Higher Dietary Magnesium Intake and Higher Magnesium Status Are Associated with Lower Prevalence of Coronary Heart Disease in Patients with Type 2 Diabetes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Study Procedures
2.4. Magnesium Measurements
2.5. Main Study Outcome
2.6. Statistics
3. Results
3.1. Association between Dietary Magnesium Intake, 24 h Urinary Magnesium Excretion, Plasma Magnesium Concentration, and the Prevalence of Coronary Heart Disease
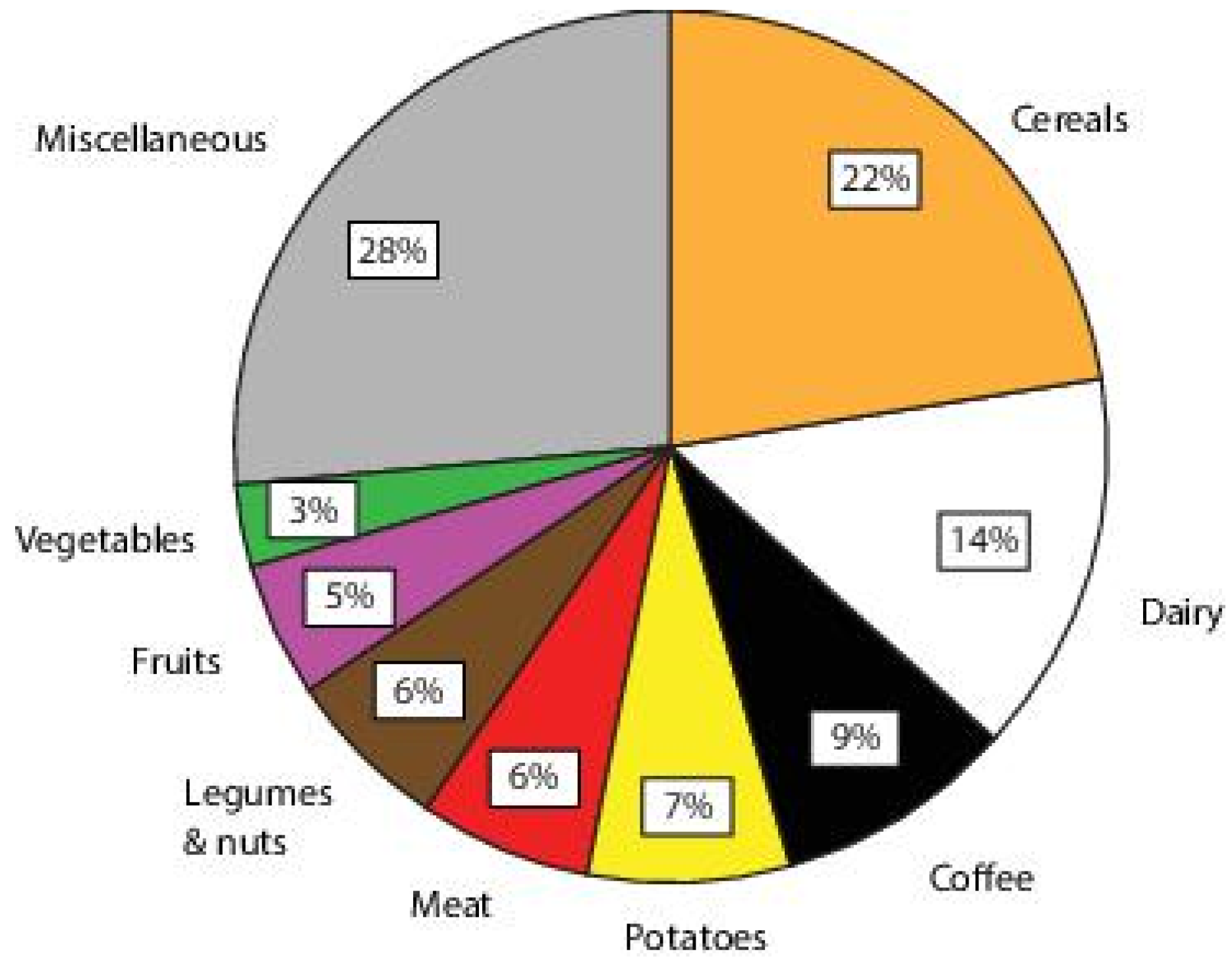
3.2. Analysis on Source of Magnesium Intake and Prevalence of CHD
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rana, J.S.; Liu, J.Y.; Moffet, H.H.; Jaffe, M.; Karter, A.J. Diabetes and Prior Coronary Heart Disease are Not Necessarily Risk Equivalent for Future Coronary Heart Disease Events. J. Gen. Intern. Med. 2016, 31, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes Mellitus, Fasting Blood Glucose Concentration, and Risk of Vascular Disease: A Collaborative Meta-Analysis of 102 Prospective Studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [PubMed]
- Chiuve, S.E.; Sun, Q.; Curhan, G.C.; Taylor, E.N.; Spiegelman, D.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Albert, C.M. Dietary and Plasma Magnesium and Risk of Coronary Heart Disease among Women. J. Am. Heart Assoc. 2013, 2, e000114. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; O’Donnell, C.J.; Jacques, P.F.; Meigs, J.B.; Hoffmann, U.; McKeown, N.M. Magnesium Intake is Inversely Associated with Coronary Artery Calcification: The Framingham Heart Study. JACC Cardiovasc. Imaging 2014, 7, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Joosten, M.M.; Gansevoort, R.T.; Mukamal, K.J.; van der Harst, P.; Geleijnse, J.M.; Feskens, E.J.; Navis, G.; Bakker, S.J.; PREVEND Study Group. Urinary and Plasma Magnesium and Risk of Ischemic Heart Disease. Am. J. Clin. Nutr. 2013, 97, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Posadas-Sanchez, R.; Posadas-Romero, C.; Cardoso-Saldana, G.; Vargas-Alarcon, G.; Villarreal-Molina, M.T.; Perez-Hernandez, N.; Rodriguez-Perez, J.M.; Medina-Urrutia, A.; Jorge-Galarza, E.; Juarez-Rojas, J.G.; et al. Serum Magnesium is Inversely Associated with Coronary Artery Calcification in the Genetics of Atherosclerotic Disease (GEA) Study. Nutr. J. 2016, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Hamano, T.; Nakano, C.; Obi, Y.; Matsui, I.; Kusunoki, Y.; Mori, D.; Oka, T.; Hashimoto, N.; Takabatake, Y.; et al. Association between Density of Coronary Artery Calcification and Serum Magnesium Levels among Patients with Chronic Kidney Disease. PLoS ONE 2016, 11, e0163673. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Xun, P.; Tang, Q.; Cai, W.; He, K. Circulating Magnesium Levels and Incidence of Coronary Heart Diseases, Hypertension, and Type 2 Diabetes Mellitus: A Meta-Analysis of Prospective Cohort Studies. Nutr. J. 2017, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary Magnesium Intake and the Risk of Cardiovascular Disease, Type 2 Diabetes, and all-Cause Mortality: A Dose-Response Meta-Analysis of Prospective Cohort Studies. BMC Med. 2016, 14, 210. [Google Scholar] [CrossRef] [PubMed]
- Gommers, L.M.; Hoenderop, J.G.; Bindels, R.J.; de Baaij, J.H. Hypomagnesemia in Type 2 Diabetes: A Vicious Circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.C.; Pham, P.M.; Pham, S.V.; Miller, J.M.; Pham, P.T. Hypomagnesemia in Patients with Type 2 Diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Han, H.; Li, M.; Liang, C.; Fan, Z.; Aaseth, J.; He, J.; Montgomery, S.; Cao, Y. Dose-Response Relationship between Dietary Magnesium Intake and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Regression Analysis of Prospective Cohort Studies. Nutrients 2016, 8, 739. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Meigs, J.B.; O’Donnell, C.J.; Jacques, P.F.; McKeown, N.M. Higher Magnesium Intake Reduces Risk of Impaired Glucose and Insulin Metabolism and Progression from Prediabetes to Diabetes in Middle-Aged Americans. Diabetes Care 2014, 37, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Liao, F.; Folsom, A.R.; Brancati, F.L. Is Low Magnesium Concentration a Risk Factor for Coronary Heart Disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 1998, 136, 480–490. [Google Scholar] [CrossRef]
- Peters, K.E.; Chubb, S.A.; Davis, W.A.; Davis, T.M. The Relationship between Hypomagnesemia, Metformin Therapy and Cardiovascular Disease Complicating Type 2 Diabetes: The Fremantle Diabetes Study. PLoS ONE 2013, 8, e74355. [Google Scholar] [CrossRef] [PubMed]
- Gant, C.M.; Binnenmars, S.H.; Berg, E.V.D.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Integrated Assessment of Pharmacological and Nutritional Cardiovascular Risk Management: Blood Pressure Control in the DIAbetes and LifEstyle Cohort Twente (DIALECT). Nutrients 2017, 9, 709. [Google Scholar] [CrossRef] [PubMed]
- Wendel-Vos, G.C.; Schuit, A.J.; Saris, W.H.; Kromhout, D. Reproducibility and Relative Validity of the Short Questionnaire to Assess Health-Enhancing Physical Activity. J. Clin. Epidemiol. 2003, 56, 1163–1169. [Google Scholar] [CrossRef]
