Relation between Temperature and Mortality in Thirteen Spanish Cities

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
3. Results and Discussion
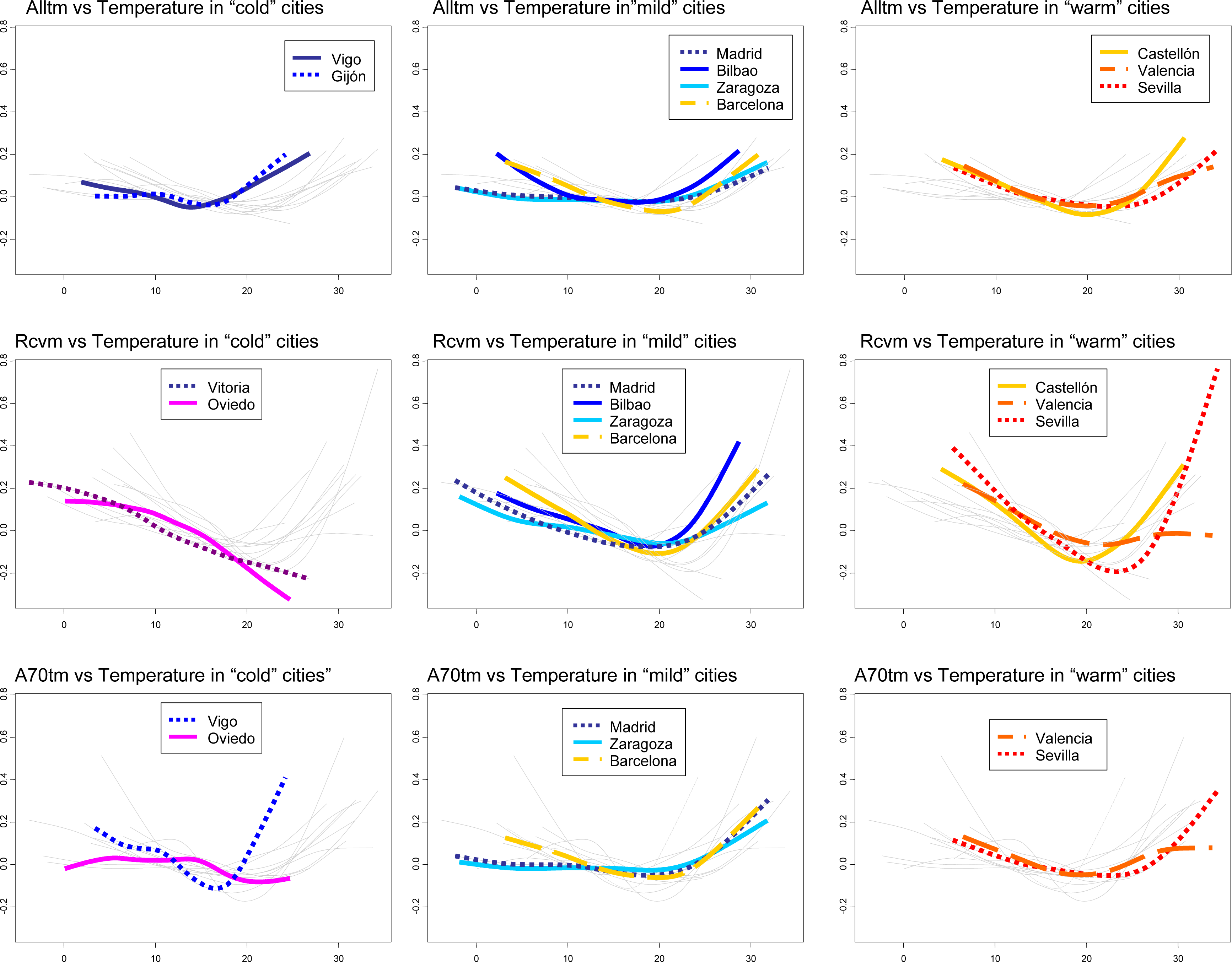
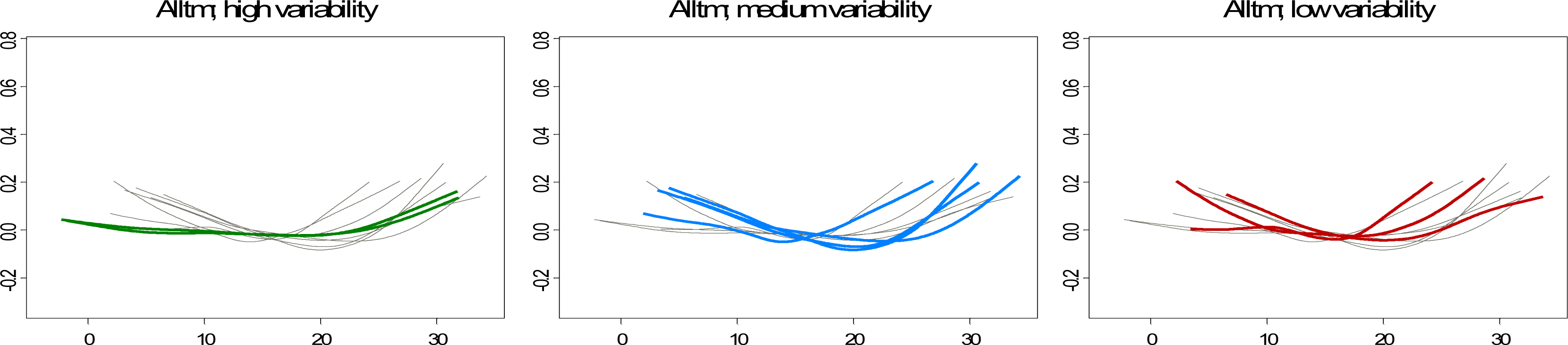
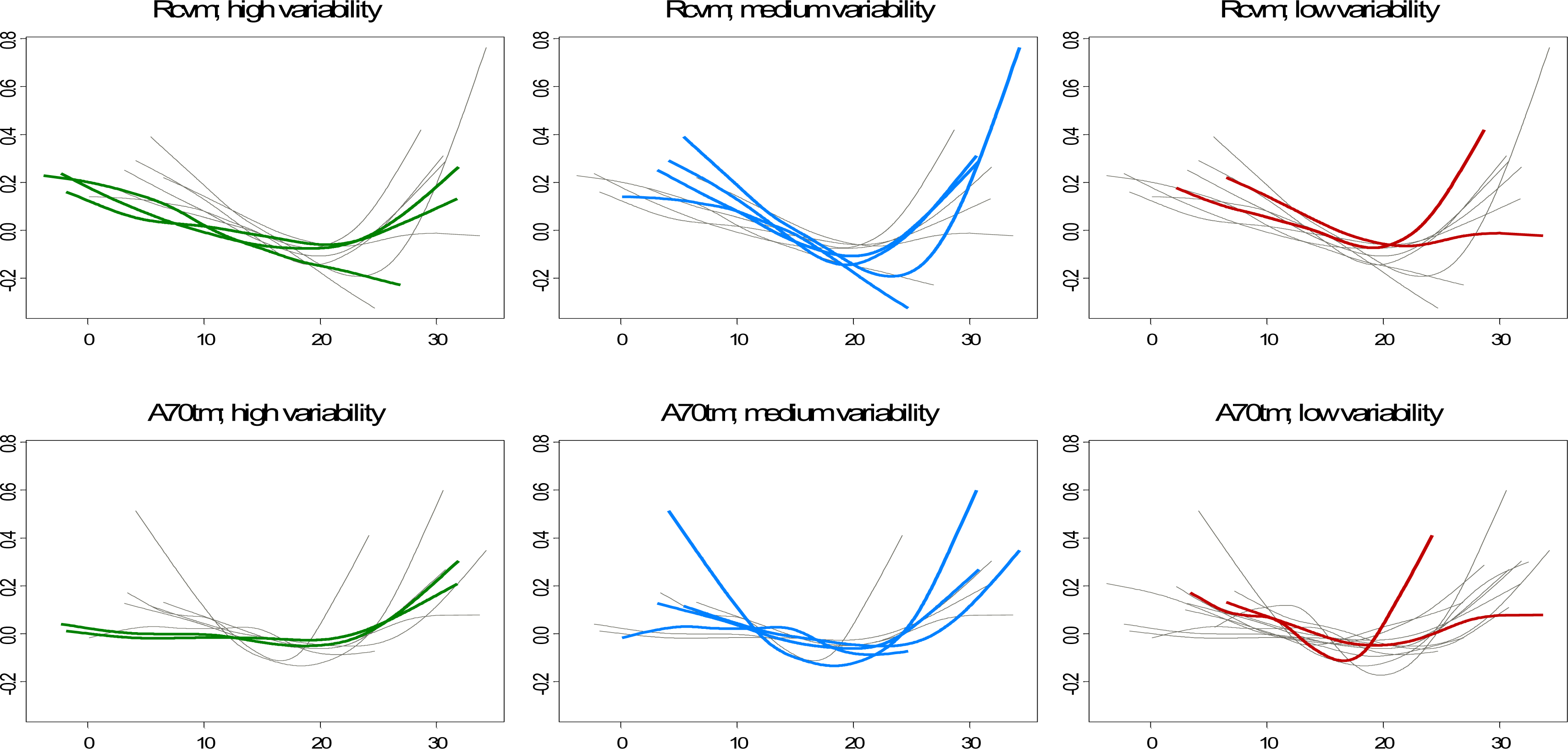
3.1. Shape of the Relationship between Temperature and Mortality
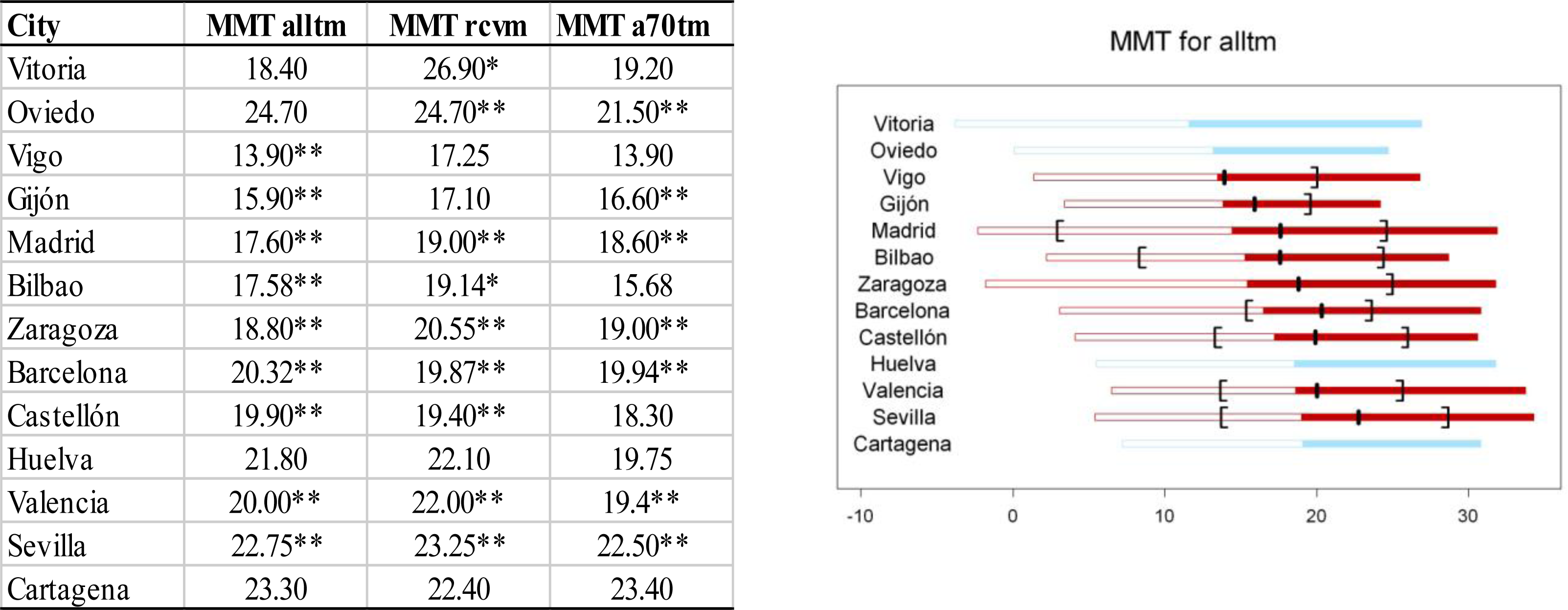
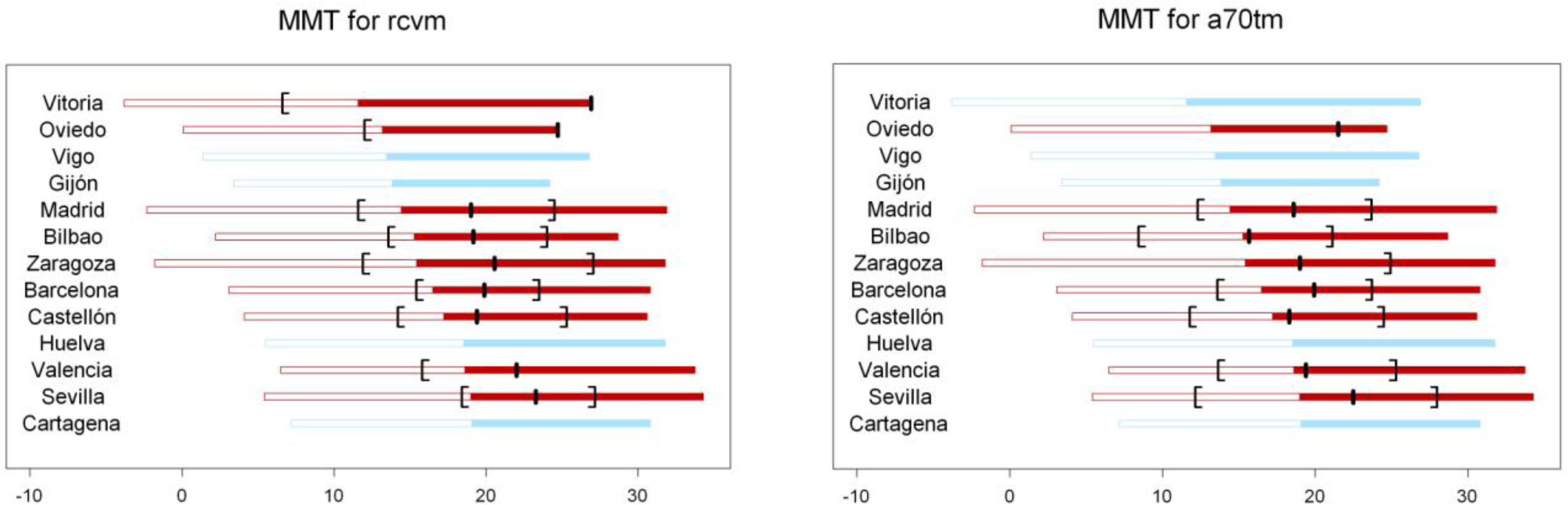
3.2. Temperature Value Associated with Minimum Mortality (MMT)
3.3. Impact of Cold and Heat on Mortality
3.4. Differences in the Impact on Specific Causes or Age Groups
3.5. Comparison with Other Studies
3.6. Implications for Public Health
4. Conclusions
Acknowledgments
References
- Huynen, MM; Martens, P; Schram, D; Weijenberg, MP; Kunst, AE. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect 2001, 109, 463–470. [Google Scholar]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ Health 2009, 8. doi:10.1186/1476-069X-8-40.. [Google Scholar]
- Kunst, AE; Looman, CW; Mackenbach, JP. Outdoor air temperature and mortality in the Netherlands: A times-series analysis. Am. J. Epidemiol 1993, 137, 331–341. [Google Scholar]
- Braga, AL; Zanobetti, A; Schwartz, J. The time course of weather-related deaths. Epidemiology 2001, 12, 662–667. [Google Scholar]
- Ballester, F; Corella, D; Pérez-Hoyos, S; Sáez, M; Hervás, A. Mortality as a function of temperature: a study in Valencia, Spain, 1991–1993. Int. J. Epidemiol 1997, 26, 551–561. [Google Scholar]
- Curriero, FC; Heiner, KS; Samet, JM; Zeger, SL; Strug, L; Patz, JA. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol 2002, 155, 80–87. [Google Scholar]
