3.1. Temperature and Humidity
The maximum daily temperature (TEMPMAX) for the entire study period ranged from −1.82 to 43.80 °C, with a mean of 22.80 °C, while the maximum apparent temperature ranged from 1.53 to 48.51 °C with a mean of 24.45 °C (the apparent temperature is a metric of how hot it feels to people when air temperature, wind, and relative humidity are considered [
29]). The distribution of the maximum temperature showed three modes, at around 17, 28, and 34 °C. The distribution of the maximum apparent temperature appeared to have two modes, at around 18 and 35 °C. The minimum daily temperature (TEMPMIN) for the entire study period ranged from −5 to 31.09 °C, with a mean value of 15.37 °C. The distribution of the minimum temperature had three modes (peaks), around 12, 18, and 26 °C, possibly corresponding to the prevailing weather conditions during the winter, the spring/summer, and the autumn months, respectively. The minimum apparent temperature ranged from −6.96 to 36.98 °C with a mean of 16.91 °C.
The minimum daily humidity (RELHUMIN) for the entire study period ranged from 8% to 91% with a mean of 47.14%, while the maximum humidity (RELHUMAX) ranged from 32% to 101% with a mean of 77.16%. While the minimum humidity followed a symmetric (nearly normal) distribution within its range of values, the maximum humidity displayed a strong negative skewness, with many values in the range of 80%–90%. It is noted that humidity is considered in the calculation of the apparent temperature.
The variation of average minimum and maximum values of temperature and humidity per month confirmed the expected seasonal variability, with higher temperature and lower humidity values during the summer months.
Finally, using the definition of heatwaves mentioned in the materials and methods section, 2012, 2007, and 2010 were the years with the highest number of heatwaves (20, 10, and 8, respectively), while 2003 (the year of the European heatwave) was only characterized by two short heatwaves in Greece. Of the other years of the sample, 2005 and 2006 had four heatwaves; 2004, 2009, and 2011 had one heatwave; and 2002 and 2008 had zero heatwaves.
3.2. Mortality
Following the examination of temperature and humidity, attention now shifts to the fatalities that occurred in the municipality of Athens during the period considered in this research (2002–2012). The number of deaths (mortality count) rather than the proportion of deaths in the population (mortality rate) was analyzed; the concept of excess mortality is discussed in the discussion section.
