Traditional Practice vs. New Tools and Routines in Stroke Treatment

University Hospital of North Norway, Norwegian Centre for Integrated Care and Telemedicine, Tromsø 35, 9038, Norway
*
Author to whom correspondence should be addressed.
Future Internet 2012, 4(3), 688-699; https://doi.org/10.3390/fi4030688
Submission received: 19 April 2012
/
Revised: 23 July 2012
/
Accepted: 25 July 2012
/
Published: 6 August 2012
(This article belongs to the Special Issue Future e-Health)
{kind=link}
{kind=link}
{kind=link}
Abstract
:In Norway, it is a national goal to provide more patients with thrombolytic treatment. A referring hospital and a specialist hospital have implemented videoconferencing (VC) equipment to share knowledge and discuss stroke patients, regarding thrombolytic treatment. VC has only been used four times within the 19 months that the service has been available. The objective in this article is to increase the understanding of the contradiction between the need for knowledge-sharing through VC technology, as well as the reasons for low frequency of use when discussing stroke patients. Semi-structured interviews were conducted with 13 professionals. The results illustrate how the technology per se is not the reason for the low frequency use. Health care is shaped by behavior, traditional rules, standards and division of labor. By using cultural historical activity theory (CHAT) as a framework, we illustrate the importance of understanding the historic way of performing an activity to be able to expand the treatment activity in the future.
1. Introduction
In Norway, 12,000 people suffer from stroke each year [1]. By giving stroke patients thrombolytic treatment in the acute phase, their prognoses are improved [2]. It is a national goal to provide more patients with thrombolytic treatment [2]. Thrombolytic treatment should be given as soon as possible, but within 4½ hours after the onset of symptoms [2]. As time matters, decisions about diagnosis must be made as soon as possible after the patient with a suspected stroke reaches the emergency unit at the referring hospital. The decision about starting thrombolytic treatment depends on several criteria, where are considered individually case-by-case. If the decision is to start thrombolytic treatment, it will be initiated and given under strict supervision from a specialist in neurology. Small hospitals do not have such competence, and in situations where a second opinion is necessary or thrombolytic treatment is given, practitioners need advice regarding treatment. Traditionally, such advice is sought over the telephone.
This study takes place in Norway, where a hospital has implemented real-time videoconferencing (VC) to access specialist knowledge from a specialist hospital to discuss acute patients suffering a potential stroke. By using VC, the physicians, nurses and specialists are able to examine the patient in a collaborative process, which may be helpful when deciding if a patient needs advanced specialist neurological or neurosurgical emergency treatment. The knowledge is then shared and constructed between the specialists at the specialist hospital and the physicians at the referring hospital. In acute situations, when the time is limited, this collaborative process can shorten decision time and improve the outcome of treatment. Stroke is a condition with paralysis and confusion, and therefore a domain that particularly benefits from seeing the patient, instead of only hearing descriptions of the patient’s condition. Although the decision to give thrombolytic treatment is comprehended as the end-point of the acute stroke consultation, it is just the beginning of care for the patient [3]. VC consultation may therefore also be useful in follow-up after the acute phase of a stroke patient. Post-thrombolytic care requires intensive cardiovascular and neurological monitoring, neurosurgical backup, and a decision whether to keep the patient or to “drip-and-ship”. The VC process provides an opportunity to both see and hear the patient and the practitioners at the same time. This is an improvement compared to using an ordinary telephone, which provides only sound and one-to-one communication, i.e., between the specialist and the physician. In this manner, the use of VC supports knowledge-sharing in teams between professionals, both in acute and post-thrombolytic care.
There is limited experience with use of VC in stroke treatment in Norway. Many hospitals use tele-radiology image transfer combined with telephone advice to support referring hospitals for stroke patients [2,4]. A VC stroke service established between Haukeland University Hospital and referring hospitals in Voss and in Førde reports an increase in thrombolytic treatment [5]. However, there is substantial scientific evidence of the medical impacts of the use of VC in stroke treatment; “telestroke” [3]. A meta-analysis shows that a telestroke network, where experienced stroke specialists perform an evaluation and examination of the patient via VC, and consider the indication for initiation of thrombolytic treatment, is comparable with face-to-face consultations [6]. There is also evidence that VC counseling is more effective than telephone counseling in the acute treatment of stroke. Several studies of telestroke solutions including video versus solutions without video show that VC may (1) reduce the number of wrong diagnoses (7.1% vs. 17.6%, p < 0.05), (2) reduce death rate (1.3% vs. 6.8%, p < 0.05) (3) reduce needs for nursing homes (2.6% vs. 5.4%, p = 0.58) [7,8,9].
In this article, we consider knowledge as a phenomenon embedded in the community, rather than just in one individual. No-one has enough knowledge to manage all the problems on their own [10]. Different specialized people must come together in order to establish the desired outcome. Medical problem-solving is thus a social process, establishing a shared understanding of treatment. Knowledge is here situated within and between activity systems: the activity system of the specialist at the specialist hospital and the activity system of the professionals at the referring hospital. VC technology is a tool that supports this kind of knowledge-sharing, including a second opinion for discussing stroke treatment. We use cultural historical activity theory (CHAT) as a lens to understand the introduction of VC equipment for knowledge-sharing. Our research focus for this part of the study is to increase the understanding of the contradiction between the need for knowledge-sharing and the reasons for the low frequency of the use of VC for discussing stroke patients.
