A Qualitative Investigation to Underpin the Development of an Electronic Tool to Assess Nutrition Literacy in Australian Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Data Analysis
3. Results
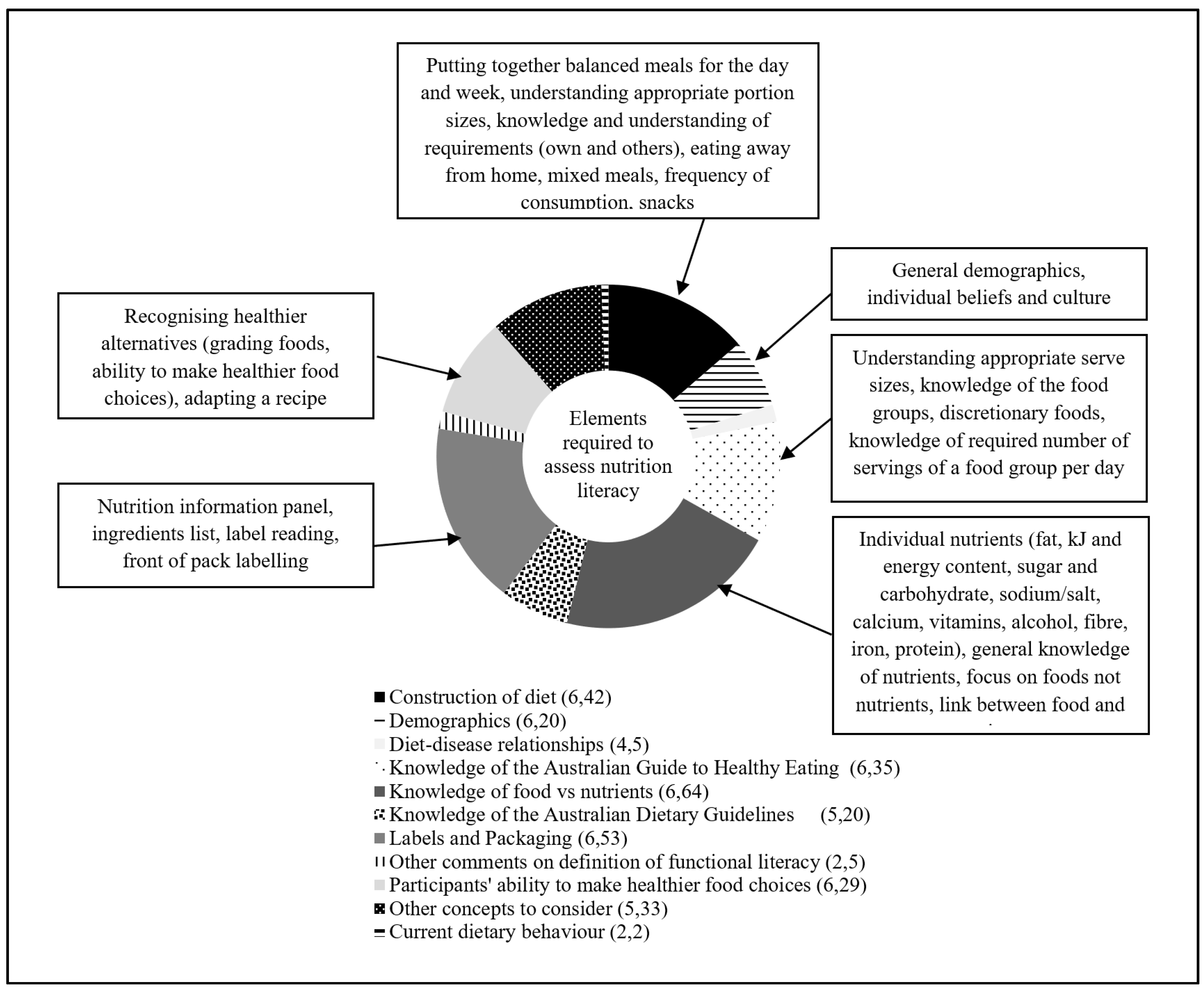
3.1. Nutrition Literacy Assessment Areas
3.1.1. Knowledge of Nutrients versus Foods
3.1.2. Knowledge of the AGHE and ADG
3.1.3. Food Packaging
3.1.4. Construction of a Healthy Diet
3.1.5. Making Healthier Food Choices
3.1.6. Demographic Characteristics
3.2. Electronic Tool Presentation Features
3.2.1. Interactive Animations
3.2.2. Presentation of Mixed Foods
3.2.3. Practical Suggestions on Item Presentation
3.2.4. Food Images
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Neuhauser, L.; Rothschild, R.; Rodriguez, F.M. MyPyramid.gov: Assessment of literacy, cultural and linguistic factors in the USDA food pyramid web site. J. Nutr. Educ. Behav. 2007, 39, 219–225. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Health Promotion. Track 2: Health Literacy and Health Behaviour. Available online: http://www.who.int/healthpromotion/conferences/7gchp/track2/en/ (accessed on 14 December 2017).