In the years 2002 to 2012, a total of 89,658 fatalities occurred due to various causes. Of these, 51.4% were female and 48.6% were male. The mean age of death from all causes was 75.6 years (72.2 for males; 78.7 for females). The distribution of total fatalities per month of the year confirmed a connection to temperature extremes: the highest mortality counts occurred in the months of December to March and July to August. Regarding the day of the week, there was a slight variation, with more fatalities occurring on Monday and fewer during the weekend (Saturday and Sunday).
A closer examination of the cause of death, shown in
Table 1, shows that cardiovascular disease, cancers, and respiratory diseases were the most frequent cause of death, jointly responsible for almost eight out of 10 deaths (78.3%) for the duration of the research.
The breakdown of fatalities by year and cause (not shown) did not reveal any significant annual changes in the distribution of deaths among the different causes for the period under study. The distribution of fatalities from different causes per month (also not shown) confirms the correlation between cardiovascular and respiratory deaths and the time of year (more in the coldest winter and hottest summer months).
The rest of this research now focuses on the deaths of individuals over 65 years of age that were due to cardiovascular and respiratory causes; these have been examined in the epidemiological research literature (e.g., [
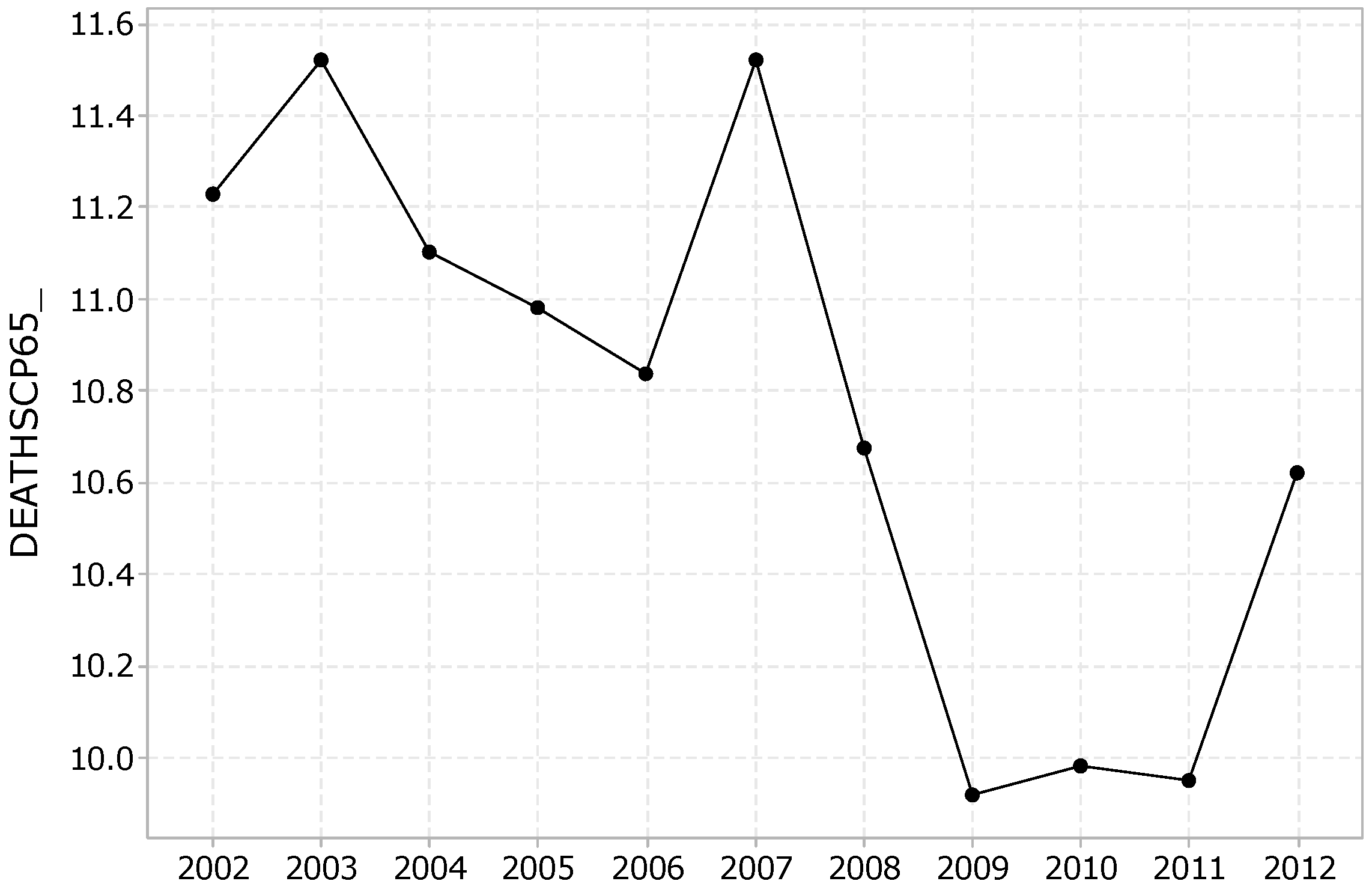
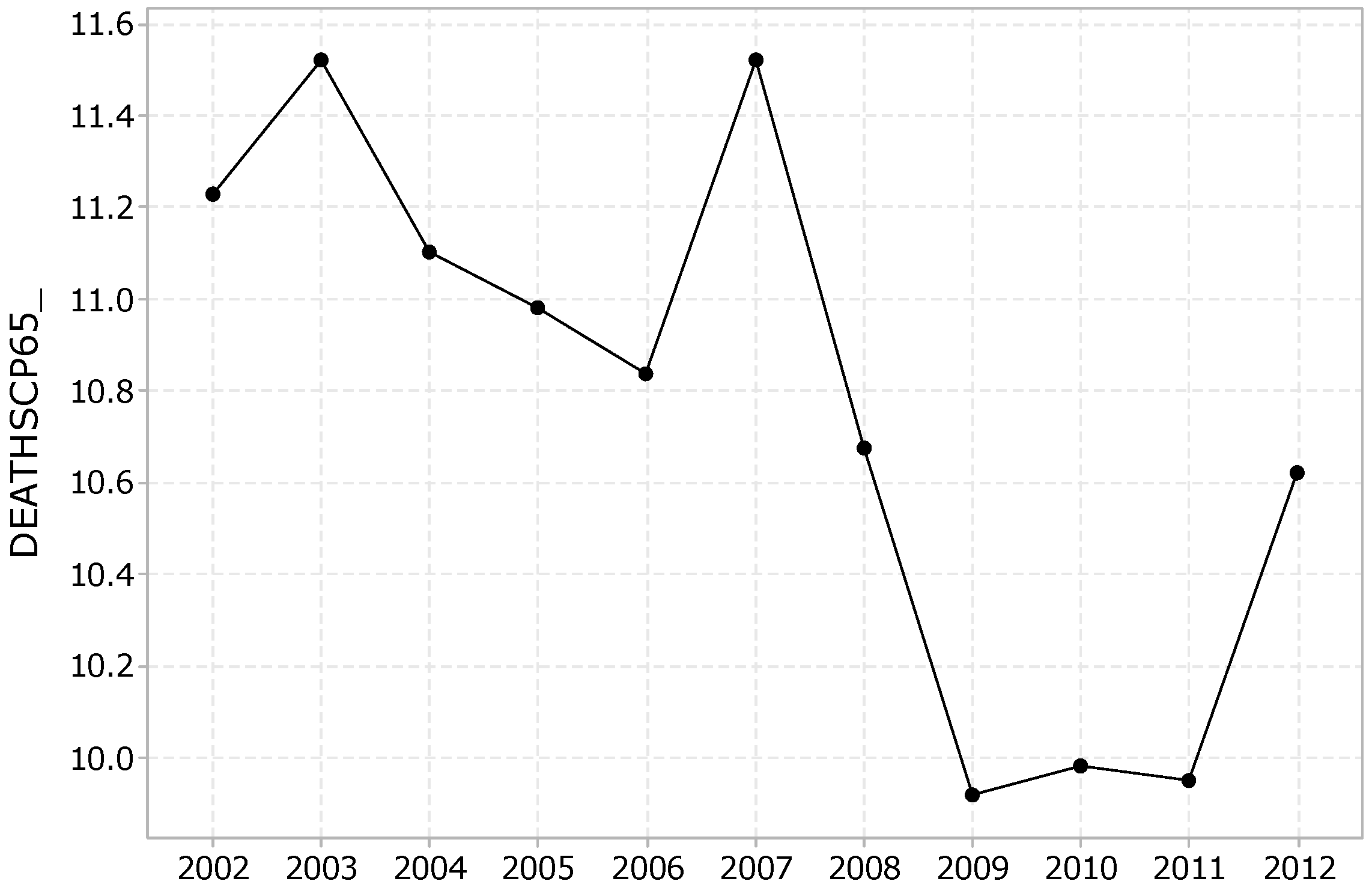
27]) as potentially attributed to temperature extremes. The total number of such fatalities was 4018 out of a total of 89,658 (4.5%). The daily average number of such deaths was equal to 10.761, with a minimum of one and a maximum of 33 deaths. The distribution of cardiovascular and respiratory fatalities of individuals over 65 years per day (i.e., the daily mortality count), follows a relatively symmetric distribution with a slight positive skew. Regarding the average annual variation of cardiovascular and respiratory fatalities of people over 65 years of age, as shown in
Figure 1, it is observed that such fatalities were exacerbated in 2003, the year of a pan-European heatwave [
16] and 2007, and appeared to have a minimum in the years 2009, 2010, and 2011.
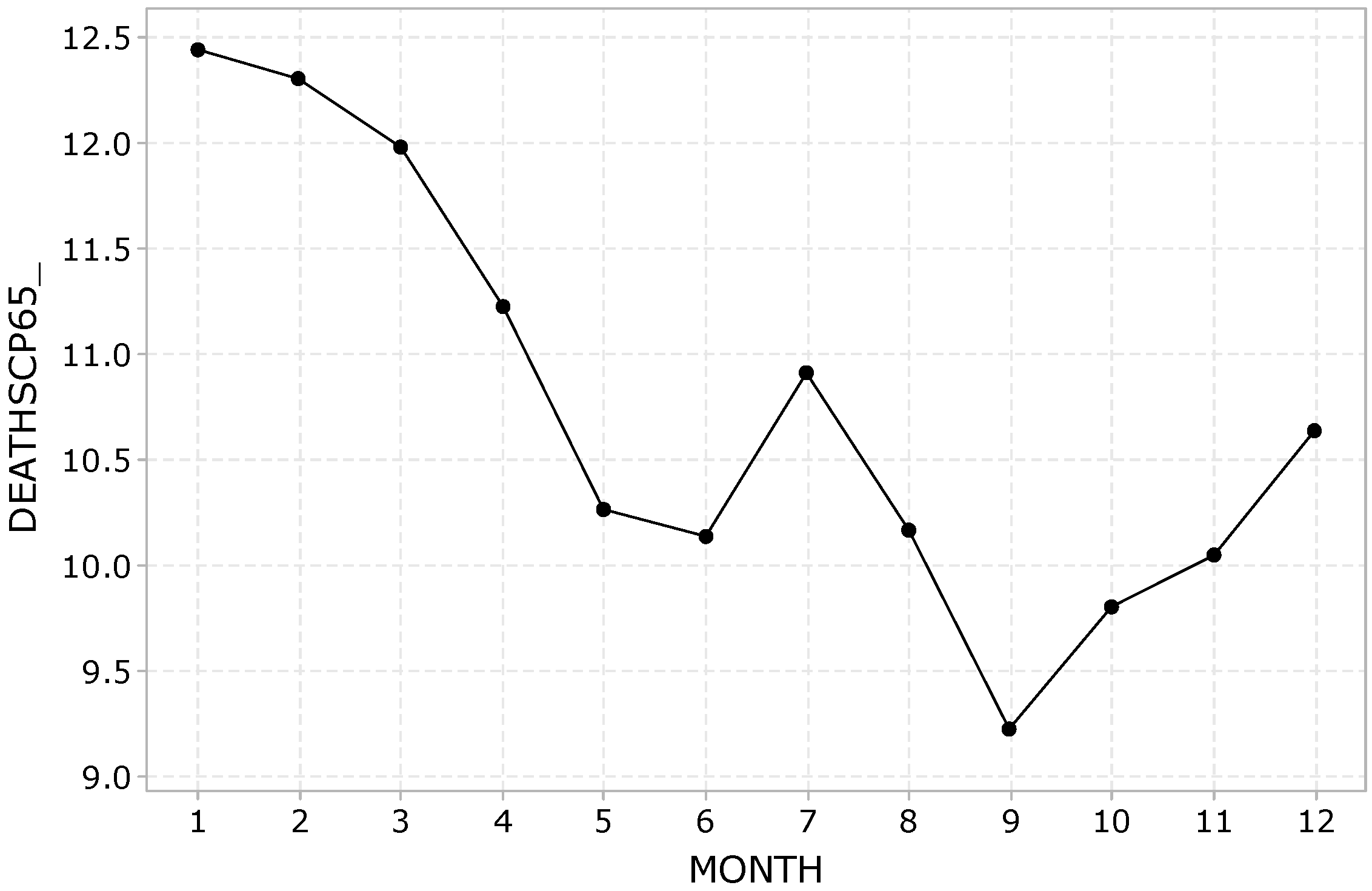
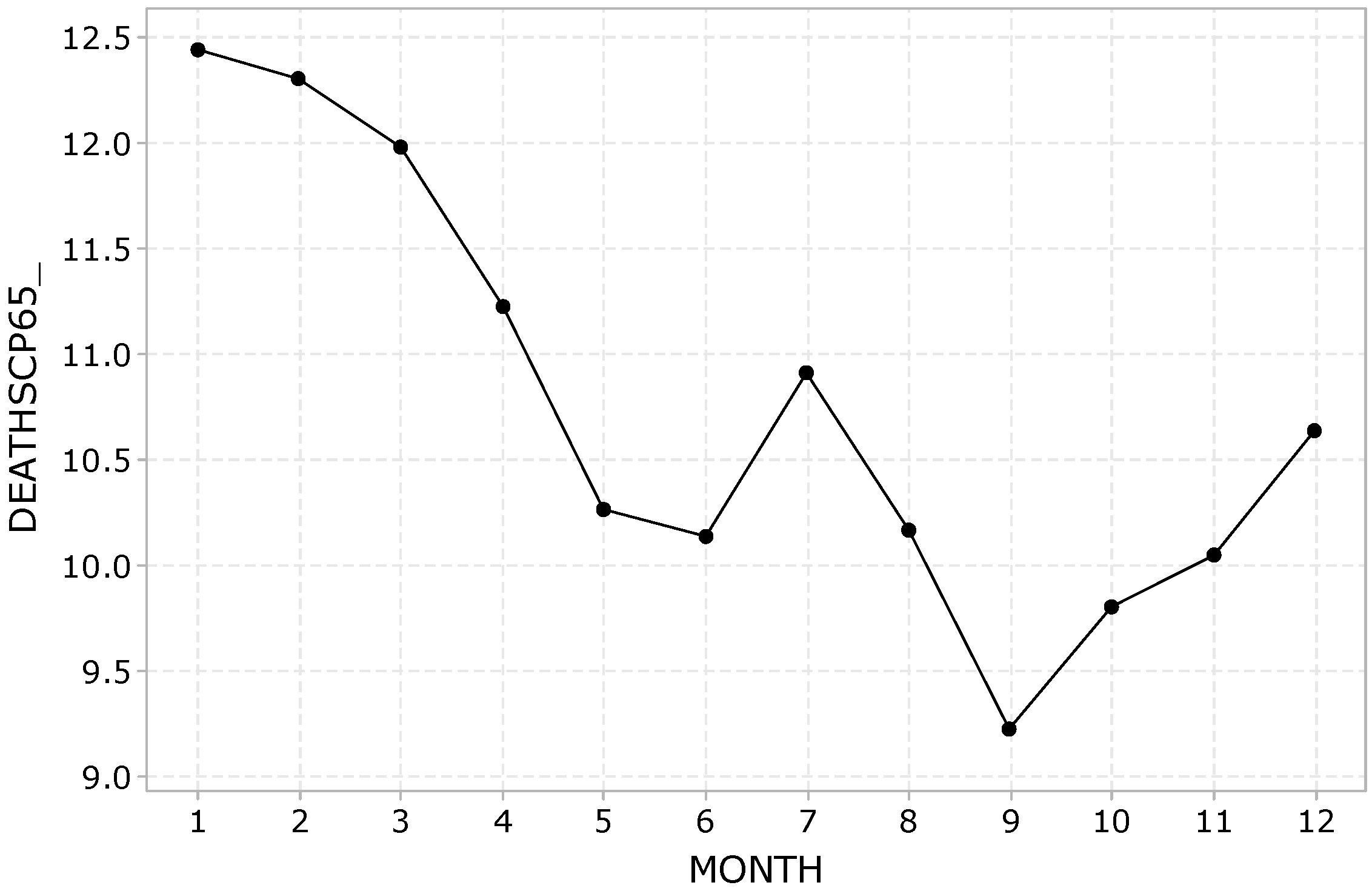
Regarding the average monthly variation of cardiovascular and respiratory deaths of people over 65 years of age, as shown in
Figure 2, these showed an upsurge in the winter months, a decline during the spring and the autumn, and a smaller peak in the middle of summer, with the lowest value occurring in September.
