Vitamin E (α- and γ-Tocopherol) Levels in the Community: Distribution, Clinical and Biochemical Correlates, and Association with Dietary Patterns

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Sample and Design
2.2. Clinical Examination and Definitions
2.3. Assessment of Dietary Variables
2.4. Laboratory Analyses
2.5. Statistical Analyses
2.6. Correlates of Circulating Vitamin E Biomarkers
2.7. Dietary Pattern Analyses
3. Results
3.1. Correlates of Vitamin E Biomarkers
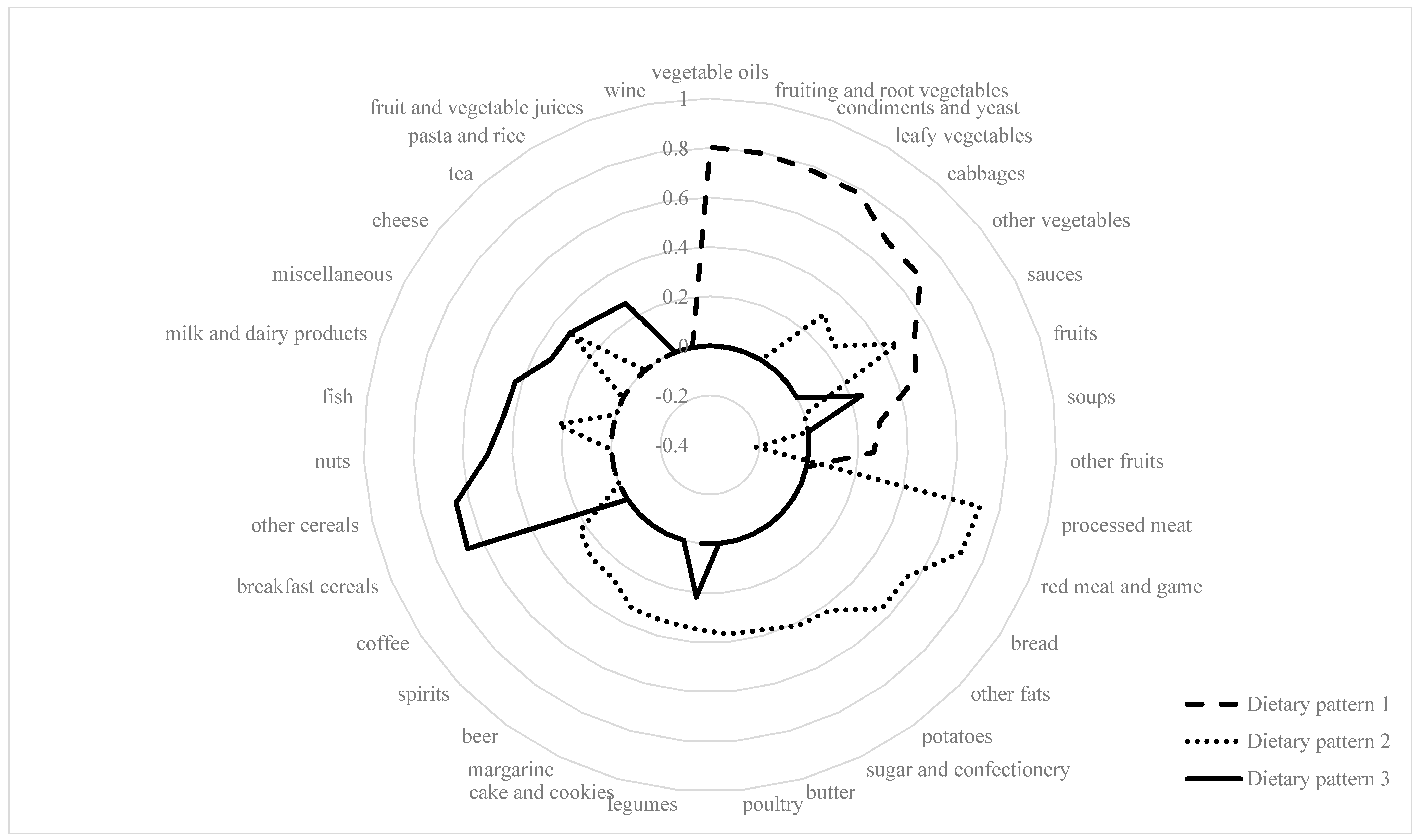
3.2. Dietary Pattern Analyses
4. Discussion
4.1. Principal Findings
4.2. In the Context of the Published Literature
Dietary Vitamin E Intake and Distribution of Circulating Vitamin E Levels in the Population
4.3. Correlates of Vitamin E Biomarkers
4.4. Lack of Association between Estimated Dietary α-Tocopherol Intake and Circulating Vitamin E Levels
4.5. Association of Dietary Patterns with Dietary Vitamin E Intake and Circulating Vitamin E Levels
4.6. Strength and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflict of Interest
References
- Sauberlich, H.E. Vitamin E (Tocopherols). In Laboratory Tests for the Assessment of Nutritional Status, 2nd ed.; CRC Press: Boca Raton, FL, USA, 1999; pp. 249–266. [Google Scholar]
- Jiang, Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radic. Biol. Med. 2014, 72, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US). Panel on Dietary Antioxidants and Related Compounds. In Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; Hardcopy Version at National Academies Press: Washington, DC, USA, 2000; pp. 186–283. [Google Scholar]
- Pham-Huy, L.A.; He, H.; Pham-Huy, C. Free radicals, antioxidants in disease and health. Int. J. Biomed. Sci. 2008, 4, 89–96. [Google Scholar] [PubMed]