- Australian Bureau of Statistics. 4233.0-Health Literacy, Australia. 2006. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/Latestproducts/4233.0Main%20Features22006?opendocument&tabname=Summary&prodno=4233.0&issue=2006&num=&view= (accessed on 14 December 2017).
- Carbone, E.T.; Zoellner, J.M. Nutrition and health literacy: A systematic review to inform nutrition research and practice. J. Acad. Nutr. Diet. 2012, 112, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission on Safety and Quality in Health Care. Consumers, the Health System and Health Literacy: Taking Action to Improve Safety and Quality. Consultation Paper. Available online: http://www.safetyandquality.gov.au/our-work/patient-and-consumer-centred-care/health-literacy/consumers-the-health-system-and-health-literacy-taking-action-to-improve-safety-and-quality-3/ (accessed on 14 December 2017).
- Dewalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes: A systematic review of the literature. J. Gen. Int. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Viera, A.; Crotty, K.; Holland, A.; Brasure, M.; Lohr, K.N.; Harden, E.; et al. Health literacy interventions and outcomes: An updated systematic review. Evid. Rep. Technol. Assess. 2011, 199, 1–941. [Google Scholar]
- Bush, R.; Boyle, F.; Ostini, R.; Ozolins, I.; Brabant, M.; Soto, E.; Eriksson, L. Advancing Health Literacy Through Primary Health Care Systems; Australian Primary Health Care Research Institute: Canberra, Australia, 2010. [Google Scholar]
- Nutbeam, D. The evolving concept of health literacy. Soc. Sci. Med. 2008, 67, 2072–2078. [Google Scholar] [CrossRef] [PubMed]
- Silk, K.J.; Sherry, J.; Winn, B.; Keesecker, N.; Horodynski, M.A.; Sayir, A. Increasing nutrition literacy: Testing the effectiveness of print, web site, and game modalities. J. Nutr. Educ. Behav. 2008, 40, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.; You, W.; Connell, C.; Smith-Ray, R.L.; Allen, K.; Tucker, K.L.; Davy, B.M.; Estabrooks, P. Health literacy is associated with healthy eating index scores and sugar-sweetened beverage intake: Findings from the rural lower Mississippi delta. J. Am. Diet. Assoc. 2011, 111, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Persoskie, A.; Hennessy, E.; Nelson, W.L. US consumers’ understanding of nutrition labels in 2013: The importance of health literacy. Prev. Chronic Dis. 2017, 14, E86. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D. Nutrition Literacy: Foundations and Development of an Instrument for Assessment. Ph.D. Thesis, University of Illinois, Urbana-Champaign, IL, USA, 2012. [Google Scholar]
- Gibbs, H.; Chapman-Novakofski, K. A review of health literacy and its relationship to nutrition education. Top. Clin. Nutr. 2012, 27, 325–333. [Google Scholar] [CrossRef]
- Wegener, J.A. Review of Nutrition Knowledge Assessment Instruments for Community-Based Settings; Public Health Agency of Canada: Ottawa, ON, Canada, 2007.