Material and Framework
When the patient arrives at the referring hospital, the physician on duty meets the patient in the emergency room. Here, the physician considers the patient condition supported by the nurses. If the patient has symptoms of stroke, he/she has to be considered for thrombolytic treatment. If the physician wants to discuss the patient with a specialist, or if the physician wants to give thrombolytic treatment, the physician calls up the specialist at a specialist hospital by telephone.
In September 2010, the VC service was ready to be used between the two hospitals in Norway included in our study, so that an image of the patient could supplement the spoken description communicated by telephone. In this way, the physicians and nurses at the smaller referring hospital could communicate with the specialist in the specialist hospital, seeing each other and the patient. When the physician calls up the specialist by telephone, he/she initiates the VC meeting, instead of only telephone consultation. While the patient has the CT taken, the specialist and the emergency team (nurses and/or other physicians) connect via VC. After the patient has been CT scanned, he/she returns to the emergency room, where the local team and the specialist through VC are waiting to start the discussion. In September 2010 the service was used for the first time, and it is still running.
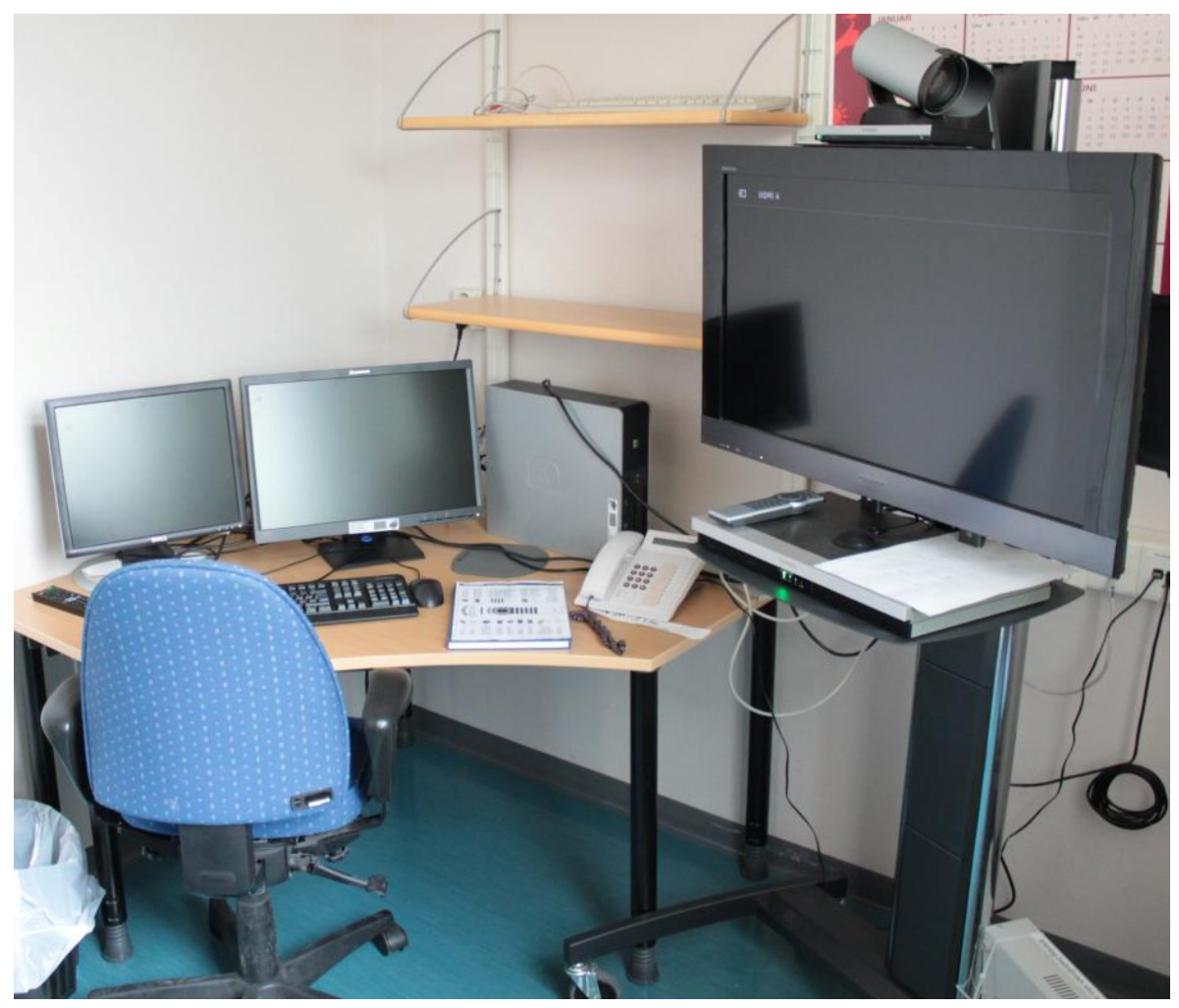
Each hospital is equipped with the same type of equipment, which reduces possible sources of error. Only minor local adjustments were made due to room configuration. The VC equipment consists of a Tandberg Quick set C60 and a Sony full HD (1080p) television, mounted on a mobile rack (Figure 1).
Figure 1.
The VC equipment in the emergency room.

