Evaluation of the Impact of the Plastic BioSand Filter on Health and Drinking Water Quality in Rural Tamale, Ghana

Abstract
:1. Introduction

2. Materials and Methods
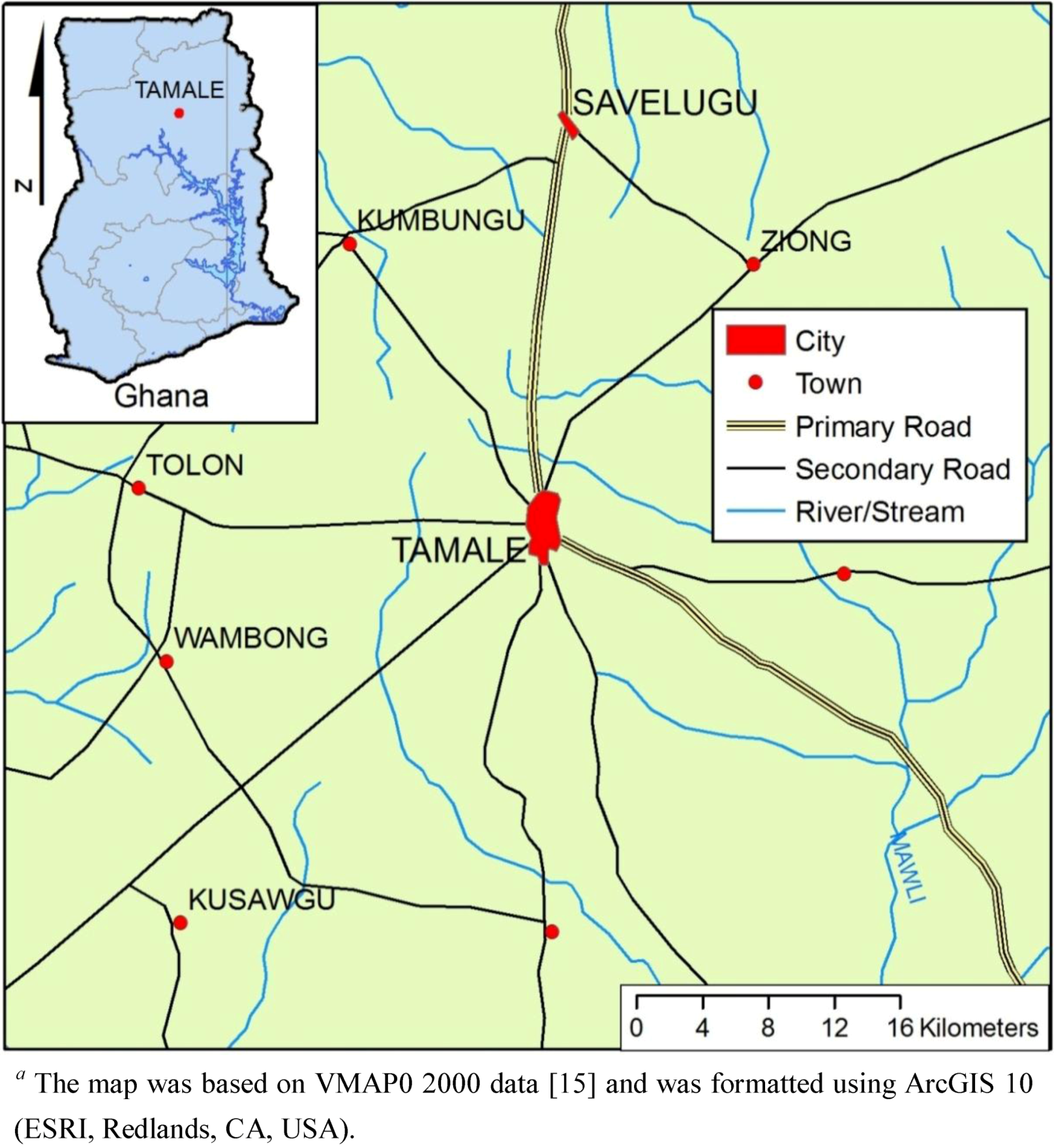
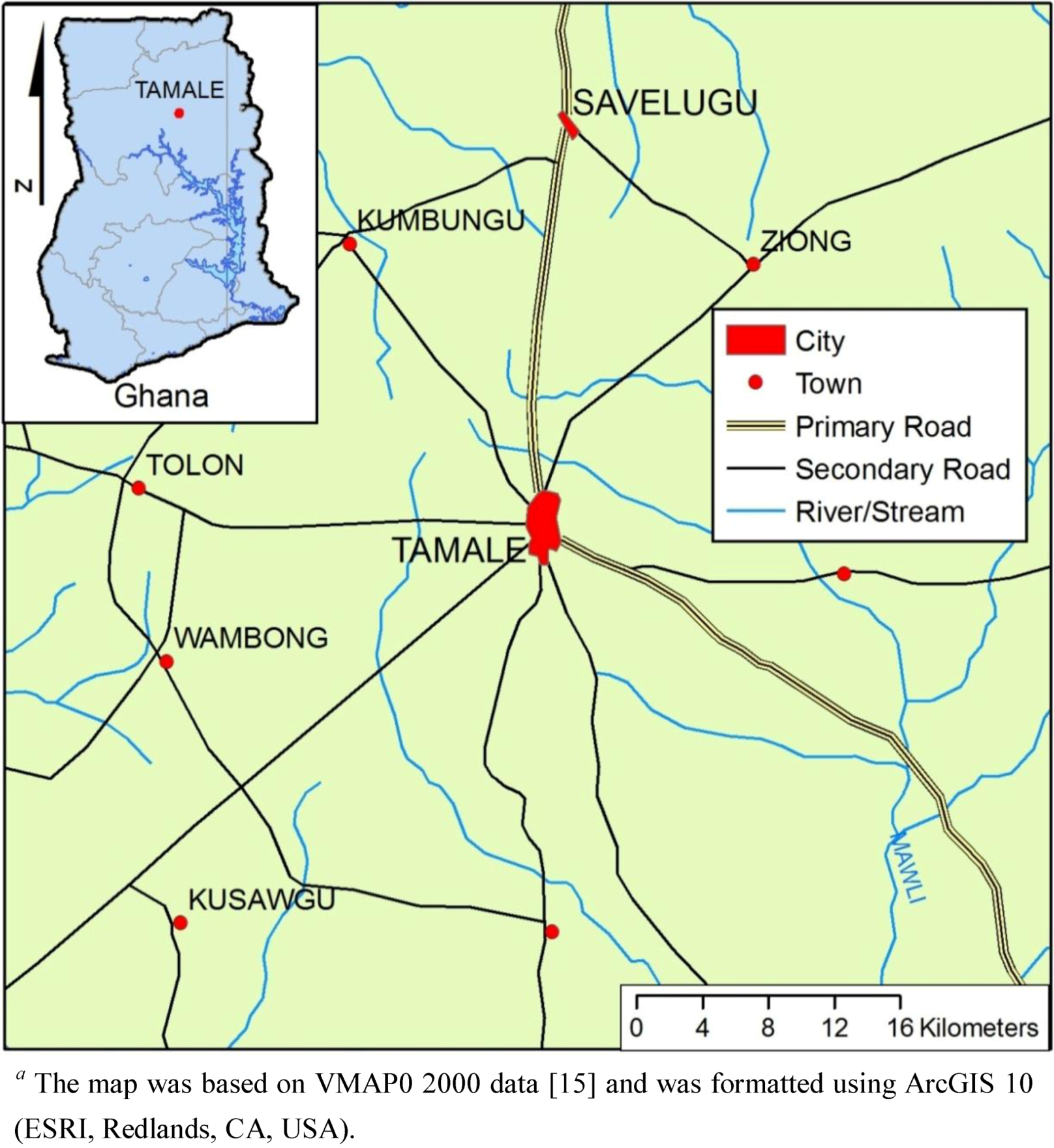
2.1. Research Setting, Study Population, and Participant Recruitment
2.2. Intervention
2.3. Diarrheal Disease Surveillance
2.4. Water Quality Sample Collection and Analysis
2.5. Data Analysis
3. Results
3.1. Study Enrollment and Completion
3.2. Baseline Characteristics and Group Comparability

{kind=link}
{kind=link}
{kind=link}
| Individual Variables | Control | Intervention | p values |
| (N = 1031) | (N = 1012) | Pearson χ2 test | |
| Age | N (%) | N (%) | |
| Participants ≥ 5 years old | 809 (78.5) | 794 (78.5) | |
| Participants 2–4 | 146 (14.3) | 116 (11.5) | |
| Participants <2 | 76 (7.4) | 102 (10.2) | 0.027 a |
| Sex | |||
| Male (≥5) | 436 (42) | 391 (39) | |
| Male (<5) | 113 (11) | 116 (11) | 0.37 a |
| Female (≥5) | 373 (36) | 401 (40) | |
