Environmental Isocyanate-Induced Asthma: Morphologic and Pathogenetic Aspects of an Increasing Occupational Disease

Abstract
:1. Introduction
Isocyanate Occurrence
2. Clinical Manifestations after Exposure to Isocyanate
2.1. Morphologic Manifestations after Isocyanate Exposure of the Lung
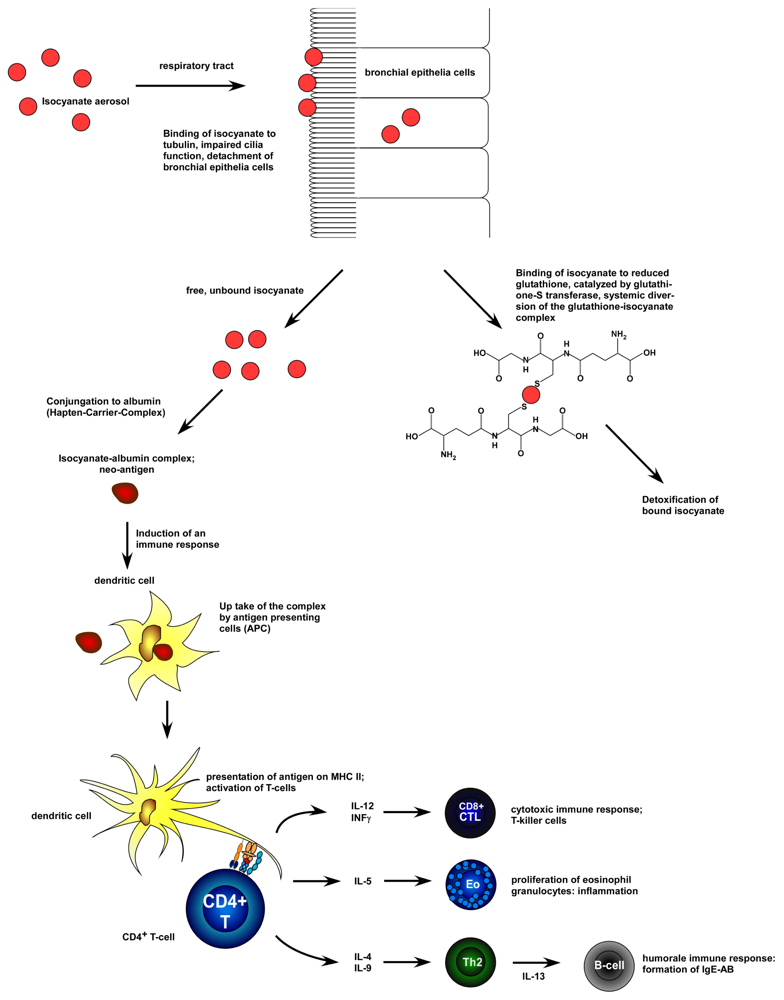
3. Pathogenesis of Isocyanate Asthma
3.1. Influence of Genetic Factors in the Development of an Isocyanate Induced Asthma
4. Diagnosis of Occupational Isocyanate Induced Asthma
5. Future Prospects
- Conflict of InterestThe authors declare no conflict of interest.
References
- International Labour Organization (ILO). Work-Related Fatalities Reach 2 Million Annually; ILO: Geneva, Switzerland, 2002. Avaiable online: http://www.ilo.org/global/about-the-ilo/press-and-media-centre/press-releases/WCMS_007789/lang--en/index.htm accessed on 27 February 2011.