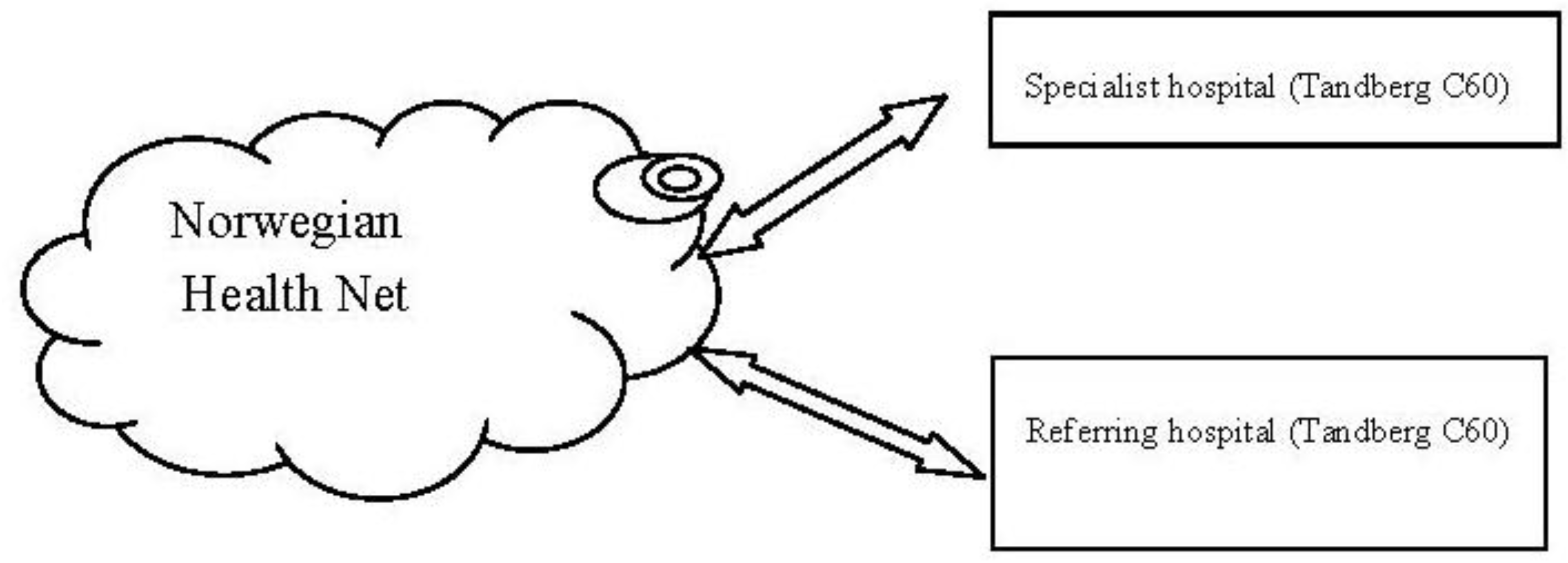
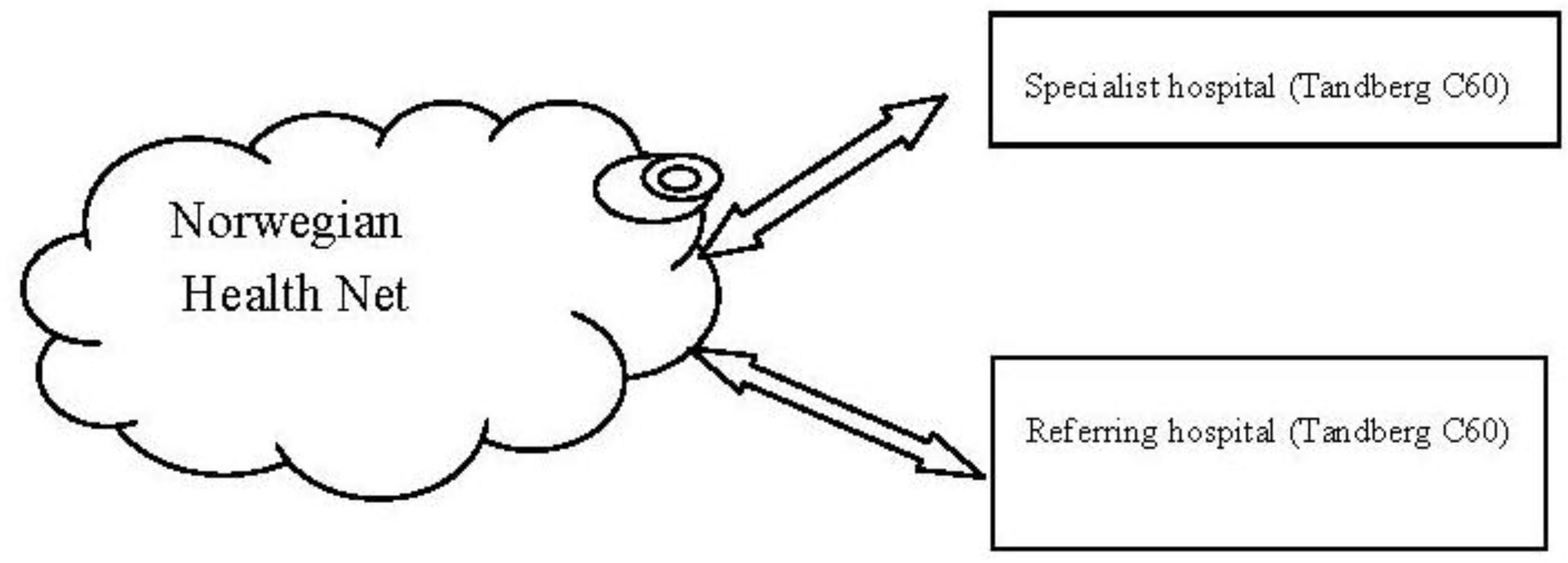
The Tandberg Quick set C60 has the capability to connect different medical equipment, such as electrocardiography (ECG) apparatus and ultrasound equipment together with two full HD (1080p) cameras. The system may also be used for multipart conferences between more than two locations. It is connected through the Norwegian Health Net [11] (Figure 2), which is a dedicated, secure network for health information. The VC is located in the emergency room at the referring hospital.