- Gibbs, H.; Chapman-Novakofski, K. Exploring nutrition literacy: Attention to assessment and the skills clients need. Health 2012, 4, 120–124. [Google Scholar] [CrossRef]
- Gibbs, H.; Chapman-Novakofski, K. Establishing content validity for the nutrition literacy assessment instrument. Prev. Chronic Dis. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D.; Ellerbeck, E.F.; Befort, C.; Gajewski, B.; Kennett, A.R.; Yu, Q.; Christifano, D.; Sullivan, D.K. Measuring nutrition literacy in breast cancer patients: Development of a novel instrument. J. Cancer Educ. 2016, 31, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D.; Kennett, A.R.; Kerling, E.H.; Yu, Q.; Gajewski, B.; Ptomey, L.T.; Sullivan, D.K. Assessing the nutrition literacy of parents and its relationship with child diet quality. J. Nutr. Educ. Behav. 2016, 48, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D.; Camargo, J.; Owens, S.; Gajewski, B.; Cupertino, A.P. Measuring nutrition literacy in Spanish-speaking Latinos: An exploratory validation study. J. Immigr. Minority Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, H.D.; Ellerbeck, E.F.; Gajewski, B.; Zhang, C.; Sullivan, D.K. The nutrition literacy assessment instrument is a valid and reliable measure of nutrition literacy in adults with chronic disease. J. Nutr. Educ. Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Velardo, S. The nuances of health literacy, nutrition literacy, and food literacy. J. Nutr. Educ. Behav. 2015, 47, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Guttersrud, Ø.; Dalane, J.Ø.; Pettersen, S. Improving measurement in nutrition literacy research using Rasch modelling: Examining construct validity of stage-specific ‘critical nutrition literacy’ scales. Public Health Nutr. 2014, 17, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Guttersrud, O.; Petterson, K.S. Young adolescents′ engagement in dietary Behaviour—The impact of gender, socio-economic status, self-efficacy and scientific literacy. Methodological aspects of constructing measures in nutrition literacy research using the Rasch model. Public Health Nutr. 2015, 18, 2565–2574. [Google Scholar] [CrossRef] [PubMed]
- Doustmohammadian, A.; Omidvar, N.; Keshavarz-Mohammadi, N.; Abdollahi, M.; Amini, M.; Eini-Zinab, H. Developing and validating a scale to measure food and nutrition literacy (FNLIT) in elementary school children in Iran. PLoS ONE 2017, 12, e0179196. [Google Scholar] [CrossRef] [PubMed]
- Perkins, L.; Cohen, J. Meeting patient needs in the hospital Setting—Are written nutrition education resources too hard to understand? Nutr. Diet. 2008, 65, 216–221. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 4102.0—Australian Social Trends, Adult Literacy. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4102.02008?OpenDocument (accessed on 25 October 2013).
- Hahn, E.A.; Burns, J.L.; Jacobs, E.A.; Ganschow, P.S.; Garcia, S.F.; Rutsohn, J.P.; Baker, D.W. Health literacy and patient-reported outcomes: A cross-sectional study of underserved English- and Spanish- Speaking patients with type 2 diabetes. J. Health Commun. 2015, 20, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Cremers, A.H.M.; Welbie, M.; Kranenborg, K.; Wittink, H. Deriving guidelines for designing interactive questionnaires for Low-Literate persons: Development of a health assessment questionnaire. Univers. Access Inf. Soc. 2017, 16, 161–172. [Google Scholar] [CrossRef]
- Morse, J.; Richards, L. Readme First for a User′S Guide to Qualitative Methods; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013.
- Brown, L.; Capra, S.; Williams, L. Profile of the Australian dietetic workforce: 1991–2005. Nutr. Diet. 2006, 63, 166–178. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; Pearson, S. Interpreting the Australian dietary guideline to “limit” into practical and personalised advice. Nutrients 2015, 7, 2026–2043. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R.; Tapsell, L.C. Food synergy: The key to a healthy diet. Proc. Nutr. Soc. 2013, 72, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Kolodinsky, J.; Harvey-Berino, J.R.; Berlin, L.; Johnson, R.K.; Reynolds, T.W. Knowledge of current dietary guidelines and food choice by college students: Better eaters have higher knowledge of dietary guidance. J. Am. Diet. Assoc. 2007, 107, 1409–1413. [Google Scholar] [CrossRef] [PubMed]
- Abramovitch, S.L.; Reddigan, J.I.; Hamadeh, M.J.; Jamnik, V.K.; Rowan, C.P.; Kuk, J.L. Underestimating a serving size may lead to increased food consumption when using Canada’s food guide. Appl. Physiol. Nutr. Metab. 2012, 37, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Wu, J.H.; Louie, J.C.; Flood, V.M.; Gill, T.; Thomas, B.; Cleanthous, X.; Neal, B.; Rangan, A. Typical food portion sizes consumed by Australian adults: Results from the 2011–12 Australian national nutrition and physical activity survey. Sci. Rep. 2016, 6, 19596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brochure: Food Labels—NSW Food Authority. Available online: https://www.yumpu.com/en/document/view/11604856/brochure-food-labels-nsw-food-authority (accessed on 19 June 2017).
