Administration of Fozivudine Tidoxil as a Single-Agent Therapeutic during Acute Feline Immunodeficiency Virus Infection Does Not Alter Chronic Infection


Abstract
:1. Introduction
2. Results and Discussion
2.1. Plasma and Cell Associated Viremia

{kind=link}
{kind=link}
| FIV-gag-mRNA | ||||
|---|---|---|---|---|
| [copies/mL plasma] | [copies/106 PBMCs] | |||
| Years Post infection | 1 | 2 | 3 | 3 |
| FZD | ||||
| Positive (%) | 100 | 100 | 100 | 40 |
| (5/5) | (5/5) | (5/5) | (2/5) | |
| Mean | 2.91 | 4.84 | 2.74 | 1.44 |
| Median | 2.80 | 4.26 | 2.77 | 1.44 |
| Range | 2.27–3.67 | 3.87–6.76 | 2.04–3.85 | 1.41–1.46 |
| Placebo | ||||
| Positive (%) | 100 | 100 | 100 | 60 |
| (5/5) | (5/5) | (5/5) | (3/5) | |
| Mean | 3.40 | 4.81 | 2.59 | 1.39 |
| Median | 3.32 | 4.27 | 2.33 | 1.46 |
| Range | 2.96–3.98 | 3.89–6.81 | 1.93–3.97 | 1.16–1.54 |
| p-value | NS | NS | NS | NS |
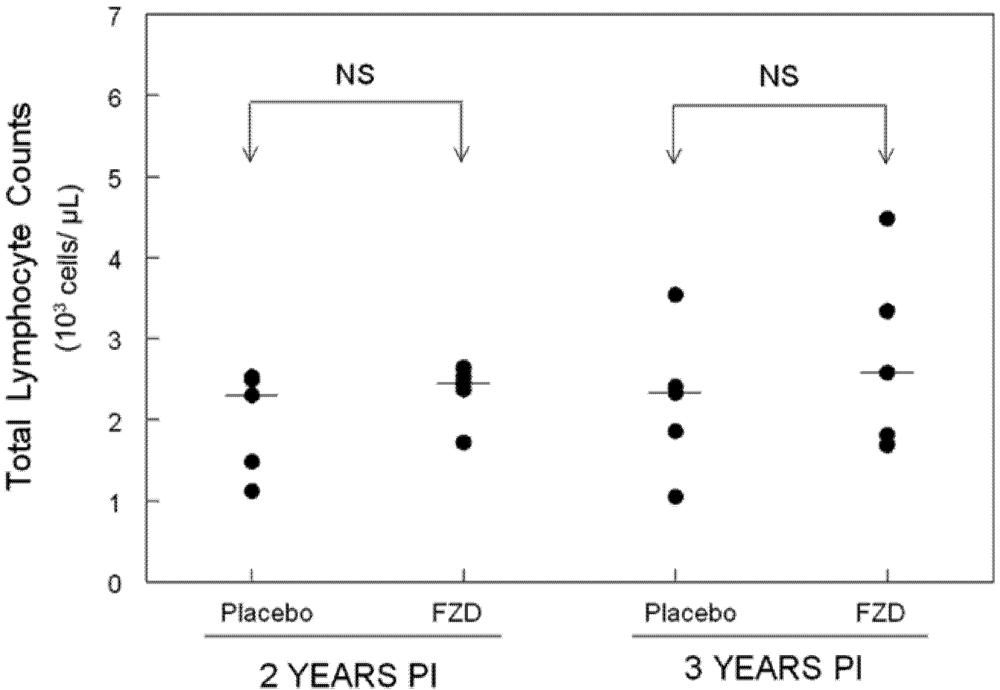
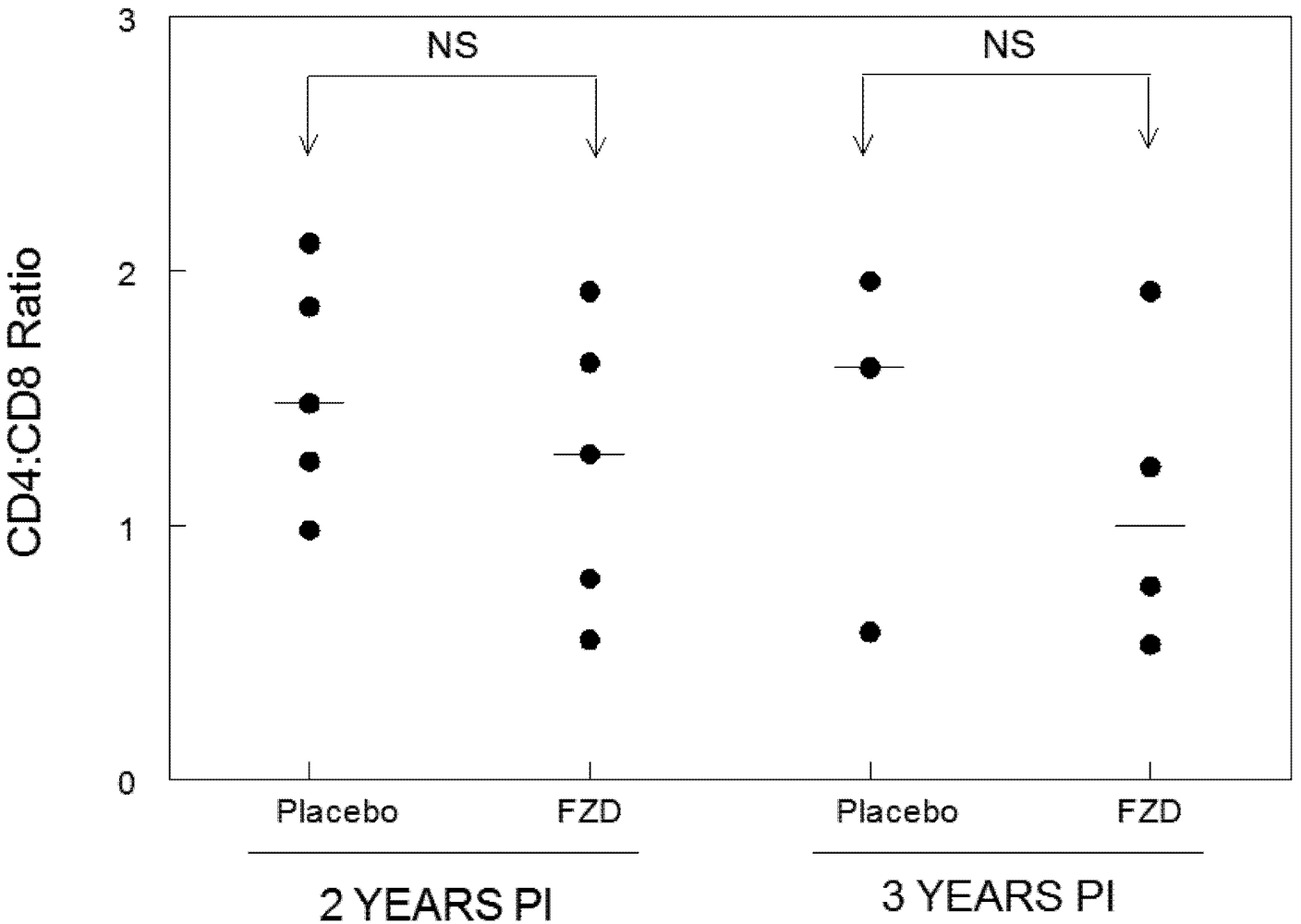
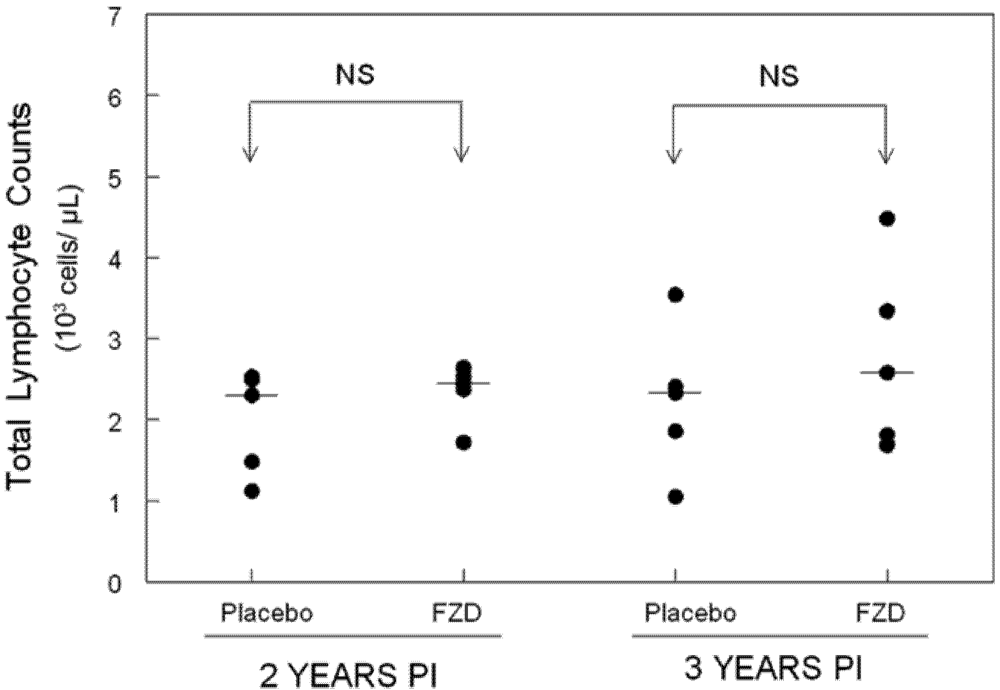
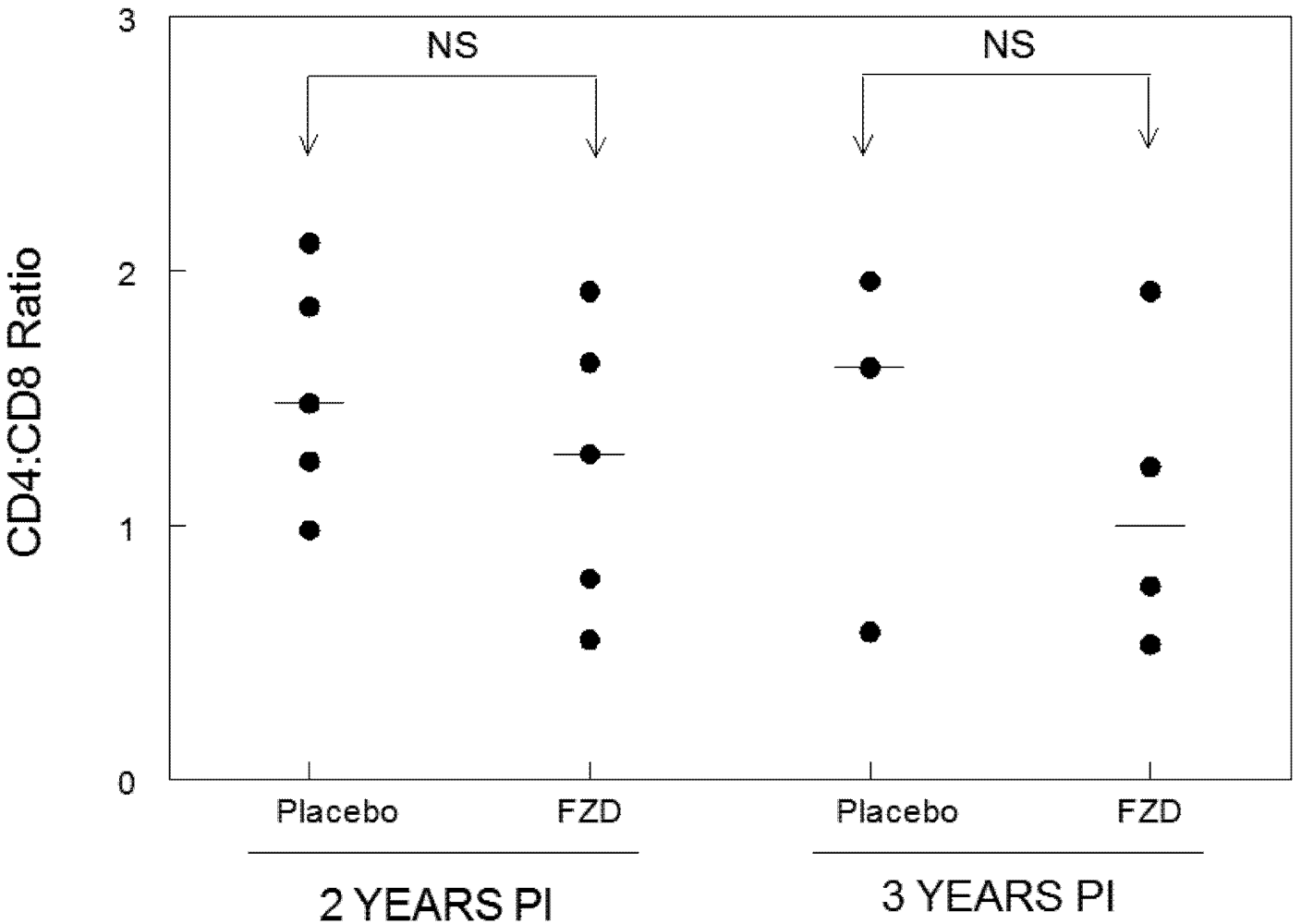
2.2. Lymphocyte Enumeration and Composition
2.3. Clinical Findings
3. Experimental Section
3.1. Cats
3.2. Fozivudine Tidoxil
3.3. Infection with FIV
3.4. Sample Collection
3.5. Lymphocyte Subset Analysis
3.6. Plasma and Cell-Associated Viremia
3.7. Statistical Analysis
4. Conclusions
Acknowledgments
Conflict of Interest
References and Notes
