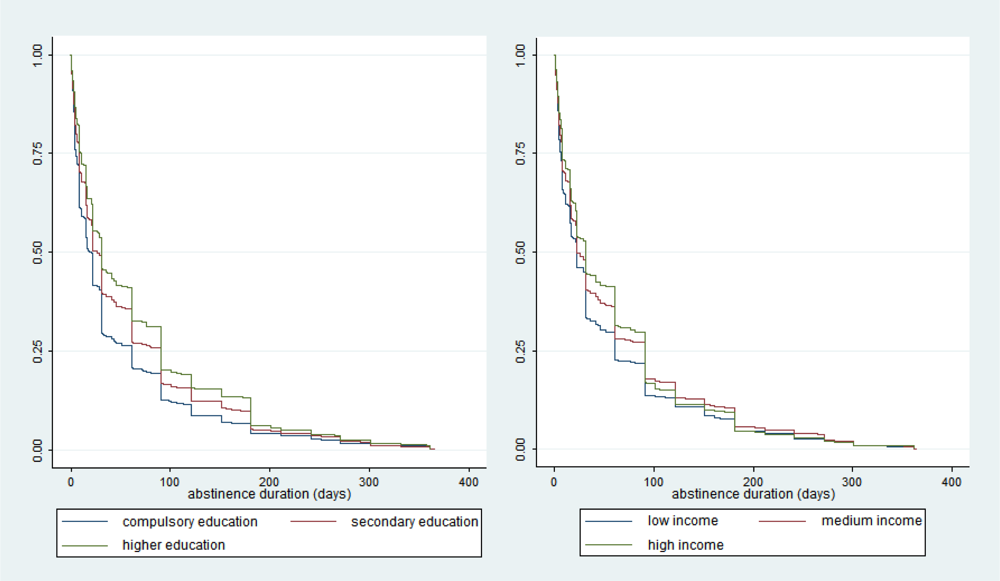
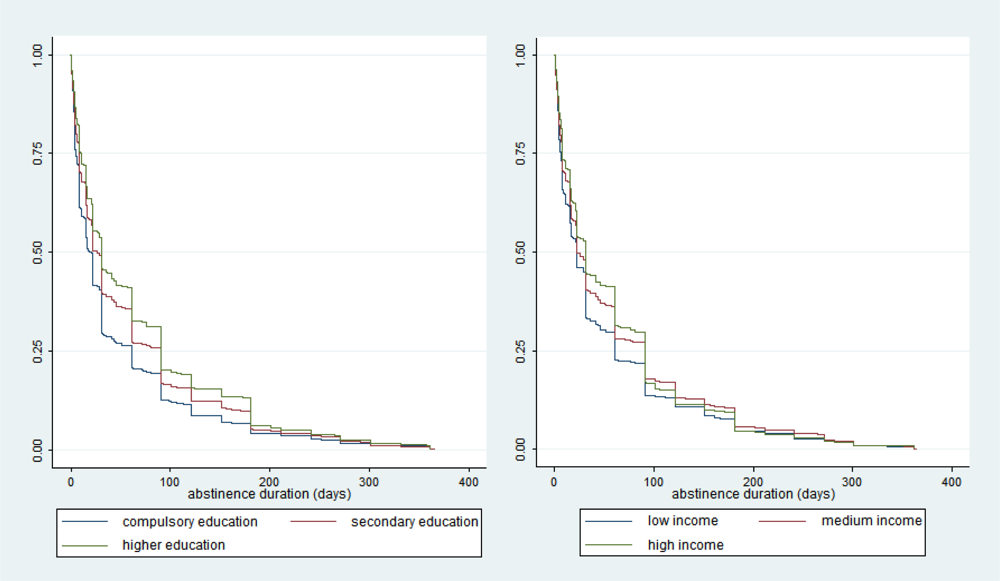
3.2.2. Abstinence Duration (Relapse Analysis)
3.3. Multivariate Analysis
3.3.1. Successful Cessation Analysis
3.3.2. Abstinence Duration (Relapse Analysis)
4. Discussion
References
- Lopez, A; Collishaw, N; Piha, T. A descriptive model of the cigarette epidemic in developed countries. Tob. Control 1994, 3, 242–247. [Google Scholar]
- Jha, P; Peto, R; Zatonski, W; Boreham, J; Jarvis, MJ; Lopez, AD. Social inequalities in male mortality, and in male mortality from smoking: Indirect estimation from national death rates in England and Wales, Poland, and North America. Lancet 2006, 368, 367–370. [Google Scholar]
- Mackenbach, JP; Huisman, M; Andersen, O; Bopp, M; Borgan, JK; Borrell, C; Costa, G; Deboosere, P; Donkin, A; Gadeyne, S; Minder, C; Regidor, E; Spadea, T; Valkonen, T; Kunst, AE. Inequalities in lung cancer mortality by the educational level in 10 European populations. Eur. J. Cancer 2004, 40, 126–135. [Google Scholar]
- Mackenbach, JP; Meerding, WJ; Kunst, A. Economic Implications of Socio-Economic Inequalities in Health in the European Union; Health and Consumer Protection Directorate-General, European Commission: Brussels, Belgium, 2007. [Google Scholar]
- Giskes, K; Kunst, AE; Benach, J; Borrell, C; Costa, G; Dahl, E; Dalstra, JA; Federico, B; Helmert, U; Judge, K; Lahelma, E; Moussa, K; Ostergren, PO; Platt, S; Prattala, R; Rasmussen, NK; Mackenbach, JP. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J. Epidemiol. Commun. H 2005, 59, 395–401. [Google Scholar] [Green Version]
- Huisman, M; Kunst, AE; Mackenbach, J. Inequalities in the prevalence of smoking in the European Union: Comparing education and income. Prev. Med 2005, 40, 756–764. [Google Scholar]
- Harman, J; Graham, H; Francis, B; Inskip, HM; SWS Study Group. Socioeconomic gradients in smoking among young women: A British survey. Soc. Sci. Med 2006, 63, 2791–2800. [Google Scholar]
- Laaksonen, M; Rahkonen, O; Karvonen, S; Lahelma, E. Socioeconomic status and smoking: Analysing inequalities with multiple indicators. Eur. J. Public Health 2005, 15, 262–269. [Google Scholar]
- Cavelaars, AE; Kunst, AE; Geurts, JJ; Crialesi, R; Grötvedt, L; Helmert, U; Lahelma, E; Lundberg, O; Matheson, J; Mielck, A; Rasmussen, NK; Regidor, E; do Rosário-Giraldes, M; Spuhler, T; Mackenbach, JP. Educational differences in smoking: international comparison. BMJ 2000, 320, 1102–1107. [Google Scholar]
- Barbeau, E; Kreiger, N; Soobader, MJ. Working class matters: Socioeconomic disadvantage, race/ethnicity, gender, and smoking in NHIS 2000. Am. J. Public Health 2004, 94, 269–278. [Google Scholar]
- Borland, R; Owen, N; Hill, D; Schofield, P. Predicting attempts and sustained cessation of smoking after the introduction of workplace smoking bans. Health Psychol 1991, 10, 336–342. [Google Scholar]