- Blewett, N.; Goddard, N.; Pettigrew, S.; Reynolds, C.; Yeatman, H. Labelling Logic: Review of Food Labelling Law and Policy; Commonwealth of Australia: Canberra, Australia, 2011.
- Gorton, D. Nutrition Labelling-Update of Scientific Evidence on Consumer Use and Understanding of Nutrition Labels and Claims: A Report Prepared for the New Zealand Food Safety Authority and the Ministry of Health. Clinical Trials Unit; University of Auckland: Auckland, New Zealand, 2007. [Google Scholar]
- Rothman, R.L.; Housam, R.; Weiss, H.; Davis, D.; Gregory, R.; Gebretsadik, T.; Shintani, A.; Elasy, T.A. Patient understanding of food labels: The role of literacy and numeracy. Am. J. Prev. Med. 2006, 31, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Ringland, E.M.; Gifford, J.A.; Denyer, G.S.; Thai, D.; Franklin, J.L.; Stevenson, M.M.; Prvan, T.; O’Connor, H.T. Evaluation of an electronic tool to assess food label literacy in adult Australians: A pilot study. Nutr. Diet. 2016, 73, 482–489. [Google Scholar] [CrossRef]
- Miller, L.M.; Cassady, D.L.; Applegate, E.A.; Beckett, L.A.; Wilson, M.D.; Gibson, T.N.; Ellwood, K. Relationships among food label use, motivation, and dietary quality. Nutrients 2015, 7, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Houts, P.S.; Doak, C.C.; Doak, L.G.; Loscalzo, M.J. The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence. Patient Educ. Couns. 2006, 61, 173–190. [Google Scholar] [CrossRef] [PubMed]
- McCaffery, K.J.; Dixon, A.; Hayen, A.; Jansen, J.; Smith, S.; Simpson, J.M. The influence of graphic display format on the interpretations of quantitative risk information among adults with lower education and literacy: A randomized experimental study. Med. Decis. Mak. 2012, 32, 532–544. [Google Scholar] [CrossRef] [PubMed]
- Hahn, E.A.; Cella, D.; Dobrez, D.; Shiomoto, G.; Marcus, E.; Taylor, S.G.; Vohra, M.; Chang, C.H.; Wright, B.D.; Linacre, J.M.; et al. The talking touchscreen: A new approach to outcomes assessment in low literacy. Psychooncology 2004, 13, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Ruzek, S.B.; Bass, S.B.; Greener, J.; Wolak, C.; Gordon, T.F. Randomized trial of a computerized touch screen decision aid to increase acceptance of colonoscopy screening in an African American population with limited literacy. Health Commun. 2016, 31, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Siozos, P.; Palaigeorgiou, G.; Triantafyllakos, G.; Despotakis, T. Computer based testing using “digital ink”: Participatory design of a Tablet PC based assessment application for secondary education. Comput. Educ. 2009, 52, 811–819. [Google Scholar] [CrossRef]
- Ruppert, B. New directions in the use of virtual reality for food shopping: Marketing and education perspectives. J. Diabetes Sci. Technol. 2011, 5, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Ershow, A.G.; Peterson, C.M.; Riley, W.T.; Rizzo, A.S.; Wansink, B. Virtual reality technologies for research and education in obesity and diabetes: Research needs and opportunities. J. Diabetes Sci. Technol. 2011, 5, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Probst, Y.; Krnavek, C.; Lockyer, L.; Tapsell, L. Development of a computer-assisted dietary assessment tool for use in primary healthcare practice: Perceptions of nutrition and computers in a sample of older adults with type 2 diabetes mellitus. Aust. J. Prim. Health 2005, 11, 54–62. [Google Scholar] [CrossRef]


{kind=link}
| Guiding Question |
|---|
| Could you describe your experience working with individuals using nutrition guidelines? |
| What problems have you encountered with communicating the Australian Dietary Guidelines to individuals? |
| What problems have you encountered with communicating the Australian Guide to Healthy Eating? |
| What problems have you encountered with communicating nutrition information panels? |
| What have you found helpful in communicating these nutrition guidelines to individuals? |
| If an electronic resource were available, what features would it have to facilitate evaluating guidelines knowledge of individuals? |
| What do you see as core to assess in such a tool? |
| Dietitians Association of Australia Work Areas | Number of Participants |
|---|---|
| Hospital */nursing home | 13 |
| Food service | 4 |
| Community health | 9 |
| Government department | 3 |
| Educational institution ** | 12 |
| Private practice | 6 |
| Industry | 8 |
| Public health nutrition † | 10 |
| Other ‡ | 11 |
| Theme | Code | Number of References † | Quotation ‡ |
|---|---|---|---|
| Knowledge of nutrients versus food | |||
| General knowledge of nutrients | 11 | Just on the point of linking foods with nutrients I think that might be maybe a key activity having the three main or like carbohydrate, protein, fat, vitamins and minerals as an option with a list of food pictures and just ticking or selecting the options of which that food might relate to that was an activity that we’ve worked—has worked well with very low literacy groups just linking the actual role of food to the food type. (Wanda, FG5) | |
