Application of a Novel Method for Assessing Cumulative Risk Burden by County

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Human Security Index
2.2. Data

{kind=link}
| Eigen Value | Factor Loadings | ||
|---|---|---|---|
| Economic Fabric Factor | 3.11 | ||
| Poverty | 0.94 | ||
| Unemployment | 0.50 | ||
| Median Household Income | 0.92 | ||
| Inequality (Gini Co-efficient) | −0.77 | ||
| % of population on Food Stamps | 0.80 | ||
| Environmental Fabric Factor | 1.46 | ||
| Particulate Days > EPA threshold | 0.41 | ||
| Ozone Days > EPA threshold | 0.75 | ||
| CO2 emissions | −0.20 | ||
| Natural Amenity Rank | 0.17 | ||
| Population change 2000–2009 | 0.79 | ||
| Social Fabric Factor | |||
| Education Subcomponent | 3.24 | ||
| High school graduate (incl. equivalency) | |||
| Average Freshman Graduate Rate | 0.30 | ||
| % population 25 yrs or older High school graduate (incl. equivalency) | 0.96 | ||
| % population > 25 yrs some college incl. Associate Degree | 0.68 | ||
| % population > 25 yrs with Bachelors degree | 0.58 | ||
| %Adult Literacy (below BPLS) | 0.95 | ||
| % not proficient in English | 0.73 | ||
| Health Subcomponent | 2.39 | ||
| M&F Life Expectancy at Birth | 0.84 | ||
| Lesser of F or M LE change 1985–2006 | −0.40 | ||
| YPLL Premature Death Rate | 0.84 | ||
| % Adult obesity | 0.65 | ||
| Motor vehicle mortality rate | 0.60 | ||
| Chlamydia Rate | 0.14 | ||
| % Adult uninsured | −0.35 | ||
| % Zip codes with Healthy Food Access outlets | 0.09 | ||
| Crime Subcomponent | 1.30 | ||
| Violent Crimes | 0.82 | ||
| Property crimes per 10,000 population | −0.10 | ||
| Incarceration | 0.79 | ||
| Social Stress Subcomponent | 3.02 | ||
| % Child Poverty | 0.85 | ||
| Mentally Unhealthy Days | 0.59 | ||
| Teen Birth Rate | 0.80 | ||
| Mortgage foreclosure Rate | 0.25 | ||
| Housing vacancy rate (excl. vacation/seasonal vacation rate) | −0.12 | ||
| Inadequate Social Support (%) | 0.32 | ||
| Grandparent performing parental Role % | 0.60 | ||
| Creative share | 0.87 | ||
| Commute Index (% Drive Alone*Commute Time) | −0.06 | ||
| Factor loading >0.5 | |
|---|---|
| Economic Fabric Factor | |
| Poverty | |
| Unemployment | |
| Median Household Income | |
| Inequality (Gini Co-efficient)% Population on food Stamps | |
| Environmental Fabric Factor | |
| Ozone Days > EPA Threshold | |
| Population Change 2000–2009 | |
| Social Fabric Factor | |
| Educational Subcomponent | |