- Ayres, JG; Boyd, R; Cowie, H; Hurley, JF. Costs of occupational asthma in the UK. Thorax 2011, 66, 128–133. [Google Scholar]
- Tarlo, SM; Broder, I. Irritant-induced occupational asthma. Chest 1989, 96, 297–300. [Google Scholar]
- Sastre, J; Vandenplas, O; Park, HS. Pathogenesis of occupational asthma. Eur Respir J 2003, 22, 364–373. [Google Scholar]
- Malo, J-L; Lemière, C; Gautrin, D; Labrecque, M. Occupational asthma. Curr Opin Pulm Med 2004, 10, 57–61. [Google Scholar]
- Dykewicz, MS. Occupational asthma: Current concepts in pathogenesis, diagnosis, and management. J Allergy Clin Immunol 2009, 123, 519–528, quiz 529–530. [Google Scholar]
- Pisati, G; Baruffini, A; Bernabeo, F; Cerri, S; Mangili, A. Rechallenging subjects with occupational asthma due to toluene diisocyanate (TDI), after long-term removal from exposure. Int Arch Occup Environ Health 2007, 80, 298–305. [Google Scholar]
- Piirilä, PL; Meuronen, A; Majuri, M-L; Luukkonen, R; Mäntylä, T; Wolff, HJ; Nordman, H; Alenius, H; Laitinen, A. Inflammation and functional outcome in diisocyanate-induced asthma after cessation of exposure. Allergy 2008, 63, 583–591. [Google Scholar]
- Liu, Q; Wisnewski, AV. Recent developments in diisocyanate asthma. Ann Allergy Asthma Immunol 2003, 90, 35–41. [Google Scholar]
- Wisnewski, AV. Developments in laboratory diagnostics for isocyanate asthma. Curr Opin Allergy Clin Immunol 2007, 7, 138–145. [Google Scholar]
- Baur, X. Isocyanates: Occupational exposures and disorders. Pneumologie 2003, 57, 526–531. [Google Scholar]
- Baur, X; Budnik, LT. New data on occupational exposure to isocyanates. Pneumologie 2009, 63, 656–661. [Google Scholar]
- BAuA-TRGS 430 Isocyanate—Exposition und Überwachung/Technische Regeln für Gefahrstoffe (TRGS)/Gefahrstoffe/Themen von A-Z/Bundesanstalt für Arbeitsschutz und Arbeitsmedizin. Technische Regel für Gefahrstoffe; BAuA: Dortmund, Germany, 2009; 430. Available online: http://www.baua.de/de/Themen-von-A-Z/Gefahrstoffe/TRGS/TRGS-430_content.html accessed September 6 2011.
- Cocker, J. Biological monitoring for isocyanates. Ann Occup Hyg 2011, 55, 127–131. [Google Scholar]
- Mishra, PK; Samarth, RM; Pathak, N; Jain, SK; Banerjee, S; Maudar, KK. Bhopal Gas Tragedy: Review of clinical and experimental findings after 25 years. Int J Occup Med Environ Health 2009, 22, 193–202. [Google Scholar]
- Lemière, C; Romeo, P; Chaboillez, S; Tremblay, C; Malo, J-L. Airway inflammation and functional changes after exposure to different concentrations of isocyanates. J Allergy Clin Immunol 2002, 110, 641–646. [Google Scholar]
- Bakerly, ND; Moore, VC; Vellore, AD; Jaakkola, MS; Robertson, AS; Burge, PS. Fifteen-year trends in occupational asthma: Data from the Shield surveillance scheme. Occup Med (London) 2008, 58, 169–174. [Google Scholar]
- Baur, X. I are we closer to developing threshold limit values for allergens in the workplace? Ann Allergy Asthma Immunol 2003, 90, 11–18. [Google Scholar]
- Dragos, M; Jones, M; Malo, J-L; Ghezzo, H; Gautrin, D. Specific antibodies to diisocyanate and work-related respiratory symptoms in apprentice car-painters. Occup Environ Med 2009, 66, 227–234. [Google Scholar]