| Focusing on foods, not nutrients | 4 | I think a whole food approach and maybe even a meal approach (Dianne, FG5) | |
| Fat | 14 | The two areas that you might want to consider I think would be energy content and saturated fat. I think trying to disentangle saturated fat from total fat would be useful. That the focus is on saturated fat and not total fat. (Wilson, FG4) | |
| Energy content/kJ (kilojoules) | 10 | I still think energy content of meals and choices is a really key thing that needs to be looked at. Can people identify which is a lower kilojoule option when they’re presented with several food options in front of them? (Wilson, FG4) | |
| Sugar and carbohydrates | 8 | With the nutrient side of things it’s also an important message to talk about added and natural sugars because that’s something at the moment, everyone’s just—sugar is getting a bad name for everything, so I do think they need to be used in conjunction and maybe looking at it more from a whole food point of view rather than reducing the intake of refined foods and for these reasons of them either higher in sugar, salt or/and fat. (Rachel, FG 6) | |
| Sodium or salt | 5 | Australians need to reduce their salt intake and then go for questions as to how you do it. You could even say ‘Australians need to reduce their salt intake because half the population has high blood pressure by the time they’re fifty or whatever and this costs us x billion dollars per year for the medication’. I don’t know if I’d go that far but just to give a rationale that the medical evidence suggest that most people need to reduce their sodium intake from salt and then you look at how you might do it. (Sonia, FG4) | |
| Calcium | 4 | Parents had forgotten that you need calcium for children so therefore they need dairy food. (Georgia, FG6) | |
| Vitamins | 2 | They had forgotten that vitamin C is an essential vitamin and therefore you need citrus fruits. I think they do need to have some understanding of the vitamins and the minerals. (Georgia, FG6) | |
| Alcohol | 2 | Maybe knowing how much alcohol is recommended, what the actual guideline is for alcohol (laughter). Even though it changes, probably, yeah, knowing what it’s supposed to be so you know what to limit down to. (Hayley, FG1) | |
| Fibre | 1 | I don’t think it’s wrong to have some nutrient focused questions if we’re talking about nutrients like sodium, saturated fat but also fibre, calcium and iron potentially and then seeking knowledge about which foods are the best sources of these nutrients. (Wilson, FG4) | |
| Iron | 1 | I don’t think it’s wrong to have some nutrient focused questions if we’re talking about nutrients like sodium, saturated fat but also fibre, calcium and iron potentially and then seeking knowledge about which foods are the best sources of these nutrients. (Wilson, FG4) | |
| Knowledge of the AGHE and Australian Dietary Guidelines | |||
| Understanding appropriate AGHE serve sizes | 12 | I certainly think that serving sizes and the number of recommended serves is a key part that have to be, I would imagine a part of any sort of tool (Wilson, FG4) | |
| Knowledge of the food groups (AGHE) | 11 | Have the groups already up there with different foods under it and getting people to select them into the appropriate group some people think that ice-cream comes under the dairy category. (Rachel, FG6) | |
| Discretionary foods (AGHE) | 9 | It’s funny what some people think is healthy. Yeah, I just think that even things like fruit juices where they might get them from Boost Juice® and they’re thinking that that’s one serve of fruit, but then again that will still fall under that fruit category, well technically juice does, but if there’s a whole heap of sugar and stuff added to it is that then technically a discretionary food? I think there are those sorts of things where you might find, yeah, that that affects what they consider a healthy diet to be. (Rachel, FG6) | |
| Knowledge of required number of serves from a food group per day (AGHE) | 3 | So I think obviously having a section on core food groups pick how many pieces of fruit you should have a day, or the minimum amount of dairy. (Sally, FG2) | |
| Knowledge of the Australian Dietary Guidelines | 20 | They actually specify fat, sugar and salt and I suppose if you measured people’s ability to determine which of two foods or which of three foods have different levels of those nutrients I suppose what it would indicate is how good the Dietary Guidelines might be in terms of changing people’s knowledge. I guess the next question is, “Does that make any difference to consumption?” (Bridget, FG6) | |
| Food Packaging | |||