Of particular interest in the literature is the correlation of the daily number of cardiovascular and respiratory deaths of individuals over 65 years of age, to the daily maximum (apparent) temperature. The functional form of some such exposure response curves, fit as quadratic equations via ordinary least squares, are shown in Equations (1)–(4).
Equations (1) and (2) show the functional form of the association between the daily mortality count of cardiovascular and respiratory deaths of individuals over 65 years of age and maximum temperature, in both raw and logarithmic form.
where DEATHSCP65_ is the daily fatality count below 65 years of age attributed to cardiovascular or respiratory causes, and TEMPMAX is the daily maximum temperature (measured in °C).
Equations (3) and (4) show the functional form of the association between the daily mortality count of cardiovascular and respiratory deaths of individuals over 65 years of age and maximum apparent temperature, also in both raw and logarithmic form:
where DEATHSCP65_ is the daily fatality count below 65 years of age attributed to cardiovascular or respiratory causes, and APPTEMPMAX is the daily maximum apparent temperature (measured in °C).
The maximum temperature is regarded as the most representative [
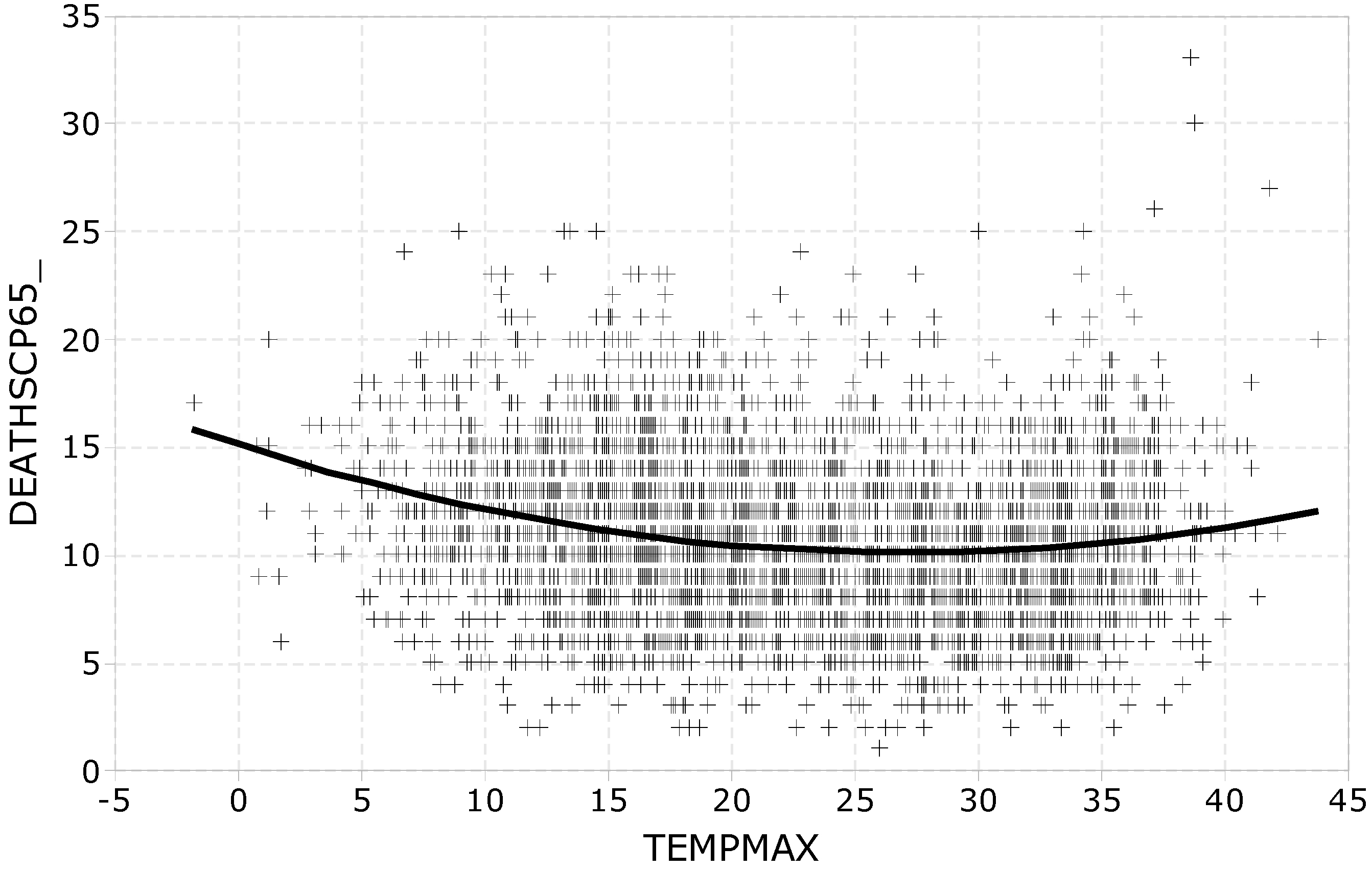
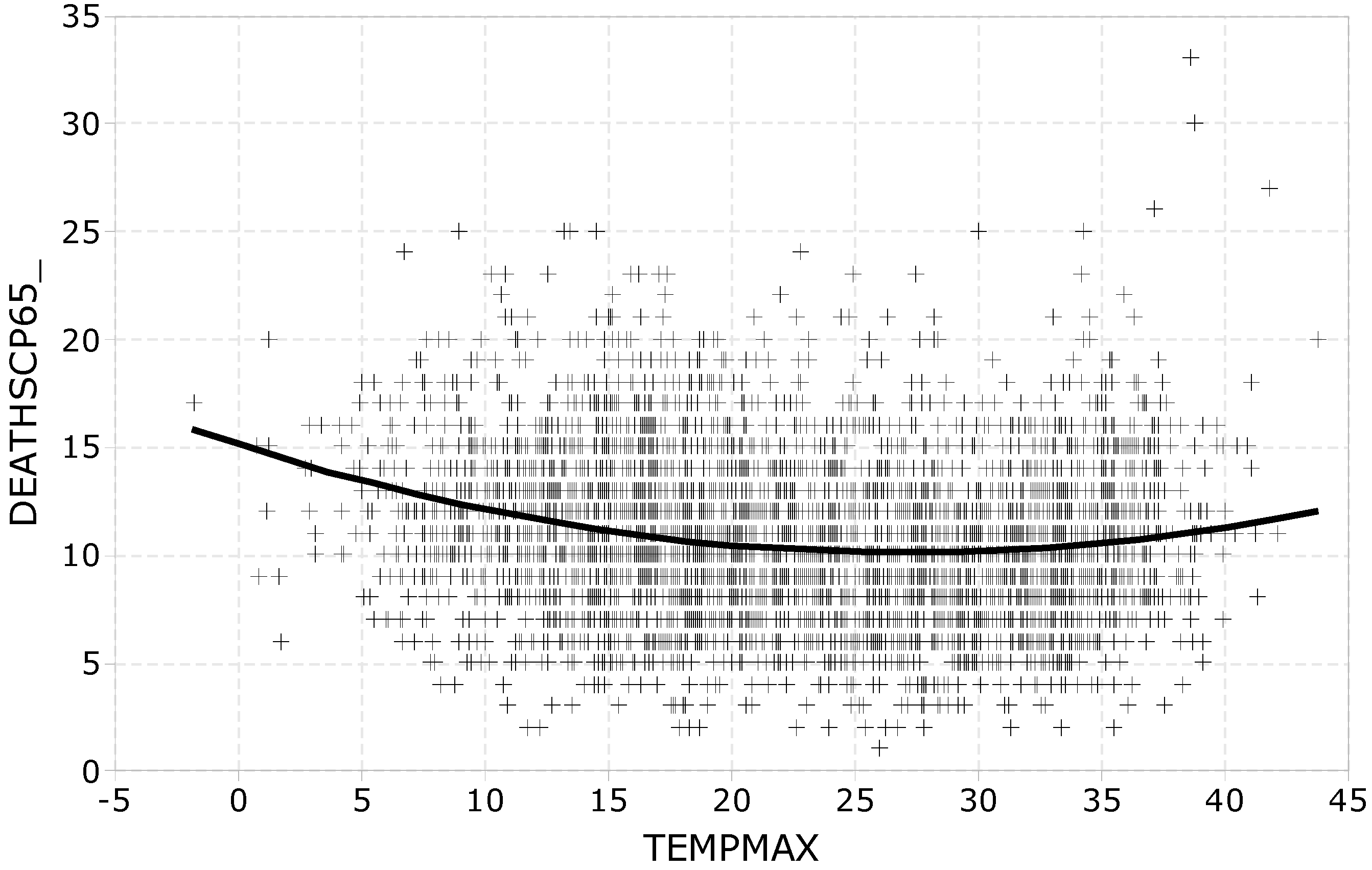
30]. As an illustration of the functional form of the above equations,
Figure 3 depicts a scatter plot of the mortality count per month as a function of the average maximum temperature values for the years 2002–2012.
Equations (1)–(4), along with the illustrative
Figure 3, confirm the U-shaped functional form of such relationships that has been reported in the literature [
22,
30]: fatalities are lowest around maximum temperature values of 20–30 °C and increase below and above these values. It may be observed that the highest daily mortality counts are positioned in the top right corner of the graph, between 35 and 40 °C; more on this in the section presenting the cluster analysis of the sample data.
The statistical significance of the increased occurrence of cardiovascular and respiratory fatalities of people over 65 years of age, in days of temperature extremes, is examined next. As mentioned previously, the analysis considers absolute rather than apparent temperature values because their association with such deaths was more pronounced.
Table 2 compares the mean number of fatalities of people over 65 years of age, in days that were characterized by temperature extremes to the number of similar fatalities in other days. The statistical significance of the difference between fatalities, as described above, is tested by appropriate one-sided