- Braga, AL; Zanobetti, A; Schwartz, J. The effect of weather on respiratory and cardiovascular deaths in 12 U.S. cities. Environ. Health Perspect 2002, 110, 859–863. [Google Scholar]
- Gosling, SN; Lowe, JA; McGregor, GR; Pelling, M; Malamud, BD. Associations between elevated atmospheric temperature and human mortality: A critical review of the literature. Climatic Change 2009, 92, 299–341. [Google Scholar]
- Hayashi, A; Akimoto, K; Sano, F; Mori, S; Tomoda, T. Evaluation of global warming impacts for different levels of stabilization as a step toward determination of the long-term stabilization target. Climatic Change 2010, 98, 87–112. [Google Scholar]
- Patz, JA; Olson, SH. Climate change and health: global to local influences on disease risk. Ann. Trop. Med. Parasitol 2006, 100, 535–549. [Google Scholar]
- Campbell-Lendrum, D; Corvalán, C. Climate change and developing-country cities: Implications for environmental health and equity. J Urban Health 2007, 84(Suppl 1), 109–117. [Google Scholar]
- Sunyer, J; Grimalt, J. Global climate change, widening health inequalities, and epidemiology. Int. J. Epidemiol 2006, 35, 213–216. [Google Scholar]
- Ballester, F; Sáez, M; Alonso, ME; Taracido, M; Ordóñez, JM. El proyecto EMECAM: Estudio español sobre la relación entre la contaminación atmosférica y la mortalidad. Antecedentes, participantes, objetivos, material y métodos. Revista Española de Salud Pública 1999, 73, 165–175. [Google Scholar]
- Dominici, F; McDermott, A; Zeger, SL; Samet, JM. On the use of generalized additive models in time-series studies of air pollution and health. Am. J. Epidemiol 2002, 156, 193–203. [Google Scholar]