| % Population > 25 yrs High School Graduate | |
| % Population > 25 yrs with Bachelors Degree | |
| % Population Adult Literacy | |
| % Not proficient in English | |
| Health Subcomponent | |
| Male and Female Life Expectancy at Birth | |
| Year Potential Life Lost Rate | |
| Adult Obesity | |
| Motor Vehicle mortality | |
| Crime and Punishment Subcomponent | |
| Violent Crime | |
| Incarceration Rate | |
| Social Stress Subcomponent | |
| Child Poverty | |
| Teen Birth Rate | |
| Insufficient Social Support | |
| Grandparent in Parental Role | |
| Creative Share Occupations | |
3. Results
3.1. HSI Association with Ethnicity/Race and Texas-Mexico Border Region
| African American | Hispanic | Immigrant | |
|---|---|---|---|
| Economic Fabric | 0.0865 (0.1873) | 0.4292 (0.0000) | 0.1354 (0.0385) |
| Environmental Fabric | 0.0851 (0.1944) | −0.1533 (0.0190) | 0.1969 (0.0025) |
| Social Fabric | 0.0451 (0.4919) | 0.5827 (0.0000) | 0.3372 (0.0000) |
| Education Subcomponent | −0.2471 (0.0001) | 0.8721 (0.0000) | 0.6996 (0.0000) |
| Health Subcomponent | 0.2096 (0.0013) | −0.3116 (0.0000) | −0.3756 (0.0000) |
| Crime Subcomponent | 0.3270 (0.0000) | 0.0907 (0.1667) | 0.0593 (0.3666) |
| Social Stress Subcomponent | −0.0096 (0.8840) | 0.3928 (0.0000) | 0.0878 (0.1805) |
| Total HSI | 0.1367 (0.0367) | 0.3013 (0.0000) | 0.4231 (0.0000) |
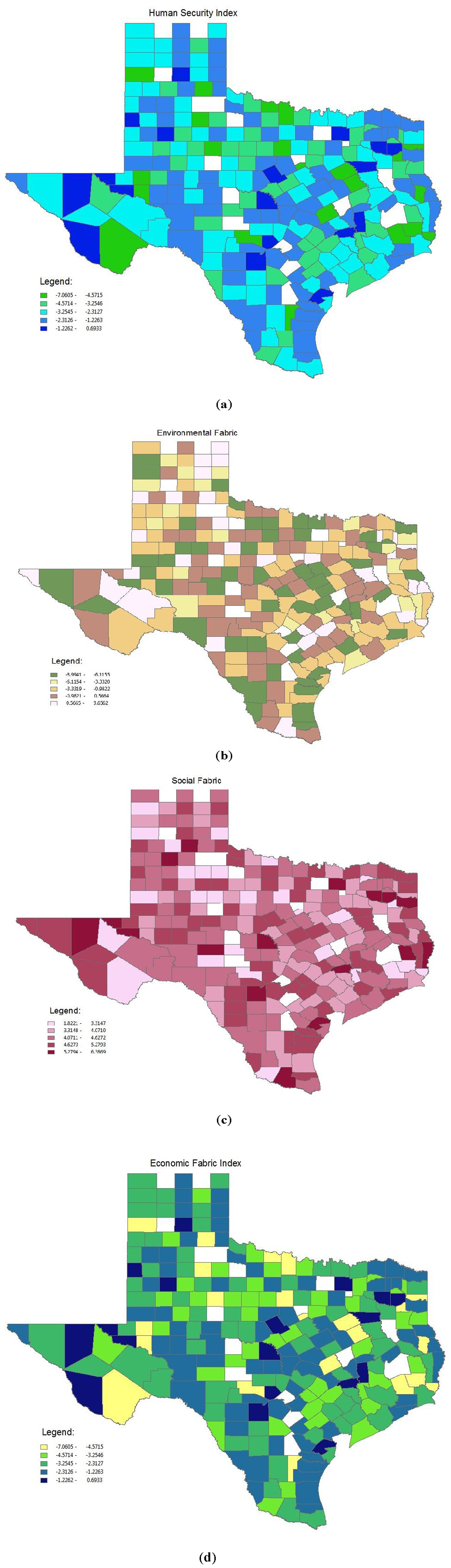
3.2. Identification of Regional or Geographic Trends

4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Zeigler-Johnson, C.M.; Tierney, A.; Rebbeck, T.R.; Rundle, A. Prostate cancer severity associations with neighborhood deprivation. Prostate Cancer 2011, 2011, 2–9. [Google Scholar]
- Cubbin, C.; Hadden, W.C.; Winkleby, M.A. Neighborhood context and cardiovascular disease risk factors: The contribution of material deprivation. Ethn. Dis. 2001, 11, 687–700. [Google Scholar]
- Knight, J.B.; Callahan, L.F.; Luong, M.L.N.; Shreffler, J.; Schoster, B.; Jordan, B.; Renner, J.B.; Jordan, J.M. The association of disability and pain with individual and community socioeconomic status in people with hip osteoarthritis. Open Rheumatol. J. 2011, 5, 51–58. [Google Scholar]
- Crimmins, E.M.; Kim, J.K.; Seeman, T.E. Poverty and biological risk: The earlier “aging” of the poor. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64A, 286–292. [Google Scholar]
- Sociodemographic Differences in Binge Drinking among Adults-14 States, 2004.; CDC: Atlanta, GA, USA, 2009.
