Climate Change and Mortality in Vienna—A Human Biometeorological Analysis Based on Regional Climate Modeling



Abstract
:1. Introduction
2. Data and Methods
2.1. Mortality data and methods
2.2. Climate station data and methods
2.3. Assessment of the impact of climate change
3. Results and Discussion
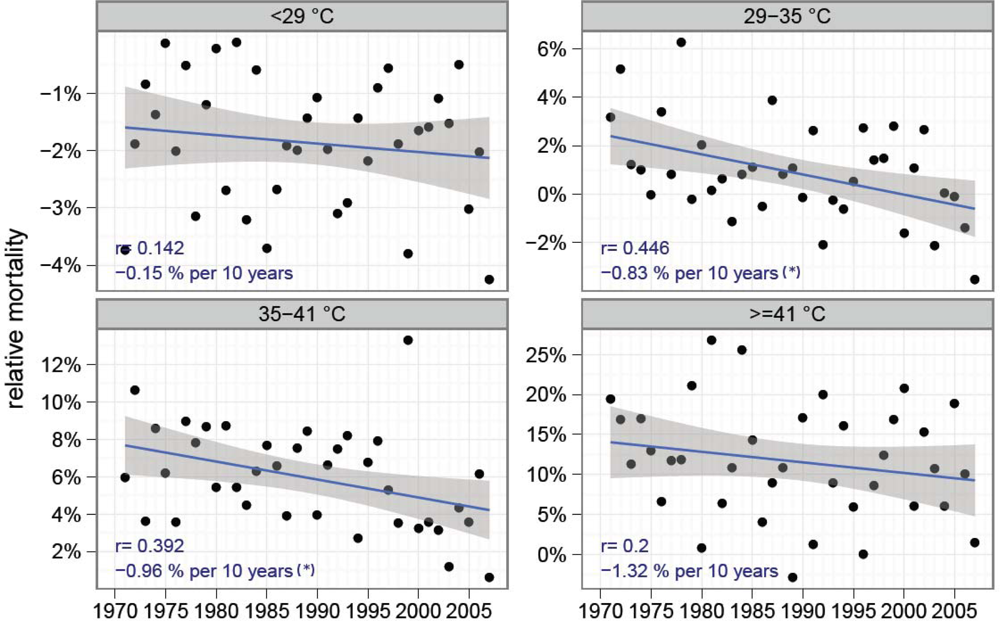
3.1. The relation of climate and mortality between 1970 and 2007
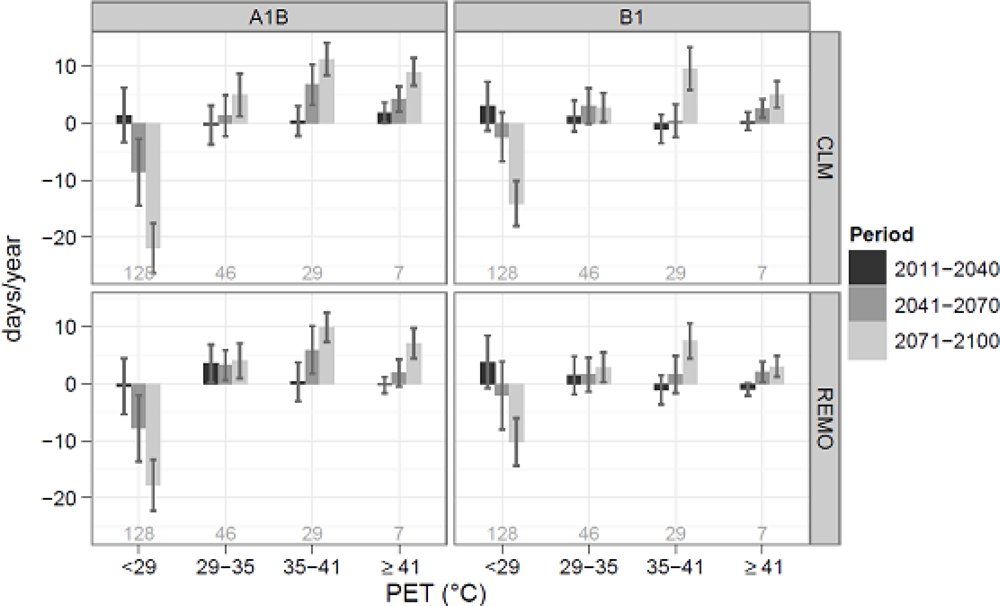
3.2. Climate change impact
3.3. Discussion
4. Conclusions
Acknowledgments
References
- Robine, JM; Cheung, SL; Le Roy, S; van Oyen, H; Herrmann, FR. Report on Excess Mortality in Europe During Summer 2003; ; EU Community Action Programme for Public Health: Grant Agreement 20051142007. [Google Scholar]
- Heudorf, U; Meyer, C. Gesundheitliche Auswirkungen extremer Hitze–am Beispiel der Hitzewelle und der Mortalität in Frankfurt am Main im August 2003. Gesundheitswesen 2005, 67, 369–374. [Google Scholar]
- Díaz, J; García-Herrera, R; Trigo, RM; Linares, C; Valente, MA; De Miguel, JM; Hernández, E. The impact of the summer 2003 heat wave in Iberia: how should we measure it? Int. J. Biometeorol 2006, 50, 159–166. [Google Scholar]
- Schär, C; Vidale, PL; Lüthi, D; Frei, C; Häberli, C; Liniger, MA; Appenzeller, C. The role of increasing temperature variability in European summer heatwaves. Nature 2004, 427, 332–336. [Google Scholar]
- Hutter, HP; Moshammer, H; Wallner, P; Leitner, B; Kundi, M. Heatwaves in Vienna: effects on mortality. Wien Klin. Wochenschr 2007, 119, 223–227. [Google Scholar]
- Tobías, A; de Olalla, P; Linares, C; Bleda, M; Caylà, J; Díaz, J. Short-term effects of extreme hot summer temperatures on total daily mortality in Barcelona, Spain. Int. J. Biometeorol 2010, 54, 115–117. [Google Scholar]
- Pascal, M; Laaidi, K; Ledrans, M; Baffert, E; Caserio-Schönemann, C; Le Tertre, A; Manach, J; Medina, S; Rudant, J; Empereur-Bissonnet, P. France‘s heat health watch warning system. Int. J. Biometeorol 2006, 50, 144–153. [Google Scholar]
- Höppe, P. Heat balance modelling. Experientia 1993, 49, 741–746. [Google Scholar]
- Matzarakis, A. Die thermische Komponente des Stadtklimas; Albert-Ludwigs-University of Freiburg: Freiburg, Germany, 2001; 6. [Google Scholar]
- Höppe, P. Aspects of human biometeorology in past, present and future. Int. J. Biometeorol 1997, 40, 19–23. [Google Scholar]