- Schmid, A.; Gianella, S.; Wyl, V.; Metzner, K.; Scherrer, A.; Niederost, B.; Althaus, C.; Rieder, P.; Grube, C.; Joos, B.; et al. Profound depletion of HIV-1 transcription in patients initiating antiretroviral therapy during acute infection. PLoS One 2010, 5, e13310. [Google Scholar]
- Streeck, H.; Jessen, H.; Alter, G.; Teigen, N.; Waring, M.; Jessen, A.; Stahmer, I.; Lunzen, J.; Lichterfeld, M.; Gao, X.; et al. Immunological and virological impact of highly active antiretroviral therapy initiated during acute HIV-1 infection. J. Infect. Dis. 2006, 194, 734–739. [Google Scholar] [CrossRef]
- Malhotra, U.; Berrey, M.; Huang, Y.; Markee, J.; Brown, D.; Ap, S.; Musey, L.; Schacker, T.; Corey, L.; McElrath, M. Effect of combination antiretroviral therapy on T-cell immunity in acute human immunodeficiency virus type 1 infection. J. Infect. Dis. 2000, 181, 121–131. [Google Scholar]
- Rosenberg, E.; Altfeld, M.; Poon, S.; Phillips, M.; Wilkes, B.; Eldridge, R.; Robbins, G.; D'Aquila, R.; Goulder, P.; Walker, B. Immune control of HIV-1 after early treatment of acute infection. Nature 2000, 407, 523–526. [Google Scholar]
- Mellors, J.; Rinaldo, C.; Gupta, P.; White, R.; Todd, J.; Kingsley, L. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 1996, 272, 1167–1170. [Google Scholar]
- Mellors, J.; Muñoz, A.; Giorgi, J.; Margolick, J.; Tassoni, C.; Gupta, P.; Kingsley, L.; Todd, J.; Saah, A.; Detels, R.; et al. Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann. Intern. Med. 1997, 126, 946–954. [Google Scholar]