Figure 2.
The VC service.
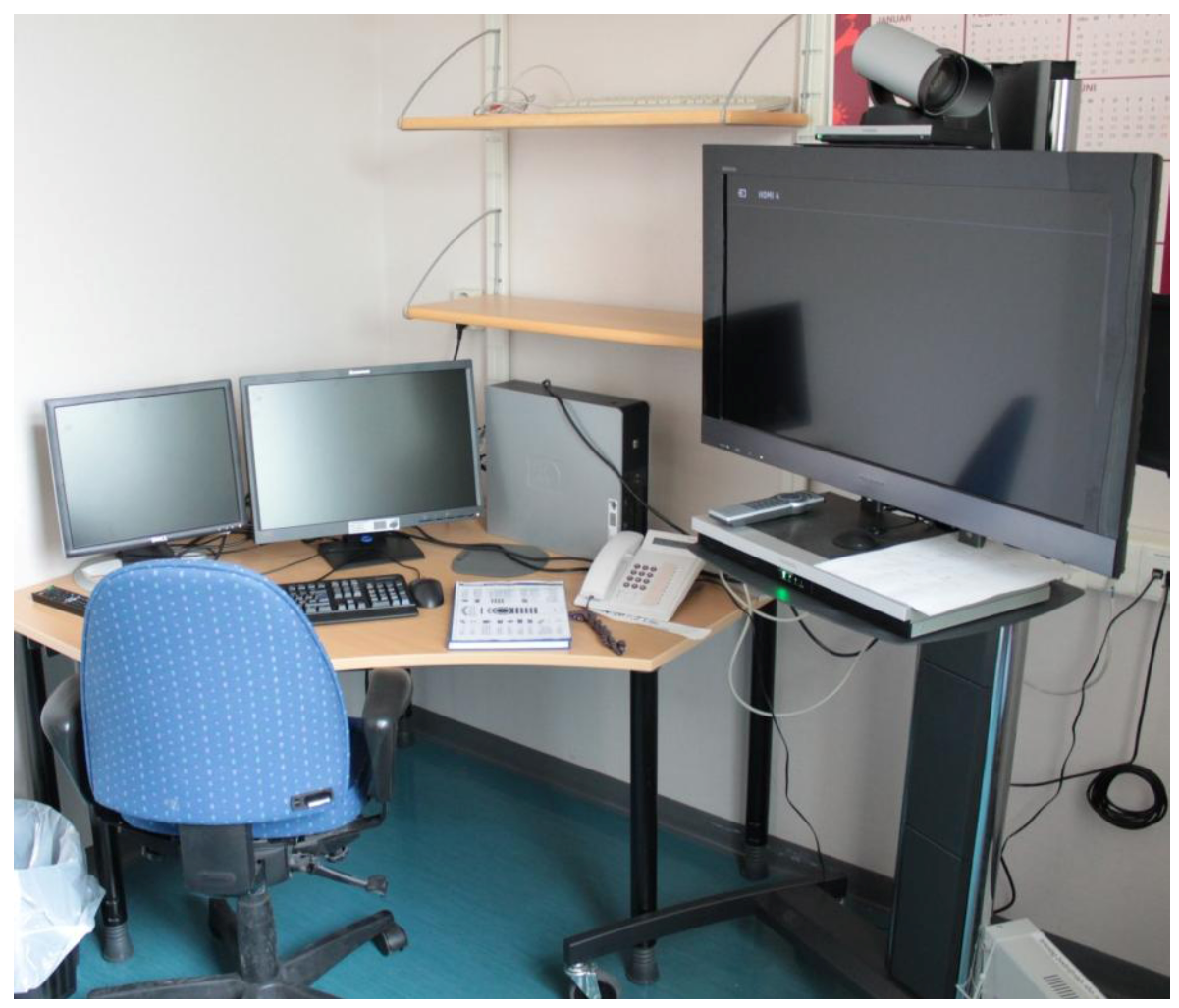
In the specialist hospital, the VC equipment is located in a dedicated room, used only for this purpose (Figure 3). When the referring hospital calls up the specialist hospital by telephone and initiates a VC meeting, the specialist immediately moves to this room.
Figure 3.
The VC equipment in the dedicated room.