- Ohrvall, M.; Sundlof, G.; Vessby, B. Gamma, but not alpha, tocopherol levels in serum are reduced in coronary heart disease patients. J. Intern. Med. 1996, 239, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.E.; Lawson, K.A.; Weinstein, S.J.; Pietinen, P.; Taylor, P.R.; Virtamo, J.; Albanes, D. Higher baseline serum concentrations of vitamin E are associated with lower total and cause-specific mortality in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Am. J. Clin. Nutr. 2006, 84, 1200–1207. [Google Scholar] [PubMed]
- Stampfer, M.J.; Hennekens, C.H.; Manson, J.E.; Colditz, G.A.; Rosner, B.; Willett, W.C. Vitamin E consumption and the risk of coronary disease in women. N. Engl. J. Med. 1993, 328, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Stampfer, M.J.; Ascherio, A.; Giovannucci, E.; Colditz, G.A.; Willett, W.C. Vitamin E consumption and the risk of coronary heart disease in men. N. Engl. J. Med. 1993, 328, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Riemersma, R.A.; Wood, D.A.; Macintyre, C.C.; Elton, R.A.; Gey, K.F.; Oliver, M.F. Risk of angina pectoris and plasma concentrations of vitamins A, C, and E and carotene. Lancet 1991, 337, 1–5. [Google Scholar] [CrossRef]
- Dong, Y.; Liu, Y.; Shu, Y.; Chen, X.; Hu, J.; Zheng, R.; Ma, D.; Yang, C.; Guan, X. Link between risk of colorectal cancer and serum vitamin E levels: A meta-analysis of case-control studies. Medicine 2017, 96, e7470. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.Y.; Appel, L.J. Supplementation of diets with alpha-tocopherol reduces serum concentrations of gamma- and delta-tocopherol in humans. J. Nutr. 2003, 133, 3137–3140. [Google Scholar] [PubMed]
- Raederstorff, D.; Wyss, A.; Calder, P.C.; Weber, P.; Eggersdorfer, M. Vitamin E function and requirements in relation to PUFA. Br. J. Nutr. 2015, 114, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- German Nutrition Society (2017). Vitamin E (Tocopherole). Available online: https://www.dge.de/wissenschaft/referenzwerte/vitamin-e/ (accessed on 18 June 2017).
