l-Carnitine Supplementation in Older Women. A Pilot Study on Aging Skeletal Muscle Mass and Function


Abstract
:1. Introduction
2. Materials and Methods
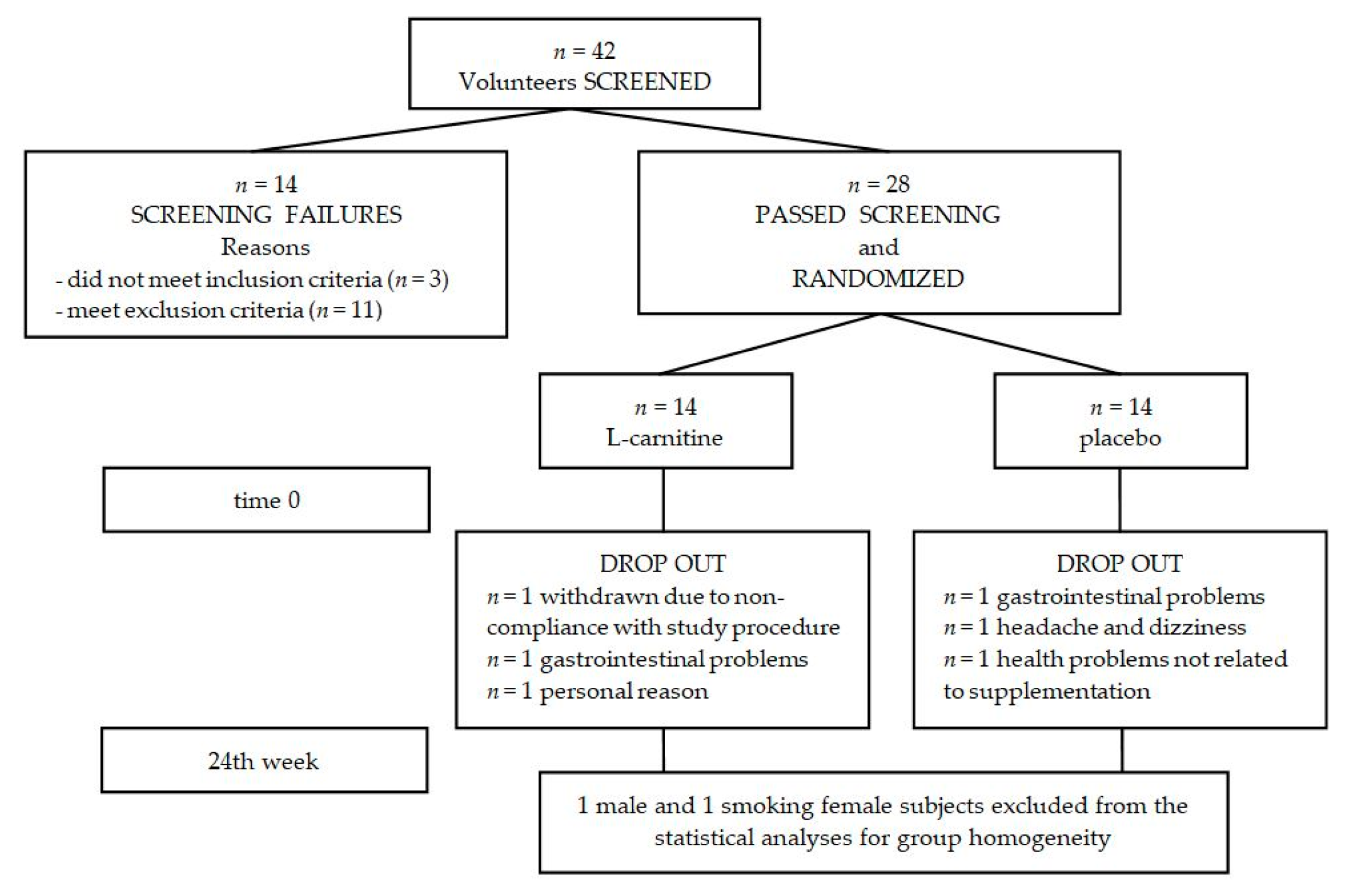
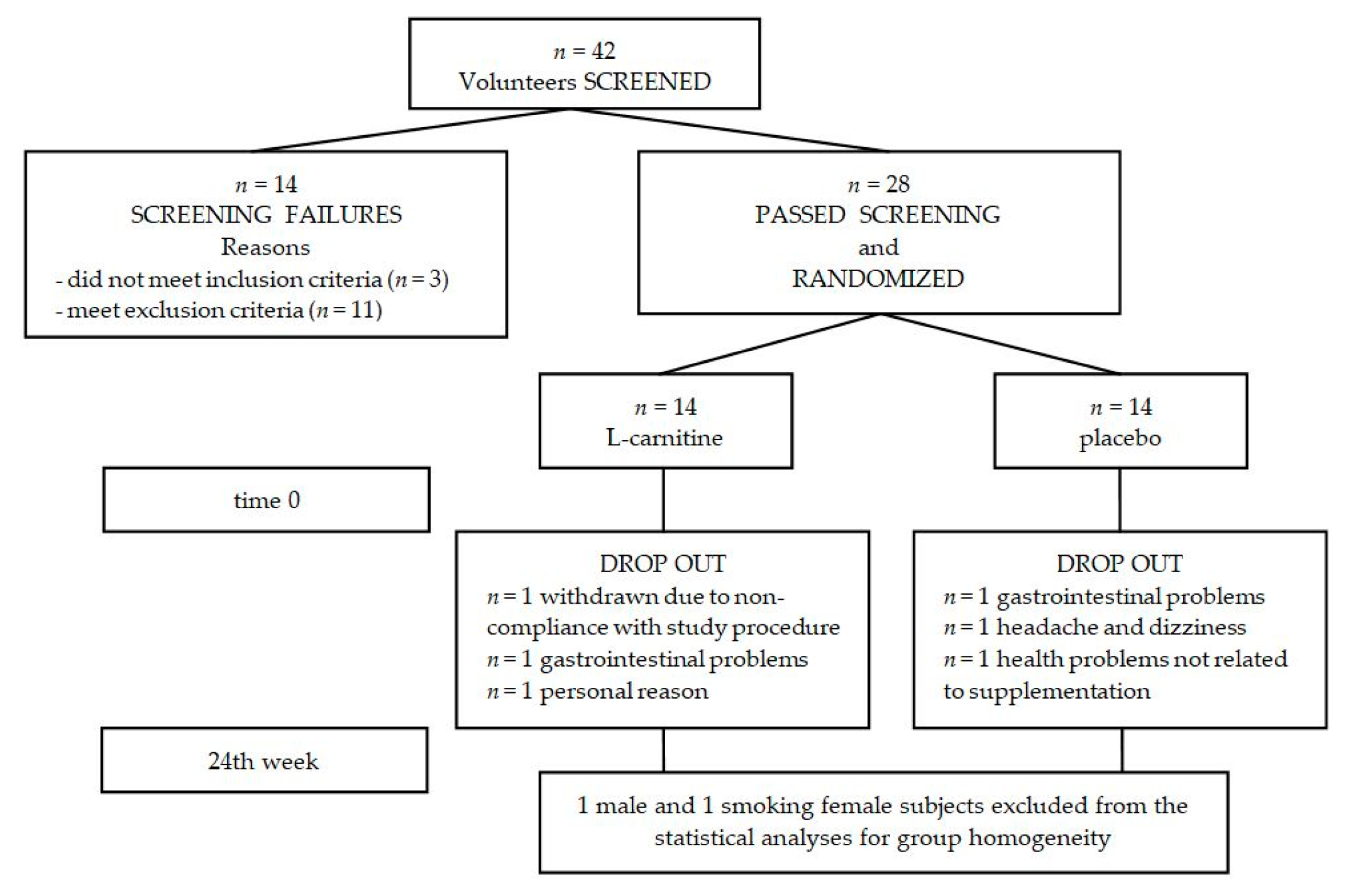
2.1. Subjects
2.2. Study Procedure
2.3. Anthropometric Measurements
2.4. Blood Sampling
2.5. Biochemical Determination
2.6. Skeletal Muscle Strength Test
2.7. Nutritional and Physical Activity Habits
- F0—never,
- F1—occasionally,
- F2—several times per year,
- F3—several times per month,
- F4—2–5 times per week,
- F5—6–7 times per week.
