1. Introduction
The number of information and communication technology (ICT) users worldwide is dramatically increasing. People around the world are using ICTs, particularly the internet, for various purposes. According to Norman
et al., the ICTs act as an amplifier of human abilities, since they can amplify the human ability to communicate and create [
1]. Some of the purposes people are using ICTs and the internet for, are also health-related. In their study, Kummervold
et al., have discovered that the use of the internet as a source for health information is growing in all age groups and for both genders. In their population study, they have found that users are also using the internet as a communications channel, both for reaching health professionals and for communicating health issues with their peers [
2]. The term e-Health was first introduced in the late 1990s as a new term that describes the combined use of ICT, especially the internet, in the health sector [
3]. The field of e-Health represents the promise of ICT to support, improve or enable health and the healthcare system [
4].
Faced with increasing costs of patient treatment, and unfavorable demographic changes because of an aging population, health-care systems are focusing on efficient cost reduction without impairing health-care quality. The Ministry of Health in Slovenia presented e-Health as a possible solution to the problem and presented Slovenia’s e-Health strategy to develop an efficient, flexible and modern national health-care informatics system [
5,
6].
Being familiar with all the benefits of e-Health and the strategic plan for the Slovenian health sector’s informatization, the University of Maribor, along with other partners, has initiated an e-Health project. The project group is developing various e-Health services that are based on modern ICT solutions and will be available on several screens, such as television, personal computer, smart-phone and tablet. Depending on the purpose of use, the specificity and utility, the e-Health services in the project can be roughly divided into two groups:
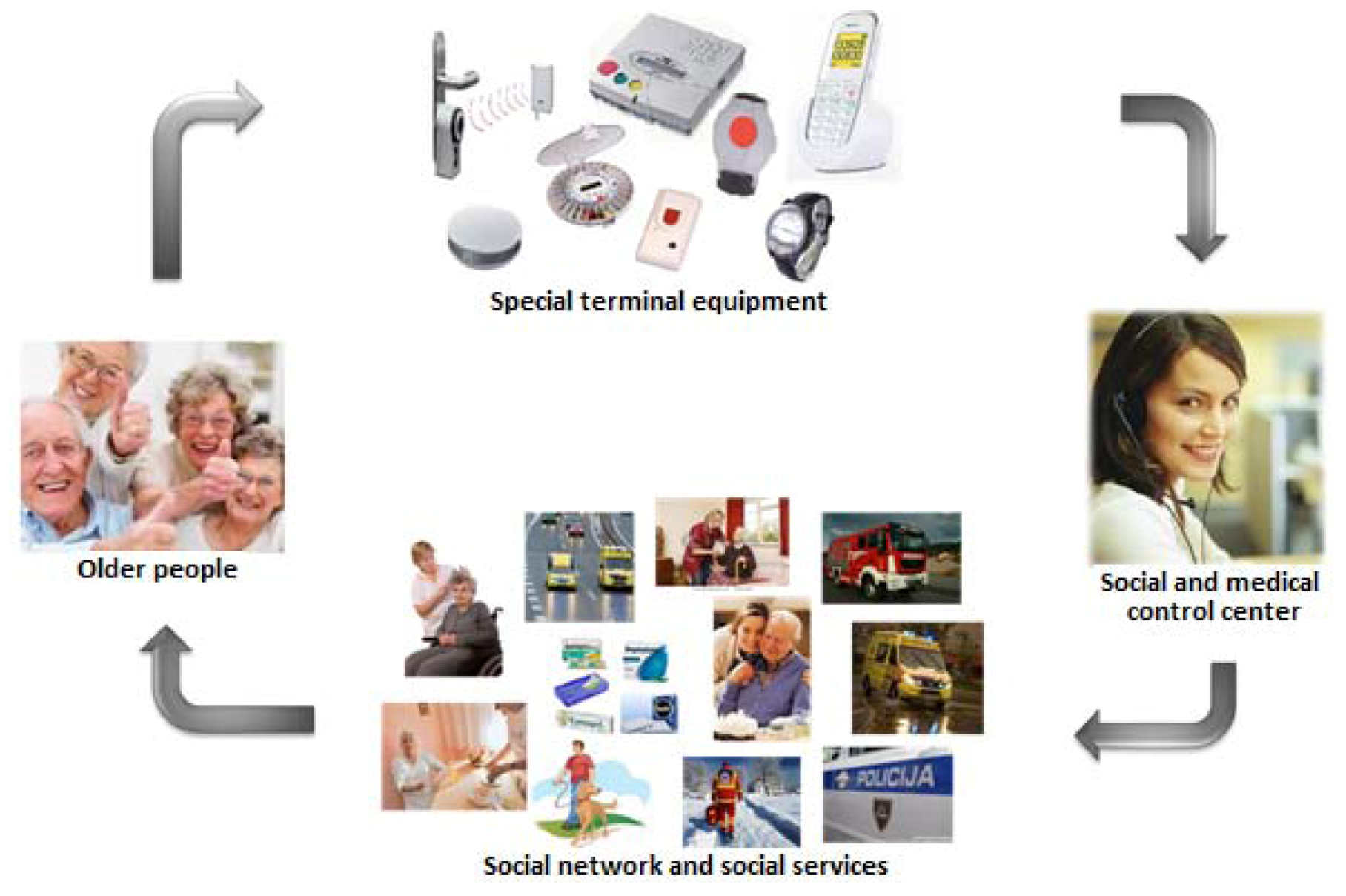
• Fully integrated telecare services for easy and safe independent living at home for older adults;
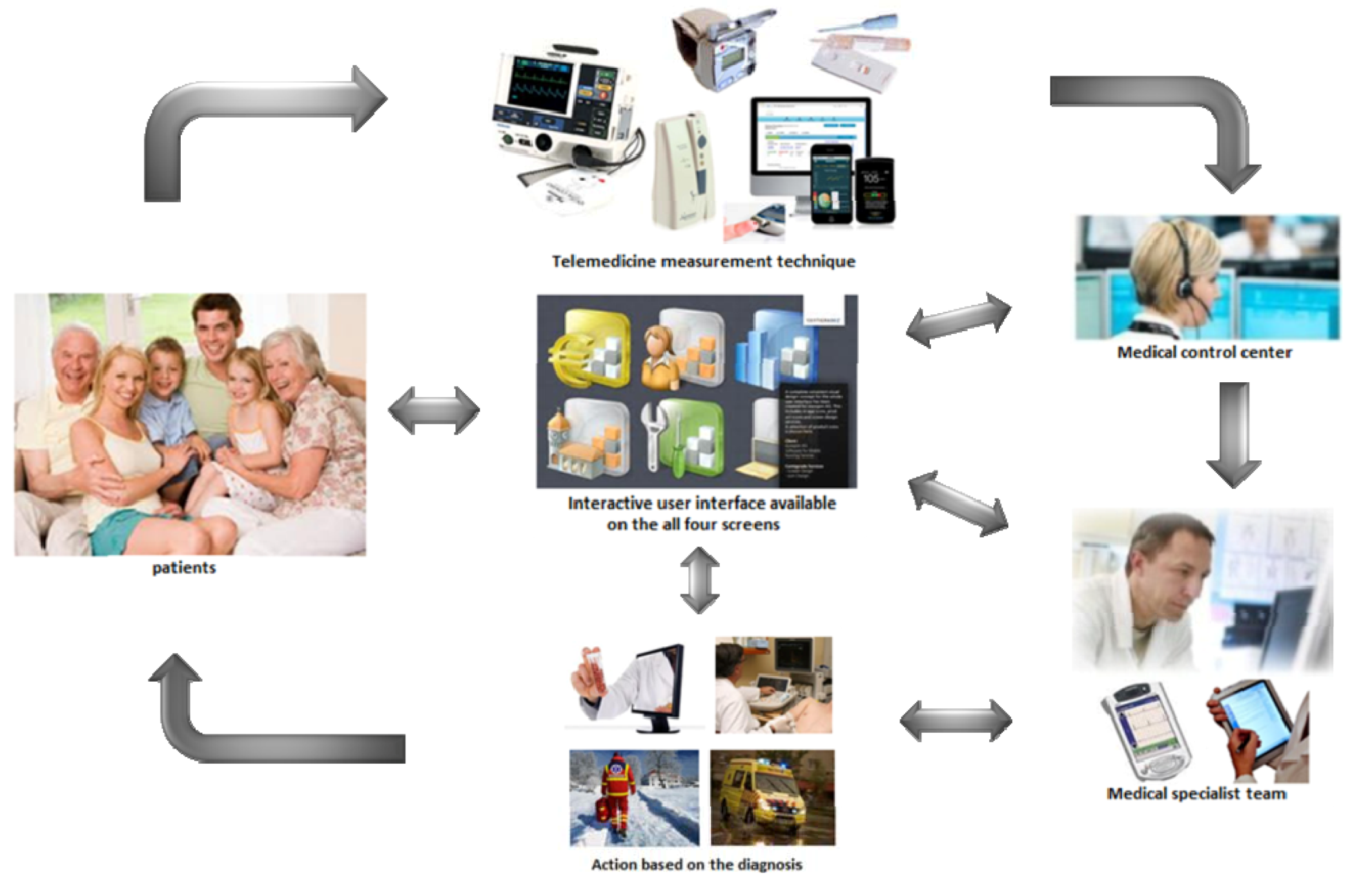
• Fully integrated telemedicine services for the remote monitoring of patients with chronic diseases, for home-care or for general practice care;
Telecare services are intended for older adults in order to provide them with longer, easier and safer living in their homes. The telecare services enable older adults to choose where and how they would like to spend their old age. This is one of the possible ways in which the needs for the institutional care for older adults and the pressure on nursing homes could be reduced. The telecare services developed in the e-Health project are presented in
Figure 1.