- Ramsay, TO; Burnett, RT; Krewski, D. The effect of concurvity in generalized additive models linking mortality to ambient particulate matter. Epidemiology 2003, 14, 18–23. [Google Scholar]
- Dominici, F; McDermott, A; Hastie, TJ. Improved semiparametric time series models of air pollution and mortality. J. Am. Stat. Assoc 2004, 99, 938–948. [Google Scholar]
- Kelsall, JE; Samet, JM; Zeger, S; Xu, J. Air pollution and mortality in Philadelphia, 1974–1988. Am. J. Epidemiol 1997, 146, 750–762. [Google Scholar]
- Le Tertre, A; Quenel, P; Medina, S; Le Moullec, Y; Festy, B; Ferry, R; Dab, W. Modélisation des liens à court terme entre la pollution atmosphérique et la santé. Un exemple: SO2 et mortalité totale, Paris, 1987–1990. Reseau National de Santé Publique 1998, 46, 316–328. [Google Scholar]
- Donaldson, GC; Keatinge, WR; Nayha, S. Changes in summer temperature and heat-related mortality since 1971 in North Carolina, South Finland, and Southeast England. Environ. Res 2003, 91, 1–7. [Google Scholar]
- Lawlor, DA; Maxwell, R; Wheeler, BW. Rurality, deprivation, and excess winter mortality: An ecological study. J. Epidemiol. Community Health 2002, 56, 373–374. [Google Scholar]
- Peacock, JL; Symonds, P; Jackson, P; Bremmer, SA; Scarlett, JF; Strachan, DP; Anderson, HR. Acute effects of winter air pollution on respiratory function in schoolchildren in southern England. Occup. Environ. Med 2003, 60, 82–89. [Google Scholar]
- Pan, WH; Li, LA; Tsai, MJ. Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet 1995, 345, 353–355. [Google Scholar]
- Healy, JD. Excess winter mortality in Europe: A cross country analysis identifying key risk factors. J. Epidemiol. Community Health 2003, 57, 784–789. [Google Scholar]