2.8. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zamboni, M.; Zoico, E.; Scartezzini, T.; Mazzali, G.; Tosoni, P.; Zivelonghi, A.; Gallagher, D.; de Pergola, G.; Di Francesco, V.; Bosello, O. Body composition changes in stable-weight elderly subjects: The effect of sex. Aging Clin. Exp. Res. 2003, 15, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Coppack, S.W. Pro-inflammatory cytokines and adipose tissue. Proc. Nutr. Soc. 2001, 60, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Roubenoff, R.; Harris, T.B.; Abad, L.W.; Wilson, P.W.; Dallal, G.E.; Dinarello, C.A. Monocyte cytokine production in an elderly population: Effect of age and inflammation. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1998, 53, M20–M26. [Google Scholar] [CrossRef]
- Budui, S.L.; Rossi, A.P.; Zamboni, M. The pathogenetic bases of sarcopenia. Clin. Cases Miner. Bone Metab. 2015, 12, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Costamagna, D.; Costelli, P.; Sampaolesi, M.; Penna, F. Role of inflammation in muscle homeostasis and myogenesis. Med. Inflamm. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Meadows, K.A.; Holly, J.M.; Stewart, C.E. Tumor necrosis factor-alpha-induced apoptosis is associated with suppression of insulin-like growth factor binding protein-5 secretion in differentiating murine skeletal myoblasts. J. Cell. Physiol. 2000, 183, 330–337. [Google Scholar] [CrossRef]
- Sharples, A.P.; Al-Shanti, N.; Stewart, C.E. C2 and C2C12 murine skeletal myoblast models of atrophic and hypertrophic potential: Relevance to disease and ageing? J. Cell. Physiol. 2010, 225, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Girven, M.; Dugdale, H.F.; Owens, D.J.; Hughes, D.C.; Stewart, C.E.; Sharples, A.P. l-glutamine improves skeletal muscle cell differentiation and prevents myotube atrophy after cytokine (TNF-α) stress via reduced p38 MAPK signal transduction. J. Cell. Physiol. 2016, 231, 2720–2732. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.P.; Chen, Y.; John, J.; Moylan, J.; Jin, B.; Mann, D.L.; Reid, M.B. TNF-α acts via p38 MAPK to stimulate expression of the ubiquitin ligase atrogin1/MAFbx in skeletal muscle. FASEB J. 2005, 19, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-α with muscle mass and muscle strength in elderly men and women: The health ABC study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef]
- Cesari, M.; Penninx, B.W.; Pahor, M.; Lauretani, F.; Corsi, A.M.; Rhys Williams, G.; Guralnik, J.M.; Ferrucci, L. Inflammatory markers and physical performance in older persons: The InCHIANTI study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, 242–248. [Google Scholar] [CrossRef]
- Penninx, B.W.; Kritchevsky, S.B.; Newman, A.B.; Nicklas, B.J.; Simonsick, E.M.; Rubin, S.; Nevitt, M.; Visser, M.; Harris, T.; Pahor, M. Inflammatory markers and incident mobility limitation in the elderly. J. Am. Geriatr. Soc. 2004, 52, 1105–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Visser, M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am. J. Med. 2006, 119, e9–e17. [Google Scholar] [CrossRef] [PubMed]