We consider the empirical field as a network of interacting activity systems, in which the practitioners in the referring hospital and the specialist hospital collaborate, giving the best treatment for stroke patients. Thus, we have a CHAT theoretical framework [12] to understand the activity across work settings. We will argue that objects are culturally and historically developed over time and that activities must be analyzed in relation to practical activities in a wide cultural, social and physical context [13]. Collaborating by using VC requires a patient as an object to discuss. The actions of the subject, the practitioners, are directed toward an object, mediated by both artefacts (tools) and the humans sharing the same object, referred to as the community [12]. VC is the tool providing visual access between the local team and the specialist hospital to share knowledge to improve general stroke treatment and support of thrombolytic treatment. The subject is related to the community by rules, and the relationship between the community and the object is mediated through the division of labor. The activity is oriented toward an outcome, which is the goal and the motivation for the activity [14].
The two hospitals, the referring and the specialist hospital, form two activity systems that interact with regard to the shared object, i.e., the stroke patient. Analyzing collaborative practice has to take place in the zone between the activity systems. The zone between the two activity systems is the boundary zone [15]. Here, routines and patterns must be constructed as something new, representing the participants’ own structures, behaviors, rules and standards. Since elements from several activities collaborate in the boundary zone, the zone is regarded as a place where understanding is negotiated [16], and the object can expand.
If collaborative practice does not work, activities cannot be analyzed in the boundary zone. Explanations for breakdowns in the activity have to be analyzed in the separate activity system. Here, we search for explanations why the object does not expand in a collaborative activity, which is the motive for introducing VC equipment as a tool. The framework of CHAT is used to analyze the activity system of the referring hospital, since the staff there initiate the VC meeting. Therefore, this article explores the empirical field of the referring hospital, with an emphasis on comments from professionals initiating the need for knowledge. Analyzing the specialist activity system and elaboration on them both is interesting for further work.
2. Methods
This is a qualitative study [17], emphasizing the need for knowledge-sharing in stroke treatment and the use of VC for this purpose. We have followed the use of the equipment since it was introduced to the clinics in September 2010. All activity using VC is automatically logged by the Norwegian Health Net VC service. As a consequence, we knew how many times, when, by whom and for how long the VC equipment had been used. This data was then used as a basis for the interviews. As the results will show, the VC equipments logs exhibited a low-frequency of use. This shaped our study, by increasing our willingness to study discontinuities in action as breakdowns in activity, and became our point of reference for studying knowledge-sharing as an empirical phenomenon.
Autumn 2011 interviews with 13 professionals were conducted through 13 semi-structured interviews. All the interviews were conducted by three researchers, with sociology, technology and pedagogic backgrounds. Twelve interviews were conducted face to face, at the hospitals. One interview was conducted by telephone, since the informant had to postpone our interview appointment when we visited the hospital. We interviewed nurses, physicians and specialists from both hospitals. The informants were selected on the basis of their roles; working with stroke patients in the acute phase and/or having participated in VC consultations. The interviews lasted from 20 minutes to two hours. They were semi-structured by an interview guide, managing pre-defined themes and questions but at the same time opening up for the informants’ own contributions on issues they regarded as important. Some informants also introduced the topics of equipment and the workplace while talking, which affected the length of the interview. All interviews were audio recorded, then transcribed. All the transcriptions were categorized according to comments that seemed to be repeated by the practitioners. In total, the results constitute our approach for understanding the need for knowledge-sharing and the non-use of VC.
As a part of understanding the overall treatment of stroke patients, both in the acute phase and in the rehabilitation phase, we were introduced to the organization of stroke treatment in the hospitals. This includes the patient trajectory from arrival in the emergency ward to the rehabilitation room. In this way, we were able to understand the organization of the work and the role of VC in daily stroke treatment. This included conversations with professionals involved in different stages of the stroke treatment (meeting the patient at the ambulance, the laboratory personnel and CT personnel), but as they were not the ones using the VC equipment in the consultations, they were not included as informants, but as a resource for understanding the treatment of stroke patients.
3. Results and Discussion
The referring hospital reported 39 patients with diagnosis stroke in the 12-month period from March 2011 to March 2012. In the period from September 2010 to April 2012 (19 months), the VC equipment was only used four times for discussing patients. As the data illustrates, the number of stroke patients is considerably higher than the number of times the professionals collaborate by using VC. To fulfill the national goal of providing more patients with thrombolytic treatment, and to improve the stroke prognosis, collaborative work is a premise. Every case is considered individually, directed by some norms, which could be discussed in each case. Thrombolytic treatment is given under the instruction of a specialist, whose competence the small hospitals do not have. This requires collaborative work between hospitals. How may we understand the contradiction between the need for knowledge-sharing and the reasons for the low frequency of use of VC for discussing stroke patients?
The experiences of the use of the VC equipment reveal no challenges in the practical use of the technology as a tool per se. All the professionals have gone through training. The informants that had used or tested the VC equipment had positive experience and said that it was easy to use. Regarding the technology as a tool in practice, the professionals say:
“All interns have training. We have an introduction course for interns and training in stroke procedures. The use of videoconferencing is a part of it.” A: Referring hospital.“I think it has worked fine.” B: Referring hospital.“The technology has worked fine; it has not been any …”Interviewer: “It is easy and understandable?”“Yes, yes I think so.” “(…) it is quite easy, easy to understand…Yes, it is easy to use. Nothing was problematic regarding the technology.” C: Specialist hospital.
It was an overall agreement that it would have been easier to include as a tool in daily services if it had been used more frequently. As the comments illustrate, VC as a tool per se is not the reason for low frequency use for discussing stroke patients.