- Höppe, P; Mayer, H. Planungsrelevante Bewertung der thermischen Komponente des Stadtklimas. Landschaft Stadt 1987, 19, 22–29. [Google Scholar]
- WHO. International Statistical Classification of Diseases and Related Health Problems. 2007.
- Gemmell, I; McLoone, P; Boddy, FA; Dickinson, GJ; Watt, GCM. Seasonal variation in mortality in Scotland. Int. J. Epidemiol 2000, 29, 274–279. [Google Scholar]
- Laschewski, G; Jendritzky, G. Effects of the thermal environment on human health: an investigation of 30 years of daily mortality data from SW Germany. Clim. Res 2002, 21, 91–103. [Google Scholar]
- Koppe, C; Jendritzky, G. Inclusion of short-term adaptation to thermal stresses in a heat load warning procedure. Meteorol. Z 2005, 14, 271–278. [Google Scholar]
- Schönwiese, CD. Praktische Statistik für Meteorologen und Geowissenschaftler; Gebrüder Borntraeger: Stuttgart, Germany, 2006. [Google Scholar]
- Matzarakis, A; Rutz, F; Mayer, H. Modelling radiation fluxes in simple and complex environments–application of the RayMan model. Int. J. Biometeorol 2007, 51, 323–334. [Google Scholar]
- Matzarakis, A; Rutz, F; Mayer, H. Modelling radiation fluxes in simple and complex environments–basics of the RayMan model. Int. J. Biometeorol 2010, 54, 131–139. [Google Scholar]
- VDI. Verein deutscher Ingenieure Interaction between Atmosphere and Surfaces–Calculation of Short-wave and Long-wave Radiation, VDI Guideline 3789 Part 2; Beuth Verlag: Berlin, Germany, 1994. [Google Scholar]
- Höppe, P. Die Energiebilanz des Menschen; Ludwig Maximilian University of Munich: Munich, Germany, 1984; 49. [Google Scholar]
- Höppe, P. The physiological equivalent temperature–a universal index for the biometeorological assessment of the thermal environment. Int. J. Biometeorol 1999, 43, 71–75. [Google Scholar]
- Mayer, H; Höppe, P. Thermal comfort of man in different urban environments. Theor. Appl. Climatol 1987, 38, 43–49. [Google Scholar]
- Hajat, S; Kovats, RS; Atkinson, RW; Haines, A. Impact of hot temperatures on death in London: a time series approach. J. Epidemiol. Commun. H 2002, 56, 367–372. [Google Scholar]
- Matzarakis, A; Mayer, H. Another kind of environmental stress: thermal stress. WHO Newsletter 1996, 18, 7–10. [Google Scholar]
- Helsel, DR; Hirsch, RM. Statistical methods in water resources. U.S. Geological Survey, Techniques of Water-Resources Investigations Book 4. 2002.