- Ahern, M.; Brown, C.; Dukas, S. A national study of the association between food environments and county-level health outcomes. J. Rural Health 2011, 27, 367–379. [Google Scholar]
- Heslop, C.L.; Miller, G.E.; Hill, J.S. Neighbourhood socioeconomics status predicts non-cardiovascular mortality in cardiac patients with access to universal health care. PLoS One 2009, 4. [Google Scholar] [CrossRef]
- Most, M.T.; Sengupta, R.; Burgener, M.A. Spatial scale and population assignment choices in environmental justice analyses. Prof. Geogr. 2004, 56, 574–586. [Google Scholar]
- Hastings, D. The Human Security Index: Potential Roles for the Environmental and Earth Observation Communities. Fostering Earth Observation & Global Awareness; Earthzine. Available online: http://www.earthzine.org/2011/05/04/the-human-security-index-potential-roles-for-the-environmental-and-earth-observation-communities/ (accessed on 10 August 2011).
- STATA 12 SE. StataCorp: College Station, TX, USA, 2011.
- Skrondal, D.; Rabe-Hesketh, S. Interdisciplinary Statistics: Generalized Latent Variable Modeling: Multilevel, Longitudinal, and Structural Equation Models; Chapman & Hall/CRC: Baca Raton, FL, USA, 2004; p. 71. [Google Scholar]
- Joseph, D. Average Poverty Rate Is Twice as High for U.S. Counties Bordering Mexico as for Rest of U.S. 2010. Available online: http://cnsnews.com/news/article/average-poverty-rate-twice-high-us-counties-bordering-mexico-rest-us (accessed on 3 May 2012).
- Gray, L.C.; Moseley, W.G. A geographical perspective on poverty-environment interactions. Geogr. J. 2005, 171, 9–23. [Google Scholar]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social conditions as fundamental causes of health inequalities: Theory, evidence, and policy implication. J. Health Soc. Behav. 2010, 5, S28–S40. [Google Scholar]
- Christiaensen, L.; Demery, L.; Paternostro, S. Macro and micro perspectives of growth and poverty in Africa. World Bank Econ. Rev. 2003, 17, 317–347. [Google Scholar]
- Sexton, K.; Linder, S. The role of cumulative risk assessment in decisions about environmental justice. Int. J. Environ. Res. Public Health 2010, 7, 4037–4049. [Google Scholar]
- Wilson, W.J. The Truly Disadvantaged: The Inner City, the Underclass, and Public Policy; University of Chicago Press: Chicago, IL, USA, 1990. [Google Scholar]
- Massey, D.S. The dimensions of residential segregation. Soc. Forces 1988, 67, 281–315. [Google Scholar]
- Morland, K.; Wing, S.; Diez Roux, A.; Poole, C. Neighborhood characteristics associated with the location of food stores and food service places. Am. J. Prev. Med. 2002, 22, 23–29. [Google Scholar]
- Williams, D.R.; Collins, C. Racial residential segregation: A fundamental cause of racial disparities in health. Public Health Rep. 2001, 116, 404–416. [Google Scholar]
- Arias, E. United States life tables, 2007. Natl. Vital Stat. Rep. 2011, 59, 1–60. [Google Scholar]
- Eschbach, K.; Ostir, G.V.; Patel, K.V.; Markides, K.S.; Goodwin, J.S. Neighborhood context and mortality among older Mexican Americans: Is there a barrio advantage? Am. J. Public Health 2004, 94, 1807–1812. [Google Scholar]
- Massey, D.S. American apartheid: Segregation and the making of the underclass. Am. J. Soc. 1990, 96, 329–357. [Google Scholar]
- Massey, D.S.; Denton, N.A. Hypersegregation in U.S. metropolitan areas: Black and Hispanic segregation along five dimensions. Demography 1989, 26, 373–391. [Google Scholar]