Telemedicine services are intended for the remote monitoring of various chronic diseases. These services increase the availability of specialist medical services in rural areas and provide the possibility to obtain a second opinion. Additionally, the telemedicine services shown in
Figure 2 provide specialist support for general practitioners, health workers, health resorts and insurance companies.
Figure 1.
e-Health project: the process of fully integrated health-care delivery.
Figure 1.
e-Health project: the process of fully integrated health-care delivery.
Figure 2.
Telemedicine services.
Figure 2.
Telemedicine services.
Despite all the benefits, institutions and organizations can spend enormous amounts of resources on e-Health projects that eventually fail. This usually happens when the e-Health services do not meet the needs and expectations of their users [
7]. Numerous design guidelines exist to support the design for different types of users. However, relying only on guidelines is not enough. Insufficient user involvement in the design and product architecture of e-Health services and the lack of evidence demonstrating the impact of e-Health services bring difficulties when it comes to the users’ acceptance and adoption of such services. In order to understand which e-Health services the users value most and how best to provide those services, designers and product architects need to involve the intended users of the e-Health services throughout the entire design process. The approach where extensive attention is given to the needs, wants and limitations of the users of the products and services, each stage of the design process is known as user-centered design (UCD) [
8]. Various UCD methods and techniques are well known and widely used, both in academia and in the research community. However, conventional UCD methods and techniques are not completely appropriate for a large diversity of users. Part of this problem lies in the differing user characteristics, languages, cultures, environments and motivations among the vast number of users. To get valuable results for their studies, instead of using the conventional UCD methods, user researchers should adapt the UCD methods for their target population.
This paper describes how four UCD methods (wants and needs analysis, focus groups, interviews and SUS questionnaire) have been modified to support the research study for the e-Health project for the target population. The research study was done for an e-Health service, named MedReminder. The target population of the MedReminder service are older adults i.e., people over 65 years. Therefore, the four UCD methods were modified and adapted for older adults.
2. Experimental Section
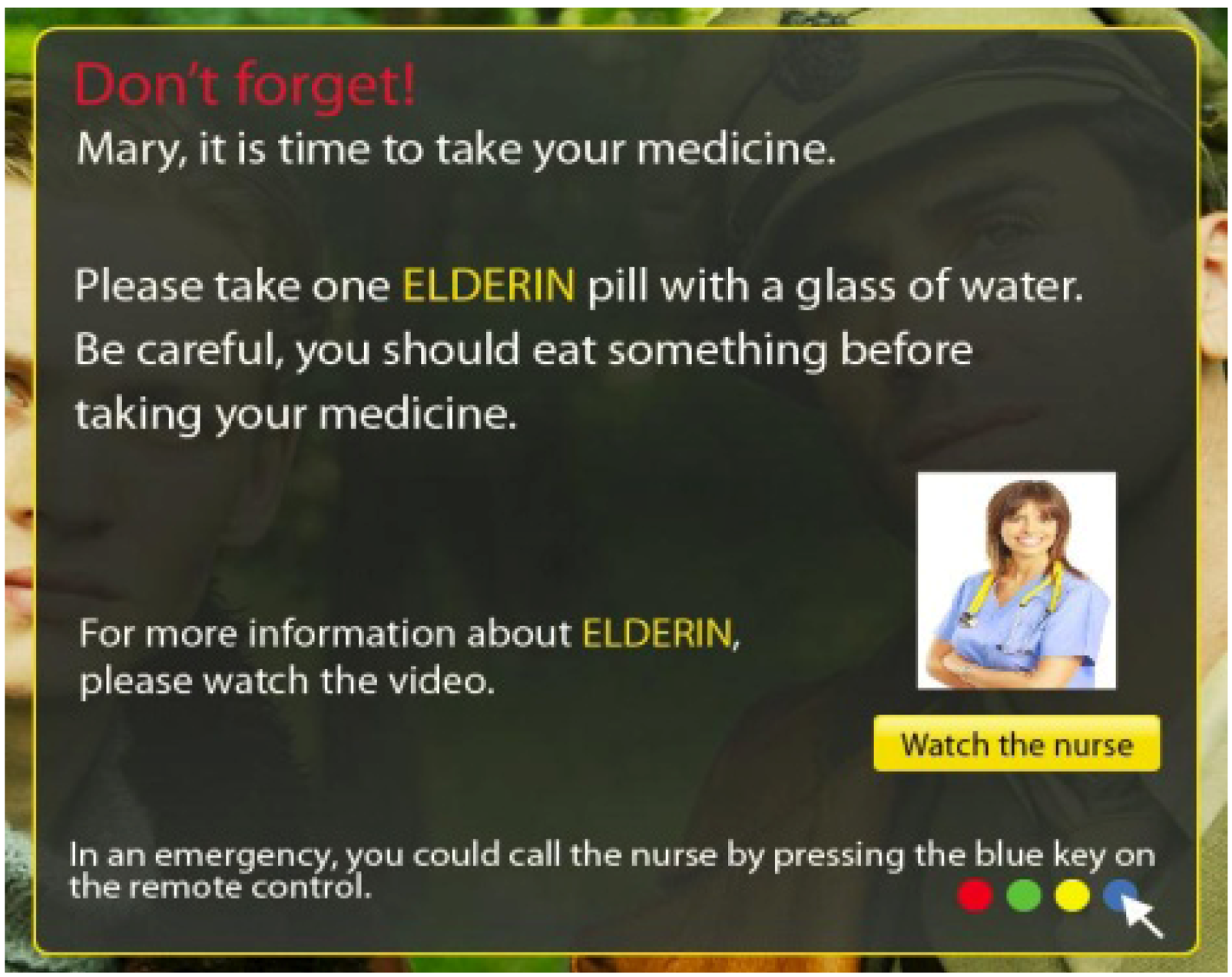
