
In Vitro Evaluation of Dentin Tubule Occlusion for Novel Calcium Lactate Phosphate (CLP) Paste


Abstract
:1. Introduction
2. Materials and Methods
2.1. Calcium Lactate Phosphate Desensitizing Paste Preparation
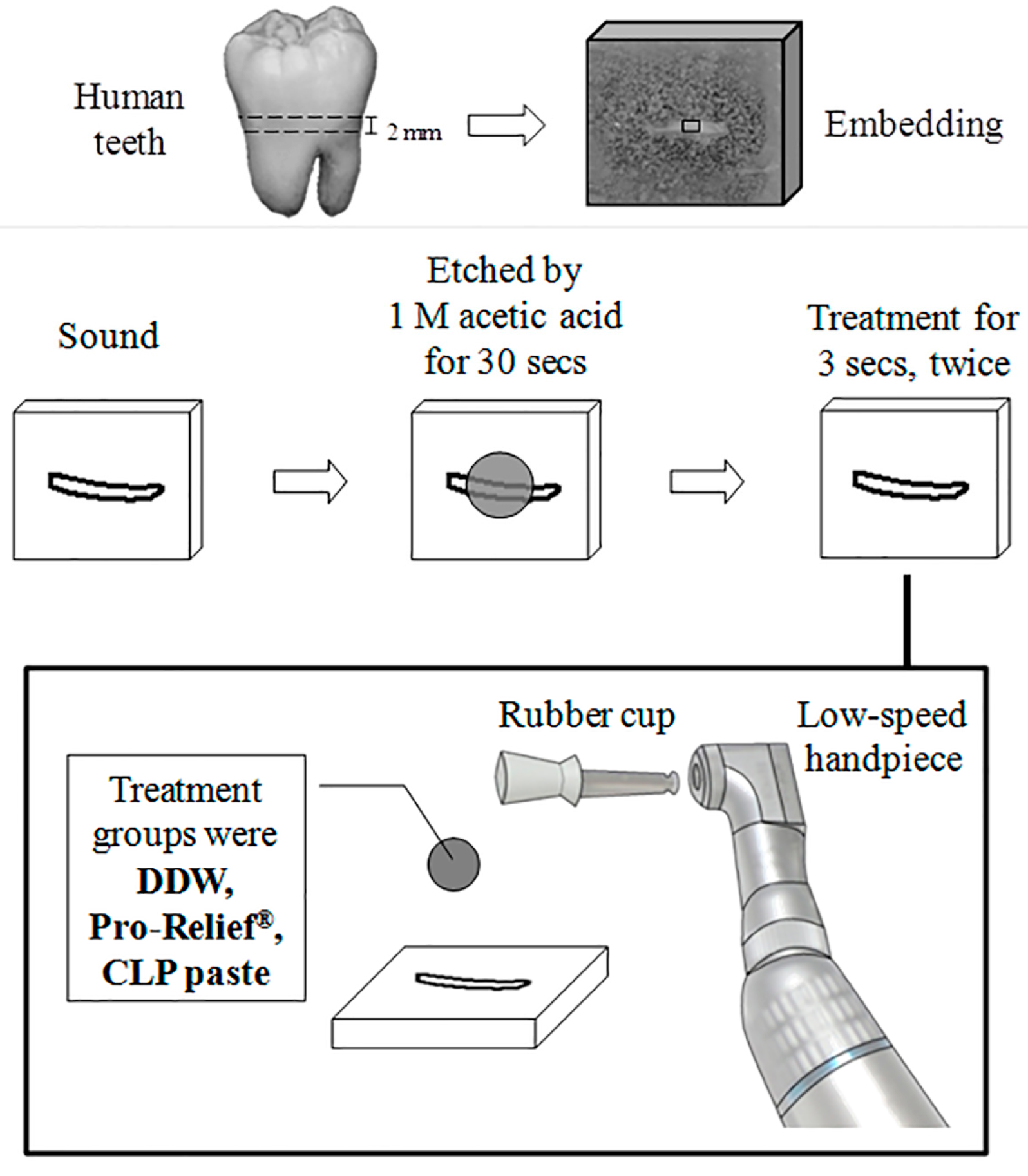
2.2. Pre-Etched Dentin Disk Preparation
2.3. Dentinal Tubule Occlusion Test
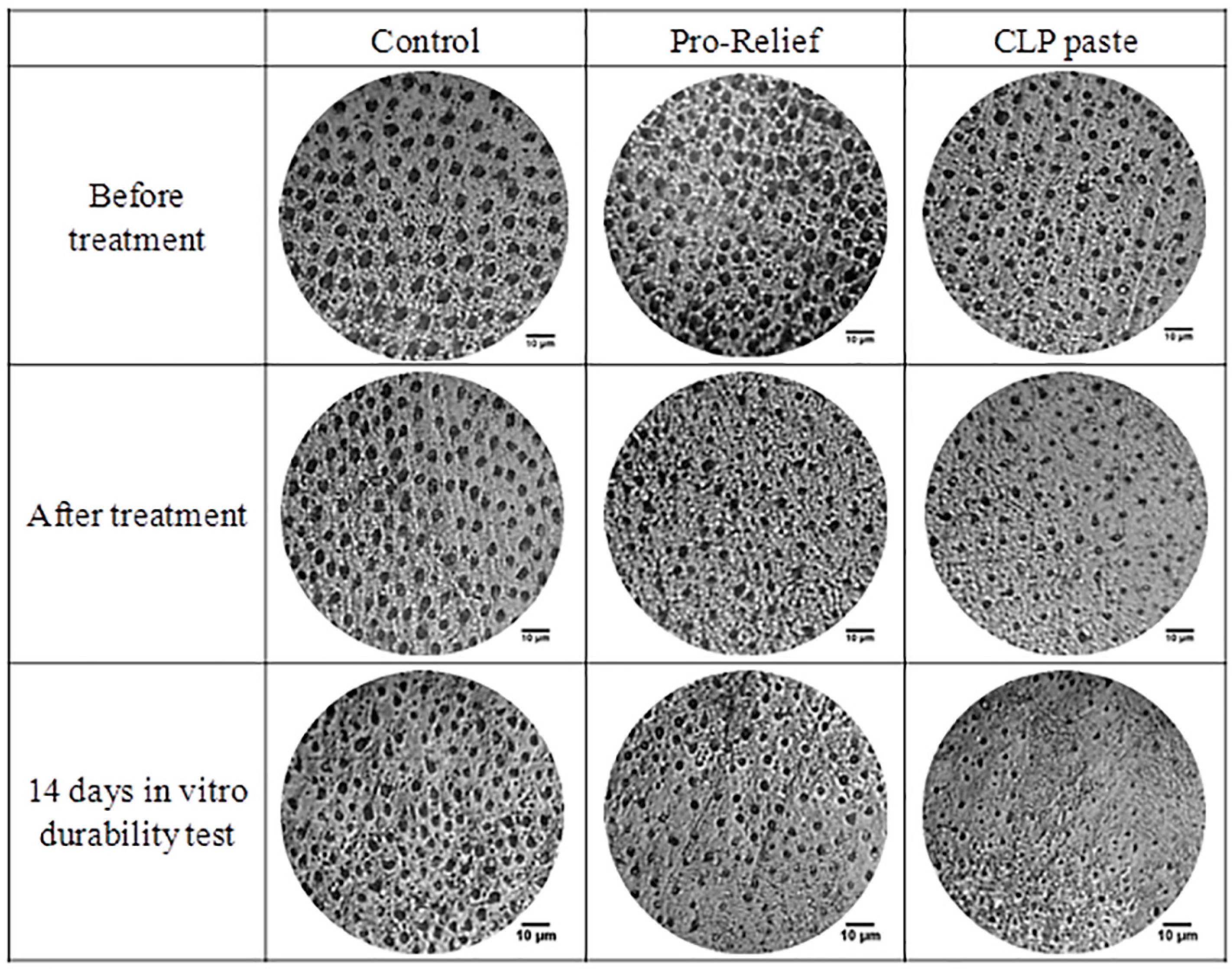
2.4. Optical Microscope Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kanapka, J.A. Current treatment for dentinal hypersensitivity. A new agent. Compend. Contin. Educ. Dent. 1982, S118–S120. [Google Scholar] [PubMed]
- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J. Can. Dent. Assoc. 2003, 69, 221–226. [Google Scholar] [PubMed]
- Pamir, T.; Ozyazici, M.; Baloglu, E.; Onal, B. The efficacy of three desensitizing agents in treatment of dentine hypersensitivity. J. Clin. Pharm. Ther. 2005, 30, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Parolia, A.; Kundabala, M.; Mohan, M. Management of dentinal hypersensitivity: A review. J. Calif. Dent. Assoc. 2011, 39, 167–179. [Google Scholar] [PubMed]
- McCormack, K.; Davies, R. The enigma of potassium ion in the management of dentine hypersensitivity: Is nitric oxide the elusive second messenger? Pain 1996, 68, 5–11. [Google Scholar] [CrossRef]
- Egbuniwe, O.; Grover, S.; Duggal, A.K.; Mavroudis, A.; Yazdi, M.; Renton, T.; Di Silvio, L.; Grant, A.D. TRPA1 and TRPV4 activation in human odontoblasts stimulates ATP release. J. Dent. Res. 2014, 93, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Lilja, J.; Nordenvall, K.J.; Branstrom, M. Dentin sensitivity, odontoblasts and nerves under desiccated or infected experimental cavities. A clinical, light microscopic and ultrastructural investigation. Swed. Dent. J. 1982, 6, 93–103. [Google Scholar] [PubMed]
- Seltzer, S. Pain Control in Dentistry: Diagnosis and Management; Lippincott: Philadelphia, PA, USA, 1978. [Google Scholar]