- Lopez, R. Segregation and black/white differences in exposure to air toxics in 1990. Environ. Health Perspect. 2002, 110, 289–295. [Google Scholar]
- Collins, C.A.; Williams, D.R. Segregation and mortality: The deadly effects of racism? Soc. Forum 1999, 14, 495–523. [Google Scholar] [CrossRef]
- Jones-Webb, R.; Wall, M. Neighborhood racial/ethnic concentration, social disadvantage, and homicide risk: An ecological analysis of 10 U.S. cities. J. Urban Health 2008, 85, 662–676. [Google Scholar]
- Rosenthal, L.; Lobel, M. Explaining racial disparities in adverse birth outcomes: Unique sources of stress for black American women. Soc. Sci. Med. 2011, 72, 977–983. [Google Scholar]
- Patel, K.V.; Eschbach, K.; Rudkin, L.L.; Peek, M.K.; Markides, K.S. Neighborhood context and self-rated health in older Mexican Americans. Ann. Epidemiol. 2003, 13, 620–628. [Google Scholar]
- Sheffield, K.M.; Peek, M.K. Neighborhood context and cognitive decline in older Mexican Americans: Results from the Hispanic established populations for epidemiologic studies of the elderly. Am. J. Epidemiol. 2009, 169, 1092–1101. [Google Scholar]
- Eschbach, K.; Mahnken, J.D.; Goodwin, J.S. Neighborhood composition and incidence of cancer among Hispanics in the United States. Cancer 2005, 103, 1036–1044. [Google Scholar]
- Markides, K.S.; Eschbach, K. Aging, migration, and mortality: Current status of research on the Hispanic parado. J. Gerontol. B Psychol. Sci. Soc. Sci. 2005, 60, S68–S75. [Google Scholar]
- Park, Y.; Neckerman, K.; Quinn, J.; Weiss, C.; Jacobson, J.; Rundle, A. Neighbourhood immigrant acculturation and diet among Hispanic female residents of New York city. Public Health Nutr. 2011, 14, 1593–1600. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Kim, J.K.; Seeman, T.E. Poverty and biological risk: The earlier “Aging” of the Poor. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64A, 286–292. [Google Scholar]
- Cutter, S.L.; Holm, D.; Clark, L. The role of geographic scale in monitoring environmental justice. Risk Anal. 1996, 16, 517–526. [Google Scholar]
Appendix A
| Variable | Source | Component |
|---|---|---|
| Poverty | SAIPE 2009 | Economic Fabric Index |
| Unemployment | BLS LAU 2010 | |
| Median Household Income | Census 2008 | |
| Inequality (Gini Co-efficient) | Burkey, ncat.edu from 2000 Census household income | |
| % of Population on Food Stamps | ERS/USDA 2007 | |
| Particulate days > EPA Threshold | CDC-Environmental Protection Agency (EPA) Collaboration 2006 | Environmental Fabric Index |
| Ozone Days > EPA Threshold | CDC-Environmental Protection Agency (EPA) Collaboration 2006 | |
| CO2 Emissions | Vulcan Project 2002 | |
| Natural Amenity Scale | Modified from USDA ERS | |
| Natural Amenity Rank | Modified from USDA ERS | |
| Population Change 2000–2009 | Census 2010 | |
| Social Fabric Index | ||
| High School Graduate (incl. GED) | US Census 2010 | Education subcomponent |
| Average Freshman Graduate Rate | National Center for Education Statistics 2006–2007 | |
| % Population 25 yrs or Older High School Graduate (incl. GED) | US Census 2010 | |
| % Population > 25 yrs Some College Incl. Associate Degree | US Census 2010 | |
| % Population > 25 yrs with Bachelors degree | US Census 2010 | |
| %Adult Literacy (below BPLS) | National Center for Education Statistics, National Assessment of Adult Literacy 2003 | |