- The Eurowinter Group; Donaldson, GC; Keatinge, WR. Cold exposure and winter mortality from ischaemic heart disease, cerebrovascular disease, respiratory disease, and all causes in warm and cold regions of Europe. Lancet 1997, 349, 1341–1346. [Google Scholar]
- Wilmshurst, P. Temperature and cardiovascular mortality excess deaths from heart disease and stroke in northern Europe are due in part to the cold. BMJ 1994, 309, 1029–1030. [Google Scholar]
- Kalkstein, LS. Direct Impacts in cities. Lancet 1993, 342, 1397–1399. [Google Scholar]
- Keatinge, WR; Donaldson, GC; Cordioli, E; Martinelli, M; Kunst, AE; Mackenbach, JP; Nayha, S; Vuori, I. Heat related mortality in warm and cold regions of Europe: Observational study. BMJ 2000, 321, 670–673. [Google Scholar]
- Laadi, M; Laaidi, K; Besancenot, JP. Temperature-related mortality in France, a comparison between regions with different climates form the perspective of global warming. Int. J. Biometeorol 2006, 51, 145–153. [Google Scholar]
- Gosling, SN; McGregor, GR; Páldy, A. Climate change and heat-related mortality in six cities part 1: Model construction and validation. Int. J. Biometeorol 2007, 51, 525–540. [Google Scholar]
- Davis, RE; Knappenberger, PC; Michaels, PJ; Novicoff, WN. Seasonality of climate-human mortality relationship in US cities and impacts of climate change. Climate Res 2004, 26, 61–76. [Google Scholar]
- Green, MS; Harari, G; Kristal-Boneh, E. Excess winter mortality from ischaemic heart disease and stroke during colder and warmer years in Israel: An evaluation and review of the role of environmental temperature. Eur. J. Pub. Health 1994, 4, 3–11. [Google Scholar]