- Lee, C; Kahende, J. Factors associated with successful smoking cessation in the United States, 2000. Am. J. Public Health 2007, 97, 1503–1509. [Google Scholar]
- Schaap, MM; Kunst, AE. Monitoring of socio-economic inequalities in smoking: Learning from the experiences of recent scientific studies. Public Health 2009, 123, 103–109. [Google Scholar]
- Keller, R; Radtke, T; Krebs, H; Hornung, R. Tabakmonitoring—Schweizerische Umfrage zum Tabakkonsum; Psychologisches Institut der Universität Zürich, Sozial- und Gesundheitspsychologie: Zürich, Switzerland, 2008. [Google Scholar]
- Chiolero, A; Wietlisbach, V; Ruffieux, C; Paccaud, F; Cornuz, J. Clustering of risk behaviors with cigarette consumption: A population-based survey. Prev. Med 2006, 42, 348–353. [Google Scholar]
- Burton, S; Tiffany, S. The effect of alcohol consumption on craving to smoke. Addiction 1997, 92, 15–26. [Google Scholar]
- Hillemacher, T; Bayerlein, K; Wilhelm, J; Frieling, H; Thürauf, N; Ziegenbein, M; Kornhuber, J; Bleich, S. Nicotine dependence is associated with compulsive alcohol craving. Addiction 2006, 101, 892–897. [Google Scholar]
- John, U; Meyer, C; Rumpf, HJ; Schumann, A; Thyrian, JR; Hapke, U. Strength of the relationship between tobacco smoking, nicotine dependence and the severity of alcohol dependence syndrome criteria in a population-based sample. Alcohol Alcoholism 2003, 38, 606–612. [Google Scholar]
- Kaplan, E; Meier, P. Nonparametric estimation from incomplete estimations. J. Am. Stat. Assoc 1958, 53, 457–481. [Google Scholar]
- Cleves, M; Gould, WW; Gutierrez, RG; Marchenko, Y. An Introduction to Survival Analysis Using Stata, 2nd ed; Stata Press: College Station, TX, USA, 2008. [Google Scholar]
- Caraballo, R; Giovino, G; Pechacek, T; Mowery, PD. Factors associated with discrepancies between self-reports on cigarette smoking and measured serum cotinine levels among persons aged 17 years or older. Am. J. Epidemiol 2001, 153, 807–814. [Google Scholar]
- Piasecki, TM; Fiore, MC; McCarthy, DE; Baker, TB. Have we lost our way? The need for dynamic formulations of smoking relapse proneness. Addiction 2002, 97, 1093–1108. [Google Scholar]
- Fiore, MC. Treating Tobacco Use and Dependence, Public Health Service Clinical Practice Guideline; US Department of Health and Human Services: Rockville, IN, USA, 2000. [Google Scholar]
- Wu, P; Wilson, K; Dimoulas, P; Mills, EJ. Effectiveness of smoking cessation therapies: A systematic review and meta-analysis. BMC Public Health 2006, 6, 300. [Google Scholar]

{kind=link}
| Cessation analysis (N = 6,290) | Abstinence duration analysis (N = 3,209) | |||||
|---|---|---|---|---|---|---|
| % of successful quitters | absolute diff. in the proportion of successful quitters compared to reference category (pp.) | relative diff. compared to reference category (%) | mean duration, in days, of longest quit attempt (unsuccessful quitters) | absolute diff. in mean duration compared to reference category | relative diff. compared to reference category (%) | |