- Max Rubner-Institut. Nationale Verzehrsstudie II. Ergebnisbericht Teil 2; MRI: Karlsruhe, Germany, 2008. [Google Scholar]
- Borel, P.; Preveraud, D.; Desmarchelier, C. Bioavailability of vitamin E in humans: An update. Nutr. Rev. 2013, 71, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.H.; Kamal-Eldin, A.; Elmadfa, I. Gamma-tocopherol—An underestimated vitamin? Ann. Nutr. Metab. 2004, 48, 169–188. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Martin, A.; Lin, H.; Bermudez, O.I.; Tucker, K.L. alpha-Tocopherol intake and plasma concentration of Hispanic and non-Hispanic white elders is associated with dietary intake pattern. J. Nutr. 2006, 136, 2574–2579. [Google Scholar] [PubMed]
- Talegawkar, S.A.; Johnson, E.J.; Carithers, T.C.; Taylor, H.A., Jr.; Bogle, M.L.; Tucker, K.L. Serum carotenoid and tocopherol concentrations vary by dietary pattern among African Americans. J. Am. Diet. Assoc. 2008, 108, 2013–2020. [Google Scholar] [CrossRef] [PubMed]
- Nothlings, U.; Krawczak, M. PopGen. A population-based biobank with prospective follow-up of a control group. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2012, 55, 831–835. [Google Scholar] [PubMed]
- Nothlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Fitting portion sizes in a self-administered food frequency questionnaire. J. Nutr. 2007, 137, 2781–2786. [Google Scholar] [PubMed]
- Barbaresko, J.; Siegert, S.; Koch, M.; Aits, I.; Lieb, W.; Nikolaus, S.; Laudes, M.; Jacobs, G.; Nothlings, U. Comparison of two exploratory dietary patterns in association with the metabolic syndrome in a Northern German population. Br. J. Nutr. 2014, 112, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Haftenberger, M.; Schuit, A.J.; Tormo, M.J.; Boeing, H.; Wareham, N.; Bueno-de-Mesquita, H.B.; Kumle, M.; Hjartaker, A.; Chirlaque, M.D.; Ardanaz, E.; et al. Physical activity of subjects aged 50–64 years involved in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002, 5, 1163–1176. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.; Norat, T.; Steindorf, K.; Boutron-Ruault, M.C.; Pischon, T.; Mazuir, M.; Clavel-Chapelon, F.; Linseisen, J.; Boeing, H.; Bergman, M.; et al. Physical activity and risk of colon and rectal cancers: The European prospective investigation into cancer and nutrition. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 2398–2407. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Dehne, L.I.; Klemm, C.; Henseler, G.; Hermann-Kunz, E. The German Food Code and Nutrient Data Base (BLS II.2). Eur. J. Epidemiol. 1999, 15, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Kroger, J.; Ferrari, P.; Jenab, M.; Bamia, C.; Touvier, M.; Bueno-de-Mesquita, H.B.; Fahey, M.T.; Benetou, V.; Schulz, M.; Wirfalt, E.; et al. Specific food group combinations explaining the variation in intakes of nutrients and other important food components in the European Prospective Investigation into Cancer and Nutrition: An application of the reduced rank regression method. Eur. J. Clin. Nutr. 2009, 63 (Suppl. S4), S263–S274. [Google Scholar] [CrossRef] [PubMed]