- Feunekes, G.I.; Van Staveren, W.A.; De Vries, J.H.; Burema, J.; Hautvast, J.G. Relative and Biomarker-Based Validity of a Food-Frequency Questionnaire Estimating Intake of Fats and Cholesterol. Am. J. Clin. Nutr. 1993, 58, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Rijksinstituut voor Volksgezondheid en Milieu. NEVO-Tabel (Dutch Food Composition Table): Nederlands Voedingsstoffenbestand, version 4.0; Rijksinstituut voor Volksgezondheid en Milieu: Bilthoven, The Netherlands, 2013.
- Willett, W.C.; Stampfer, M. Implications of total energy intake for epidemiologic analyses. In Nutritional Epidemology; Willett, W.C., Ed.; Oxford University Press: New York, NY, USA, 1998; pp. 273–301. [Google Scholar]
- Zhang, W.; Iso, H.; Ohira, T.; Date, C.; Tamakoshi, A.; JACC Study Group. Associations of Dietary Magnesium Intake with Mortality from Cardiovascular Disease: The JACC Study. Atherosclerosis 2012, 221, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Van Rossum, C.; Fransen, H.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.; Ocke, M. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years; National Institute for Public Health and the Environment: Bilthoven, The Netherlands, 2011.
- Davies, B.E. The UK Geochemical Environment and Cardiovascular Diseases: Magnesium in Food and Water. Environ. Geochem. Health 2015, 37, 411–427. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Mokdad, A.H. Dietary Magnesium Intake in a National Sample of US Adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [CrossRef] [PubMed]
- Kurstjens, S.; de Baaij, J.H.; Bouras, H.; Bindels, R.J.; Tack, C.J.; Hoenderop, J.G. Determinants of Hypomagnesemia in Patients with Type 2 Diabetes Mellitus. Eur. J. Endocrinol. 2017, 176, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Grober, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [PubMed]
- McNair, P.; Christensen, M.S.; Christiansen, C.; Madsbad, S.; Transbol, I. Renal Hypomagnesaemia in Human Diabetes Mellitus: Its Relation to Glucose Homeostasis. Eur. J. Clin. Investig. 1982, 12, 81–85. [Google Scholar] [CrossRef]
- Rodriguez-Moran, M.; Guerrero-Romero, F. Oral Magnesium Supplementation Improves Insulin Sensitivity and Metabolic Control in Type 2 Diabetic Subjects: A Randomized Double-Blind Controlled Trial. Diabetes Care 2003, 26, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Schuchardt, J.P.; Hahn, A. Intestinal Absorption and Factors Influencing Bioavailability of Magnesium-an Update. Curr. Nutr. Food Sci. 2017, 13, 260–278. [Google Scholar] [CrossRef] [PubMed]
- Gant, C.M.; Binnenmars, S.H.; Harmelink, M.; Soedamah-Muthu, S.S.; Bakker, S.J.L.; Navis, G.J.; Laverman, G.D. Real-Life Achievement of Lipid-Lowering Treatment Targets in the DIAbetes and LifEstyle Cohort Twente: Systemic Assessment of Pharmacological and Nutritional Factors. Nutr. Diabetes 2018, in press. [Google Scholar]