| Education Level | ||||||
| Compulsory | 34.5 | - | - | 61.8 | - | - |
| Secondary | 45.4 | +10.9 | +31.6 | 86.6 | +24.8 | +40.1 |
| Higher | 54.2 | +19.7 | +57.1 | 99.4 | +37.6 | +60.8 |
| Household Income | ||||||
| Up to 4,000 | 39.6 | - | - | 79.4 | - | - |
| 4,000–8,000 | 47.5 | +7.9 | +19.9 | 87.1 | +7.7 | +9.7 |
| 8,000 + | 53.9 | +14.3 | +36.1 | 100.5 | +21.1 | +26.6 |
| Odds of successfully quitting | ||
|---|---|---|
| Men | Women | |
| Education | ||
| Compulsory Secondary Higher | 1.00 (ref.) 1.13 (0.92) 1.39* (2.15) | 1.00 (ref.) 1.40** (3.10) 1.78*** (4.49) |
| Household Income | ||
| Up to 4000 | 1.00 (ref.) | 1.00 (ref.) |
| 4–8 8+ | 1.13 (1.11) 1.65*** (3.98) | 1.27** (2.76) 1.47*** (3.58) |
| Age | ||
| 18–24 25–44 45–65 | 1.00 (ref.) 2.20*** (5.83) 2.59*** (6.59) | 1.00 (ref.) 1.32** (2.38) 1.18 (1.30) |
| Marital status | ||
| Non-married Married | 1.00 (ref.) 1.36* (3.46) | 1.00 (ref.) 1.36*** (4.17) |
| Heavy drinking (“regular drinker”) | ||
| No Yes | 1.00 (ref.) 0.91 (−1.14) | 1.00 (ref.) 1.00 (0.02) |
| Interest in healthy diet | ||
| No Yes | 1.00 (ref.) 1.08 (0.82) | 1.00 (ref.) 1.50** (3.30) |
| Region with high prevention intensity | ||
| No Yes | 1.00 (ref.) 1.09 (1.09) | 1.00 (ref.) 0.99 (−0.04) |
| N | 2,691 | 3,599 |
| Time ratios | ||
|---|---|---|
| _Men | _Women | |
| Education (ref: compulsory) | ||
| Secondary | 1.28 (1.68) | 1.61*** (3.69) |
| Higher | 2.16*** (4.19) | 2.27*** (4.89) |
| Income (ref: low income) | ||
| Middle income High income | 1.23 (1.58) 1.47* (2.47) | 1.12 (0.96) 1.44* (2.47) |
| Age (ref: 18–24) | ||
| 25–44 | 0.93 (−0.50) | 0.82 (−1.37) |
| 45–65 | 0.57** (−3.34) | 0.48*** (−4.84) |
| Marital status (ref: non-married) | ||
| Married | 0.99 (−0.05) | 0.99 (−0.02) |
| Heavy drinking (ref: no) | ||
| Yes | 0.76* (−2.55) | 0.83 (−1.49) |
| Interest in healthy diet (ref: no) | ||
| Yes | 1.47** (3.24) | 1.35* (2.01) |
| Region with high prevention intensity (ref: no) | ||
| Yes | 1.73*** (5.26) | 2.04*** (7.26) |
| N | 2,614 | 3,522 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Marti, J. Successful Smoking Cessation and Duration of Abstinence—An Analysis of Socioeconomic Determinants. Int. J. Environ. Res. Public Health 2010, 7, 2789-2799. https://doi.org/10.3390/ijerph7072789
Marti J. Successful Smoking Cessation and Duration of Abstinence—An Analysis of Socioeconomic Determinants. International Journal of Environmental Research and Public Health. 2010; 7(7):2789-2799. https://doi.org/10.3390/ijerph7072789
Chicago/Turabian StyleMarti, Joachim. 2010. "Successful Smoking Cessation and Duration of Abstinence—An Analysis of Socioeconomic Determinants" International Journal of Environmental Research and Public Health 7, no. 7: 2789-2799. https://doi.org/10.3390/ijerph7072789