- Brannstrom, M. Dentin sensitivity and aspiration of odontoblasts. J. Am. Dent. Assoc. 1963, 66, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Bergenholtz, G.; Horsted-Bindslev, P.; Reit, C. Textbook of Endodontology, 2nd ed.; Chichester: West Sussex, UK; Wiley-Blackwell: Ames, IA, USA, 2010; p. 382. [Google Scholar]
- Scherman, A.; Jacobsen, P.L. Managing Dentin Hypersensitivity: What Treatment to Recommend to Patients. J. Am. Dent. Assoc. 1992, 123, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.C.; Lin, C.P.; Lan, W.H. Sealing depth of Nd:YAG laser on human dentinal tubules. J. Endod. 1997, 23, 691–693. [Google Scholar] [CrossRef]
- Kuo, T.C.; Lee, B.S.; Kang, S.H.; Lin, F.H.; Lin, C.P. Cytotoxicity of DP-bioglass paste used for treatment of dentin hypersensitivity. J. Endod. 2007, 33. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Chang, J.; Deng, Y.; Joiner, A. Tricalcium silicate induced mineralization for occlusion of dentinal tubules. Aust. Dent. J. 2011, 56, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Limeback, H. Comprehensive Preventive Dentistry; Wiley-Blackwell: Ames, IA, USA, 2012; p. 391. [Google Scholar]
- Cochrane, N.J.; Cai, F.; Huq, N.L.; Burrow, M.F.; Reynolds, E.C. New approaches to enhanced remineralization of tooth enamel. J. Dent. Res. 2010, 89, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Amaral, F.L.; Colucci, V.; Palma-Dibb, R.G.; Corona, S.A. Assessment of in vitro methods used to promote adhesive interface degradation: A critical review. J. Esthet. Restor. Dent. 2007, 19, 340–353. [Google Scholar] [CrossRef] [PubMed]
- Bird, R.B.; Stewart, W.E.; Lightfoot, E.N. Transport Phenomena, 2nd ed.; J. Wiley: New York, NY, USA, 2002; p. 895. [Google Scholar]
- Miglani, S.; Aggarwal, V.; Ahuja, B. Dentin hypersensitivity: Recent trends in management. J. Conserv. Dent. 2010, 13, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Landry, R.G.; Voyer, R. Treatment of dentin hypersensitivity: A retrospective and comparative study of two therapeutic approaches. J. Can. Dent. Assoc. 1990, 56, 1035–1041. [Google Scholar] [PubMed]