- Zhu, X.; Zuo, L. Characterization of Oxygen Radical Formation Mechanism at Early Cardiac Ischemia. Cell Death Dis. 2013, 4, e787. [Google Scholar] [CrossRef] [PubMed]
- Keyzer, C.A.; Vermeer, C.; Joosten, M.M.; Knapen, M.H.; Drummen, N.E.; Navis, G.; Bakker, S.J.; de Borst, M.H. Vitamin K Status and Mortality After Kidney Transplantation: A Cohort Study. Am. J. Kidney Dis. 2015, 65, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Riphagen, I.J.; Keyzer, C.A.; Drummen, N.E.A.; de Borst, M.H.; Beulens, J.W.J.; Gansevoort, R.T.; Geleijnse, J.M.; Muskiet, F.A.J.; Navis, G.; Visser, S.T.; et al. Prevalence and Effects of Functional Vitamin K Insufficiency: The PREVEND Study. Nutrients 2017, 9, 1334. [Google Scholar] [CrossRef] [PubMed]
- Kieneker, L.M.; Gansevoort, R.T.; Mukamal, K.J.; de Boer, R.A.; Navis, G.; Bakker, S.J.; Joosten, M.M. Urinary Potassium Excretion and Risk of Developing Hypertension: The Prevention of Renal and Vascular End-Stage Disease Study. Hypertension 2014, 64, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Di Bella, G.; Brucato, V.; D’Angelo, D.; Damiani, P.; Monteverde, A.; Belvedere, M.; Dominguez, L.J. Serum Ionized Magnesium in Diabetic Older Persons. Metabolism 2014, 63, 502–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alesutan, I.; Tuffaha, R.; Auer, T.; Feger, M.; Pieske, B.; Lang, F.; Voelkl, J. Inhibition of Osteo/Chondrogenic Transformation of Vascular Smooth Muscle Cells by MgCl2 Via Calcium-Sensing Receptor. J. Hypertens. 2017, 35, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Kircelli, F.; Peter, M.E.; Sevinc Ok, E.; Celenk, F.G.; Yilmaz, M.; Steppan, S.; Asci, G.; Ok, E.; Passlick-Deetjen, J. Magnesium Reduces Calcification in Bovine Vascular Smooth Muscle Cells in a Dose-Dependent Manner. Nephrol. Dial. Transplant. 2012, 27, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Verduyn, S.C.; Vos, M.A.; van der Zande, J.; van der Hulst, F.F.; Wellens, H.J. Role of Interventricular Dispersion of Repolarization in Acquired Torsade-De-Pointes Arrhythmias: Reversal by Magnesium. Cardiovasc. Res. 1997, 34, 453–463. [Google Scholar] [CrossRef]
- Dibaba, D.T.; Xun, P.; Song, Y.; Rosanoff, A.; Shechter, M.; He, K. The Effect of Magnesium Supplementation on Blood Pressure in Individuals with Insulin Resistance, Prediabetes, or Noncommunicable Chronic Diseases: A Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2017, 106, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Temple, N.J.; La Vecchia, C.; Castellan, G.; Tavani, A.; Guercio, V. Mediterranean Diet and Cardiovascular Disease: A Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-Style Diet and Risk of Coronary Heart Disease and Stroke in Women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Zuo, L.; He, F.; Tinsley, G.M.; Pannell, B.K.; Ward, E.; Arciero, P.J. Comparison of High-Protein, Intermittent Fasting Low-Calorie Diet and Heart Healthy Diet for Vascular Health of the Obese. Front. Physiol. 