| Female (<5) | 108 (11) | 104 (10) | 0.12 a |
| Ever or currently attending school | 261 (25.3) | 260 (25.7) | 0.85 |
| Household Level Variables | Control | Intervention | p values |
|---|---|---|---|
| (N = 143) | (N = 117) | (χ2 test) | |
| Use surface water during dry season | 95.0% | 98.3% | 0.16 |
| Use surface water during rainy season | 70.6% | 94.0% | <0.001 |
| Reported sieving drinking water through cloth | 96.5% | 96.6% | 0.97 |
| At least one person attending school in household | 70.4% | 74.8% | 0.39 |
| Lack access to sanitation a | 97.1% | 98.3% | 0.67 |
| Multi-child household b | 56.7% | 55.6% | 0.86 |
3.3. Diarrheal Disease
| Data collection Period | Age stratum | Unadjusted LP a—Control Villages | Unadjusted LP a—Plastic BSF Villages | Adjusted LPR (95% CI) |
|---|---|---|---|---|
| Baseline (May–August 2008) b | All | 0.024 | 0.020 | 0.98 (0.23, 3.95) c |
| <2 years of age | 0.081 | 0.10 | 1.56 (0.25, 9.83) d | |
| <5 years of age | 0.078 | 0.074 | 1.38 (0.19, 10.17) d | |