- Keatinge, WR. Winter mortality and its causes. Int. J. Circumpolar Health 2002, 61, 292–299. [Google Scholar]
- Sáez, M; Sunyer, J; Tobías, A; Ballester, F; Antó, JM. Ischaemic heart disease mortality and weather temperature in Barcelona, Spain. Eur. J. Pub. Health 2000, 10, 58–63. [Google Scholar]
- Sáez, M; Sunyer, J; Castellsague, J; Murillo, C; Antó, JM. Relationship between weather temperature and mortality: A time series analysis approach in Barcelona. Int. J. Epidemiol 1995, 24, 576–582. [Google Scholar]
- Mackenbach, JP; Looman, CW; Kunst, AE. Air pollution, lagged effects of temperature, and mortality: The Netherlands 1979–1987. J. Epidemiol. Community Health 1993, 47, 121–126. [Google Scholar]
- Basu, R; Feng, WY; Ostro, BD. Characterizing temperature and mortality in nine California counties. Epidemiology 2008, 19, 138–145. [Google Scholar]
- McMichael, AJ; Wilkinson, P; Kovats, RS; Pattenden, S; Hajat, S; Armstrong, B; Vajanapoom, N; Niciu, EM; Mahomed, H; Kingkeow, C; Kosnik, M; O’Neill, MS; Romieu, I; Ramirez-Aguilar, M; Barreto, ML; Gouveia, N; Nikiforov, B. International study of temperature, heat and urban mortality: The ‘ISOTHURM’ project. Int. J. Epidemiol 2008, 37, 1121–1231. [Google Scholar]
- Michelozzi, P; Kirchmayer, U; Katsouyanni, K; Biggeri, A; McGregor, G; Menne, B; Kassomenos, P; Anderson, HR; Baccini, M; Accetta, G; Analytis, A; Kosatsky, T. Assessment and prevention of acute health effects of weather conditions in Europe, the PHEWE project: Background, objectives, design. Environ Health 2007, 6. doi:10.1186/1476-069X-6-12.. [Google Scholar]
- Baccini, M; Biggeri, A; Accetta, G; Kosatsky, T; Katsouyanni, K; Analitis, A; Anderson, HR; Bisanti, L; D’Ippoliti, D; Danova, J; Forsberg, B; Medina, S; Paldy, A; Rabczenko, D; Schindler, D; Michelozzi, P. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar]