- Jones, MG; Floyd, A; Nouri-Aria, KT; Jacobson, MR; Durham, SR; Taylor, AN; Cullinan, P. Is occupational asthma to diisocyanates a non-IgE-mediated disease? J Allergy Clin Immunol 2006, 117, 663–669. [Google Scholar]
- Ye, Y-M; Kim, C-W; Kim, H-R; Kim, H-M; Suh, C-H; Nahm, D-H; Park, H-S; Redlich, CA; Wisnewski, AV. Biophysical determinants of toluene diisocyanate antigenicity associated with exposure and asthma. J Allergy Clin Immunol 2006, 118, 885–891. [Google Scholar]
- Redlich, CA; Karol, MH. Diisocyanate asthma: Clinical aspects and immunopathogenesis. Int Immunopharmacol 2002, 2, 213–224. [Google Scholar]
- Wisnewski, AV; Jones, M. Pro/Con debate: Is occupational asthma induced by isocyanates an immunoglobulin E-mediated disease? Clin Exp Allergy 2010, 40, 1155–1162. [Google Scholar]
- Mapp, CE; Boschetto, P; Miotto, D; De Rosa, E. Asthma induced by isocyanates: A model of IgE-independent asthma. Acta Biomed 2005, 76(Suppl 2), 15–19. [Google Scholar]
- Fabbri, LM; Picotti, G; Mapp, CE. Late asthmatic reactions, airway inflammation and chronic asthma in TDI sensitized subjects. Eur Respir J 1991, 13(Suppl), s136–s138. [Google Scholar]
- Fabbri, LM; Maestrelli, P; Saetta, M; Mapp, CE. Airway inflammation during late asthmatic reactions induced by toluene diisocyanate. Am Rev Respir Dis 1991, 143, S37–S38. [Google Scholar]
- Saetta, M; Di Stefano, A; Maestrelli, P; De Marzo, N; Milani, GF; Pivirotto, F; Mapp, CE; Fabbri, LM. Airway mucosal inflammation in occupational asthma induced by toluene diisocyanate. Am Rev Respir Dis 1992, 145, 160–168. [Google Scholar]
- Lange, RW; Lantz, RC; Stolz, DB; Watkins, SC; Sundareshan, P; Lemus, R; Karol, MH. Toluene diisocyanate colocalizes with tubulin on cilia of differentiated human airway epithelial cells. Toxicol Sci 1999, 50, 64–71. [Google Scholar]
- Pons, F; Fischer, A; Frossard, N; Lugnier, A. Effect of toluene diisocyanate and its corresponding amines on viability and growth of human lung fibroblasts in culture. Cell Biol Toxicol 1999, 15, 333–340. [Google Scholar]
- Matheson, JM; Johnson, VJ; Vallyathan, V; Luster, MI. Exposure and immunological determinants in a murine model for toluene diisocyanate (TDI) asthma. Toxicol Sci 2005, 84, 88–98. [Google Scholar]
- Johnson, VJ; Yucesoy, B; Reynolds, JS; Fluharty, K; Wang, W; Richardson, D; Luster, MI. Inhalation of toluene diisocyanate vapor induces allergic rhinitis in mice. J Immunol 2007, 179, 1864–1871. [Google Scholar]
- Marek, W; Mensing, T; Riedel, F; Viso, N; Marczynski, B; Baur, X. Hexamethylene diisocyanate induction of transient airway hyperresponsiveness in guinea pigs. Respiration 1997, 64, 35–44. [Google Scholar]
- Svensson-Elfsmark, L; Koch, BL; Gustafsson, A; Bucht, A. Rats repeatedly exposed to toluene diisocyanate exhibit immune reactivity against methyl isocyanate-protein conjugates. Int Arch Allergy Immunol 2009, 150, 229–236. [Google Scholar]
- Pauluhn, J. Brown Norway rat asthma model of diphenylmethane-4,4′-diisocyanate (MDI): Impact of vehicle for topical induction. Regul Toxicol Pharmacol 2008, 50, 144–154. [Google Scholar]