- Augustin, K.; Blank, R.; Boesch-Saadatmandi, C.; Frank, J.; Wolffram, S.; Rimbach, G. Dietary green tea polyphenols do not affect vitamin E status, antioxidant capacity and meat quality of growing pigs. J. Anim. Physiol. Anim. Nutr. 2008, 92, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Thurnham, D.I.; Davies, J.A.; Crump, B.J.; Situnayake, R.D.; Davis, M. The use of different lipids to express serum tocopherol: Lipid ratios for the measurement of vitamin E status. Ann. Clin. Biochem. 1986, 23 Pt 5, 514–520. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Schulze, M.B.; Schienkiewitz, A.; Nothlings, U.; Boeing, H. Application of a new statistical method to derive dietary patterns in nutritional epidemiology. Am. J. Epidemiol. 2004, 159, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, Z.C. Vitamin E Intake and Cardiovascular Diseases in the EPIC-Potsdam Study. Ph.D. Thesis, Technical University of Berlin, Berlin, Germany, 2011. [Google Scholar]
- Jenab, M.; Salvini, S.; van Gils, C.H.; Brustad, M.; Shakya-Shrestha, S.; Buijsse, B.; Verhagen, H.; Touvier, M.; Biessy, C.; Wallstrom, P.; et al. Dietary intakes of retinol, beta-carotene, vitamin D and vitamin E in the European Prospective Investigation into Cancer and Nutrition cohort. Eur. J. Clin. Nutr. 2009, 63 (Suppl. S4), S150–S178. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wilde, P.E.; Lichtenstein, A.H.; Bermudez, O.I.; Tucker, K.L. The maximal amount of dietary alpha-tocopherol intake in U.S. adults (NHANES 2001–2002). J. Nutr. 2006, 136, 1021–1026. [Google Scholar] [PubMed]
- Max Rubner-Institut. Nationale Verzehrsstudie II. Lebensmittelverzehr und Nährstoffzufuhr auf Basis von 24h-Recalls; MRI: Karlsruhe, Germany, 2013. [Google Scholar]
- Wolters, M.; Hermann, S.; Golf, S.; Katz, N.; Hahn, A. Selenium and antioxidant vitamin status of elderly German women. Eur. J. Clin. Nutr. 2006, 60, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Kompauer, I.; Heinrich, J.; Wolfram, G.; Linseisen, J. Association of carotenoids, tocopherols and vitamin C in plasma with allergic rhinitis and allergic sensitisation in adults. Public Health Nutr. 2006, 9, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Schleicher, R.L.; Mokdad, A.H.; Ajani, U.A.; Liu, S. Distribution of serum concentrations of alpha-tocopherol and gamma-tocopherol in the US population. Am. J. Clin. Nutr. 2006, 84, 375–383. [Google Scholar] [PubMed]
- Péter, S.; Friedel, A.; Roos, F.F.; Wyss, A.; Eggersdorfer, M.; Hoffmann, K.; Weber, P. A Systematic Review of Global Alpha-Tocopherol Status as Assessed by Nutritional Intake Levels and Blood Serum Concentrations. Int. J. Vitam. Nutr. Res. 2016, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Stuetz, W.; Weber, D.; Dolle, M.E.; Jansen, E.; Grubeck-Loebenstein, B.; Fiegl, S.; Toussaint, O.; Bernhardt, J.; Gonos, E.S.; Franceschi, C.; et al. Plasma Carotenoids, Tocopherols, and Retinol in the Age-Stratified (35–74 Years) General Population: A Cross-Sectional Study in Six European Countries. Nutrients 2016, 8, 614. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Christen, S.; Shigenaga, M.K.; Ames, B.N. gamma-tocopherol, the major form of vitamin E in the US diet, deserves more attention. Am. J. Clin. Nutr. 2001, 74, 714–722. [Google Scholar] [PubMed]