| % Not Proficient in English | US Census 2008 | |
| M&F Life Expectancy at Birth | HHS 2010 | Health subcomponent |
| Lesser of F or M LE change 1999–1983 | Ezzati et al. PLoS medicine | |
| YPLL Premature Death Rate | National Center for Health Statistics (NCHS) 2005–2007 | |
| % Adult Obesity | National Center for Chronic Disease Prevention and Health Promotion 2008 | |
| Motor Vehicle Mortality Rate | NCHS 2001–2007 | |
| Chlamydia Rate | Texas DSHS 2010 | |
| Adult uninsured | SAHIE 2007 | |
| Adult insured (<200% of poverty level) | SAHIE 2007 | Health subcomponent |
| % Zip codes with Healthy Food Access outlets | Census Zipcode business Patterns 2008 | |
| Violent Crimes | Uniform Crime Reporting, Federal Bureau of Investigation 2010 | Crime and punishment subcomponent |
| Property crimes per 10000 population | ||
| Incarceration | Census 2010 | |
| % Child Poverty | SAIPE 2009 | |
| Mentally Unhealthy Days | BRFSS 2003–2009 | Social Stress subcomponent |
| Teen Birth Rate | NCHS 2001–2007 | |
| Mortgage foreclosure Rate | ||
| Housing vacancy rate (excl. vacation/seasonal vacation rate) | US Census 2010 | |
| Inadequate Social Support (%) | BRFSS 2005–2009 | |
| Grandparent performing parental Role % | US Census 2010 | |
| Employed in creative class occupations | USDA ERS 2003 | |
| Creative share | USDA ERS 2003 | |
| Commute Index (% Drive Alone*Commute Time) | ACS 5 Year Estimates 2005–009 |
| Economic Fabric | Environmental Fabric | Social Fabric | Educational Subcomponent | Health Subcomponent | Crime Subcomponent | Social Stress Subcomponent | Total HSI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Highest | Lowest | Highest | Lowest | Highest | Lowest | Highest | Lowest | Highest | Lowest | Highest | Lowest | Highest | Lowest | Highest | Lowest | |
| Starr * | Williamson | Titus | Maverick * | Brooks * | Collin | Starr * | Marion | Wheeler | Presidio | Potter | Shackelford | Zapata * | Collin | Starr * | Carson | |
| Population Size | 60,968 | 422,679 | 32,334 | 54,258 | 7,223 | 782,341 | 60,968 | 10,546 | 5,410 | 7,818 | 121,073 | 3,378 | 14,018 | 782,341 | 60,968 | 6,182 |
| % Hispanic | 95.5% | 23.2% | 39.6% | 95.7% | 91.2% | 14.7% | 95.5% | 3.1% | 24.8% | 83.4% | 35.3% | 10.1% | 93.3% | 14.7% | 95.5% | 8.5% |
| %African American | 0.1% | 6.2% | 9.6% | 0.2% | 0.5% | 8.5% | 0.1% | 22.0% | 2.1% | 0.6% | 10.2% | 0.9% | 0.1% | 8.5% | 0.1% | 0.6% |
| Foreign Born | 30.0% | 10.3% | 19.3% | 34.2% | 4.4% | 17.2% | 30.0% | 2.3% | 7.4% | 28.1% | 13.2% | 2.9% | 26.1% | 17.2% | 30.0% | 2.0% |
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Salinas, J.J.; Shah, M.; Abdelbary, B.; Gay, J.L.; Sexton, K. Application of a Novel Method for Assessing Cumulative Risk Burden by County. Int. J. Environ. Res. Public Health 2012, 9, 1820-1835. https://doi.org/10.3390/ijerph9051820
Salinas JJ, Shah M, Abdelbary B, Gay JL, Sexton K. Application of a Novel Method for Assessing Cumulative Risk Burden by County. International Journal of Environmental Research and Public Health. 2012; 9(5):1820-1835. https://doi.org/10.3390/ijerph9051820
Chicago/Turabian StyleSalinas, Jennifer J., Manasi Shah, Bassent Abdelbary, Jennifer L. Gay, and Ken Sexton. 2012. "Application of a Novel Method for Assessing Cumulative Risk Burden by County" International Journal of Environmental Research and Public Health 9, no. 5: 1820-1835. https://doi.org/10.3390/ijerph9051820