- Fabbri, LM; Mapp, C. Bronchial hyperresponsiveness, airway inflammation and occupational asthma induced by toluene diisocyanate. Clin Exp Allergy 1991, 21(Suppl 1), 42–47. [Google Scholar]
- Fabbri, LM; Saetta, M; Picotti, G; Mapp, CE. Late asthmatic reactions, airway inflammation and chronic asthma in toluene-diisocyanate-sensitized subjects. Respiration 1991, 58(Suppl 1), 18–21. [Google Scholar]
- Saetta, M; Maestrelli, P; Di Stefano, A; De Marzo, N; Milani, GF; Pivirotto, F; Mapp, CE; Fabbri, LM. Effect of cessation of exposure to toluene diisocyanate (TDI) on bronchial mucosa of subjects with TDI-induced asthma. Am Rev Respir Dis 1992, 145, 169–174. [Google Scholar]
- Saetta, M; Maestrelli, P; Turato, G; Mapp, CE; Milani, G; Pivirotto, F; Fabbri, LM; Di Stefano, A. Airway wall remodeling after cessation of exposure to isocyanates in sensitized asthmatic subjects. Am J Respir Crit Care Med 1995, 151, 489–494. [Google Scholar]
- Maestrelli, P; Del Prete, GF; De Carli, M; D’Elios, MM; Saetta, M; Di Stefano, A; Mapp, CE; Romagnani, S; Fabbri, LM. CD8 T-cell clones producing interleukin-5 and interferon-gamma in bronchial mucosa of patients with asthma induced by toluene diisocyanate. Scand J Work Environ Health 1994, 20, 376–381. [Google Scholar]
- Boulet, L-P; Lemière, C; Gautrin, D; Cartier, A. New insights into occupational asthma. Curr Opin Allergy Clin Immunol 2007, 7, 96–101. [Google Scholar]
- Hur, G-Y; Koh, D-H; Choi, G-S; Park, H-J; Choi, S-J; Ye, Y-M; Kim, K-S; Park, H-S. Clinical and immunologic findings of methylene diphenyl diisocyanate-induced occupational asthma in a car upholstery factory. Clin Exp Allergy 2008, 38, 586–593. [Google Scholar]
- Wisnewski, AV; Liu, Q; Liu, J; Redlich, CA. Human innate immune responses to hexamethylene diisocyanate (HDI) and HDI-albumin conjugates. Clin Exp Allergy 2008, 38, 957–967. [Google Scholar]
- Maestrelli, P; Di Stefano, A; Occari, P; Turato, G; Milani, G; Pivirotto, F; Mapp, CE; Fabbri, LM; Saetta, M. Cytokines in the airway mucosa of subjects with asthma induced by toluene diisocyanate. Am J Respir Crit Care Med 1995, 151, 607–612. [Google Scholar]
- Maestrelli, P; Occari, P; Turato, G; Papiris, SA; Di Stefano, A; Mapp, CE; Milani, GF; Fabbri, LM; Saetta, M. Expression of interleukin (IL)-4 and IL-5 proteins in asthma induced by toluene diisocyanate (TDI). Clin Exp Allergy 1997, 27, 1292–1298. [Google Scholar]
- Wisnewski, AV; Herrick, CA; Liu, Q; Chen, L; Bottomly, K; Redlich, CA. Human gamma/delta T-cell proliferation and IFN-gamma production induced by hexamethylene diisocyanate. J Allergy Clin Immunol 2003, 112, 538–546. [Google Scholar]
- Fabbri, LM; Boschetto, P; Zocca, E; Milani, G; Pivirotto, F; Plebani, M; Burlina, A; Licata, B; Mapp, CE. Bronchoalveolar neutrophilia during late asthmatic reactions induced by toluene diisocyanate. Am Rev Respir Dis 1987, 136, 36–42. [Google Scholar]
- Park, H; Jung, K; Kim, H; Nahm, D; Kang, K. Neutrophil activation following TDI bronchial challenges to the airway secretion from subjects with TDI-induced asthma. Clin Exp Allergy 1999, 29, 1395–1401. [Google Scholar]
- Lee, Y-M; Kim, H-A; Park, H-S; Lee, S-K; Nahm, D-H. Exposure to toluene diisocyanate (TDI) induces IL-8 production from bronchial epithelial cells: Effect of pro-inflammatory cytokines. J Korean Med Sci 2003, 18, 809–812. [Google Scholar]