2016, 7, 350. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Population | No CHD | CHD | p-Value | |||
|---|---|---|---|---|---|---|
| n | n = 450 | n = 350 (78%) | n = 100 (22%) | |||
| Patient characteristics | ||||||
| Age, years | 450 | 63 ± 9 | 62 ± 9 | 66 ± 7 | <0.001 | |
| Male, n (%) | 450 | 261 (58) | 190 (54) | 71 (71) | 0.003 | |
| Diabetes duration, years | 450 | 11 (7–18) | 11 (7–17) | 13 (7–20) | 0.15 | |
| Systolic blood pressure, mmHg | 449 | 136 ± 16 | 136 ± 16 | 136 ± 19 | 0.81 | |
| Diastolic blood pressure, mmHg | 449 | 74 ± 9 | 75 ± 9 | 72 ± 10 | 0.01 | |
| Heart rate, beats/min | 444 | 74 ± 13 | 75 ± 13 | 69 ± 11 | <0.001 | |
| Body surface area, m2 | 448 | 2.10 ± 0.22 | 2.10 ± 0.23 | 2.07 ± 0.19 | 0.27 | |
| Urinary creatinine excretion, µmol/24 h | 446 | 13.8 ± 4.8 | 13.8 ± 5.0 | 13.8 ± 4.2 | 0.97 | |
| Complications | ||||||
| Cerebrovascular disease, n (%) | 450 | 47 (11) | 87 (22) | 13 (27) | 0.44 | |
| Peripheral artery disease, n (%) | 450 | 44 (10) | 80 (20) | 20 (44) | <0.001 | |
| Retinopathy, n (%) | 447 | 106 (24) | 78 (23) | 32 (32) | 0.05 | |
| Neuropathy, n (%) | 450 | 157 (36) | 116 (33) | 46 (46) | 0.02 | |
| Diabetic nephropathy, n (%) | 446 | 183 (42) | 131 (38) | 58 (58) | <0.001 | |
| eGFR < 60 mL/min·1.73 m2 | 450 | 101 (23) | 74 (21) | 30 (30) | 0.06 | |
| Microalbuminuria, n (%) | 445 | 131 (30) | 92 (27) | 44 (44) | 0.001 | |
| Lifestyle | ||||||
| Body mass index, kg/m2 | 448 | 32.8 ± 6.2 | 33.1 ± 6.4 | 32.1 ± 5.6 | 0.15 | |
| Body mass index ≥ 30 kg/m2, n (%) | 448 | 290 (65) | 233 (67) | 57 (58) | 0.12 | |
| Smoking, former or current, n (%) | 450 | 306 (70) | 235 (67) | 78 (78) | 0.04 | |
| Alcohol | 424 | |||||
| No alcohol, n (%) | 148 (36) | 123 (37) | 32 (34) | 0.80 | ||
| 0–13 units per week, n (%) | 206 (50) | 159 (48) | 49 (52) | |||
| ≥14 units per week, n (%) | 61 (15) | 47 (14) | 14 (15) | |||
| Adherence guideline physical activity, n (%) | 433 | 249 (59) | 201 (60) | 52 (54) | 0.34 | |
| Pharmacological treatment | ||||||
| Insulin use, n (%) | 450 | 275 (63) | 218 (62) | 68 (68) | 0.30 | |
| Statin use, n (%) | 450 | 331 (76) | 254 (73) | 86 (86) | 0.006 | |
| Beta blocker treatment, n (%) | 450 | 202 (46) | 131 (37) | 77 (77) | <0.001 | |