- Grossman, L.E. The treatment of hypersensitive dentine. J. Am. Dent. Assoc. 1935, 22, 592–602. [Google Scholar]
- Chiang, Y.C.; Chen, H.J.; Liu, H.C.; Kang, S.H.; Lee, B.S.; Lin, F.H.; Lin, H.P.; Lin, C.P. A novel mesoporous biomaterial for treating dentin hypersensitivity. J. Dent. Res. 2010, 89, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Naveena, P.; Nagarathana, C.; Sakunthala, B.K. Remineralizing Agent—Then and Now—An Update. Dentistry 2014, 4. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, E.J.; Kim, D.S.; Lee, I.B. The evaluation of dentinal tubule occlusion by desensitizing agents: A real-time measurement of dentinal fluid flow rate and scanning electron microscopy. Oper. Dent. 2013, 38, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Tung, M.S.; Eichmiller, F.C. Dental applications of amorphous calcium phosphates. J. Clin. Dent. 1999, 10, 1–6. [Google Scholar] [PubMed]
- Wolff, M.S. Dentin hypersensitivity, the biofilm, and remineralization: What is the connection? Adv. Dent. Res. 2009, 21, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Pei, D.; Chen, Z.; Lei, J.; Zhou, L.; Huang, C. Effects of the application sequence of calcium-containing desensitising pastes during etch-and-rinse adhesive restoration. J. Dent. 2014, 42, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Shivaprasad, B.M.; Padmavati, P.; Sanghani, N.N. Chair Side Application of NovaMin for the Treatment of Dentinal Hypersensitivity—A Novel Technique. J. Clin. Diagn. Res. 2014, 8. [Google Scholar] [CrossRef]
- Madhavan, S.; Nayak, M.; Shenoy, A.; Shetty, R.; Prasad, K. Dentinal hypersensitivity: A comparative clinical evaluation of CPP-ACP F, sodium fluoride, propolis, and placebo. J. Conserv. Dent. 2012, 15, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.W.; Wolff, M.S.; Winston, A.E.; Triol, C.W. Clinical evaluation of the effect of a remineralizing toothpaste on dentinal sensitivity. J. Clin. Dent. 1999, 10, 50–54. [Google Scholar] [PubMed]