- Millen, A.E.; Dodd, K.W.; Subar, A.F. Use of vitamin, mineral, nonvitamin, and nonmineral supplements in the United States: The 1987, 1992, and 2000 National Health Interview Survey results. J. Am. Diet. Assoc. 2004, 104, 942–950. [Google Scholar] [CrossRef] [PubMed]
- White, E.; Kristal, A.R.; Shikany, J.M.; Wilson, A.C.; Chen, C.; Mares-Perlman, J.A.; Masaki, K.H.; Caan, B.J. Correlates of serum alpha- and gamma-tocopherol in the Women’s Health Initiative. Ann. Epidemiol. 2001, 11, 136–144. [Google Scholar] [CrossRef]
- McBurney, M.I.; Yu, E.A.; Ciappio, E.D.; Bird, J.K.; Eggersdorfer, M.; Mehta, S. Suboptimal Serum alpha-Tocopherol Concentrations Observed among Younger Adults and Those Depending Exclusively upon Food Sources, NHANES 2003-20061-3. PLoS ONE 2015, 10, e0135510. [Google Scholar] [CrossRef] [PubMed]
- Handelman, G.J.; Machlin, L.J.; Fitch, K.; Weiter, J.J.; Dratz, E.A. Oral alpha-tocopherol supplements decrease plasma gamma-tocopherol levels in humans. J. Nutr. 1985, 115, 807–813. [Google Scholar] [PubMed]
- Gaedicke, S.; Zhang, X.; Huebbe, P.; Boesch-Saadatmandi, C.; Lou, Y.; Wiswedel, I.; Gardemann, A.; Frank, J.; Rimbach, G. Dietary vitamin E, brain redox status and expression of Alzheimer’s disease-relevant genes in rats. Br. J. Nutr. 2009, 102, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Traber, M.G. Mechanisms for the prevention of vitamin E excess. J. Lipid Res. 2013, 54, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Hosomi, A.; Arita, M.; Sato, Y.; Kiyose, C.; Ueda, T.; Igarashi, O.; Arai, H.; Inoue, K. Affinity for alpha-tocopherol transfer protein as a determinant of the biological activities of vitamin E analogs. FEBS Lett. 1997, 409, 105–108. [Google Scholar] [CrossRef]
- Traber, M.G. Vitamin E regulatory mechanisms. Annu. Rev. Nutr. 2007, 27, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Sontag, T.J.; Parker, R.S. Cytochrome P450 omega-hydroxylase pathway of tocopherol catabolism. Novel mechanism of regulation of vitamin E status. J. Biol. Chem. 2002, 277, 25290–25296. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bohlscheid-Thomas, S.; Voss, S.; Schneeweiss, S.; Wahrendorf, J. The relative validity of vitamin intakes derived from a food frequency questionnaire compared to 24-h recalls and biological measurements: Results from the EPIC pilot study in Germany. European Prospective Investigation into Cancer and Nutrition. Int. J. Epidemiol. 1997, 26 (Suppl. S1), S82–S90. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Marks, G.C.; Gaffney, P.; Williams, G.; Green, A. Validation of a food-frequency questionnaire assessment of carotenoid and vitamin E intake using weighed food records and plasma biomarkers: The method of triads model. Eur. J. Clin. Nutr. 2005, 59, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Stampfer, M.J.; Colditz, G.A.; Rimm, E.B.; Litin, L.; Willett, W.C. Correlations of vitamin A and E intakes with the plasma concentrations of carotenoids and tocopherols among American men and women. J. Nutr. 1992, 122, 1792–1801. [Google Scholar] [PubMed]