| RAAS inhibition, n (%) | 450 | 289 (66) | 225 (64) | 73 (73) | 0.10 | |
| Calcium antagonists, n (%) | 450 | 98 (22) | 66 (19) | 36 (36) | <0.001 | |
| Thiazide diuretics, n (%) | 450 | 136 (31) | 108 (31) | 29 (29) | 0.72 | |
| Loop diuretics, n (%) | 450 | 75 (17) | 48 (14) | 33 (33) | <0.001 | |
| Number of antihypertensives | 450 | 2 (1–3) | 2 (1–3) | 3 (2–4) | <0.001 | |
| Magnesium parameters | ||||||
| Dietary magnesium intake *, mg/day | 438 | 305 ± 46 | 309 ± 47 | 292 ± 40 | 0.001 | |
| Urinary magnesium excretion, mmol/24 h | 402 | 3.94 ± 2.05 | 4.03 ± 2.05 | 3.66 ± 2.02 | 0.13 | |
| Plasma magnesium concentration, mmol/L | 432 | 0.77 ± 0.09 | 0.78 ± 0.08 | 0.76 ± 0.09 | 0.06 | |
| Hypomagnesemia, n (%) | 432 | 73 (17) | 53 (16) | 20 (20) | 0.35 | |
| Serum values | ||||||
| Total cholesterol, mmol/L | 447 | 4.0 ± 0.9 | 4.1 ± 0.9 | 3.8 ± 1.1 | 0.04 | |
| HDL cholesterol, mmol/L | 445 | 1.1 ± 0.3 | 1.2 ± 0.4 | 1.0 ± 0.3 | <0.001 | |
| LDL cholesterol, mmol/L | 428 | 2.0 ± 0.7 | 2.0 ± 0.7 | 1.9 ± 0.8 | 0.25 | |
| HbA1c, mmol/mol | 448 | 57 ± 12 | 57 ± 12 | 58 ± 12 | 0.43 | |
| Dietary intake | ||||||
| Total energy intake, kcal/day | 438 | 1922 ± 629 | 1904 ± 649 | 1932 ± 630 | 0.71 | |
| Urinary sodium excretion, mmol/24 h | 444 | 185 ± 79 | 183 ± 67 | 197 ± 84 | 0.14 | |
| Urinary potassium excretion, mmol/24 h | 439 | 77 ± 25 | 78 ± 26 | 77 ± 21 | 0.87 | |
| Calcium intake, mg/day | 438 | 969 ± 441 | 979 ± 467 | 905 ± 358 | 0.16 | |
| Fiber intake, g/day | 438 | 20.9 ± 6.6 | 20.8 ± 7.0 | 20.4 ± 6.1 | 0.60 | |
| Cholesterol, g/day | 438 | 194 ± 96 | 195 ± 101 | 188 ± 79 | 0.51 | |
| Total fat intake, g/day | 438 | 79 ± 39 | 78 ± 34 | 81 ± 34 | 0.52 | |
| Total protein intake, g/day | 438 | 79 ± 23 | 79 ± 24 | 76 ± 22 | 0.18 | |
| Total carbohydrate intake, g/day | 438 | 207 ± 69 | 205 ± 72 | 209 ± 67 | 0.61 | |
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Trend | |
|---|---|---|---|---|---|
| Dietary Mg intake *, mg/day | 254 ± 25 | 291 ± 7 | 315 ± 8 | 361 ± 39 | |
| n cases/n total | 33/109 | 25/110 | 23/110 | 13/109 | |
| Model 1 a | 1.00 | 0.71 (0.42, 1.22) | 0.64 (0.37, 1.10) | 0.40 (0.20, 0.77) | 0.005 |
| Model 2 b | 1.00 | 0.72 (0.42, 1.23) | 0.69 (0.40, 1.21) | 0.42 (0.22, 0.82) | 0.01 |
| Model 3 c | 1.00 | 0.71 (0.41, 1.23) | 0.72 (0.41, 1.27) | 0.40 (0.20, 0.79) | 0.01 |
| Urinary Mg excretion, mmol/24 h | 1.81 ± 0.63 | 3.05 ± 0.32 | 4.32 ± 0.57 | 6.64 ± 1.75 | |
| n cases/n total | 24/101 | 24/100 | 19/101 | 15/100 | |
| Model 1 a | 1.00 | 0.95 (0.54, 1.67) | 0.73 (0.39, 1.35) | 0.63 (0.33, 1.19) | 0.24 |
| Model 2 b | 1.00 | 1.28 (0.71, 2.30) | 0.96 (0.51, 1.82) | 0.74 (0.39, 1.42) | 0.33 |