| Plastic BSF Intervention (September–December 2008) | All | 0.012 | 0.0063 | 0.40 (0.05, 0.80) c |
| <2 years of age | 0.028 | 0.015 | 0.37 (0.15, 0.90) d | |
| <5 years of age | 0.034 | 0.018 | 0.26 (0.07, 0.89) d |
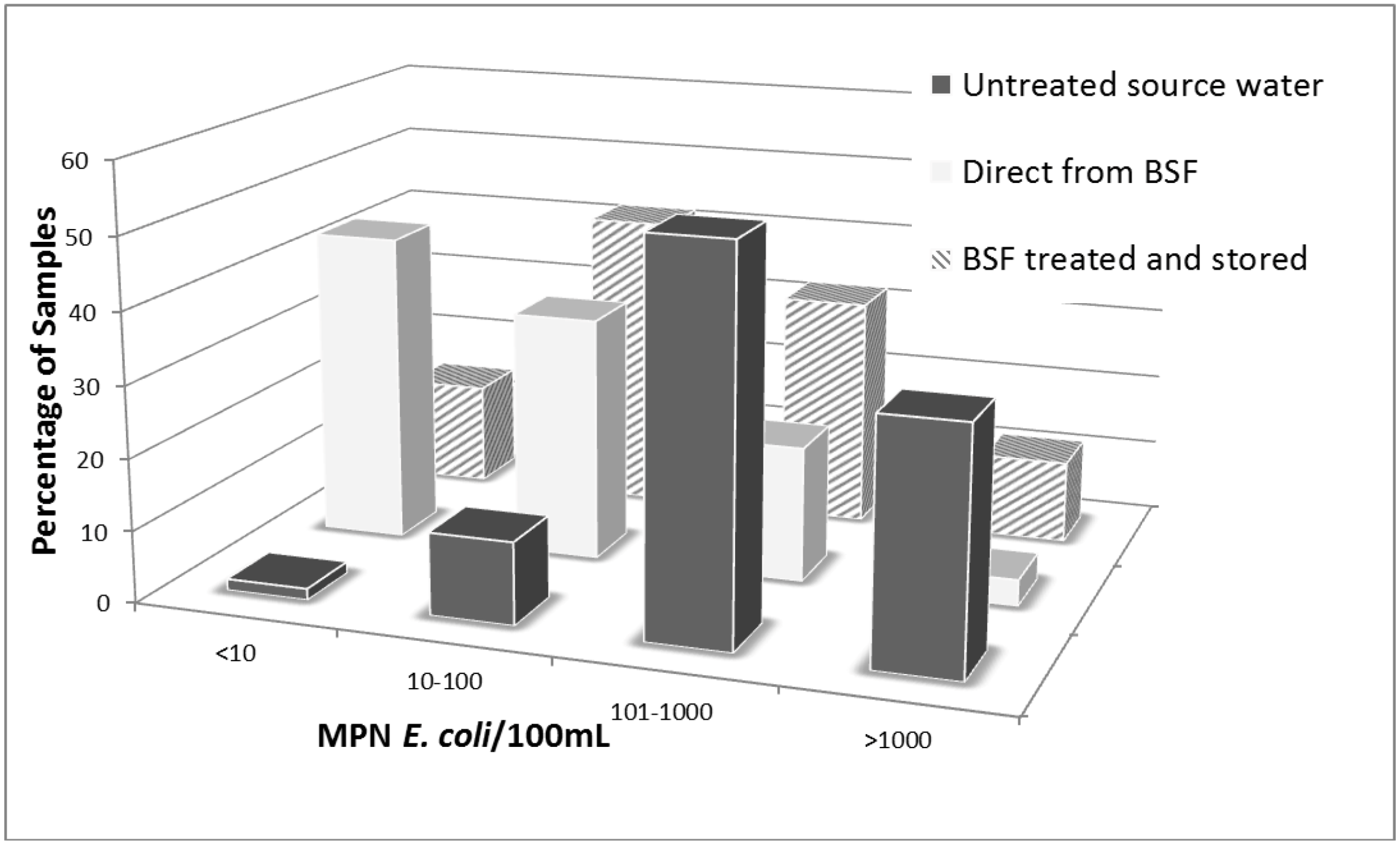
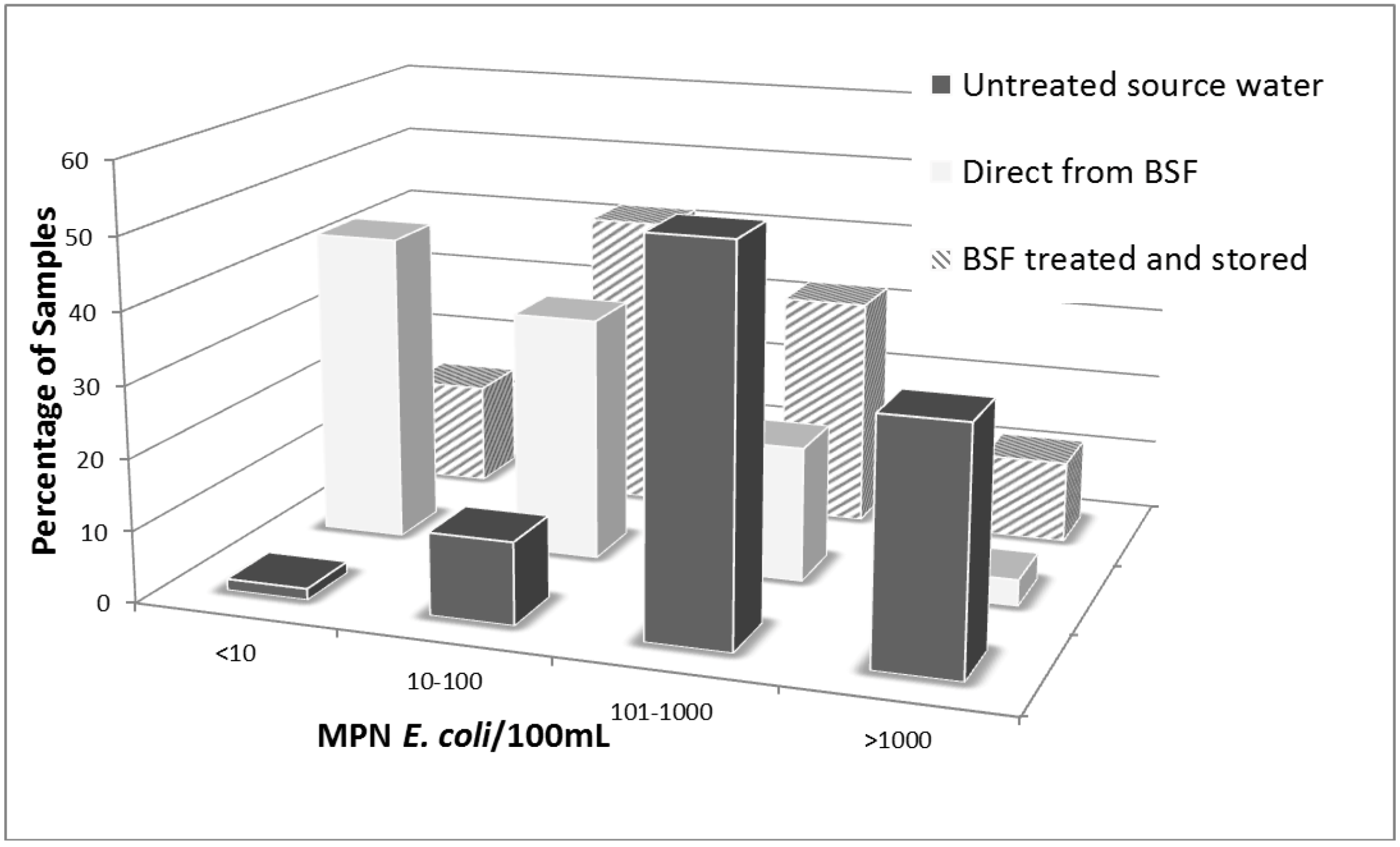
3.4. Water Quality Analysis
| Baseline (May–August 2008) | Plastic BSF Intervention (September–December 2008) | |||||
|---|---|---|---|---|---|---|
| Water Quality Parameter | Control HH Water | Plastic BSF HH Water | Control HH Water | Plastic BSF Untreated Water b | Plastic BSF Direct Filtrate | Plastic BSF Stored Filtrate |
| E. coli (95%CI) a | 724 (631–851) | 832 (724–977) | 490 (426–549) | 437 (380–501) | 16 (13–20) | 76 (62–91) |
| (N = 516) | (N = 424) | (N = 587) | (N = 385) | (N = 382) | (N = 381) | |
| NTU | 95 (83–109) | 85 (74–98) | 25 (23–27) | 47 (42–51) | 15 (13–17) | 15 (14–18) |
| (N = 523) | (N = 430) | (N = 787) | (N = 527) | (N = 524) | (N = 527) | |
| % E. coli Reductions c | -- | -- | -- | -- | 97 | 85 |
| % NTU Reductions c | -- | -- | -- | -- | 67 | 66 |