The focus of the research study presented in this paper is the UCD process for a telecare service named MedReminder. The MedReminder service is intended to remind people to take their medicines on time or to call a relative or a medical person in an emergency situation [
9] as shown in
Figure 3. The service can be used in an interactive TV system. It was assumed that MedReminder will be mostly used by adults older than 65. The reason for this assumption is that older adults use more medications than any other age group since most of them live with one or more chronic conditions, such as diabetes, high blood pressure, arthritis or cancer. Additionally, many older adults take multiple medications at the same time. As a result, the UCD process for MedReminder was created from the perspective of older adults.
Figure 3.
Reminder for taking a medicine.
Figure 3.
Reminder for taking a medicine.
The term UCD has its origins in the mid 1980s. One of the best known guides in implementing the UCD approach in practice is ISO 13407, which defines the standards that support the design, development and evaluation of usable products [
10,
11]. The standard represents a general reference and describes five main activities for a software life cycle: plan the human-centered process, specify the context of use, specify the user and organizational requirements, and produce the design solutions.
Taking into account the described activities in ISO 13407 and the criteria for selecting the methods in UCD [
12], for the purpose of the MedReminder, the following methods were selected:
• Wants and needs analysis. This is a quick, inexpensive and brainstorming method for gathering data about users’ wants and needs from multiple users simultaneously.
• Focus group. For this method, a group of six to 10 people is brought together to discuss their experiences or opinions about a topic presented by the user researcher.
• Interview. This method is one of the most frequently used methods for gathering user requirements.
• Questionnaire. For the purposes of this study, the system usability scale (SUS) questionnaire was chosen.
2.1. Adapting a Wants and Needs Analysis for Older Adults
Gathering requirements from older adults is considerably more difficult than it is from other groups of people [
13]. For example, most older adults have never used e-Health services. Hence, when asking them questions about their wants, needs or expectations from an e-Health service that they are not familiar with, they will not always know what they would really like. Additionally, when presenting them a single alternative for the service, they might have problems estimating whether they like the alternative or not. Another important problem that usually appears with older adults is that they are often reluctant to complain or criticize products or services.