- Stryker, W.S.; Kaplan, L.A.; Stein, E.A.; Stampfer, M.J.; Sober, A.; Willett, W.C. The relation of diet, cigarette smoking, and alcohol consumption to plasma beta-carotene and alpha-tocopherol levels. Am. J. Epidemiol. 1988, 127, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Kardinaal, A.F.; van ’t Veer, P.; Brants, H.A.; van den Berg, H.; van Schoonhoven, J.; Hermus, R.J. Relations between antioxidant vitamins in adipose tissue, plasma, and diet. Am. J. Epidemiol. 1995, 141, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Solvoll, K.; Johansson, L.R.; Salminen, I.; Aro, A.; Drevon, C.A. Evaluation of a food frequency questionnaire with weighed records, fatty acids, and alpha-tocopherol in adipose tissue and serum. Am. J. Epidemiol. 1999, 150, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Schmolz, L.; Birringer, M.; Lorkowski, S.; Wallert, M. Complexity of vitamin E metabolism. World J. Biol. Chem. 2016, 7, 14–43. [Google Scholar] [CrossRef] [PubMed]
- Galli, F.; Azzi, A.; Birringer, M.; Cook-Mills, J.M.; Eggersdorfer, M.; Frank, J.; Cruciani, G.; Lorkowski, S.; Ozer, N.K. Vitamin E: Emerging aspects and new directions. Free Radic. Biol. Med. 2017, 102, 16–36. [Google Scholar] [CrossRef] [PubMed]
- Mah, E.; Sapper, T.N.; Chitchumroonchokchai, C.; Failla, M.L.; Schill, K.E.; Clinton, S.K.; Bobe, G.; Traber, M.G.; Bruno, R.S. alpha-Tocopherol bioavailability is lower in adults with metabolic syndrome regardless of dairy fat co-ingestion: A randomized, double-blind, crossover trial. Am. J. Clin. Nutr. 2015, 102, 1070–1080. [Google Scholar] [CrossRef] [PubMed]
- Traber, M.G.; Mah, E.; Leonard, S.W.; Bobe, G.; Bruno, R.S. Metabolic syndrome increases dietary alpha-tocopherol requirements as assessed using urinary and plasma vitamin E catabolites: A double-blind, crossover clinical trial. Am. J. Clin. Nutr. 2017, 105, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Chuang, J.C.; Matel, H.D.; Nambiar, K.P.; Kim, S.H.; Fadel, J.G.; Holstege, D.M.; Clifford, A.J. Quantitation of [5-14CH3]-(2R, 4′R, 8′R)-alpha-tocopherol in humans. J. Nutr. 2011, 141, 1482–1488. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | |
| Men, % | 59.4 |
| Age, years | 61.2 (11.6) |
| Body mass index, kg/m2 | 27.2 (4.5) |
| Weight, kg | 80.5 (15.7) |
| Hip circumference, cm | 102.3 (8.8) |
| Waist circumference, cm | 96.2 (13.0) |
| Systolic blood pressure, mmHg | 139.6 (18.2) |
| Diastolic blood pressure, mmHg | 85.0 (8.9) |
| Prevalent hypertension, % | 69.0 |
| Current smokers, % | 10.9 |
| High education (≥11 years), % | 35.9 |
| Prevalent diabetes, % | 10.8 |
| Vitamin E supplementation, % | 7.5 |
| Physical activity, MET-hour/week | 90.0 (58.3, 131.6) |
| Alcohol consumption, g/day | 9.6 (3.7, 18.7) |
| Dietary α-tocopherol intake (FFQ), mg/day | 11.6 (9.7, 13.9) |
| Biochemical features | |
| α-tocopherol, μmol/L | 31.5 (27.27, 37.03) |
| α-tocopherol > 30 μmol/L, % * | 57.6 |
| α-tocopherol/cholesterol ratio, μmol/mmol | 5.53 (4.88, 6.33) |
| γ-tocopherol, μmol/L | 1.35 (0.99, 1.79) |