3.5. Plastic BSF Performance
4. Discussion
4.1. Effect of the Plastic BSF on Household Drinking Water Quality
5. Conclusions
Acknowledgments
Conflict of Interest
References
- WHO/UNICEF Joint Monitoring Programme. In Progress on Sanitation and Drinking Water: 2012 Update; WHO, UNICEF: Geneva, Switzerland.
- Ghana Demographic and Health Survey (Ghana DHS), 2008. Available online: http://www.measuredhs.com/pubs/pdf/FR221/FR221.pdf (accessed on 23 September 2011).
- Fewtrell, L.; Kaufmann, R.B.; Kay, D.; Enanoria, W.; Haller, L.; Colford, J.M., Jr. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis. Lancet Infect. Dis. 2005, 5, 42–52. [Google Scholar] [CrossRef]
- Clasen, T.; Schmidt, W.P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: systematic review and meta-analysis. BMJ 2007, 334, 782–785. [Google Scholar]
- Manz Water Info database. Available online: www.manzwaterinfo.ca (accessed on 6 August 2012).
- Sobsey, M.; Stauber, C.E.; Casanova, L.M.; Brown, J.M.; Elliott, M.A. Point of use household drinking water filtration: a practical, effective solution for providing sustained access to safe drinking water in the developing world. Environ. Sci. Technol. 2008, 42, 4261–4267. [Google Scholar]
- Stauber, C.E.; Ortiz, G.M.; Loomis, D.P.; Sobsey, M.D. A randomized controlled trial of the concrete biosand filter and its impact on diarrheal disease in Bonao, Dominican Republic. Am. J. Trop. Med. Hyg. 2009, 80, 286–293. [Google Scholar]
- Tiwari, S.; Schmidt, W.P.; Darby, J.; Kariuki, Z.G.; Jenkins, M.W. Intermittent slow sand filtration for preventing diarrhoea among children in households using unimproved water sources: a randomized controlled trial. Trop. Med. Int. Health 2009, 14, 1374–1382. [Google Scholar] [CrossRef]
- Liang, K.; Sobsey, M.; Stauber, C. Field Note: Improving Household Water Quality—Use of Biosand Filters in Cambodia. Water and Sanitation Program—Cambodia. 2010. Available online: http://www.wsp.org/wsp/sites/wsp.org/files/publications/WSP_biosand_cambodia.pdf (accessed on 23 September 2011).