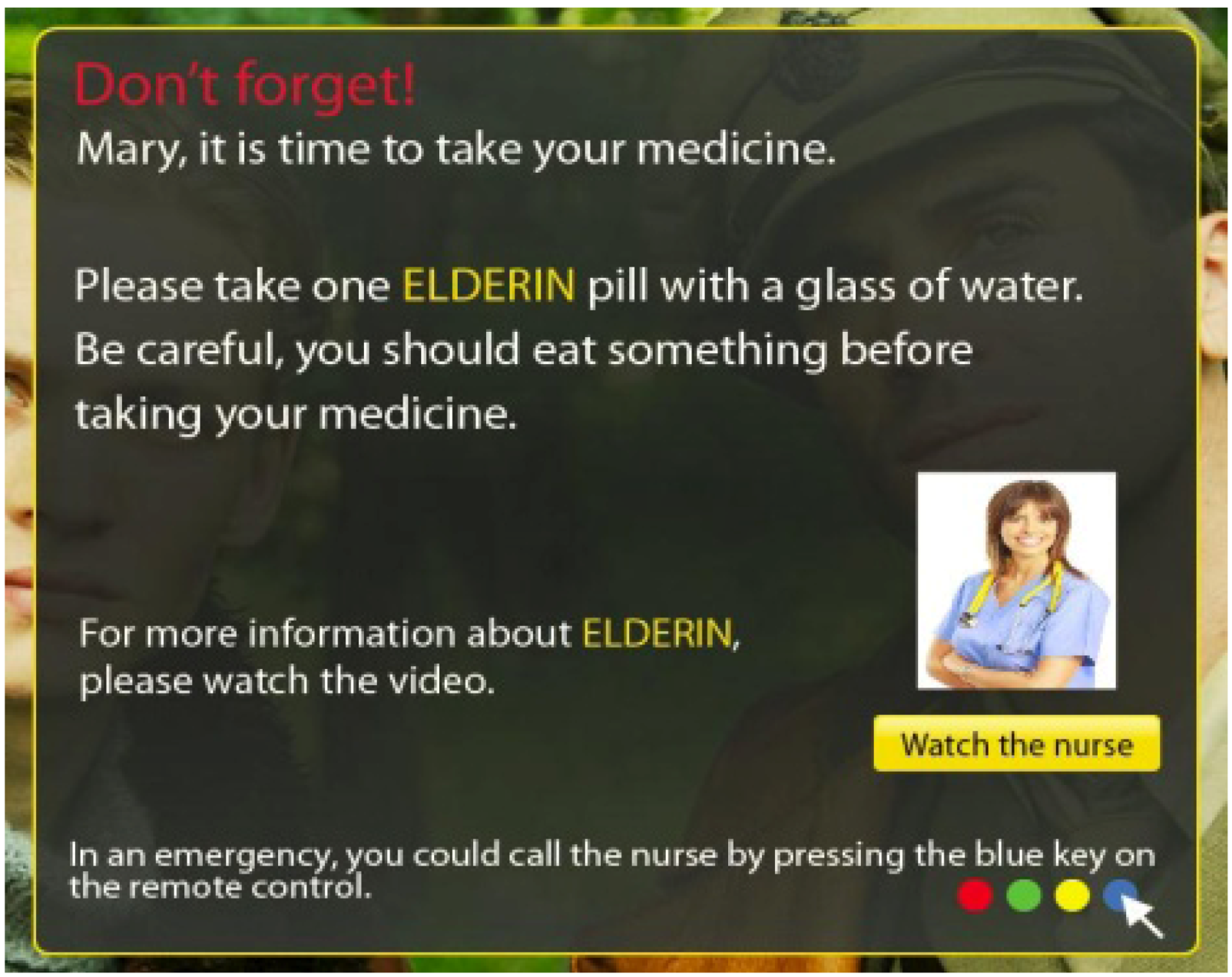
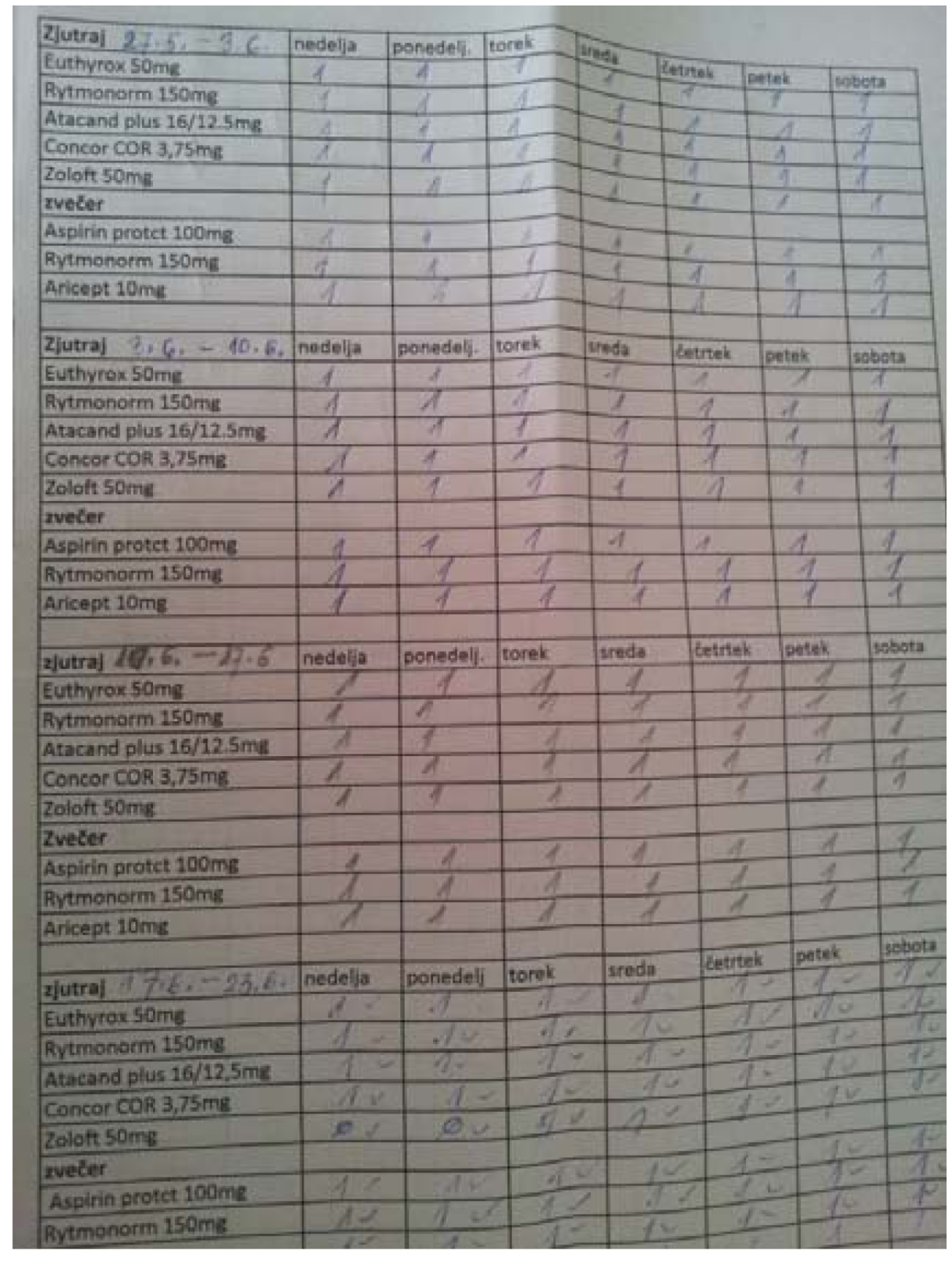
Figure 4.
An example of a medicine reminder.
Figure 4.
An example of a medicine reminder.
In order to get valuable results for what the intended users want and need from the MedReminder service, we visited the study participants in their homes. At the start, we talked about general things and got to know each other well. As a result, the study participants became confident in talking to us, the researchers. Later, we asked the participants about their general health condition and their medication usage. We were interested in whether they were taking any medications, what were their experiences and habits when taking the medications and, whether and how often they were forgetting to take the medications. In addition to the answers on our questions, some of the study participants showed us the procedures they were using to remember to take their medicines. For example, a 75-year-old lady with mild dementia was using a list of medicines with use instructions, as shown on
Figure 4. Each time she took a medicine, she put a mark on the list, so that she and her relatives would know that she did not forget to take the medicine.
Then we presented the study participants with the MedReminder service and some basic use-case scenarios, so that they would become acquainted with MedReminder. When we were positive that the study participants had become familiar with MedReminder, we made some stories and asked participants to play a certain role when using MedReminder. For example, one of the study participants, a 72-year-old lady, was playing the role of a diabetic patient. In her role, she was supposed to take two different kinds of medicine twice a day. While playing the role, she explained what the reminder message should look like and what kind of information it should contain to be useful. Several other study participants played this and similar roles.