- Jacob, D; Podzun, R. Sensitivity studies with the Regional Climate Model REMO. Meteorol. Atmos. Phys 1997, 63, 119–129. [Google Scholar]
- Böhm, U; Kücken, M; Ahrens, W; Block, A; Hauffe, D; Keuler, K; Rockel, B; Will, A. CLM–The Climate Version of LM: Brief description and long-term application. COSMO-Newsletter 2006, 6, 225–235. [Google Scholar]
- Rockel, B; Will, A; Hense, A. The regional climate model COSMO-CLM (CCLM). Meteorol. Z 2008, 17, 347–348. [Google Scholar]
- MPI. Hinweise für REMO-Datennutzer; MPI: Hamburg, Germany, 2006. [Google Scholar]
- Jacob, D; Bärring, L; Christensen, OB; Christensen, JH; Castro, M de; Déqué, M; Giorgi, F; Hagemann, S; Hirschi, M; Jones, R; Kjellström, E; Lenderink, G; Rockel, B; Sánchez, E; Schär, C; Seneviratne, SI; Somot, S; van Ulden, A; van den Hurk, B. An inter-comparison of regional climate models for Europe: model performance in present-day climate. Climatic Change 2007, 81, 31–52. [Google Scholar]
- Brockhaus, P; Lüthi, D; Schär, C. Aspects of the diurnal cycle in a regional climate model. Meteorol. Z 2008, 17, 433–443. [Google Scholar]
- Kalkstein, LS; Greene, JS. An evaluation of climate/mortality relationships in large U.S. cities and the possible impacts of a climate change. Environ. Health Persp 1997, 105, 84–93. [Google Scholar]
- Díaz, J; García, R; de Castro Velázquez, F; Hernández, E; López, C; Otero, A. Effects of extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int. J. Biometeorol 2002, 46, 145–149. [Google Scholar]
- Koppe, C. Gesundheitsrelevante Bewertung von thermischer Belastung unter Berücksichtigung der kurzfristigen Anpassung der Bevölkerung an die lokalen Witterungsverhältnisse, , PhD Thesis, Albert-Ludwigs-University Freiburg: Freiburg, Germany2005.
- Schwartz, J. Who is sensitive to extremes of temperature? Epidemiology 2005, 16, 67–72. [Google Scholar]
- Schwartz, J; Samet, J; Patz, J. Hospital admissions for heart disease: the effects of temperature and humidity. Epidemiology 2004, 15, 755–761. [Google Scholar]
- Shao, L; Luo, M; Walker, R; Liu, X; Hwang, S; Robert, C. Impact of hot weather conditions on respiratory and cardiovascular hospital admissions in New York city, USA. Epidemiology 2008, 19, S302–S303. [Google Scholar]
- Kalkstein, LS; Smoyer, KE. The impact of climate change on human health: Some international implications. Cell. Mol. Life Sci 1993, 49, 969–979. [Google Scholar]
- Kovats, RS; Ebi, KL. Heatwaves und public health in Europe. Eur. J. Public Health 2006, 16, 592–599. [Google Scholar]
- Chau, P; Chan, K; Woo, J. Hot weather warning might help to reduce elderly mortality in Hong Kong. Int. J. Biometeorol 2009, 53, 461–468. [Google Scholar]
- Statistik Austria. Bevölkerungsvorausschätzung 2008–2050; Statistik Austria: Vienna, Austria, 2009. [Google Scholar]
- Keatinge, WR; Donaldson, GC; Cordiolo, E; Martinelli, M; Kunst, AE; Mackenback, JP; Nayha, S; Vuori, I. Heat related mortality in warm and cold regions of Europe: observational study. Brit. Med. J 2000, 321, 670–673. [Google Scholar]
- Keatinge, WR; Donaldson, GC. The Impact of global warming on health and mortality. Southern. Med. J 2004, 97, 1093–1099. [Google Scholar]