- Park, H-S; Kim, H-A; Jung, J-W; Kim, Y-K; Lee, S-K; Kim, S-S; Nahm, D-H. Metalloproteinase-9 is increased after toluene diisocyanate exposure in the induced sputum from patients with toluene diisocyanate-induced asthma. Clin Exp Allergy 2003, 33, 113–118. [Google Scholar]
- Piirilä, P; Lauhio, A; Majuri, M-L; Meuronen, A; Myllärniemi, M; Tervahartiala, T; Vuorinen, K; Laitinen, A; Alenius, H; Kinnula, VL; et al. Matrix metalloproteinases-7, -8, -9 and TIMP-1 in the follow-up of diisocyanate-induced asthma. Allergy 2010, 65, 61–68. [Google Scholar]
- Zocca, E; Fabbri, LM; Boschetto, P; Plebani, M; Masiero, M; Milani, GF; Pivirotto, F; Mapp, CE. Leukotriene B4 and late asthmatic reactions induced by toluene diisocyanate. J Appl Physiol 1990, 68, 1576–1580. [Google Scholar]
- Scheerens, H; Buckley, TL; Muis, T; Van Loveren, H; Nijkamp, FP. The involvement of sensory neuropeptides in toluene diisocyanate-induced tracheal hyperreactivity in the mouse airways. Br J Pharmacol 1996, 119, 1665–1671. [Google Scholar]
- Mapp, CE; Lucchini, RE; Miotto, D; Chitano, P; Jovine, L; Saetta, M; Maestrelli, P; Springall, DR; Polak, J; Fabbri, LM. Immunization and challenge with toluene diisocyanate decrease tachykinin and calcitonin gene-related peptide immunoreactivity in guinea pig central airways. Am J Respir Crit Care Med 1998, 158, 263–269. [Google Scholar]
- Redlich, CA. Skin exposure and asthma: Is there a connection? Proc Am Thorac Soc 2010, 7, 134–137. [Google Scholar]
- Redlich, CA; Herrick, CA. Lung/skin connections in occupational lung disease. Curr Opin Allergy Clin Immunol 2008, 8, 115–119. [Google Scholar]
- De Vooght, V; Haenen, S; Verbeken, E; Nemery, B; Hoet, PHM; Vanoirbeek, JAJ. Successful transfer of chemical-induced asthma by adoptive transfer of low amounts of lymphocytes in a mouse model. Toxicology 2011, 279, 85–90. [Google Scholar]
- Wisnewski, AV; Liu, Q; Liu, J; Redlich, CA. Glutathione protects human airway proteins and epithelial cells from isocyanates. Clin Exp Allergy 2005, 35, 352–357. [Google Scholar]
- Ye, Y-M; Nahm, D-H; Kim, C-W; Kim, H-R; Hong, C-S; Park, C-S; Suh, C-H; Park, H-S. Cytokeratin autoantibodies: Useful serologic markers for toluene diisocyanate-induced asthma. Yonsei Med J 2006, 47, 773–781. [Google Scholar]
- Wisnewski, AV; Liu, J; Redlich, CA. Antigenic changes in human albumin caused by reactivity with the occupational allergen diphenylmethane diisocyanate. Anal Biochem 2010, 400, 251–258. [Google Scholar]
- Wisnewski, AV; Stowe, MH; Cartier, A; Liu, Q; Liu, J; Chen, L; Redlich, CA. Isocyanate vapor-induced antigenicity of human albumin. J Allergy Clin Immunol 2004, 113, 1178–1184. [Google Scholar]
- Beck, LA; Leung, DY. Allergen sensitization through the skin induces systemic allergic responses. J Allergy Clin Immunol 2000, 106, S258–S263. [Google Scholar]
- Piirilä, P; Wikman, H; Luukkonen, R; Kääriä, K; Rosenberg, C; Nordman, H; Norppa, H; Vainio, H; Hirvonen, A. Glutathione S-transferase genotypes and allergic responses to diisocyanate exposure. Pharmacogenetics 2001, 11, 437–445. [Google Scholar]