- Bucci, L.; Yani, S.L.; Fabbri, C.; Bijlsma, A.Y.; Maier, A.B.; Meskers, C.G.; Narici, M.V.; Jones, D.A.; McPhee, J.S.; Seppet, E.; et al. Circulating levels of adipokines and IGF-1 are associated with skeletal muscle strength of young and old healthy subjects. Biogerontology 2013, 14, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Bezkorovainy, A. Carnosine, carnitine, and Vladimir Gulevich. J. Chem. Educ. 1974, 51, 652–654. [Google Scholar] [CrossRef] [PubMed]
- Winter, B.K.; Fiskum, G.; Gallo, L.L. Effects of l-carnitine on serum triglyceride and cytokine levels in rat models of cachexia and septic shock. Br. J. Cancer 1995, 72, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Izgut-Uysal, V.N.; Agac, A.; Derin, N. Effect of l-carnitine on carrageenan-induced inflammation in aged rats. Gerontology 2003, 49, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Demiroren, K.; Dogan, Y.; Kocamaz, H.; Ozercan, I.H.; Ilhan, S.; Ustundag, B.; Bahcecioglu, I.H. Protective effects of l-carnitine, N-acetylcysteine and genistein in an experimental model of liver fibrosis. Clin. Res. Hepatol. Gastroenterol. 2014, 38, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Zhang, Z.; Zhang, Y.; Wu, J.; Yu, L.; Liu, S. l-carnitine ameliorates the liver inflammatory response by regulating carnitine palmitoyltransferase I-dependent PPARγ signaling. Mol. Med. Rep. 2016, 13, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Lin, J.S.; Lin, Y.C.; Lin, P.T. Antiinflammatory effects of l-carnitine supplementation (1000 mg/d) in coronary artery disease patients. Nutrition 2015, 31, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Ringseis, R.; Koc, A.; Lukas, I.; Kluge, H.; Eder, K. Supplementation with l-carnitine downregulates genes of the ubiquitin proteasome system in the skeletal muscle and liver of piglets. Animal 2012, 6, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Couturier, A.; Haferkamp, M.; Most, E.; Eder, K. Supplementation of carnitine leads to an activation of the IGF-1/PI3K/Akt signalling pathway and down regulates the E3 ligase MuRF1 in skeletal muscle of rats. Nutr. Metab. 2013, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Costell, M.; O’Connor, J.E.; Grisolia, S. Age-dependent decrease of carnitine content in muscle of mice and humans. Biochem. Biophys. Res. Commun. 1989, 161, 1135–1143. [Google Scholar] [CrossRef]
- Stephens, F.B.; Constantin-Teodosiu, D.; Laithwaite, D.; Simpson, E.J.; Greenhaff, P.L. Insulin stimulates l-carnitine accumulation in human skeletal muscle. FASEB J. 2006, 20, 377–379. [Google Scholar] [CrossRef] [PubMed]
- Wall, B.T.; Stephens, F.B.; Constantin-Teodosiu, D.; Marimuthu, K.; Macdonald, I.A.; Greenhaff, P.L. Chronic oral ingestion of l-carnitine and carbohydrate increases muscle carnitine content and alters muscle fuel metabolism during exercise in humans. J. Physiol. 2011, 589, 963–973. [Google Scholar] [CrossRef] [PubMed]
- Ziemann, E.; Olek, R.A.; Grzywacz, T.; Antosiewicz, J.; Kujach, S.; Luszczyk, M.; Smaruj, M.; Sledziewska, E.; Laskowski, R. Whole-body cryostimulation as an effective method of reducing low-grade inflammation in obese men. J. Physiol. Sci. 2013, 63, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Grinberga, S.; Dambrova, M.; Latkovskis, G.; Strele, I.; Konrade, I.; Hartmane, D.; Sevostjanovs, E.; Liepinsh, E.; Pugovics, O. Determination of trimethylamine-N-oxide in combination with l-carnitine and γ-butyrobetaine in human plasma by UPLC/MS/MS. BMC 2015, 29, 1670–1674. [Google Scholar] [PubMed]