| γ-tocopherol/cholesterol ratio, μmol/mmol | 0.24 (0.18, 0.31) |
| HbA1c, % | 5.60 (5.40, 5.90) |
| C-reactive protein, mg/dL | 1.20 (0.45, 2.50) |
| HDL-cholesterol, mg/dL | 65.81 (18.61) |
| LDL-cholesterol, mg/dL | 131.36 (34.07) |
| Total cholesterol, mg/dL | 223.42 (41.38) |
| Triglycerides, mg/dL | 106.0 (76.0, 139.0) |
| (a) α-Tocopherol * | β Estimate | SE | p Value |
| Age | −0.0006 | 0.0007 | 0.358 |
| Sex | −0.0108 | 0.0184 | 0.556 |
| Triglycerides | 0.0015 | 0.0001 | <0.0001 |
| HDL-cholesterol | 0.0033 | 0.0005 | <0.0001 |
| LDL-cholesterol | 0.0027 | 0.0002 | <0.0001 |
| Vitamin E supplementation | 0.0863 | 0.0307 | 0.005 |
| R2 = 0.359 | |||
| (b) α-Tocopherol/Cholesterol Ratio * | |||
| Age | −0.0014 | 0.0007 | 0.040 |
| Sex | −0.0096 | 0.0187 | 0.606 |
| Triglycerides | 0.0009 | 0.0001 | <0.0001 |
| HDL-cholesterol | −0.0013 | 0.0005 | 0.015 |
| LDL-cholesterol | −0.0021 | 0.0002 | <0.0001 |
| Vitamin E supplementation | 0.0777 | 0.0311 | 0.013 |
| R2 = 0.197 | |||
| (c) γ-Tocopherol * | |||
| Age | −0.0011 | 0.1562 | 0.474 |
| Sex | −0.0681 | 0.0016 | 0.108 |
| Triglycerides | 0.0019 | 0.0423 | <0.0001 |
| HDL-cholesterol | 0.0031 | 0.0003 | 0.011 |
| LDL-cholesterol | 0.0018 | 0.0012 | 0.001 |
| Vitamin E supplementation | −0.3170 | 0.0006 | <0.0001 |
| R2 = 0.127 | |||
| (d) γ-Tocopherol/Cholesterol Ratio * | |||
| Age | −0.0020 | 0.0016 | 0.201 |
| Sex | −0.0454 | 0.0381 | 0.235 |
| Triglycerides | 0.0015 | 0.0003 | <0.0001 |
| LDL-cholesterol | −0.0030 | 0.0006 | <0.0001 |
| Vitamin E supplementation | −0.3225 | 0.0707 | <0.0001 |
| R2 = 0.106 |
| α-Tocopherol | γ-Tocopherol | |||
|---|---|---|---|---|
| rho | 95% CI | rho | 95% CI | |
| Leafy vegetables | 0.03 | −0.05, 0.10 | 0.01 | −0.07, 0.08 |
| Fruiting and root vegetables | 0.01 | −0.06, 0.09 | 0.04 | −0.04, 0.12 |
| Cabbages | −0.04 | −0.12, 0.04 | 0.05 | −0.02, 0.13 |
| Other vegetables | −0.04 | −0.12, 0.04 | 0.03 | −0.04, 0.11 |
| Legumes | 0.02 | −0.06, 0.10 | 0.05 | −0.03, 0.12 |
| Nuts | 0.08 | −0.002, 0.15 | 0.07 | −0.01, 0.15 |
| Other fruits | 0.11 | 0.04, 0.20 | 0.12 | 0.04, 0.19 |
| Breakfast cereals | 0.06 | −0.001, 0.14 | 0.03 | −0.05, 0.11 |
| Other cereals | 0.03 | −0.04, 0.11 | 0.01 | −0.07, 0.09 |
| Margarine | 0.01 | −0.07, 0.08 | 0.02 | −0.06, 0.10 |
| Vegetables oils | 0.06 | −0.07, 0.14 | 0.02 | −0.06, 0.10 |
| Dietary α-tocopherol intake (FFQ) | 0.01 | −0.07, 0.09 | 0.005 | −0.07, 0.08 |
| Dietary α-tocopherol intake (FFQ) * | 0.01 | −0.07, 0.09 | 0.01 | −0.07, 0.09 |
| α-Tocopherol | |||||||||
| Overall (n = 641) | Dietary Pattern 1 | Dietary Pattern 2 | Dietary Pattern 3 | ||||||
| β Estimate | SE | p Value | β Estimate | SE | p Value | β Estimate | SE | p Value | |
| α-tocopherol, µmol/L *,† | −0.007 | 0.008 | 0.415 | −0.026 | 0.015 | 0.089 | 0.015 | 0.008 | 0.077 |
| α-tocopherol/cholesterol ratio, µmol/mmol *,† | −0.006 | 0.009 | 0.508 | −0.020 | 0.016 | 0.207 | 0.015 | 0.009 | 0.087 |
| Dietary α-tocopherol intake (FFQ), mg/day † | 0.72 ‡ | 0.68, 0.75 | <0.0001 | −0.18 ‡ | −0.25, −0.10 | 0.002 | 0.32 ‡ | 0.24, 0.39 | <0.0001 |