- Schacker, T.; Hughes, J.; Shea, T.; Coombs, R.; Corey, L. Biological and virologic characteristics of primary HIV infection. Ann. Intern. Med. 1998, 128, 613–620. [Google Scholar]
- Hare, C.; Pappalardo, B.; Busch, M.; Karlsson, A.; Phelps, B.; Alexander, S.; Bentsen, C.; Ramstead, C.; Nixon, D.; Levy, J.; et al. Seroreversion in subjects receiving antiretroviral therapy during acute/early HIV infection. Clin. Infect. Dis. 2006, 42, 700–708. [Google Scholar] [CrossRef]
- Fogle, J.; Tompkins, W.; Campbell, B.; Sumner, D.; Tompkins, M. Fozivudine tidoxil as single-agent therapy decreases plasma and cell-associated viremia during acute feline immunodeficiency virus infection. J. Vet. Intern. Med. 2011, 25, 413–418. [Google Scholar]
- Furman, P.; Fyfe, J.; St. Clair, M.; Weinhold, K.; Rideout, J.; Freeman, G.; Lehrman, S.; Bolognesi, D.; Broder, S.; Mitsuya, H. Phosphorylation of 3’-azido-3’-deoxythymidine and selective interaction of the 5’-triphosphate with human immunodeficiency virus reverse transcriptase. Proc. Natl. Acad. Sci. U. S. A. 1986, 83, 8333–8337. [Google Scholar]
- Girard, P.; Pegram, P.; Diquet, B.; Anderson, R.; Raffi, F.; Tubiana, R.; Sereni, D.; Boerner, D. Phase II placebo-controlled trial of fozivudine tidoxil for HIV infection: Pharmacokinetics, tolerability and efficacy. J. Acquir. Immune. Defic. Syndr. 2000, 23, 227–235. [Google Scholar]
- Kucera, G.; Goff, C.; Iyer, N.; Morris-Natschke, S.; Ishaq, K.; Wyrick, S.; Fleming, R.; Kucera, L. Cellular metabolism in lymphocytes of a novel thioether-phospholipid-AZT conjugate with anti-HIV activity. Antivir. Res. 2001, 50, 129–137. [Google Scholar]