- Analitis, A; Katsouyanni, K; Biggeri, A; Baccini, M; Forsberg, B; Bisanti, L; Kirchmayer, U; Ballester, F; Cadum, E; Goodman, PG; Hojs, A; Sunyer, J; Tiitanen, P; Michelozzi, P. Effects of cold weather on mortality: Results from 15 European cities within the PHEWE project. Am. J. Epidemiol 2008, 168, 1397–1408. [Google Scholar]
- Hayashi, A; Akimoto, K; Sano, F; Mori, S; Tomoda, T. Evaluation of global warming impacts for different levels of stabilization as a step toward determination of the long-term stabilization target. Climatic Change 2010, 98, 87–112. [Google Scholar]
- Bosello, F; Roson, R; Tol, RSJ. Economy-wide estimates of the implications of climate change: Human health. Ecol. Econ 2006, 58, 579–591. [Google Scholar]
- Kalkstein, LS. Saving lives during extreme weather in summer. Interventions from local health agencies and doctors can reduce mortality (editorial). BMJ 2000, 321, 650–651. [Google Scholar]
- Smoyer-Tomic, KE; Rainham, DG. Beating the heat: development and evaluation of a Canadian hot weather health-response plan. Environ. Health Perspect 2001, 109, 1241–1248. [Google Scholar]
- Lippmann, M. Winter air pollution and respiratory function. Occup. Environ. Med 2003, 60, 81. [Google Scholar]
- Olsen, ND. Prescribing warmer, healthier homes. BMJ 2001, 322, 748–749. [Google Scholar]
- Rogot, E; Sorlie, PD; Backlund, E. Air-conditioning and mortality in hot weather. Am. J. Epidemiol 1992, 136, 106–116. [Google Scholar]
- Oke, TR. Boundary Layer Climates, 2nd ed; Routledge: London, UK, 1987; p. 435. [Google Scholar]