As can be seen from the text above, for the purpose of the MedReminder study, the conventional wants and needs analysis method was adapted for older adults. Instead of conventional requirements gathering, we presented the MedReminder service in a real case scenario and asked the participants to play real case roles. After the method’s adaptation, the study participants had an idea of what the MedReminder service is and what they could gain from it. As a result, it was easier for them to think about the service and express their wants, needs, requirements and limitations.
The results from the modified wants and needs analysis were considered and a prototype for MedReminder was developed.
2.2. Adapting Focus Groups for Older Adults
In the next step of the study, we organized two focus groups. Several authors have reported [
14] that it is not easy to keep a focus group of older adults focused on the subject being discussed. Unfamiliar environments and social meetings with unfamiliar people may exhaust users quickly. To overcome such problems, we organized both focus groups for MedReminder in the participants’ premises, where they were in a familiar and safe environment. The focus-group participants were selected among relatives and friends,
i.e., they knew each other from before. The first focus group was organized in a married couple’s premises. Most of the participants that took part in this focus group (eight out of nine) were also married couples and they had all been friends for many years. The other focus group was organized in a widowed lady’s premises. The other participants in this group were also living alone and knew each other from before–they were either friends or neighbors.
The focus groups for the MedReminder study differed from conventional focus groups in the location where the focus groups took part and the way the participants were selected. As already stated, both focus groups took part at a location where all the participants had already been and with whom they were familiar. This is contrary to the usual research practice, where focus groups take part in a laboratory, at a university or some other research institution. Such locations are problematic for older people, for many reasons. For example, they may have problems with transportation, since they usually live in environments that are far away from universities and research institutions.