- Keatinge, WR. Winter mortality and its causes. Int. J. Circumpolar Health 2002, 61, 292–299. [Google Scholar]
- Davis, RE; Knappenberger, PC; Michaels, PJ; Novicoff, WM. Seasonality of climate-human mortality relationships in US cities and impacts of climate change. Clim. Res 2004, 26, 61–76. [Google Scholar]
- Keatinge, WR; Donaldson, GC; Bucher, K; Jendritzky, G; Cordiolo, E; Martinelli, M; Dardanoni, L; Katsouyanni, K; Kunst, AE; Mackenbach, JP; McDonald, C; Näyha, AE; Vuori, I. Cold exposure and winter mortality from ischaemic heart disease, cerebrovascular disease, respiratory disease, and all causes in warm and cold regions of Europe. The Lancet 1997, 349, 1341–1346. [Google Scholar]
- Mayer, H; Holst, J; Dostal, P; Imbery, F; Schindler, D. Human thermal comfort in summer within an urban street canyon in Central Europe. Meteorol. Z 2008, 17, 241–250. [Google Scholar]
- Lin, TP; Matzarakis, A; Hwang, RL. Shading effect on long-term outdoor thermal comfort. Build Environ 2010, 45, 213–221. [Google Scholar]
- WHO. Heat-Waves: Risks and Responses; World Health Organization: Copenhagen, Denmark, 2004. [Google Scholar]
- Fouillet, A; Rey, G; Wagner, V; Laaidi, K; Empereur-Bissonnet, P; Le Tertre, A; Frayssinet, P; Bessemoulin, P; Laurent, F; de Crouy-Chanel, P; Jougla, E; Hémon, D. Has the impact of heat waves on mortality changed in France since the European heat wave of summer 2003? A study of the 2006 heat wave. Environ. Epidemiol 2008, 37, 309–317. [Google Scholar]
- van der Linden, P; Mitchell, J. ENSEMBLES: Climate Change and Its Impacts: Summary of Research and Results from the ENSEMBLES Project; Met. Office Hadley Centre: London, UK, 2009. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | PET < 29°C | PET 29–35 °C | PET 35–41 °C | PET ≥ 41 °C |
|---|---|---|---|---|
| All causes | −1.8 ± 0.3 | 0.9 ± 0.5 | 5.8 ± 0.7 | 13.0 ± 1.7 |
| All causes–women | −2.1 ± 0.4 | 0.8 ± 0.7 | 6.6 ± 0.9 | 15.3 ± 2.3 |
| All causes–men | −1.3 ± 0.4 | 1.0 ± 0.7 | 5.0 ± 1.0 | 10.4 ± 2.1 |
| C + R | −1.8 ± 0.4 | 1.1 ± 0.7 | 6.7 ± 1.0 | 15.7 ± 2.2 |
| C + R–women | −2.0 ± 0.7 | 1.1 ± 1.2 | 7.3 ± 1.6 | 17.2 ± 3.6 |
| C + R–men | −0.8 ± 0.8 | 1.0 ± 1.4 | 5.7 ± 1.9 | 12.6 ± 3.9 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Muthers, S.; Matzarakis, A.; Koch, E. Climate Change and Mortality in Vienna—A Human Biometeorological Analysis Based on Regional Climate Modeling. Int. J. Environ. Res. Public Health 2010, 7, 2965-2977. https://doi.org/10.3390/ijerph7072965
Muthers S, Matzarakis A, Koch E. Climate Change and Mortality in Vienna—A Human Biometeorological Analysis Based on Regional Climate Modeling. International Journal of Environmental Research and Public Health. 2010; 7(7):2965-2977. https://doi.org/10.3390/ijerph7072965
Chicago/Turabian StyleMuthers, Stefan, Andreas Matzarakis, and Elisabeth Koch. 2010. "Climate Change and Mortality in Vienna—A Human Biometeorological Analysis Based on Regional Climate Modeling" International Journal of Environmental Research and Public Health 7, no. 7: 2965-2977. https://doi.org/10.3390/ijerph7072965