t-tests for independent samples, following an examination of the equal standard deviations assumption by Levene’s test. The first four rows in
Table 2 consider days with extreme values of the minimum temperature (TEMPMIN); the next four examine days with extreme values of the maximum temperature (TEMPMAX); and the last two combine extreme temperature criteria, so that steadily cold (TEMPMIN ≤ 5 and TEMPMAX ≤ 10) and steadily hot (TEMPMIN ≥ 25 and TEMPMAX ≥ 35) days are examined.
As far as days with extreme minimum temperatures are concerned, no reliable conclusions may be drawn regarding the average number of deaths in days that had a minimum temperature above 30 degrees (TEMPMIN ≥ 30) because the total number of such days was very small (six out of a total of 4018). On days that had a minimum temperature below zero degrees (TEMPMIN ≤ 0), the average number of deaths was 12.85, which is 19.5% higher than the average number of deaths in the remaining days (10.75), with this difference being statistically significant at a 99% confidence level (t = 2.50, p = 0.006). The average number of deaths on days with a minimum temperature below 5 degrees (TEMPMIN ≤ 5) was equal to 12.53, which is 19.5% greater than the average number of deaths in the remaining days (10.65), a difference with a very high statistical significance (t = 7.73, p = 0.000). Finally, the average number of deaths on days with a minimum temperature above 25 degrees (TEMPMIN ≥ 25) is equal to 11.55, which is 8.1% greater than the average number of deaths in the remaining days (10.68), a difference that is also statistically very significant (t = 4.36, p = 0.000).
Turning our attention to the values of the maximum temperature, it is observed that fatalities were increased on days when the maximum temperature was above 35 °C (11.69 compared to 10.69 on other days), with the significance being very high in all cases (p = 0.000). On the 12 days when the maximum temperature exceeded 40 degrees, the largest increase in mean deaths was noted: 14.42 versus 10.75 on the remaining days.
The last two rows of
Table 2 concern steadily cold (TEMPMIN ≤ 5 and TEMPMAX ≤ 10) or steadily hot (TEMPMIN ≥ 25 and TEMPMAX ≥ 35) days, where again there was an increase in cardiovascular and respiratory mortality of people over 65 years old, at a confidence level greater than or equal to 99.9%.
3.3. Time Series Analyses
In this section, the statistical analysis that took into consideration the temporal nature of the daily cardiovascular and respiratory mortality of people over 65 years of age (DEATHSCP65_) is presented.