The next adaptation made in the MedReminder study was the way the focus-group participants were selected. In conventional focus groups, participants are selected among various users that match the selected user type. In our study, besides matching the selected user type (older adults), the study participants were either friends or neighbors, had a similar way of living and similar interests.
Both focus groups’ adaptations made for the older adults for the MedReminder study provided an atmosphere in which the participants were encouraged to value their own opinions, express themselves honestly, and enjoy their experience.
2.3. Adapting Interviews for Older Adults
Widely used interviews present a guided conversation in which the researcher seeks information from the user. As such, the interviews depend a lot upon the users’ self-reporting skills. In our experience, older adults usually have little experience with modern technology. Concerning modern technology, they usually find it difficult to identify and report anything other than a general impression, such as “I think this is complicated” or “This service does not work”. They are not familiar with the technical terminology and so it is difficult for them to express the problems they encounter. Confusion among older adults without previous experience with technology is often general, poorly reported and non-specific.
To overcome this kind of communication problems, during the interviews for the MedReminder study, participants were provided with a TV set where the MedReminder service was installed. So, whenever they wanted to express an opinion or a problem about the service and did not find the appropriate words, they just demonstrated the problem using the technology. According to them, this was much easier than when they were trying to describe their thoughts with words.
As can be seen above, the conventional interviews were adapted for the older adults. In addition to the guided conversation, during the interviews, the participants in the MedReminder study were also able to demonstrate the way in which they were using the service.
2.4. Adapting the SUS Questionnaire for Older Adults
Different questionnaires are another type of method that is regularly used by researchers when conducting user studies. The problem that appears with older adults is that they are more likely to use “do not know” responses to questions that have complex syntax or are semantically complex [
15]. Additionally, many questionnaires include technical terminology that older adults do not use in their everyday lives, and because of that, they are not familiar with it. In order to evaluate the overall satisfaction with the MedReminder service, we used the SUS questionnaire. The SUS questionnaire is composed of 10 statements and can be used to evaluate the usability aspects of a variety of products and services [
16].
To obtain usable results, we modified the SUS questionnaire in such a way that we used terminology that is understandable by the older adults. Furthermore, we tried to use sentences and questions that are syntactical and semantically simple. Last, but not least, we have replaced the word “system” with the name of the service, i.e., MedReminder.
For example, the fifth item in the original SUS questionnaire is: “I found the various functions in this system were well integrated”.
After the modification, the fifth item from the SUS questionnaire was: “I found the various functions in MedReminder are logically connected together”.
Before submitting the SUS questionnaire to the study participants, we kindly asked them when expressing their opinions about the statements in the questionnaire to try to avoid the neutral option. If they found something in the questionnaire that was incomprehensible, we asked the participants to require us to help them out instead of choosing the neutral option.
3. Results and Discussion
Four UCD methods were used in the research study. All four UCD methods were adapted for the intended users of the MedReminder service, i.e., older adults.
3.1. Study Participants
Twelve participants took part in the research study. Five of them were male and seven were female. There were four married couples among the participants. The remaining four participants lived in a single household. The youngest participant was 67 years old, whilst the oldest participant was 79 years old. The average age of the study participants was 72.17 years.
At the beginning of the study, important information about participants’ wants, needs, backgrounds and concerns was gathered with the modified wants and needs analysis. Six of the participants had a university diploma; five of them had finished some high school, while just one had finished only elementary school. Five participants out of 12 were using computers. On the other hand, all 12 participants owned a mobile phone and watched TV regularly. The study results showed that on average, the participants spend approximately 3.5 hours a day watching TV. Many of them explained they usually watch TV in the evenings, after 6:00 pm.
The participants described their general health condition as appropriate for their age. The most common diseases reported among the participants were high blood pressure, high cholesterol, stomach diseases and diabetes. Some of the participants had some additional chronic diseases they did not want to reveal. All 12 participants reported they were taking medicines on a daily basis. Seven of them take a medicine only once a day. Three participants take a medicine three times a day and only two of them take their medicine twice a day. When asked whether they were forgetting to take their medicines, both prescribed and not prescribed, the participants reported they usually do not forget; however there were times when they failed to remember to take the medicine. The participants presented several different remembering procedures, such as: special medicine boxes, particular medicine placements (near the remote control, on the table in the living room, in the kitchen), lists and medicine schedules, and “living” reminders (usually partners, children or relatives). In our discussions with the participants, we also found out that often they forget the instructions about taking a specific medicine. To help them in such situations, video clips containing the instructions were added to the MedReminder service.
3.2. Results from the Modified UCD Methods
In the focus groups and the personal interviews, we used the MedReminder prototype developed for an interactive TV environment. Two focus groups were organized. After each focus group, we had personal interviews with the participants. Nine participants took part in the first focus group and three of them took part in the second focus group. Eight out of nine participants in the first focus group were married couples, whereas the participants in the second focus group were older woman, living alone. We found out that the people who were living alone were more enthusiastic about the MedReminder service, since they could not use “living” reminders as easily as the married couples did. Besides that, no significant gender or educational differences were observed in the study.