3.1. Organization of Knowledge
The referring hospital is organized according to normal standards for small hospitals in Norway. The stroke patients arrive at the hospital through the emergency unit. There, the intern on duty evaluates the patient. Stroke patients are sent for blood tests and CT scanning. The intern decides if thrombolytic treatment is relevant for the patient, based on procedures for treatment. If the intern does not consider thrombolytic treatment as an option, the use of VC is not considered. If necessary, the intern contacts the second on-call specialist to discuss treatment options. If thrombolytic treatment is considered as an option, the nurses prepare for a VC meeting. If the second call on duty wants to discuss the case, he or she calls up (by telephone) the specialist hospital. They decide if the patient is to have thrombolytic treatment, if so, they connect via VC.
“The intern starts the procedure (…) for a stroke regardless whether it’s day or night. Inform the second call and take responsibility for having the blood tests (…) and the CT rapidly. (…) Thrombolytic treatment and CT are considered, and the second call considers the patient. Thrombolytic treatment is not given by the interns themselves. There is always a second call and/or a neurologist involved. We have our procedure. But, if it is a patient where this [thrombolytic treatment] per definition is prevented (…) then the second call does not have to be involved” A: Referring hospital.
The physician describes how they are organized:
“They [the interns] are the ones who see the patient’s condition first, who are in the arrival and who have to make a kind of judgment or decide how serious this is. Should we call someone …” F: Referring hospital.“The intern who is on duty calls, as per the procedure, I come in and we wait together to be ready.” E: Referring hospital.
As the referring hospital does not have a neurological department, stroke patients are treated in the medical department. In the evening period, the interns on duty need to cover several departments.
“The interns work both acute and on the medical department at the same time during evenings and nights. It means that new interns starting at the surgical department must also handle the medical part. We have stroke patients, medical patients … no neurological department.” A: Referring hospital.
Even though the interns are newly arrived the hospital, staying in i.e., the surgical department, he or she must handle medical problems related to other departments as well. The interns work both in acute care and the medical department during evenings and nights.
3.2. Access to Knowledge
Access to a second opinion at the hospital is organized with a second call on duty 24 hours a day. During the day, the physician is in the hospital. During evenings and nights the second call is not at the hospital, but within a specified time limit near the hospital.
“The treatment of a stroke is in principle the same regardless of time of day or night. We have our routines: we examine, take blood tests, CT, is the standard examination … it happens regardless of what time. Everyone knows it, or should know (…). Both interns and us [physicians]” A: Referring hospital.
Here the physician describes how routines are a way of managing the treatment. Even though the knowledge is organized across departments, the routines constitute the practice. Both interns and physicians follow standard rules for treatment. If the intern decides on thrombolytic treatment, the treatment is discussed with the second on-call specialist. As physician D explains, the physicians may not have worked specifically with stroke patients before. Since the referring hospital does not have a neurologist, they need to contact the specialist hospital in all cases when considering thrombolytic treatment.
“When it comes to thrombolytic treatment, the second call night duty is always involved. We do not have a neurologist here. It is chief physicians on duty, stand-ins, who do not do stroke treatment in the hospitals where they come from. Therefore, we think there should be a neurologist involved in our discussion.” D: Referring hospital.
The need for access to knowledge is first searched for locally, defining the need for further knowledge by evaluating standardized rules for stroke treatment. Secondly, if thrombolytic treatment is an option, neurologists at the specialist hospital are contacted.
Even though the specialist hospital has its own neurological department, with physicians who are specialists in their field, they have also been organized in a way that they have interns on duty during nights and evenings. They also have their second on-call duty specialist located within a specific time limit from the hospital. The interns at the specialist hospital call up their second on-call specialist on duty if they cannot handle the question from the smaller hospitals. They do not decide on thrombolytic treatment without discussing it with their second on-call specialist on duty. Hence the VC equipment is only used when the specialists are staying in the specialist hospital.
“After 19.30 on week days, we cannot use videoconferencing. Not after 13.00 Saturdays and not Sundays.” A: Referring hospital.Interviewer: So, if the service had been there 24 hours a day, could it have been more helpful?“If there had been more routines on it; it would have been used more often.” G: Specialist hospital.
Having stroke patients arriving 24 hours a day requires access to competence at all times. As the service is only available from 7:00 in the morning to 7:30 in the evening, most of the informants indicated that it would have been better, easier with the same routines 24/7, and that they would have been feeling safer if they were able to use the VC equipment whenever a difficult case came in during day/night. Most of the specialists were positive about a 24/7 service, but some of the more experienced ones did not think it was a good idea. They indicated that in the evenings they will only meet a less experienced doctor who has to contact the “on-call” duty specialist for backup when they get inquiries regarding stroke patients, and they will only have the phone. Otherwise the specialist has to come to the hospital to participate in the VC consultation, which could delay the treatment of the patient. The traditional use of the telephones gives access to knowledge regardless of the time, as the second calls on duty in the specialist hospital may be contacted at their homes and do not have to travel to the hospital to access the VC equipment.
3.3. Organizational Practice as a Challenge for Access to Knowledge
In this article we analyze the contradiction between the need for knowledge-sharing through VC technology as well as the reasons for the low frequency of its use for discussing stroke patients. The results illustrate how the technology per se is not the reason for the low frequency use of VC. We argue for analyzing technology in practice not according to single problems, but according to the stroke treatment activity as a whole. Further, we analyze the use of VC as a tool for the treatment of stroke patients, where the outcome is seen as individual stroke treatment, sharing knowledge between the local and the specialist hospital. We are searching for reasons for the low frequency of use, which demands analyzing the activity—here, the referring hospital—as an activity system.