- Arai, M.; Earl, D.; Yamamoto, J. Is AZT/3TC therapy effective against FIV infection or immunopathogenesis? Vet. Immunol. Immunopathol. 2002, 85, 189–204. [Google Scholar] [CrossRef]
- Hayes, K.; Lafrado, L.; Erickson, J.; Marr, J.; Mathes, L. Prophylactic ZDV therapy prevents early viremia and lymphocyte decline but not primary infection in feline immunodeficiency virus-inoculated cats. J. Acquir. Immune. Defic. Syndr. 1993, 6, 127–134. [Google Scholar]
- Hayes, K.; Phipps, A.; Francke, S.; Mathes, L. Antiviral therapy reduces viral burden but does not prevent thymic involution in young cats infected with feline immunodeficiency virus. Antimicrob. Agents Chemother. 2000, 44, 2399–2405. [Google Scholar]
- Hayes, K.; Wilkinson, J.; Frick, R.; Francke, S.; Mathes, L. Early suppression of viremia by ZDV does not alter the spread of feline immunodeficiency virus infection in cats. J. Acquir. Immune. Defic. Syndr. 1995, 9, 114–122. [Google Scholar]
- English, R.; Nelson, P.; Johnson, C.; Nasisse, M.; Tompkins, W.; Tompkins, M. Development of clinical disease in cats experimentally infected with feline immunodeficiency virus. J. Infec. Dis. 1994, 170, 543–552. [Google Scholar]
- Davidson, M.; Rottman, J.; English, R.; Lappin, M.; Tompkins, M. Feline immunodeficiency virus predisposes cats to acute generalized toxoplasmosis. Am. J. Pathol. 1993, 143, 1486–1497. [Google Scholar]