- Pepelassi, E.; Rahiotis, C.; Peponi, E.; Kakaboura, A.; Vrotsos, I. Effectiveness of an in-office arginine-calcium carbonate paste on dentine hypersensitivity in periodontitis patients: A double-blind, randomized controlled trial. J. Clin. Periodontol. 2015, 42, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Tegethoff, F.W.; Rohleder, J.; Kroker, E. Calcium Carbonate: From the Cretaceous Period into the 21st Century; Birkhauser Verlag: Boston, MA, USA, 2001; p. 342. [Google Scholar]



{kind=link}
{kind=link}
| Groups | The Diameter of Dentinal Tubule (μm) | ||
|---|---|---|---|
| ddH2O | Pro-Relief Paste | CLP Paste | |
| Before treatment | 4.00 ± 0.64 a | 3.85 ± 0.49 a | 3.52 ± 0.83 a |
| After treatment | 3.13 ± 0.45 b | 3.33 ± 0.72 a,b | 2.62 ± 0.42 c |
| In vitro 14 days aging test | 3.43 ± 0.87 a,b | 3.02 ± 0.56 b | 1.71 ± 0.45 d |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.-C.; Hu, H.-T.; Lee, S.-Y.; Hsieh, S.-C.; Huang, P.-C.; Ma, C.-F.; Ji, D.-Y.; Chang, L.-Y.; Teng, N.-C. In Vitro Evaluation of Dentin Tubule Occlusion for Novel Calcium Lactate Phosphate (CLP) Paste. Materials 2017, 10, 228. https://doi.org/10.3390/ma10030228
Yang J-C, Hu H-T, Lee S-Y, Hsieh S-C, Huang P-C, Ma C-F, Ji D-Y, Chang L-Y, Teng N-C. In Vitro Evaluation of Dentin Tubule Occlusion for Novel Calcium Lactate Phosphate (CLP) Paste. Materials. 2017; 10(3):228. https://doi.org/10.3390/ma10030228
Chicago/Turabian StyleYang, Jen-Chang, Hsin-Tai Hu, Sheng-Yang Lee, Sung-Chih Hsieh, Pei-Chi Huang, Chen-Feng Ma, Dian-Yu Ji, Liang-Yu Chang, and Nai-Chia Teng. 2017. "In Vitro Evaluation of Dentin Tubule Occlusion for Novel Calcium Lactate Phosphate (CLP) Paste" Materials 10, no. 3: 228. https://doi.org/10.3390/ma10030228