Most of the participants found the MedReminder not to be complicated and to be really useful, especially for those who watch TV a lot. Eleven out of 12 participants reported they would like to use the MedReminder service in the future. Only one participant reported, “It (the MedReminder service) is just another unnecessary complication for everyday life”. The focus groups and the personal interviews revealed some of MedReminder’s disadvantages as well. Participants reported they had many problems when they were trying to set reminders for their medicine. However, when observing them as they were presenting their problems using the MedReminder service, we found they did not have problems with the service itself, but they were simply not fond of entering a lot of information in the system. Many study participants recommended that somebody else, for example, a physician, pharmacist or relative could set the medicine reminders on their behalf. They have suggested that setting the reminder in the doctor’s office, immediately after the medicine prescription, or from the pharmacy, would be proper solutions to the problem. Another great concern that the study participants reported during the focus groups is what happens when the TV is off or the MedReminder user is not near the TV (he or she is in another room, or even away from home). As a possible solution, we presented them our idea to connect MedReminder with a mobile or stationary phone. They liked our idea and further suggested that when the TV is off, a reminder SMS should be sent to a mobile phone and/or a stationary phone should start ringing.
At the end of the research study, the study participants filled out the SUS questionnaire. The result of the questionnaire is an easy-to-understand single-score ranging from zero (negative) to 100 (positive). The SUS single score that the MedReminder service obtained is 56.67 with standard deviation of 14.28. The lowest obtained SUS score in the user evaluation study was 35, whilst the highest SUS score was 85. In terms of adjective rating, according to the results obtained, the MedReminder service can be described as “OK” [
17]. This grade means the study participants evaluated MedReminder as acceptable; however, additional improvements are needed.
In the research study, we were particularly interested in the acceptance rate of new e-Health services among their intended users, in particular the acceptance rate of the MedReminder service among older adults. This is the main reason why we were especially looking for participants’ opinions about item 1 in the SUS questionnaire, which states: “I think that I would like to use this system frequently”. The results showed that seven participants out of 12 “strongly agree” or “agree” and only two participants “did not agree” with this statement, which confirms that most of the study participants would like to use the service more often. Additionally, study participants reported they believe that other people of their age would also like to use the application, especially if it is provided free of charge. Overall, the analysis of the results obtained from the conducted user-evaluation study showed that the MedReminder service has good potential for a high acceptance among its target population, i.e., older adults.
4. Conclusions
People of both genders and different ages frequently use ICTs for various purposes, particularly the internet. This includes health-related issues. Many academic and commercial studies have reported that e-Health is effective in terms of significant cost reductions, increased health service efficiency, increased technical quality and usability and increased user satisfaction. Being familiar with all the benefits of e-Health and the strategic plan for the Slovenian health sector’s informatization, Telekom Slovenia and the Faculty of Medicine from the University of Maribor, along with other partners, have initiated an e-Health project. The project group is developing various e-Health services that are based on modern ICT solutions and will be available on several screens, such as television, personal computer, smart-phone and tablet. In order to meet the users’ needs and expectations and consequently achieve the high acceptance of e-Health services, the UCD approach was practiced in the e-Health project.
This paper presented the UCD process for MedReminder, a telecare service developed as a part of the e-Health project and intended to remind people to take their medicines on time or to call a relative or a medical person in an emergency situation. Since it was assumed that MedReminder will be mostly used by adults older than 65, the UCD process for MedReminder was made from the perspective of older adults. Using a standard for the UCD approach and criteria for the UCD methods’ selection, four UCD methods were selected.
During the research, it was found that conventional UCD methods are not completely appropriate for older users. The reason for this is that older adults have different characteristics, backgrounds, environments and motivations than other groups of users. Because of that, the selected UCD methods in this study were modified and adapted for older adults, the MedReminder’s target population.
Using the results of the adapted UCD methods, a prototype for the MedReminder service was developed. The prototype was evaluated by a group of 12 study participants. These study participants evaluated the MedReminder service as acceptable with a good potential for a high adoption rate among its target population, i.e., older adults.
In the example of MedReminder, the research study revealed the older adults’ perceptions of the e-Health services and pointed out key aspects that increase the adoption rate of such services among the target population. The MedReminder study once more showed that people are the central and most important part of the creation and use of e-Health products and services. Sufficient user involvement in the design and creation of e-Health applications and services is one of the most important factors for e-Health project success. In addition to this, the research study showed that in order to get valuable results for their studies, instead of using conventional UCD methods, user researchers should modify the UCD methods and adapt them for their target population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}