- Aiken, B.A.; Stauber, C.E.; Ortiz, G.M.; Sobsey, M.D. An assessment of continued use and health impact of the concrete biosand filter in Bonao, Dominican Republic. Am. J. Trop. Med. Hyg. 2011, 85, 309–317. [Google Scholar] [CrossRef]
- Clasen, T. Scaling Up Household Water Treatment among Low-Income Populations; WHO/HSE/WSH/09.02; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Stauber, C.E.; Printy, E.R.; McCarty, F.A.; Liang, K.R.; Sobsey, M.D. Cluster randomized trial of the plastic biosand water filter in Cambodia. Environ. Sci. Technol. 2012, 46, 722–728. [Google Scholar]
- Fabiszewski de Aceituno, A.M.; Stauber, C.E.; Walters, A.R.; Meza Sanchez, R.E.; Sobsey, M.D. A randomized controlled trial of the plastic-housing biosand filter and its impact on diarrheal disease in Copan, Honduras. Am. J. Trop. Med. Hyg. 2012, 86, 913–921. [Google Scholar] [CrossRef]
- Cobbina, S.J.; Anyidoho, L.Y.; Nyame, F.; Hodgson, I.O.A. Water quality status of dugouts from five districts in Northern Ghana: Implications for sustainable water resources management in a water stressed tropical savannah environment. Environ. Monit. Assess. 2010, 167, 405–416. [Google Scholar] [CrossRef]
- GISuser.com website. Available online: www.gisuser.com (accessed on 24 September 2012).
- du Preez, M.; Conroy, R.M.; Wright, J.A.; Moyo, S.; Potgieter, N.; Gundry, S.W. Use of ceramic water filtration in the prevention of diarrheal disease: a randomized controlled trial in rural South Africa and Zimbabwe. Am. J. Trop. Med. Hyg. 2008, 79, 696–701. [Google Scholar]
- Arnold, B.; Colford, J. Treating water with chlorine at point-of-use to reduce child diarrhea and improve water quality in developing countries: a systemic review and meta-analysis. Am. J. Trop. Med. Hyg. 2007, 76, 354–364. [Google Scholar]
- Schmidt, W.; Cairncross, S. Household water treatment in poor populations: is there enough evidence for scaling up now? Environ. Sci. Technol. 2009, 43, 986–992. [Google Scholar] [CrossRef]
- Clasen, T.; Bartram, J.; Colford, J.; Luby, S.; Quick, R.; Sobsey, M. Comment on “Household water treatment in poor populations: is there enough evidence for scaling up now?”. Environ. Sci. Technol. 2009, 53, 5542–5544. [Google Scholar]
- Hunter, P. Household water treatment in developing countries: comparing different intervention types using meta-regression. Environ. Sci. Technol. 2009, 43, 8991–8997. [Google Scholar]
- Boisson, S.; Kiyombo, M.; Sthreshley, L.; Tumba, S.; Makambo, J.; Clasen, T. Field assessment of a novel household-based water filtration device: a randomized, placebo-controlled trial in the Democratic Republic of Congo. PLoS ONE 2010, 5, e12613. [Google Scholar]
- du Preez, M.; Conroy, R.M.; Ligondo, S.; Hennessy, J.; Elmore-Meegan, M.; Soita, A.; McGuigan, K.G. Randomized intervention study of solar disinfection of drinking water in the prevention of dysentery in Kenyan children aged under 5 years. Environ. Sci. Technol. 2011, 45, 9315–9323. [Google Scholar]
- Arnold, B.; Mausezahl, D.; Schmidt, W.P.; Christen, A.; Colford, J.M., Jr. Comment on randomized intervention study of solar disinfection of drinking water in the prevention of dysentery in Kenyan children aged under 5 years. Environ. Sci. Technol. 2012, 46, 3031–3032. [Google Scholar]
- Hunter, P.; Bartram, J.; Cairncross, S. Comment on randomized intervention study of solar disinfection of drinking water in the prevention of dysentery in Kenyan children aged under 5 years. Environ. Sci. Technol. 2012, 46, 3035. [Google Scholar]
- Clasen, T.F.; Brown, J.; Collin, S.M. Preventing diarrhoea with household ceramic water filters: assessment of a pilot project in Bolivia. Int. J. Environ. Health Res. 2006, 16, 231–239. [Google Scholar] [CrossRef]