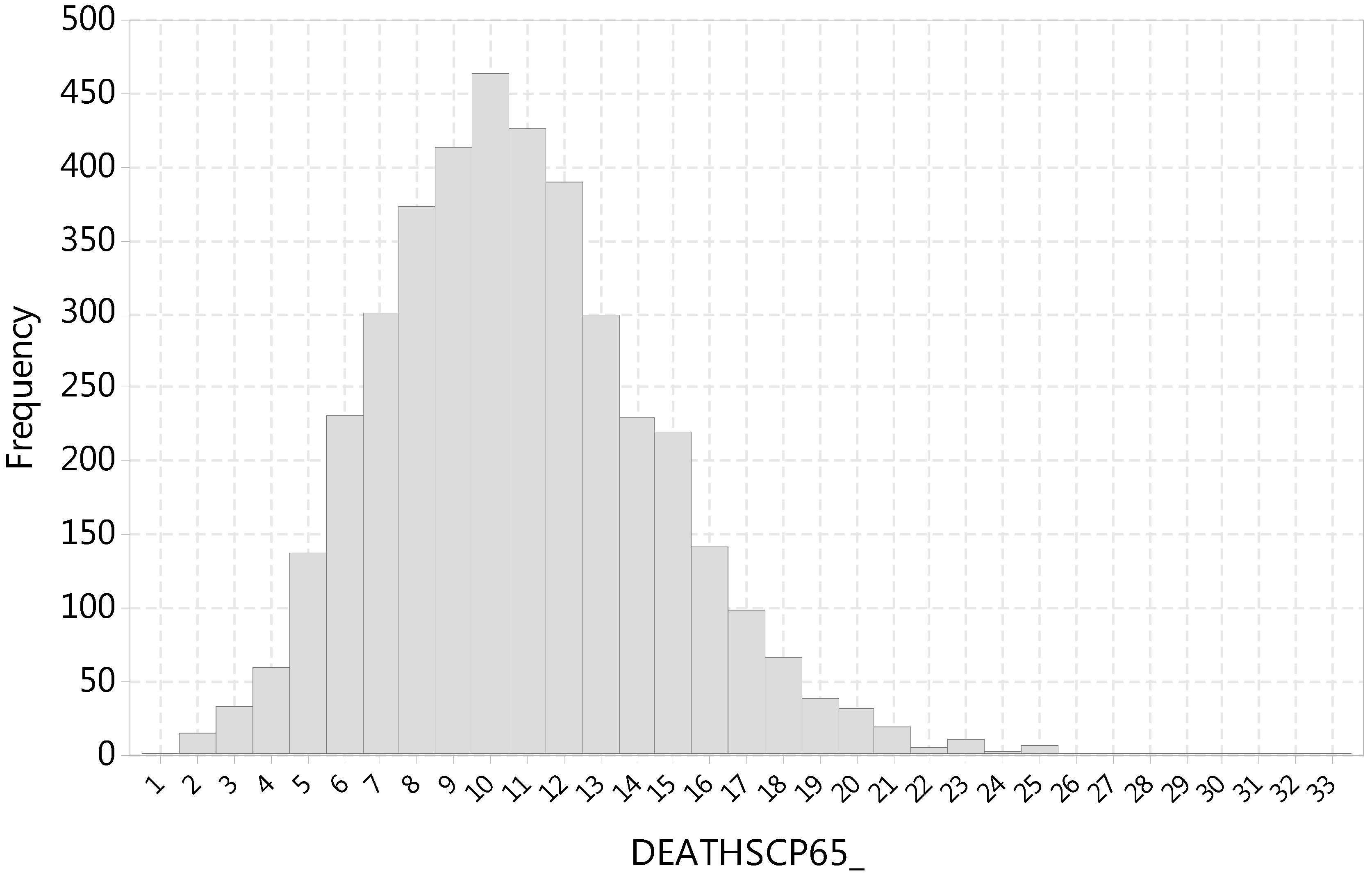
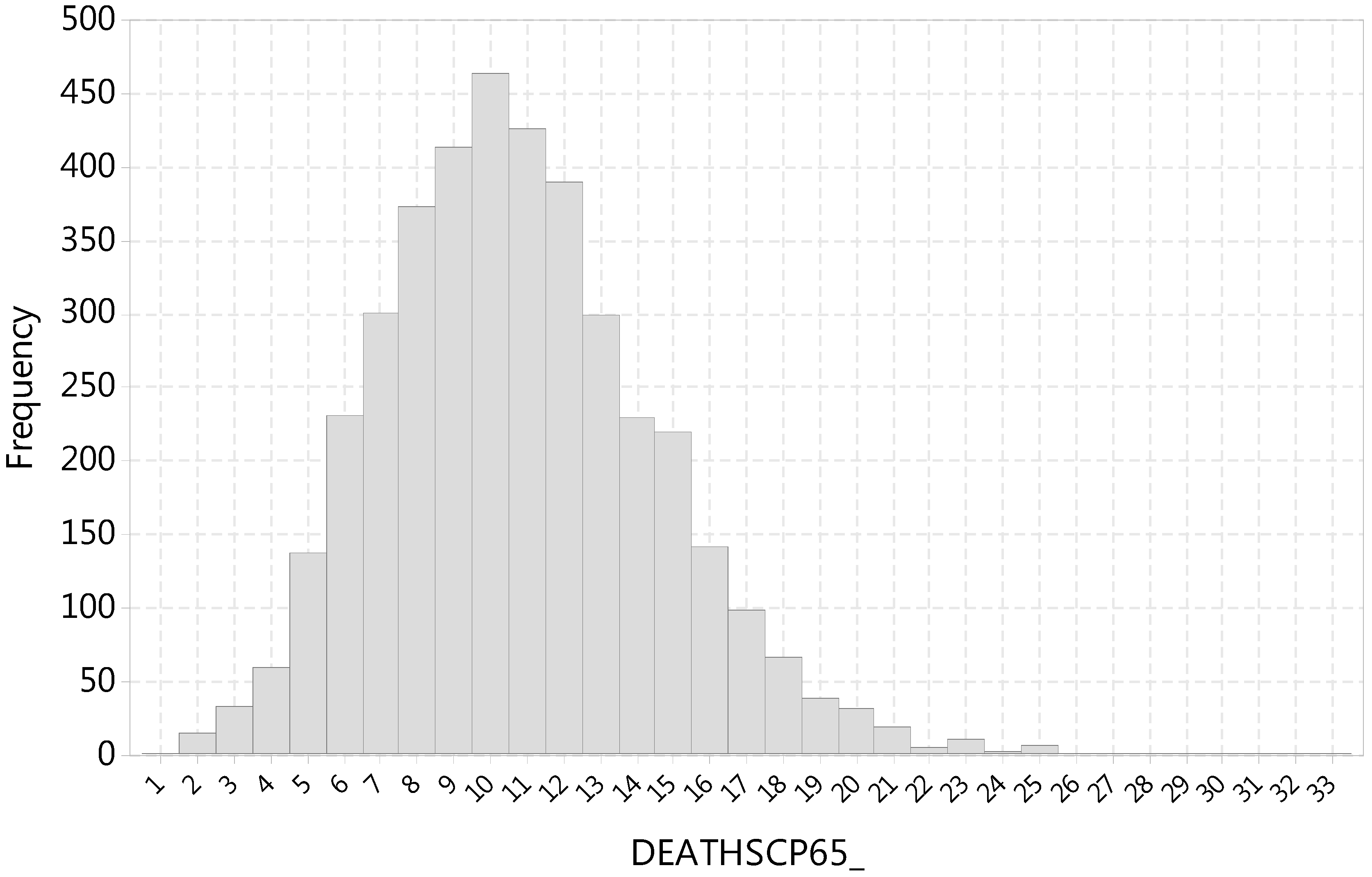
Considering the entire population of people over 65 years of age in Athens, DEATHSCP65_ is a rare event that takes positive integer values ranging from one to 33. As shown by the histogram of discrete values in
Figure 4, the distribution of DEATHSCP65_ is characterized by some positive skewness. Therefore, DEATHSCP65_ should be analyzed with statistical modeling techniques appropriate for count data [
40].
While count variables should be modeled based on the Poisson or negative binomial distribution [
41], the histogram in
Figure 4 shows that the daily mortality values are large enough for their distribution to approximate the normal distribution (although some positive skewness remains). Given that the Central Limit Theorem (CLT) states that, as the sample size increases, the sampling distribution of the mean (as in the case of regression coefficients) becomes normally distributed regardless of the shape of the original distribution of the sample [
42], ordinary least Squares (OLS) could probably be used, although at some risk of being unable to detect true effects [
43]. Compared to an OLS model, a distinct advantage of resorting to a Poisson or negative binomial regression would be that negative numbers would be precluded. In any case, several alternative statistical models are presented in this research.
The Poisson distribution is restricted to have the same parameter for both the mean and the variance of the count process that it models. This restriction relates to the concept of overdispersion if the Poisson distribution is used to model count processes that have a variance that is (significantly) larger than their mean (not difficult to achieve given that the variance is the square of the standard deviation). Compared to the Poisson distribution, the negative binomial distribution has separate parameters for the mean and the variance, allowing for overdispersion as well as a bigger number of zero counts [
44]. In the case of DEATHSCP65_, there are no zero mortality counts; furthermore, the overall mean of the mortality daily count time series equals 10.761, with the overall variance equaling 14.039. Broken down by year, the annual mean of DEATHSCP65_ varies from 9.923 to 11.526, with the annual variance varying from 10.978 to 16.239. One of the reasons that the values of the means are approximately equal to the values of the variances is that there are no excess zero values in the daily mortality counts. It may be argued that overdispersion does not constitute a significant problem in this analysis, especially considering that the introduction of covariates (i.e., independent variables in the regression models) implies that the equality of the mean and the variance is conditional on the values of these covariates. In any case, both Poisson and negative binomial regression models were estimated in this research.