- Ossowski, Z.M.; Skrobot, W.; Aschenbrenner, P.; Cesnaitiene, V.J.; Smaruj, M. Effects of short-term Nordic walking training on sarcopenia-related parameters in women with low bone mass: A preliminary study. Clin. Interv. Aging 2016, 11, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Goodpaster, B.H.; Carlson, C.L.; Visser, M.; Kelley, D.E.; Scherzinger, A.; Harris, T.B.; Stamm, E.; Newman, A.B. Attenuation of skeletal muscle and strength in the elderly: The health ABC study. J. Appl. Physiol. 2001, 90, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Steiber, A.; Kerner, J.; Hoppel, C.L. Carnitine: A nutritional, biosynthetic, and functional perspective. Mol. Asp. Med. 2004, 25, 455–473. [Google Scholar] [CrossRef] [PubMed]
- Kasielski, M.; Eusebio, M.O.; Pietruczuk, M.; Nowak, D. The relationship between peripheral blood mononuclear cells telomere length and diet-unexpected effect of red meat. Nutr. J. 2016, 15, 68. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. Spreadsheets for analysis of controlled trials, with adjustment for a subject characteristic. Sportscience 2006, 10, 46–50. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Ringseis, R.; Keller, J.; Eder, K. Mechanisms underlying the anti-wasting effect of l-carnitine supplementation under pathologic conditions: Evidence from experimental and clinical studies. Eur. J. Nutr. 2013, 52, 1421–1442. [Google Scholar] [CrossRef] [PubMed]
- Pooyandjoo, M.; Nouhi, M.; Shab-Bidar, S.; Djafarian, K.; Olyaeemanesh, A. The effect of (l-)carnitine on weight loss in adults: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, F.B.; Coswig, V.S.; Galliano, L.M. Comment on ‘the effect of (l-)carnitine on weight loss in adults: A systematic review and meta-analysis of randomized controlled trials’. Obes. Rev. 2017, 18, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Maffioli, P.; Salvadeo, S.A.; Ferrari, I.; Gravina, A.; Mereu, R.; D’Angelo, A.; Palumbo, I.; Randazzo, S.; Cicero, A.F. Effects of combination of sibutramine and l-carnitine compared with sibutramine monotherapy on inflammatory parameters in diabetic patients. Metab. Exp. 2011, 60, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Maffioli, P.; Ferrari, I.; D’Angelo, A.; Fogari, E.; Palumbo, I.; Randazzo, S.; Cicero, A.F. Comparison between orlistat plus l-carnitine and orlistat alone on inflammation parameters in obese diabetic patients. Fundam. Clin. Pharmacol. 2011, 25, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, M.; Gargante, M.P.; Russo, C.; Antic, T.; Vacante, M.; Avitabile, T.; Li Volti, G.; Galvano, F. l-carnitine supplementation to diet: A new tool in treatment of nonalcoholic steatohepatitis—A randomized and controlled clinical trial. Am. J. Gastroenterol. 2010, 105, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, M.; Cammalleri, L.; Gargante, M.P.; Vacante, M.; Colonna, V.; Motta, M. l-carnitine treatment reduces severity of physical and mental fatigue and increases cognitive functions in centenarians: A randomized and controlled clinical trial. Am. J. Clin. Nutr. 2007, 86, 1738–1744. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A. Effect of l-carnitine supplementation on circulating C-reactive protein levels: A systematic review and meta-analysis. J. Med. Biochem. 2015, 34, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Hakeshzadeh, F.; Tabibi, H.; Ahmadinejad, M.; Malakoutian, T.; Hedayati, M. Effects of l-carnitine supplement on plasma coagulation and anticoagulation factors in hemodialysis patients. Ren. Fail. 2010, 32, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Shakeri, A.; Tabibi, H.; Hedayati, M. Effects of l-carnitine supplement on serum inflammatory cytokines, c-reactive protein, lipoprotein (a), and oxidative stress in hemodialysis patients with Lp (a) hyperlipoproteinemia. Hemodial. Int. 2010, 14, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Malek Mahdavi, A.; Mahdavi, R.; Kolahi, S. Effects of l-carnitine supplementation on serum inflammatory factors and matrix metalloproteinase enzymes in females with knee osteoarthritis: A randomized, double-blind, placebo-controlled pilot study. J. Am. Coll. Nutr. 2016, 35, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Rafraf, M.; Karimi, M.; Jafari, A. Effect of l-carnitine supplementation in comparison with moderate aerobic training on serum inflammatory parameters in healthy obese women. J. Sports Med. Phys. Fit. 2015, 55, 1363–1370. [Google Scholar]
- Calvani, R.; Joseph, A.M.; Adhihetty, P.J.; Miccheli, A.; Bossola, M.; Leeuwenburgh, C.; Bernabei, R.; Marzetti, E. Mitochondrial pathways in sarcopenia of aging and disuse muscle atrophy. Biol. Chem. 2013, 394, 393–414. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.S.; Kelleher, A.R.; Kimball, S.R. Regulation of muscle protein synthesis and the effects of catabolic states. Int. J. Biochem. Cell Boil. 2013, 45, 2147–2157. [Google Scholar] [CrossRef] [PubMed]
- Doberenz, J.; Birkenfeld, C.; Kluge, H.; Eder, K. Effects of l-carnitine supplementation in pregnant sows on plasma concentrations of insulin-like growth factors, various hormones and metabolites and chorion characteristics. J. Anim. Physiol. Anim. Nutr. 2006, 90, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Rommel, C.; Bodine, S.C.; Clarke, B.A.; Rossman, R.; Nunez, L.; Stitt, T.N.; Yancopoulos, G.D.; Glass, D.J. Mediation of IGF-1-induced skeletal myotube hypertrophy by PI(3)K/Akt/mTOR and PI(3)k/Akt/GSK3 pathways. Nat. Cell Boil. 2001, 3, 1009–1013. [Google Scholar] [CrossRef] [PubMed]
- Bodine, S.C.; Stitt, T.N.; Gonzalez, M.; Kline, W.O.; Stover, G.L.; Bauerlein, R.; Zlotchenko, E.; Scrimgeour, A.; Lawrence, J.C.; Glass, D.J.; et al. Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo. Nat. Cell Boil. 2001, 3, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Stitt, T.N.; Drujan, D.; Clarke, B.A.; Panaro, F.; Timofeyva, Y.; Kline, W.O.; Gonzalez, M.; Yancopoulos, G.D.; Glass, D.J. The IGF-1/PI3K/Akt pathway prevents expression of muscle atrophy-induced ubiquitin ligases by inhibiting FOXO transcription factors. Mol. Cell 2004, 14, 395–403. [Google Scholar] [CrossRef]