- Duke, W.F.; Nordin, R.N.; Baker, D.; Mazumder, A. The use and performance of BioSand filters in the Artibonite Valley of Haiti: A field study of 107 households. Rural Rem. Health 2006, 6, 570. [Google Scholar]
- Elliott, M.A.; Stauber, C.E.; Koksal, F.; DiGiano, F.A.; Sobsey, M. Reductions of E. coli, echovirus type 12 and bacteriophages in an intermittently operated household-scale slow sand filter. Wat. Res. 2008, 42, 2662–2670. [Google Scholar]
- Palmateer, G.; Manz, D.; Jurkovic, A.; McInnis, R.; Unger, S.; Kwan, K.K.; Dutka, B.J. Toxicant and parasite challenge of manz intermittent slow sand filter. Environ. Tox. 1999, 14, 217–225. [Google Scholar] [CrossRef]
- Elliott, M.A.; DiGiano, F.A.; Sobsey, M.D. Virus attenuation by microbial mechanisms during the idle time of a household slow sand filter. Wat. Res. 2011, 45, 4092–4102. [Google Scholar]
- Binka, F.K. The incidence and risk factors of pediatric rotavirus diarrhea in Northern Ghana. Trop. Med. Int. Health. 2003, 8, 840–846. [Google Scholar] [CrossRef]
- Fiore, M.M.; Minnings, K.; Fiore, L.D. Assessment of biosand filter performance in rural communities in southern coastal Nicaragua: An evaluation of 199 households. Rural Rem. Health 2010, 10, 1483. [Google Scholar]
- Psutka, R.; Peletz, R.; Michelo, S.; Kelly, P.; Clasen, T. Assessing the microbiological performance and potential cost of boiling drinking water in urban Zambia. Environ. Sci. Technol. 2011, 15, 6095–6101. [Google Scholar]
- Crump, J.A.; Otieno, P.O.; Slutsker, L.; Keswick, B.H.; Rosen, D.H.; Hoekstra, R.M.; Vulule, J.M.; Luby, S.P. Household based treatment of drinking water with flocculant-disinfectant for preventing diarrhoea in areas with turbid source water in rural western Kenya: Cluster randomised controlled trial. BMJ 2005, 331. [Google Scholar] [CrossRef]
- Crump, J.A.; Okoth, G.O.; Slutsker, L.; Ogaja, D.O.; Keswick, B.H.; Luby, S.P. Effect of point-of-use disinfection, flocculation and combined flocculation-disinfection on drinking water quality in western Kenya. J. Appl. Microbiol. 2004, 97, 225–231. [Google Scholar] [CrossRef]
- Mwabi, J.K.; Mamba, B.B.; Momba, M.N. Removal of Escherichia coli and faecal coliforms from surface water and groundwater by household water treatment devices/systems: A sustainable solution for improving water quality in rural communities of the Southern African development community region. Int. J. Environ. Res. Public Health 2012, 9, 139–170. [Google Scholar] [CrossRef]
- Zwane, A.P.; Zinman, J.; Van Dusen, E.; Pariente, W.; Null, C.; Miguel, E.; Kremer, M.; Karlan, D.S.; Hornbeck, R.; Giné, X.; et al. Being surveyed can change later behavior and related parameter estimates. PNAS 2011, 108, 1821–1826. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Stauber, C.E.; Kominek, B.; Liang, K.R.; Osman, M.K.; Sobsey, M.D. Evaluation of the Impact of the Plastic BioSand Filter on Health and Drinking Water Quality in Rural Tamale, Ghana. Int. J. Environ. Res. Public Health 2012, 9, 3806-3823. https://doi.org/10.3390/ijerph9113806
Stauber CE, Kominek B, Liang KR, Osman MK, Sobsey MD. Evaluation of the Impact of the Plastic BioSand Filter on Health and Drinking Water Quality in Rural Tamale, Ghana. International Journal of Environmental Research and Public Health. 2012; 9(11):3806-3823. https://doi.org/10.3390/ijerph9113806
Chicago/Turabian StyleStauber, Christine E., Byron Kominek, Kaida R. Liang, Mumuni K. Osman, and Mark D. Sobsey. 2012. "Evaluation of the Impact of the Plastic BioSand Filter on Health and Drinking Water Quality in Rural Tamale, Ghana" International Journal of Environmental Research and Public Health 9, no. 11: 3806-3823. https://doi.org/10.3390/ijerph9113806