An important question in the regression of time series data is how to deal with variables that are nonstationary. A time series plot of DEATHSCP65_ (not shown) lacks any trending and wandering, but is characterized by seasonality, with most fatalities occurring in cold and hot weather. Autocorrelation function (ACF) plots (not shown) display a significant amount of positive serial correlation, with strong seasonality becoming apparent when the plots are extended into many lags. Taking the first differences of these daily mortality counts to stationarize the time series renders a series with an ACF plot (not shown) that has a highly negative AFC in the first lag and insignificant ACF values in the next lags. This is an indication of overcompensating for nonstationarity and, possibly, not in the proper way, e.g., the series could be trend stationary, in which case the proper way to stationarize it would be to subtract the trend rather than take differences. In this research, addressing nonstationarity in modeling followed the methodology of Katsouyianni et al. [
45], who argued that the objective of any transformation of daily mortality counts should be to make any structures (related to trend, seasonality, and interventions) invisible in the residual plots of the fitted models, so that the final residual plots reflect only white noise.
The estimated models are shown in
Table 3. The maximum likelihood method used to estimate the Poisson and negative binomial regression models requires a large sample, a stipulation satisfied in the case of this research (4017 observations with no missing data). All models were estimated with robust standard errors. The dependent variable in all models was the natural logarithm of the daily mortality counts, a transformation feasible since DEATHSCP65_ had no zero values. There was no need to estimate zero-truncated models because, although there were no zero fatalities in DEATHSCP65_, the number zero would be an acceptable value.
Resorting to cross-correlation values between mortality counts and lags of temperature or humidity to assess the delay at which the effect of these covariates on mortality is maximum [
46] was not particularly helpful because these were (a) greatly influenced by seasonality and (b) unclear when the seasonality was removed, e.g., by subtracting a 30-day moving average of the mortality counts. So, lags of up to 12 days were tried, as these have been reported to represent a central value in a broad range of lags attempted in the literature [
47]. Of these, only the first lag of temperature had a meaningful statistically significant coefficient and was kept in the final model formulations. The regression models presented in
Table 3 do not include the square of the maximum temperature, which was included in the quadratic exposure response function presented previously [
48] because its inclusion failed to render meaningful statistical coefficients for temperature and did not improve the fit.
To account for the year-to-year changes in mortality patterns (i.e., the long-term trend), two alternative formulations were tried in the models: (a) dummy variables for each year (2002–2012), or (b) a linear or a quadratic time trend [
48]. Not accounting for a long-term trend at all gave models that fit the data poorly, especially after 2008. Of the two alternative formulations (dummy variables versus trend), it was decided that the yearly dummy variables would be maintained as they rendered a marginally better fit and were easier to interpret meaningfully. Seasonality was accounted for by including indicator (dummy) variables for each month (except December, to avoid perfect multicollinearity). Dummy variables were also included for each day of the week (except Sunday); alternative models including weekend dummies were also tried but were found to be inferior. The potential interaction between year and season was not accounted for because including year and month interaction terms for all 11 years of the sample would be too complex for the scheme to be useful. Finally, an attempt to account for temperature–humidity interactions [
48] also failed to improve any of the models.
Regarding overdispersion, although a likelihood-ratio test showed that the negative binomial regression model was more appropriate than the Poisson one,
Table 3 shows that, in fact, these two models are very similar.
Comparing the overall fit of the three models, it is observed that all information criteria (Akaike, Swartz, and Hannan–Quinn) concurred that the OLS model is superior to both the Poisson and the Negative Binomial model. Although the R-squared values are not comparable among the models (i.e., McFadden in Poisson and pseudo R-square in Negative Binomial), they show clearly that all three models fit the data very poorly. Plots of fitted vs. observed and residual values over time (not shown) showed that non-stationarity had been removed, but they also confirmed that the models fit the data poorly.
A few remarks may be made, keeping in mind the very poor fit of the models:
The yearly dummies that were added to account for the existence of a time trend showed that daily mortality counts appeared to decrease over time, especially after 2008 (with the corresponding negative coefficients being statistically significant, at a 5% or 10% level, in the Poisson and the negative binomial models).
Regarding the day of the week, it should be kept in mind that the day of the week coefficients compared the effect of the corresponding day of the week to Sunday, which was the day for which no dummy was included in the models. Mondays appeared to have a statistically significant aggravating effect on mortality in all models, with no other days of the week being associated with increased or decreased mortality in a statistically significant way.
The monthly dummy variables compared the effect of the months to December, which was the month for which no dummy was included in the models. Thus, it was shown that the cold months aggravated mortality while the summer months alleviated it (more on the effect of temperature later), with January being the worst and September being the best months, mortality-wise.
While the maximum temperature (of the day the fatality occurred) did not appear to have a significant effect on mortality, the maximum temperature lagged by one day had a significant aggravating effect on mortality, in all models. This shows that it takes one day for the temperature to have a drastic effect on the cardiovascular and respiratory health of people over 65 years of age, a fact that sheds more light on the literature findings cited previously [
47]. Unfortunately, the very poor fit of all the models adds ambiguity to this finding. The number of heatwave days also had a clear, statistically significant effect on mortality, showing that, as a heatwave is prolonged, it is associated with increased mortality.
Turning to humidity, one sees that the maximum humidity has a negative effect on mortality that is statistically significant (at an 18% confidence level or less). Apparently, there are low-humidity days that are characterized by high cardiovascular and respiratory health issues of people over 65 years of age. More on this association will be presented in the cluster analysis results, presented in the next section.
It is worth mentioning that air pollutant (ozone, sulfur dioxide, and nitrogen dioxide) concentrations were employed as independent variables but were found to have statistically insignificant coefficients and were, thus, excluded from the models; particulate concentrations, which (as mentioned previously) were available only for a few years towards the end of the study period, were characterized by great gaps of missing data, and thus were of no use in time series analysis.
To recap the findings of the time series models, mortality appeared to fall after 2008, a result possibly pointing to a better level of preparedness of the state and society in Greece. In addition, it was found that the effect of temperature was most significant at a lag of one day. Nevertheless, it was concluded that a time series approach had mediocre success in discovering associations in the mortality counts of Athens and it was decided that an alternative multivariate analysis approach would be attempted in the next section. To the knowledge of the authors, such an approach has not been tried before in temperature–mortality research.
3.4. Cluster Analysis
Following the estimation of time series models of the cardiovascular and respiratory mortality of people over 65 years of age, an attempt is made now to discover meaningful associations between mortality, temperature, and humidity by carrying out a cluster analysis. It was decided to limit the analysis on the months of May to September to analyze the effect of high temperatures. The usage of cluster analysis constitutes a rather novel approach in the mortality–temperature literature.
Estimates regarding the number of clusters, based in part on the multimodal shape of the distribution of temperatures, had indicated the presence of three or more (some possible small) clusters [
49]. On the issue of sample size, Formann [
50], as cited by Mooi and Sarstedt [
51] (p. 243), recommends a sample of at least 2
m cases, where m equals the number of clustering variables. These recommendations imply that a sample size of 1678 observations with no missing data (which was left for clustering, as shown in
Table 4) could support up to 10 variables (2
10 = 1024 while 2
11 = 2048).
To arrive at a relatively robust clustering scheme, Ward’s method, with the squared Euclidean distance being the recommended distance metric [
52], was run to estimate and compare three-, four-, five-, and six-cluster solutions that were suggested by the dendrogram (not shown). Of these, the five- and six-cluster solutions were particularly appealing because they classified heatwave days into their own cluster. A two-step cluster analysis (effective with large datasets [
51]), which was run (with SPSS) to determine the final number of clusters and membership scheme, rendered the six-cluster solution optimal. This was chosen as the final clustering scheme and is tabulated in
Table 4, which shows the centroid values of variables used in the cluster analysis. To facilitate interpretation, the clusters were numbered in order of increasing mortality.
Table 5 shows the centroid or percentage values of the variables that were not used in the cluster analysis.
To confirm the significance of the selected clustering scheme, it is not enough to consider the high significance of ANOVA or Welch tests, shown in
Table 4 and
Table 5: this was expected because of the large sample size. Therefore, a multiple discriminant analysis was run on the clustering variables of
Table 5, which employed five canonical discriminant functions (with eigenvalues of 4.756, 1.657, 1.172, 0.359, and 0.038) and cumulatively accounted for 100% of the variance. Prior probabilities were not adjusted for group size, so as not to bias the classification results with a priori knowledge of cluster sizes. The classification results (confusion matrix) of the multiple discriminant analysis are (is) shown in
Table 6.