- Evans, M.; Guthrie, N.; Pezzullo, J.; Sanli, T.; Fielding, R.A.; Bellamine, A. Efficacy of a novel formulation of l-carnitine, creatine, and leucine on lean body mass and functional muscle strength in healthy older adults: A randomized, double-blind placebo-controlled study. Nutr. Metab. 2017, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.; Heywood, L.; Rutherford, S.; Cobbold, C. Creatine supplementation: Can it improve quality of life in the elderly without associated resistance training? Curr. Aging Sci. 2013, 6, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.R.; Tan, Z.J.; Zhang, Q.; Gui, Q.F.; Yang, Y.M. The effectiveness of leucine on muscle protein synthesis, lean body mass and leg lean mass accretion in older people: A systematic review and meta-analysis. Br. J. Nutr. 2015, 113, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Buckinx, F.; Rabenda, V.; Gillain, S.; Cavalier, E.; Slomian, J.; Petermans, J.; Reginster, J.Y.; Bruyere, O. The effects of vitamin D on skeletal muscle strength, muscle mass, and muscle power: A systematic review and meta-analysis of randomized controlled trials. J. Clin. Endocrinol. Metab. 2014, 99, 4336–4345. [Google Scholar] [CrossRef] [PubMed]
- Young, A.; Stokes, M.; Crowe, M. Size and strength of the quadriceps muscles of old and young women. Eur. J. Clin. Investing. 1984, 14, 282–287. [Google Scholar] [CrossRef]
- Hughes, V.A.; Frontera, W.R.; Wood, M.; Evans, W.J.; Dallal, G.E.; Roubenoff, R.; Fiatarone Singh, M.A. Longitudinal muscle strength changes in older adults: Influence of muscle mass, physical activity, and health. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, B209–B217. [Google Scholar] [CrossRef]
- Silverio, R.; Laviano, A.; Rossi Fanelli, F.; Seelaender, M. l-carnitine and cancer cachexia: Clinical and experimental aspects. J. Cachexia Sarcopenia Muscle 2011, 2, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Prado, R.; Esteras, R.; Perez-Gomez, M.V.; Gracia-Iguacel, C.; Gonzalez-Parra, E.; Sanz, A.B.; Ortiz, A.; Sanchez-Nino, M.D. Nutrients turned into toxins: Microbiota modulation of nutrient properties in chronic kidney disease. Nutrients 2017, 9, 489. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Placebo | l-Carnitine | ||
|---|---|---|---|---|
| Mean ± SD (Standard Deviation) | Mean ± SD | |||
| Age (years) | 66.4 ± 1.3 | 67.8 ± 2.3 | ||
| Height (cm) | 162 ± 5.3 | 159 ± 5.4 | ||
| BMI (kg/m2) | 26.5 ± 4.4 | 27.5 ± 4.5 | ||
| n | % | n | % | |
| Education level | ||||
| Primary | 0 | 0 | 0 | 0 |
| Secondary | 2 | 22.2 | 4 | 36.4 |
| High | 7 | 77.8 | 7 | 63.6 |
| Physical activity | ||||
| Low | 0 | 0 | 0 | 0 |
| Moderate | 4 | 44.4 | 6 | 54.5 |
| High | 5 | 55.6 | 5 | 45.5 |
| median | range | median | range | |
| Meat consumption | ||||
| Poultry | F4 | F3–F4 | F4 | F0–F4 |
| Pork | F2 | F0–F3 | F3 | F0–F4 |
| Beef | F1 | F0–F3 | F2 | F0–F4 |
| Fish | F3 | F1–F4 | F2 | F1–F4 |
| Lamb | F0 | F0–F3 | F0 | F0–F3 |
| Venison | F0 | F0–F3 | F0 | F0–F1 |
| Horseflesh | F0 | F0–F2 | F0 | F0–F1 |
| Variables | Group | Baseline Mean ± SD | Observed Change Mean ± SD | Adjusted Change a Mean ± SD | Adjusted Effect b | |
|---|---|---|---|---|---|---|
| Mean; CL | Inference | |||||
| BM (kg) | placebo | 69.7 ± 12.1 | −0.3 ± 2.8% | −0.3 ± 2.1% | 0.5%; ±1.9% | trivial † |