| Non vitamin E supplement users (n = 593) | |||||||||
| α-tocopherol, µmol/L *,§ | −0.003 | 0.009 | 0.712 | −0.032 | 0.016 | 0.047 | 0.015 | 0.009 | 0.097 |
| α-tocopherol/cholesterol ratio, µmol/mmol *,§ | −0.002 | 0.009 | 0.790 | −0.025 | 0.016 | 0.135 | 0.014 | 0.009 | 0.112 |
| Dietary α-tocopherol intake (FFQ), mg/day § | 0.71 ‡ | 0.67, 0.75 | <0.0001 | −0.16 ‡ | −0.24, −0.08 | 0.0001 | 0.34 ‡ | 0.27, 0.41 | <0.0001 |
| γ-Tocopherol | |||||||||
| Overall (n = 641) | |||||||||
| γ-tocopherol, µmol/L *,† | 0.006 | 0.019 | 0.759 | −0.013 | 0.036 | 0.715 | 0.027 | 0.019 | 0.165 |
| γ-tocopherol/cholesterol ratio, µmol/mmol *,|| | 0.007 | 0.019 | 0.715 | −0.004 | 0.036 | 0.920 | 0.024 | 0.019 | 0.216 |
| Non vitamin E supplement users (n = 593) | |||||||||
| γ-tocopherol, µmol/L *,§ | 0.004 | 0.020 | 0.844 | 0.004 | 0.036 | 0.906 | 0.022 | 0.019 | 0.262 |
| γ-tocopherol/cholesterol ratio, µmol/mmol *,¶ | 0.005 | 0.020 | 0.790 | 0.014 | 0.036 | 0.695 | 0.018 | 0.019 | 0.352 |
| α-Tocopherol | ||||
| Overall (n = 641) | β Estimate | SE | p Value | R2 |
| α-tocopherol, µmol/L *,† | −0.002 | 0.003 | 0.475 | 0.359 |
| α-tocopherol/cholesterol ratio, µmol/mmol *,† | −0.001 | 0.004 | 0.683 | 0.198 |
| Dietary α-tocopherol intake (FFQ), mg/day † | 0.51 ‡ | 0.45, 0.56 | <0.0001 | |
| Non vitamin E supplement users (n = 593) | ||||
| α-tocopherol, µmol/L *,§ | −0.001 | 0.004 | 0.749 | 0.355 |
| α-tocopherol/cholesterol ratio, µmol/mmol *,§ | −0.0002 | 0.004 | 0.947 | 0.179 |
| Dietary α-tocopherol intake (FFQ), mg/day § | 0.49 ‡ | 0.42, 0.55 | <0.0001 | |
| γ-Tocopherol | ||||
| Overall (n = 641) | ||||
| γ-tocopherol, µmol/L *,† | 0.006 | 0.008 | 0.431 | 0.100 |
| γ-tocopherol/cholesterol ratio, µmol/mmol *,|| | 0.008 | 0.008 | 0.346 | 0.080 |
| Non vitamin E supplement users (n = 593) | ||||
| γ-tocopherol, µmol/L *,§ | 0.005 | 0.008 | 0.549 | 0.107 |
| γ-tocopherol/cholesterol ratio, µmol/mmol *,¶ | 0.007 | 0.008 | 0.412 | 0.084 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Waniek, S.; Di Giuseppe, R.; Esatbeyoglu, T.; Plachta-Danielzik, S.; Ratjen, I.; Jacobs, G.; Nöthlings, U.; Koch, M.; Schlesinger, S.; Rimbach, G.; et al. Vitamin E (α- and γ-Tocopherol) Levels in the Community: Distribution, Clinical and Biochemical Correlates, and Association with Dietary Patterns. Nutrients 2018, 10, 3. https://doi.org/10.3390/nu10010003
Waniek S, Di Giuseppe R, Esatbeyoglu T, Plachta-Danielzik S, Ratjen I, Jacobs G, Nöthlings U, Koch M, Schlesinger S, Rimbach G, et al. Vitamin E (α- and γ-Tocopherol) Levels in the Community: Distribution, Clinical and Biochemical Correlates, and Association with Dietary Patterns. Nutrients. 2018; 10(1):3. https://doi.org/10.3390/nu10010003
Chicago/Turabian StyleWaniek, Sabina, Romina Di Giuseppe, Tuba Esatbeyoglu, Sandra Plachta-Danielzik, Ilka Ratjen, Gunnar Jacobs, Ute Nöthlings, Manja Koch, Sabrina Schlesinger, Gerald Rimbach, and et al. 2018. "Vitamin E (α- and γ-Tocopherol) Levels in the Community: Distribution, Clinical and Biochemical Correlates, and Association with Dietary Patterns" Nutrients 10, no. 1: 3. https://doi.org/10.3390/nu10010003