The membership in Clusters 1 to 6 was classified correctly in 89.2, 96.1, 92.4, 97.4, 64.7, and 97.8% of the cases. Of these, the membership in Cluster 5 (the heatwave cluster, as explained below) was classified correctly in 64.7% of the cases, with the rest 31.4% misclassified into Cluster 6 (the cluster with the highest mortality counts, a cluster similar to Cluster 5 yet distinct in an important way, as will be discussed below) and 3.9% into Cluster 2. The overall clustering scheme is deemed satisfactory since 93.8% of the total cases were classified into the correct cluster.
Having validated the clustering scheme, attention now turns to the description of the six clusters.
Cluster 1 had the lowest mortality, 7.77 daily fatalities of people over 65 due to cardiovascular and respiratory causes. The minimum and maximum temperature centroids were equal to 23.64 and 32.94 °C respectively, with their apparent values equal to 26.35 and 34.01 °C, respectively, certainly not the lowest among the clusters. The minimum and maximum relative humidity were equal to 29.42% and 60.9%, respectively, among the lowest in the clusters. The cases of this cluster were dispersed in August, July, and June, mostly, with fewer cases being in September and fewest in May.
Cluster 2 was also a cluster of low mortality, with 8.15 daily fatalities. Centroid minimum and maximum temperatures equaled 18.54 and 26.07 °C, respectively (or 22.99–30.28 °C in apparent values), among the lowest in the clusters. The minimum and maximum relative humidity were equal to 53.09% and 85.32%, respectively, the highest among all the clusters. Almost half of the cases of this cluster were in September, with about one-third in May, almost one-fifth in June, and very few in July and August.
The mortality centroid jumped to 10.66 in Cluster 3, which had minimum and maximum temperatures equal to 17.82 and 26.68 °C, respectively (with 19.99 and 27.99 °C being the apparent values). The minimum and maximum relative humidity were equal to 36.83% and 71.75%, respectively. Over half of the cases of this cluster were in May, with about one-fifth in September and June; July and August contained very few cases belonging to this cluster.
Cluster 4 had a centroid daily mortality equal to 11.02, and minimum and maximum centroid temperatures equal to 23.72 and 32.88 °C respectively (and apparent values equal to 29.24 and 37.9 °C). The minimum and maximum relative humidity were high, equal to 44.81% and 77.46%, respectively. This cluster contained cases mostly from August and July, with fewer from September and June, and very few from May.
Cluster 5 was the heatwave cluster, with a centroid value of 2.745 heatwave days. Its mortality at the centroid was equal to 12.98, which was the second highest among all six clusters. The heatwave cluster had the second highest minimum and maximum centroid temperatures, equal to 28.25 to 38.57 °C, respectively (apparent values equal to 30.86 and 39.49 °C). The minimum and maximum relative humidity were the smallest among the six clusters, equal to 25.14% and 52.37% respectively. Over 90% of the cases in this cluster fell in the months of July and August, with a few cases in June and almost none in May and September.