- Tan, J; Zheng, Y; Xu, T; Guo, C; Li, L; Song, G; Zhen, X; Yuan, D; Kalkstein, AJ; Li, F; Chen, H. The urban heat island and its impact on heat waves and human health in Shanghai. Int. J. Biometeorol 2010, 54, 75–84. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City | Population | na | Total mortalityb | Mortality among 70+b | Cardio-respiratory mortalityb | Temperature | |
|---|---|---|---|---|---|---|---|
| mean | CV | ||||||
| Vitoria | 214,148 | 1,826 | 3.53(1.9) | 2.38(1.6) | 1.58(1.3) | 11.59 | 0.53 |
| Oviedo | 198,050 | 1,461 | 4.53(2.2) | 3.25(1.9) | 2.01(1.5) | 13.19 | 0.34 |
| Vigo | 274,574 | 1,461 | 5.31(2.4) | 3.49(2.0) | 2.51(1.6) | 13.49 | 0.35 |
| Gijon | 261,724 | 1,096 | 6.34(2.7) | 1.77(1.4) | 1.30(1.2) | 13.83 | 0.30 |
| Madrid | 2,940,896 | 1,461 | 60.82(11.1) | 40.47(8.7) | 27.83(7.7) | 14.43 | 0.53 |
| Bilbao | 667,034 | 1,461 | 13.62(4.0) | 8.89(3.3) | 5.97(2.6) | 15.28 | 0.31 |
| Zaragoza | 572,212 | 1,826 | 12.49(3.9) | 8.94(3.2) | 5.80(2.7) | 15.45 | 0.48 |
| Barcelona | 1,643,545 | 1,826 | 43.62(8.6) | 31.04(7.2) | 21.23(6.1) | 16.49 | 0.35 |
| Castellón | 134,213 | 1,826 | 2.9(1.8) | 2.15(1.5) | 1.58(1.3) | 17.23 | 0.33 |
| Huelva | 142,547 | 1,097 | 2.59(1.7) | 1.77(1.4) | 1.30(1.2) | 18.53 | 0.30 |
| Valencia | 749,796 | 1,096 | 16.09(4.6) | 11.1(3.7) | 7.73(3.1) | 18.61 | 0.29 |
| Seville | 683,028 | 1,380 | 13.53(4.3) | 8.92(3.4) | 6.75(3.0) | 19.00 | 0.33 |
| Cartagena | 168,023 | 1,827 | 3.47(2.0) | 2.47(1.6) | 1.77(1.4) | 19.07 | 0.27 |
| city | % ∇Alltm | % ∇Rcvm | % ∇A70tm | |||
|---|---|---|---|---|---|---|
| cold | heat | cold | heat | cold | heat | |
| Vitoria | 1.12 | 1.52 | 1.86* | 1.44 | 0.99 | |