| l-carnitine | 69.8 ± 12.9 | 0.2 ± 2.9% | 0.2 ± 2.9% | |||
| FFM (kg) | placebo | 45.8 ± 6.7 | −1.6 ± 5.2% | −1.1 ± 3.7% | 0.7%; ±2.6% | trivial * |
| l-carnitine | 43.9 ± 4.6 | 0.0 ± 3.5% | −0.4 ± 2.8% | |||
| SMM (kg) | placebo | 24.9 ± 4.1 | −1.9 ± 6.4% | −1.3 ± 4.4% | 1.2%; ±3.2% | trivial * |
| l-carnitine | 23.9 ± 2.7 | −0.2 ± 3.8% | −0.1 ± 3.2% | |||
| Variables | Group | Baseline Mean ± SD | Observed Change Mean ± SD | Adjusted Change a Mean ± SD | Adjusted Effect b | |
|---|---|---|---|---|---|---|
| Mean; CL | Inference | |||||
| free carnitine (µmol/L) | placebo | 39.5 ± 3.7 | 10 ± 11% | 8 ± 6% | 13%; ±5.8% | moderate † |
| l-carnitine | 41.1 ± 6.4 | 22 ± 9% | 22 ± 8% | |||
| CRP (mg/L) | placebo | 1.8 ± 0.8 | −6 ± 15% | −4.7 ± 15% | 21%; ±37% | unclear |
| l-carnitine | 2.6 ± 1.1 | 8 ± 68% | 16 ± 65% | |||
| IL-6 (ng/L) | placebo | 1.8 ± 0.7 | −10 ± 23% | −13 ± 20% | 4.9%; ±22% | trivial * |
| l-carnitine | 2.2 ± 1.1 | −11 ± 42% | −8.2 ± 32% | |||
| TNF (ng/L) | placebo | 0.56 ± 0.26 | 14 ± 70% | 12 ± 68% | 9.0%; ±50% | trivial * |
| l-carnitine | 0.58 ± 0.32 | 24 ± 82% | 28 ± 38% | |||
| IGF-1 (µg/L) | placebo | 78 ± 19 | −10 ± 12% | −10 ± 13% | 1.8%; ±16% | trivial * |
| l-carnitine | 69 ± 15 | −6 ± 28% | −8 ± 28% | |||
| Variables | Group | Baseline Mean ± SD | Observed Change Mean ± SD | Adjusted Change a Mean ± SD | Adjusted Effect b | |
|---|---|---|---|---|---|---|
| Mean; CL | Inference | |||||
| TW extension (J/kg) | placebo | 76 ± 15 | 7.4 ± 26% | 5.7 ± 8.3% | 5.6%; ±7.1% | trivial * |
| l-carnitine | 78 ± 11 | 11 ± 13% | 12 ± 9.5% | |||
| TW flexion (J/kg) | placebo | 43 ± 17 | 9.4 ± 40% | 13 ± 13% | −2.9%; ±13% | trivial * |
| l-carnitine | 36 ± 9 | 14 ± 34% | 9.7 ± 23% | |||
| APT extension (Nm/kg) | placebo | 12.0 ± 2.6 | 4.7 ± 20% | 1.9 ± 9.7% | 3.0%; ±9.0% | unclear |
| l-carnitine | 12.8 ± 2.3 | 2.7 ± 18% | 5.0 ± 13% | |||
| APT flexion (Nm/kg) | placebo | 6.8 ± 2.6 | 4.9 ± 26% | 7.0 ± 7.8% | −4.2%; ±9.0% | trivial * |
| l-carnitine | 5.9 ± 1.1 | 5.0 ± 22% | 2.6 ± 16% | |||
| AP extension (W/kg) | placebo | 8.3 ± 2.0 | 6.3 ± 25% | 3.9 ± 6.2% | 1.4%; ±6.8% | trivial † |
| l-carnitine | 8.6 ± 1.4 | 3.3 ± 18% | 5.4 ± 11% | |||
| AP flexion (W/kg) | placebo | 4.4 ± 1.7 | 10 ± 40% | 14 ± 12% | −7.1%; ±9.7% | trivial † |
| l-carnitine | 3.9 ± 1.4 | 12 ± 83% | 5.8 ± 17% | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawicka, A.K.; Hartmane, D.; Lipinska, P.; Wojtowicz, E.; Lysiak-Szydlowska, W.; Olek, R.A. l-Carnitine Supplementation in Older Women. A Pilot Study on Aging Skeletal Muscle Mass and Function. Nutrients 2018, 10, 255. https://doi.org/10.3390/nu10020255
Sawicka AK, Hartmane D, Lipinska P, Wojtowicz E, Lysiak-Szydlowska W, Olek RA. l-Carnitine Supplementation in Older Women. A Pilot Study on Aging Skeletal Muscle Mass and Function. Nutrients. 2018; 10(2):255. https://doi.org/10.3390/nu10020255
Chicago/Turabian StyleSawicka, Angelika K., Dace Hartmane, Patrycja Lipinska, Ewa Wojtowicz, Wieslawa Lysiak-Szydlowska, and Robert A. Olek. 2018. "l-Carnitine Supplementation in Older Women. A Pilot Study on Aging Skeletal Muscle Mass and Function" Nutrients 10, no. 2: 255. https://doi.org/10.3390/nu10020255