- Mapp, CE; Fryer, AA; De Marzo, N; Pozzato, V; Padoan, M; Boschetto, P; Strange, RC; Hemmingsen, A; Spiteri, MA. Glutathione S-transferase GSTP1 is a susceptibility gene for occupational asthma induced by isocyanates. J Allergy Clin Immunol 2002, 109, 867–872. [Google Scholar]
- Fryer, AA; Bianco, A; Hepple, M; Jones, PW; Strange, RC; Spiteri, MA. Polymorphism at the glutathione S-transferase GSTP1 locus. A new marker for bronchial hyperresponsiveness and asthma. Am J Respir Crit Care Med 2000, 161, 1437–1442. [Google Scholar]
- Broberg, K; Tinnerberg, H; Axmon, A; Warholm, M; Rannug, A; Littorin, M. Influence of genetic factors on toluene diisocyanate-related symptoms: Evidence from a cross-sectional study. Environ Health 2008, 7, 15. [Google Scholar]
- Broberg, KE; Warholm, M; Tinnerberg, H; Axmon, A; Jönsson, BA; Sennbro, CJ; Littorin, M; Rannug, A. The GSTP1 Ile105 Val polymorphism modifies the metabolism of toluene diisocyanate. Pharmacogenet Genomics 2010, 20, 104–111. [Google Scholar]
- Mapp, CE; Beghè, B; Balboni, A; Zamorani, G; Padoan, M; Jovine, L; Baricordi, OR; Fabbri, LM. Association between HLA genes and susceptibility to toluene diisocyanate-induced asthma. Clin Exp Allergy 2000, 30, 651–656. [Google Scholar]
- Rihs, HP; Barbalho-Krölls, T; Huber, H; Baur, X. No evidence for the influence of HLA class II in alleles in isocyanate-induced asthma. Am J Ind Med 1997, 32, 522–527. [Google Scholar]
- Choi, J-H; Lee, K-W; Kim, C-W; Park, C-S; Lee, H-Y; Hur, G-Y; Kim, S-H; Hong, C-S; Jang, A-S; Park, H-S. The HLA DRB1*1501-DQB1*0602-DPB1*0501 haplotype is a risk factor for toluene diisocyanate-induced occupational asthma. Int Arch Allergy Immunol 2009, 150, 156–163. [Google Scholar]
- Beghé, B; Padoan, M; Moss, CT; Barton, SJ; Holloway, JW; Holgate, ST; Howell, WM; Mapp, CE. Lack of association of HLA class I genes and TNF alpha-308 polymorphism in toluene diisocyanate-induced asthma. Allergy 2004, 59, 61–64. [Google Scholar]
- Kim, S-H; Cho, B-Y; Park, C-S; Shin, E-S; Cho, E-Y; Yang, E-M; Kim, C-W; Hong, C-S; Lee, J-E; Park, H-S. Alpha-T-catenin (CTNNA3) gene was identified as a risk variant for toluene diisocyanate-induced asthma by genome-wide association analysis. Clin Exp Allergy 2009, 39, 203–212. [Google Scholar]
- Wikman, H; Piirilä, P; Rosenberg, C; Luukkonen, R; Kääriä, K; Nordman, H; Norppa, H; Vainio, H; Hirvonen, A. N-Acetyltransferase genotypes as modifiers of diisocyanate exposure-associated asthma risk. Pharmacogenetics 2002, 12, 227–233. [Google Scholar]
- Bernstein, DI; Wang, N; Campo, P; Chakraborty, R; Smith, A; Cartier, A; Boulet, L-P; Malo, J-L; Yucesoy, B; Luster, M; et al. Diisocyanate asthma and gene-environment interactions with IL4RA, CD-14, and IL-13 genes. Ann Allergy Asthma Immunol 2006, 97, 800–806. [Google Scholar]
- Bernstein, DI; Kissling, GE; Khurana Hershey, G; Yucesoy, B; Johnson, VJ; Cartier, A; Gautrin, D; Sastre, J; Boulet, L-P; Malo, J-L; et al. Hexamethylene diisocyanate asthma is associated with genetic polymorphisms of CD14, IL-13, and IL-4 receptor α. J Allergy Clin Immunol 2011, 128, 418–420. [Google Scholar]
- Baur, X. Bronchial challenge tests. Pneumologie 2011, 65, 340–346. [Google Scholar]