| Model 3 c | 1.00 | 1.27 (0.70, 2.30) | 0.85 (0.44, 1.65) | 0.63 (0.32, 1.26) | 0.13 |
| Plasma Mg concentration, mmol/L | 0.67 ± 0.06 | 0.75 ± 0.02 | 0.80 ± 0.02 | 0.88 ± 0.04 | |
| n cases/n total | 29/113 | 22/106 | 27/111 | 16/102 | |
| Model 1 a | 1.00 | 0.91 (0.52, 1.60) | 1.03 (0.60, 1.77) | 0.60 (0.31, 1.14) | 0.15 |
| Model 2 b | 1.00 | 0.91 (0.51, 1.62) | 1.09 (0.63, 1.89) | 0.58 (0.30, 1.12) | 0.17 |
| Model 3 c | 1.00 | 0.91 (0.51, 1.63) | 1.12 (0.65, 1.94) | 0.62 (0.32, 1.20) | 0.26 |
| Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|
| Source of magnesium intake | PR (95% CI) | PR (95% CI) | PR (95% CI) |
| Magnesium intake from cereals *, 10 mg/day | 1.02 (0.94, 1.10) | 1.02 (0.94, 1.10) | 0.95 (0.86, 1.05) |
| Magnesium intake from dairy *, 10 mg/day | 0.95 (0.87, 1.03) | 0.95 (0.87, 1.03) | 0.92 (0.84, 1.01) |
| Magnesium intake from coffee *, 10 mg/day | 0.95 (0.83, 1.06) | 0.95 (0.83, 1.08) | 0.96 (0.84, 1.10) |
| Magnesium intake from potatoes *, 10 mg/day | 1.03 (0.87, 1.22) | 1.02 (0.86, 1.21) | 0.97 (0.80, 1.16) |
| Magnesium intake from meat *, 10 mg/day | 0.91 (0.70, 1.20) | 0.91 (0.69, 1.19) | 0.80 (0.59, 1.09) |
| Magnesium intake from legumes & nuts *, 10 mg/day | 0.96 (0.89, 1.05) | 0.96 (0.88, 1.06) | 0.95 (0.86, 1.05) |
| Magnesium intake from fruit *, 10 mg/day | 1.00 (0.81, 1.23) | 0.98 (0.79, 1.20) | 0.96 (0.78, 1.19) |
| Magnesium intake from vegetables *, 10 mg/day | 0.71 (0.51, 1.01) | 0.71 (0.50, 1.01) | 0.75 (0.52, 1.08) |
| Magnesium intake from miscellaneous sources *, 10 mg/day | 0.95 (0.89, 1.02) | 0.95 (0.89, 1.03) | 0.90 (0.82, 0.99) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gant, C.M.; Soedamah-Muthu, S.S.; Binnenmars, S.H.; Bakker, S.J.L.; Navis, G.; Laverman, G.D. Higher Dietary Magnesium Intake and Higher Magnesium Status Are Associated with Lower Prevalence of Coronary Heart Disease in Patients with Type 2 Diabetes. Nutrients 2018, 10, 307. https://doi.org/10.3390/nu10030307
Gant CM, Soedamah-Muthu SS, Binnenmars SH, Bakker SJL, Navis G, Laverman GD. Higher Dietary Magnesium Intake and Higher Magnesium Status Are Associated with Lower Prevalence of Coronary Heart Disease in Patients with Type 2 Diabetes. Nutrients. 2018; 10(3):307. https://doi.org/10.3390/nu10030307
Chicago/Turabian StyleGant, Christina M., Sabita S. Soedamah-Muthu, S. Heleen Binnenmars, Stephan J. L. Bakker, Gerjan Navis, and Gozewijn D. Laverman. 2018. "Higher Dietary Magnesium Intake and Higher Magnesium Status Are Associated with Lower Prevalence of Coronary Heart Disease in Patients with Type 2 Diabetes" Nutrients 10, no. 3: 307. https://doi.org/10.3390/nu10030307