- Tompkins, M.; Gebhard, D.; Bingham, H.; Hamilton, M.; Davis, W.; Tompkins, W. Characterization of monoclonal antibodies to feline T lymphocytes and their use in the analysis of lymphocyte tissue distribution in the cat. Vet. Immunol. Immunopathol. 1990, 26, 305–317. [Google Scholar]
- Mexas, A.; Fogle, J.; Tompkins, W.; Tompkins, M. CD4+CD25+ regulatory T cells are infected and activated during acute FIV infection. Vet. Immunol. Immunopathol. 2008, 126, 263–272. [Google Scholar]
- Fogle, J.; Mexas, A.; Tompkins, W.; Tompkins, M. CD4(+)CD25(+) T regulatory cells inhibit CD8(+) IFN-gamma production during acute and chronic FIV infection utilizing a membrane TGF-beta-dependent mechanism. AIDS Res. Hum. Retroviruses 2010, 26, 201–216. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Miller, M.M.; Fogle, J.E. Administration of Fozivudine Tidoxil as a Single-Agent Therapeutic during Acute Feline Immunodeficiency Virus Infection Does Not Alter Chronic Infection. Viruses 2012, 4, 954-962. https://doi.org/10.3390/v4060954
Miller MM, Fogle JE. Administration of Fozivudine Tidoxil as a Single-Agent Therapeutic during Acute Feline Immunodeficiency Virus Infection Does Not Alter Chronic Infection. Viruses. 2012; 4(6):954-962. https://doi.org/10.3390/v4060954
Chicago/Turabian StyleMiller, Michelle M., and Jonathan E. Fogle. 2012. "Administration of Fozivudine Tidoxil as a Single-Agent Therapeutic during Acute Feline Immunodeficiency Virus Infection Does Not Alter Chronic Infection" Viruses 4, no. 6: 954-962. https://doi.org/10.3390/v4060954