The patient arrives as an acute case, where time is critical. When the patient arrives, the intern is the one who evaluates the patient’s condition. This is the first contradiction in the activity: considering following standard rules for thrombolytic treatment, or discussing every case individually. The work is organized so that the intern is the one deciding if the patient is a candidate for thrombolytic treatment, or if the second call on duty should be contacted. This is the second contradiction between the division of labor and the subject, in this case the intern. If the intern wants to discuss the patient, or decides to give thrombolytic treatment, the second call on duty is contacted. Here, the third contradiction is between the tool and the institutional rules for stroke treatment. They follow the use of the VC technology for discussing stroke patients relatively strictly. If the patient is not a candidate for thrombolytic treatment, they do not use the VC equipment. If the rules for giving thrombolytic treatment are fulfilled, they use VC as a tool for obtaining approval or a second opinion for giving or not giving the treatment.
Health care is shaped by behavior, traditional rules, standards and division of labor. In this case, the reason for low frequency use may be explained by constant reproduction of the activity. The use of VC for stroke, often referred to the use of telemedicine, in its nature conflicts with traditional routines and the way of performing daily work practice. An activity system, such as a hospital, produces a large number of actions, often repeated with small variations. Over time, actions become automatic, as routines. Each phase in the stroke consultation may be seen as an action situation, where each action is shaped by, and in turn gives shape to, the historically evolving structure and contradictions of the entire activity system. Medical cognition is a collaborative achievement between the professionals at the referring hospital. The interns use the procedures as a tool to manage their problems, or search for the second call on duty. The second call on duty traditionally uses the telephone to discuss medical problems. In this sense, Norwegian health care is deeply rooted in traditional ways of performing treatment. To reach the potential of telemedicine, and for knowledge-sharing, professionals must change the traditional way of performing and thinking medical practice.
We argue that to fulfill the national goal to provide more patients with thrombolytic treatment, cases of stroke patients where the indications are blurred need to be discussed. In a CHAT perspective, each activity system has its own motives for a particular outcome. Both interns and the physicians may aim to fulfill the goal of giving thrombolytic treatment, following rules for such treatment. Changing the motive for the action from giving thrombolytic treatment to knowledge-sharing between professionals for improved stroke treatment may change the use of VC technology as a tool. Here, the motive is visual collaborative work, emphasizing the opportunity to see the situation, instead of the telephone’s capability to only hear a professional’s descriptions of stroke patients.
Here, VC is designed to be used, not only for a single problem, but for multiple discussions for individual treatment and knowledge-sharing. The use of VC is a tool for knowledge-sharing, and access to several stroke cases may develop knowledge. Over time, sharing knowledge may assess the ability of determining stroke treatment in the emergency unit. Sharing knowledge, as in the four times the VC has been used, opens for the door for analyzing the collaborative practice about the shared object in the boundary zone. These situations illustrate how routines and patterns are challenges in changing behavior, standards and rules. As several activity systems collaborate—in this case the referring hospital and the larger one—stroke treatments for patients can expand.
4. Conclusions
Previous research has referred to characteristics about the technology, user and staff resistance [18], difficulties when using the technology [19], or more general barriers for adoption [20] as obstacles for using VC. However, from our findings, we can say that the VC technology is ready for this kind of use. It is clearly easy to use and works without any problems, and the users seem satisfied. A positive effect of such consultations is the possibility of knowledge-sharing from more experienced specialists at the specialist hospital to the physicians at the referring hospital.
Here, we argue for the importance of contradictions at the level of the institutional activity system for the understanding of difficulties and low frequency use in medical cognition. By using CHAT as a framework for understanding low frequency use of VC as a tool for discussing individual stroke treatment, we illustrate how traditional ways of performing stroke treatment is a challenge for future development. In this article, we illustrate inner contradictions in a medical activity system. The treatment activity is shaped by institutional rules and division of labor, which affects the way the treatment activity is performed. To understand innovation in the future, it is important to understand the historic way of performing an activity, i.e., the organizing of health care and how knowledge is traditionally accessed in health care.
The results show that VC for collaborating between the activity systems was used only four times. Since the equipment, the network, and the routines works fine, we can only believe that it will take more time to have VC fully integrated in stroke services within health care. However, as a discreet conclusion for future e-health; there is clearly a need for future internet to ensure a secure and reliable connection for VC services between health care institutions, as we believe it takes a long time for a large organization to adjust to new routines, technology, and services.
We will continue our research within the area, which will make it possible to analyze what happens in the boundary zone between the two activity systems: the zone where the collaborative activity expands the stroke treatment and might create a new collective practice. Discussing medical problems may improve knowledge among health care professionals and prepare them for medical conditions that are constantly emerging. It may also prepare the health care system for technological changes in society in general, expanding from using traditional telephones to more modern forms of communication. As the patients use modern technology and access an increasing amount of medical information by using these technological tools, the expansion from collaboration by telephone to VC may prevent the health care system from falling behind.
Acknowledgments
We wish to thank the practitioners who agreed to participate in the study. We acknowledge the collaboration with the chief physicians at the two hospitals. Thanks to Kari Dyb for taking part in the interviews and discussion of the findings.