Finally, Cluster 6 had the highest centroid mortality (13.24), yet it was characterized by the second highest centroid minimum and maximum temperatures, equal to 25.35 and 34.82 °C, respectively (with 27.73 and 35.44 °C being their apparent values), which was rather surprising. Like Cluster 5, Cluster 6 was also characterized by low values of the minimum and maximum relative humidity (26.29% and 54.05%, respectively). Finally, Cluster 6 contained cases from July, August and July, with fewer cases from September and May.
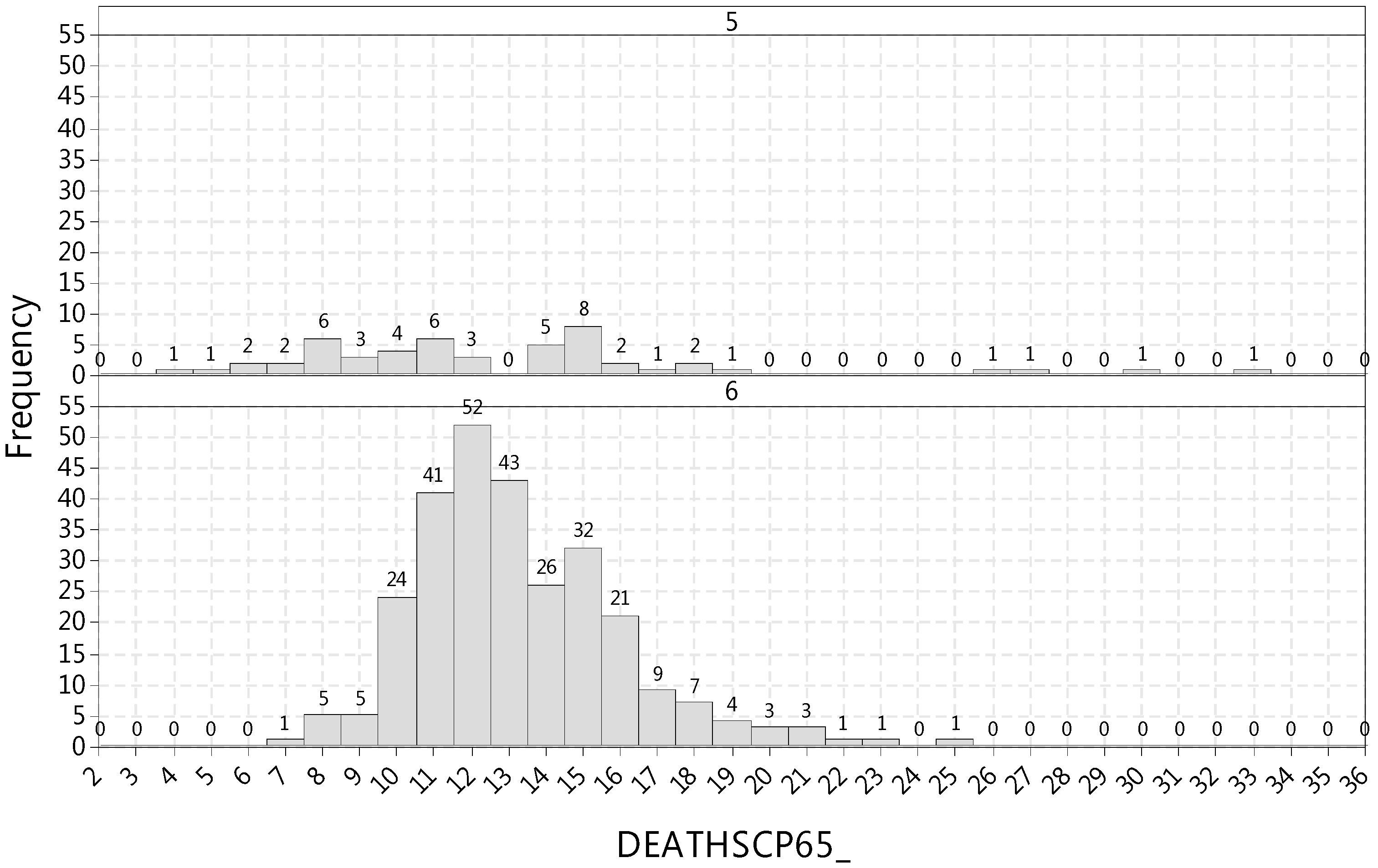
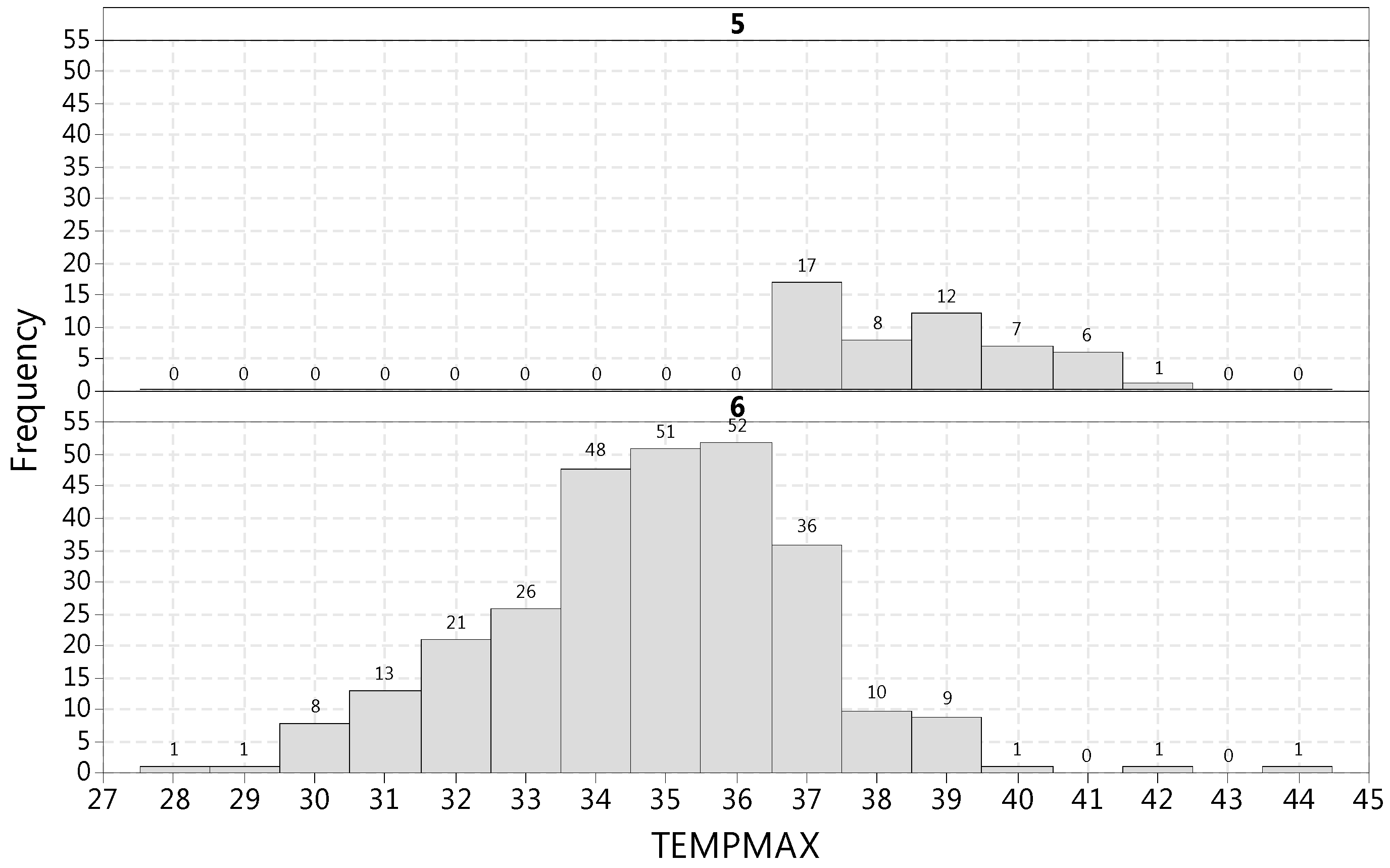
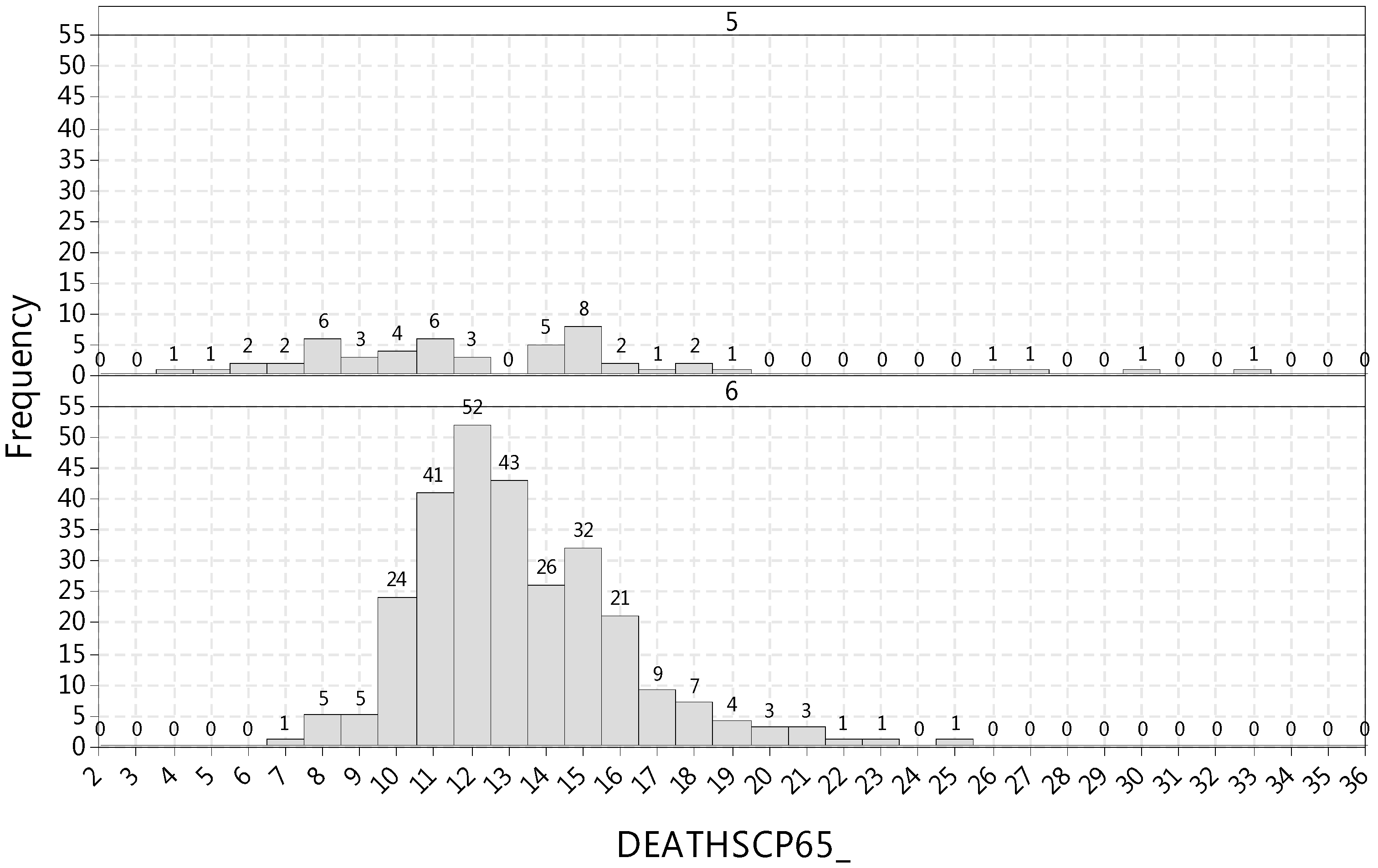
The apparent discrepancy between temperature and mortality of clusters 5 and 6 was investigated further with the aid of the histograms displayed in
Figure 5 and
Figure 6. Cluster 5 contained cases with the maximum temperature ranging from 36.5 to 41.8 °C (top panel of
Figure 5) and the mortality varying from four to 33 daily fatalities (top panel of
Figure 6). Cluster 6 contained cases with the maximum temperature ranging from 28.4 to 43.8 °C (bottom panel of
Figure 5), with the mortality varying from seven to 25 daily fatalities (bottom panel of
Figure 6). Yet, as shown in
Figure 6, the mortality of Cluster 5 was essentially distributed from 4 to 19, with four distant observations raising the maximum value to 33. While Cluster 6 contained a few unusually hot days (that were not part of a heatwave), the highest maximum temperature day (43.8 °C) being one of them (bottom panel of
Figure 5), it was not these very few outlying observations that caused the higher centroid mortality of Cluster 6, but mostly the fact that the entire distribution of mortality of Cluster 6 was shifted to the right (i.e., towards higher fatality values) compared to Cluster 5 (
Figure 6).
Neither the weekend nor the weekday indicator variables contributed in a significant or meaningful way to discerning any differences among the clusters. Finally, air pollutant concentrations were not found to contribute meaningfully in any clustering scheme, while particulate concentrations (being available for a few years only and with many missing values) were excluded from the analysis because they would greatly reduce the sample size.
The approach of cluster analysis overcame the problem of analyzing discontinuous observations, i.e., May to September only. The findings shed light on the interaction of temperature and mortality. The mortality of Cluster 5 (the heatwave cluster) is important because heatwaves exacerbate the UHI [
10], yet the existence of Cluster 6 showed that older people perhaps get acclimated and develop better responses to conditions prevalent in heatwaves, thus running a smaller risk of suffering adverse health effects compared to isolated days of very high temperature.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}