| Oviedo | 0.96 | 2.15* | 0.68* | 0.46* | ||
| Vigo | 1.19* | 1.93* | 1.55 | 3.66 | 1.58 | 1.37 |
| Gijón | 0.57* | 2.88* | 1.31 | 1.33 | 2.43* | 6.50* |
| Madrid | 0.27* | 0.93* | 1.31* | 2.40* | 0.38* | 2.43* |
| Bilbao | 0.85* | 1.59* | 1.48* | 3.74* | 1.32 | 1.86 |
| Zaragoza | 0.14* | 1.39* | 0.76* | 1.74* | 0.06* | 1.79* |
| Barcelona | 1.41* | 2.52* | 2.23* | 3.42* | 1.21* | 2.82* |
| Castellón | 1.74* | 2.60* | 3.28* | 3.59* | 3.95 | 4.46 |
| Huelva | 1.11 | 2.10 | 2.95 | 4.17 | 3.07 | 4.83 |
| Valencia | 1.29* | 1.44* | 1.90* | 0.87* | 1.44* | 1.45* |
| Sevilla | 0.88* | 2.00* | 3.16* | 7.72* | 0.85* | 2.87* |
| Cartagena | 1.45 | 2.16 | 3.40 | 4.70 | 1.32 | 2.23 |
| R mean | 0.43 | 0.05 | 0.46 | 0.40 | 0.37 | 0.48 |
| R CV | −0.28 | −0.40 | −0.52 | −0.28 | −0.48 | −0.01 |
© 2010 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Iñiguez, C.; Ballester, F.; Ferrandiz, J.; Pérez-Hoyos, S.; Sáez, M.; López, A. Relation between Temperature and Mortality in Thirteen Spanish Cities. Int. J. Environ. Res. Public Health 2010, 7, 3196-3210. https://doi.org/10.3390/ijerph7083196
Iñiguez C, Ballester F, Ferrandiz J, Pérez-Hoyos S, Sáez M, López A. Relation between Temperature and Mortality in Thirteen Spanish Cities. International Journal of Environmental Research and Public Health. 2010; 7(8):3196-3210. https://doi.org/10.3390/ijerph7083196
Chicago/Turabian StyleIñiguez, Carmen, Ferran Ballester, Juan Ferrandiz, Santiago Pérez-Hoyos, Marc Sáez, and Antonio López. 2010. "Relation between Temperature and Mortality in Thirteen Spanish Cities" International Journal of Environmental Research and Public Health 7, no. 8: 3196-3210. https://doi.org/10.3390/ijerph7083196