References
- Thomassen, L. Akutt hjerneslag—Ei orientering til pasientar og pårørande. Available online: http://www.helse-bergen.no/aktuelt/tema/hjerneslag/Sider/akutt-hjerneslag.aspx (accessed on 8 March 2012).
- Helsedirektoratet. Health Directorate National guideline for stroke treatment and rehabilitation. Available online: http://www.helsedirektoratet.no/publikasjoner/nasjonal-faglig-retningslinje-for-behandling-og-rehabilitering-ved-hjerneslag-kortversjon/Publikasjoner/Nasjonal-retningslinje-for-behandling-og-rehabilitering-ved-hjerneslag-(kortversjon).pdf (accessed on 8 March 2012).
- Hess, D.C. Telestroke: Extending stroke expertise into underserved areas. Lancet Neurol. 2006, 5, 275–278. [Google Scholar] [CrossRef]
- Rønning, O.M.; Thommassen, L.; Russell, D. Kvalitetsindikatorer for behandling av akutt hjerneslag. Tidsskr. Den Nor. Legeforening 2007, 127, 1219–1223. [Google Scholar]
- Thomassen, L. Behandling av akutt hjerneinfarkt. Tidsskr. Den Nor. Legeforening 2007, 127, 1060–1063. [Google Scholar]
- Schwamm, L.H. A review of the evidence for the use of telemedicine within stroke systems of care. Stroke 2009, 40, 2616–2634. [Google Scholar] [CrossRef]
- Handschu, R. Telemedicine in acute stroke: Remote video-examination compared to simple telephone consultation. J. Neurol. 2008, 255, 1792–1797. [Google Scholar] [CrossRef]
- Meyer, B.C. Efficacy of site-independent telemedicine in the STRokE DOC trial: A randomised, blinded, prospective study. Lancet Neurol. 2008, 7, 787–795. [Google Scholar] [CrossRef]
- Demaerschalk, B.M.; Bobrow, B.J.; Raman, R.; Kiernan, T.E.; Aguilar, M.I.; Ingall, T.J.; Dodick, D.W.; Ward, M.P.; Richemont, P.C.; Brazdys, K.; et al. Stroke team remote evaluation using a digital observation camera in Arizona: The initial mayo clinic experience trial. Stroke 2010, 41, 1251–1258. [Google Scholar]
- Hutchins, E. Cognition in the Wild; MIT Press: Cambridge, MA, USA, 1995. [Google Scholar]
- Om oss. Available online: http://www.nhn.no/om-oss (accessed on 13 April 2012).
- Engeström, Y. Learning by Expanding: An Activity-Theoretical Approach to Developmental Research; Orienta-Konsultit: Helsinki, Finland, 1987. [Google Scholar]
- Engeström, Y. Activity Theory and Individual and Social Transformation. In Perspectives on Activity Theory; Engeström, Y., Miettinen, R., Punamäki, R.-L., Eds.; Cambridge University Press: New York, NY, USA, 1999; pp. 19–38. [Google Scholar]
- Kaptelinin, V. The object of activity: Making sence of the sence-maker. Mind Cult. Act. 2005, 12, 4–18. [Google Scholar] [CrossRef]
- Kerosuo, H. Boundaries in Health Care Discussions: An Activity Theoretical Approach to the Analysis of Boundaries. In Managing Boundaries in Organizations. Multiple Perspectives; Paulsen, N., Hernes, T., Eds.; Palgrave: Basingstoke, UK, 2003; pp. 169–187. [Google Scholar]
- Lund, A.; Rasmussen, I.; Smørdal, O. Joint Designs for Working in Wikis. A Case of Practicing Across Settings and Modes of Work. In Activity Theory in Practice: Promoting Learning across Boundaries and Agencies; Daniels, H., Edwards, A., Engeström, Y., Gallagher, T., Ludvigsen, S.R., Eds.; Routledge: New York, NY, USA, 2010; pp. 207–230. [Google Scholar]
- Miller, G.; Dingwall, R. Context & Method in Qualitative Reserch; Sage Publications: London, UK, 1997. [Google Scholar]
- Anderson, J.G. Evaluating Health Care Information Systems: Methods and Applications; Carolyn, E.A., Stephen, J.J., Eds.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1993; p. 322. [Google Scholar]
- Gelber, H.; Alexander, M. An evaluation of an Australian videoconferencing project for child and adolescent telepsychiatry. J. Telemed. Telecare 1999, 5, 21–23. [Google Scholar] [CrossRef]
- Rogove, H.J.; McArthur, D.; Demaerschalk, B.M.; Vespa, P.M. Barriers to telemedicine: Survey of current users in acute care units. Telemed. eHealth 2012, 18, 48–53. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Nilsen, L.L.; Solvoll, T. Traditional Practice vs. New Tools and Routines in Stroke Treatment. Future Internet 2012, 4, 688-699. https://doi.org/10.3390/fi4030688
AMA Style
Nilsen LL, Solvoll T. Traditional Practice vs. New Tools and Routines in Stroke Treatment. Future Internet. 2012; 4(3):688-699. https://doi.org/10.3390/fi4030688
Chicago/Turabian StyleNilsen, Line Lundvoll, and Terje Solvoll. 2012. "Traditional Practice vs. New Tools and Routines in Stroke Treatment" Future Internet 4, no. 3: 688-699. https://doi.org/10.3390/fi4030688