| Nutrition information panels | 35 | What conclusions should they be drawing from the panel, and what’s meaningful to them, and how to use it is probably the most helpful thing. (Sarah, FG3) | |
| Ingredients list | 11 | It would be interesting to find out what people’s perception is of the ingredient list, because I was just, you know well participant said ‘there’s more information than just the energy and macronutrients but with the ingredient list, I’d be interested to know whether people look at something like this one, for example, banana 8%, strawberry 6%, do they go “well that’s great, it’s got fruit in it, obviously that fits in to my healthy eating, my food groups so I’m going to consume that”. That would be interesting to sort of look at that level, their perception of the ingredients. (Patricia, FG2) | |
| Label reading | 4 | But maybe in addition there should be something about skills in, say, label reading. I mean we have labels and we have lots of nutrition information, we want people to be able to use it in a different way. So I would personally like to see that as part of any sort of nutrition literacy tool. (Wilson, FG4) | |
| Front of pack labelling | 3 | So I think people need to look at that ingredient list and hopefully front of pack labelling will give them a bit more quick information when they’re actually shopping—although it’s also intended to be something people observe when they’re sitting at the breakfast table, reading the cereal or milk and the information on it. (Sonia, FG4) | |
| Construction of diet | |||
| Putting together balanced meals for the day/week | 10 | You’d have a protein in a section and fruit or veggies in another and grains in another bit and so you’d sort of be able to, that works for a meal rather than a day, but I think that idea of being able to build, build your meal or build a day. (Bec, FG2) | |
| Understanding appropriate portion sizes | 10 | I guess we’re recommending they need to just have an understanding of the right portion size for their needs, or for the needs of the people that they are catering for. (Danielle, FG3) | |
| Knowledge and understanding of own and others requirements | 7 | If somebody’s exercising a lot, if somebody has a certain disease, if somebody’s caring for somebody else, if somebody’s overweight, maybe just can they prepare a meal a day of food choice for certain people as well. (Heidi, FG5) | |
| Eating away from home | 6 | You have to remember that labelled food probably makes up at most two thirds of what people eat, probably less than that. And so we don’t want to forget all of those out of home occasions when people are buying food too. So in a way we want to test their skills to be able to make those judgments without reading labels. (Wilson, FG4) | |
| Mixed meals | 4 | It seems to be one area where people just throw their hands up and forget about the serves because you can’t pull out every single ingredient or it may be above their level to be able to pull out every ingredient and stick it into a food category and work out how much their getting in that meal or in a day. So that would be a key example I think. (Wanda, FG5) | |
| Frequency of consumption | 3 | Obviously how often you have a food is as important as how much there is there. (Ben, FG5) | |
| Snacks | 2 | I think snacks and what people consider as a snack in the first place, but picking out and choosing healthier options in lists of snacks would be another area to look at as well. (Wendy, FG6) | |
| Participants ability to make healthier food choices | |||
| Recognising healthier alternatives | 27 | I think two things that are relevant to all people, irrespective of their energy requirements, are the need to eat a variety of food, and to make healthy choices within those food groups, and that’s applicable to all. But I think that fundamental concept of so many groups of foods, healthy choices within, you can apply that universally. (Sam, FG3) | |
| Adapting a recipe | 2 | Or you could do something specific like how would you increase the fibre in this meal or reduce the saturated fat in this meal? (Wendy, FG6) | |
| Demographics | |||
| General (Age, sex, education level, lifestyle factors, diets followed) | 10 | So whenever you do any sort of survey the demographics of that group is really important. (Irene, FG5) | |
| Knowledge of the individual’s beliefs and culture | 10 | Yeah from the point of view of setting up the literacy tool, you probably have to look at peoples’ source of belief in working with individuals. I mean who have they believed and why? But looking at their belief system I think is probably the most important thing if you’re going to get through to an individual. (Sonia, FG4) |
| Theme | Code | Number of References † | Quotation ‡ |
|---|---|---|---|
| Visual representation | |||