- Tarlo, SM; Balmes, J; Balkissoon, R; Beach, J; Beckett, W; Bernstein, D; Blanc, PD; Brooks, SM; Cowl, CT; Daroowalla, F; et al. Diagnosis and management of work-related asthma: American College Of Chest Physicians Consensus Statement. Chest 2008, 134, S1–S41. [Google Scholar]
- Banks, DE. Use of the specific challenge in the diagnosis of occupational asthma: A “gold standard” test or a test not used in current practice of occupational asthma? Curr Opin Allergy Clin Immunol 2003, 3, 101–107. [Google Scholar]
- Sastre, J; Fernández-Nieto, M; Novalbos, A; De Las Heras, M; Cuesta, J; Quirce, S. Need for monitoring nonspecific bronchial hyperresponsiveness before and after isocyanate inhalation challenge. Chest 2003, 123, 1276–1279. [Google Scholar]
- Caron, S; Boileau, J-C; Malo, J-L; Leblond, S. New methodology for specific inhalation challenges with occupational agents. Respir Res 2010, 11, 72. [Google Scholar]
- Piirilä, PL; Nordman, H; Keskinen, HM; Luukkonen, R; Salo, SP; Tuomi, TO; Tuppurainen, M. Long-term follow-up of hexamethylene diisocyanate-, diphenylmethane diisocyanate-, and toluene diisocyanate-induced asthma. Am J Respir Crit Care Med 2000, 162, 516–522. [Google Scholar]
- Palikhe, NS; Kim, J-H; Park, H-S. Biomarkers predicting isocyanate-induced asthma. Allergy Asthma Immunol Res 2011, 3, 21–26. [Google Scholar]


{kind=link}
| Diagnostic Approach | Result |
|---|---|
| Medical examination | |
| Occupational anamnesis, exposure on the job | Clinical verification of the asthmatic disease Confirmation of isocyanate exposure: characterization of the chemical substances Specification of the grade of exposure |
| Physiological tests: | |
| Metacholine provocation test Spirometry PERFs (peak expiratory flow rate) | Confirmation of the diagnose “asthma” and documentation of the occupational causation |
| SIC (specific inhalation challenge) | “Diagnostic reference standard”, characterization of the specific substance |
| Immunological investigations | |
| Isocyanate specific IgE | Strong indicator for isocyanate induced asthma, not very sensitive |
| Isocyanate specific IgG | Conformation of exposure towards isocyanate |
© 2011 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Fisseler-Eckhoff, A.; Bartsch, H.; Zinsky, R.; Schirren, J. Environmental Isocyanate-Induced Asthma: Morphologic and Pathogenetic Aspects of an Increasing Occupational Disease. Int. J. Environ. Res. Public Health 2011, 8, 3672-3687. https://doi.org/10.3390/ijerph8093672
Fisseler-Eckhoff A, Bartsch H, Zinsky R, Schirren J. Environmental Isocyanate-Induced Asthma: Morphologic and Pathogenetic Aspects of an Increasing Occupational Disease. International Journal of Environmental Research and Public Health. 2011; 8(9):3672-3687. https://doi.org/10.3390/ijerph8093672
Chicago/Turabian StyleFisseler-Eckhoff, Annette, Holger Bartsch, Rica Zinsky, and Joachim Schirren. 2011. "Environmental Isocyanate-Induced Asthma: Morphologic and Pathogenetic Aspects of an Increasing Occupational Disease" International Journal of Environmental Research and Public Health 8, no. 9: 3672-3687. https://doi.org/10.3390/ijerph8093672