| Interactive animations | 30 | So the drag and drop concept is an interesting one, provided that—two things: one that the drag and drop components were in meaningful portions of the way people eat it, or prepare it. So for example, is this a half a mango if they’re going to have a serve, or how much meat, or the vegetables, or the pasta. And then for the second part, being that if we want to enable them or increase their knowledge, is that within any group, or what you’re serving, is there a good, better, best. And if I choose this meat verses that meat, understanding the impact of that, and then being able to see it, on what that would do for their nutritional status. (Sarah, FG3) | |
| Presentation of mixed foods § | 30 | And I think more broadly, part of the issue is that when it comes to nutrition guidelines or Australian Guide to Healthy Eating or dietetic advice in general, a lot of it is based around assembling meals from scratch, like one would do in one’s kitchen. But a lot of people’s experience with food is like at a food hall, where they go when meals are already prepared for them. So the advice that they might have been given and how to apply it, is just met with a huge disconnect, so it’s not simple. (Sam, FG3) | |
| Practical suggestions on presentation and assessment | 22 | The other thing you might want to look into (name) is the whole area of infographics, so the style of the way—it could still be a multiple choice question but you can say a lot more of the question with a visual infographic which is asking the question not just the responses as well. Very clever infographic designers these days can turn one very long, long question into a quick infographic that poses the same thing. (Samantha, FG4) | |
| Food images | 16 | Make sure it’s good food photography and when you’re showcasing even from one question to the next, that it’s shot in a way that the portions don’t distort. I think that often we see—we certainly want real food images, so real food photography not drawn pictures and trying to make sure that the portion sizes are all in the same proportion as you move through the questionnaire. (Samantha, FG4) | |
| Audio | |||
| General | 5 | I think it would be useful, even—I don’t know, but if you have people with visual difficulties as well then the sound would be good for that. (Rachel, FG6) | |
| Specific languages available | 2 | It speaks and you’ve got the pictures of the foods but all languages actually sound, audio and in the language of choice. (Fran, FG1) | |
| Other features | |||
| Other ways to assess (non audio-visual) | 7 | Well personally I’ve always been in favour of the food frequency questionnaire approach at a macro level because it’s certainly can provide an opportunity for a ranking score that you can do just to give somebody some feedback on how they rank in terms of food choice. (Diane, FG5) | |
| Use language and concepts suitable to the audience | 6 | My experience with English as a second language, it’s not always the ESL * understand the word ‘serve’. In fact they can get confused, that they think a serve of fruit is a whole mango, or a whole rockmelon. So we use the word ‘portion’. (Sarah, FG3) | |
| Focus on foods not nutrients | 5 | Where you get your macronutrients from. It seems so basic to us but you do get people just unsure where their protein’s coming from or which foods are the ones that have the most effect on blood glucose. (Fran, FG1) | |
| Be explicit | 3 | The information we communicate is not actually helpful to people, because the other thing probably that I’d like to add, is that we spend a lot of time telling people why, why, why, why, justifying why, why, why. They don’t really care, they’re just tell me what to do. (Danielle, FG3) | |
| Provide feedback | 2 | If it’s going to be an online tool it’s got to be interactive with immediate feedback. (Diane, FG5) | |
| Be non-judgemental | 1 | So we need to get a much better pattern of what people are doing and to do that I think we have to do it in a very non-judgmental way or we won’t get the information. (Sonia, FG4) | |
| Use of examples | 1 | Well they’ve given all of the examples of food that would illustrate what they mean. (Fran, FG1) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassar, A.M.; Denyer, G.S.; O’Connor, H.T.; Gifford, J.A. A Qualitative Investigation to Underpin the Development of an Electronic Tool to Assess Nutrition Literacy in Australian Adults. Nutrients 2018, 10, 251. https://doi.org/10.3390/nu10020251
Cassar AM, Denyer GS, O’Connor HT, Gifford JA. A Qualitative Investigation to Underpin the Development of an Electronic Tool to Assess Nutrition Literacy in Australian Adults. Nutrients. 2018; 10(2):251. https://doi.org/10.3390/nu10020251
Chicago/Turabian StyleCassar, Alyssa M, Gareth S Denyer, Helen T O’Connor, and Janelle A Gifford. 2018. "A Qualitative Investigation to Underpin the Development of an Electronic Tool to Assess Nutrition Literacy in Australian Adults" Nutrients 10, no. 2: 251. https://doi.org/10.3390/nu10020251