Cardiorespiratory Fitness as a Mediator of the Influence of Diet on Obesity in Children

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Measures
2.2.1. Anthropometrics
2.2.2. Dietary Factors
2.2.3. Cardiorespiratory Fitness
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
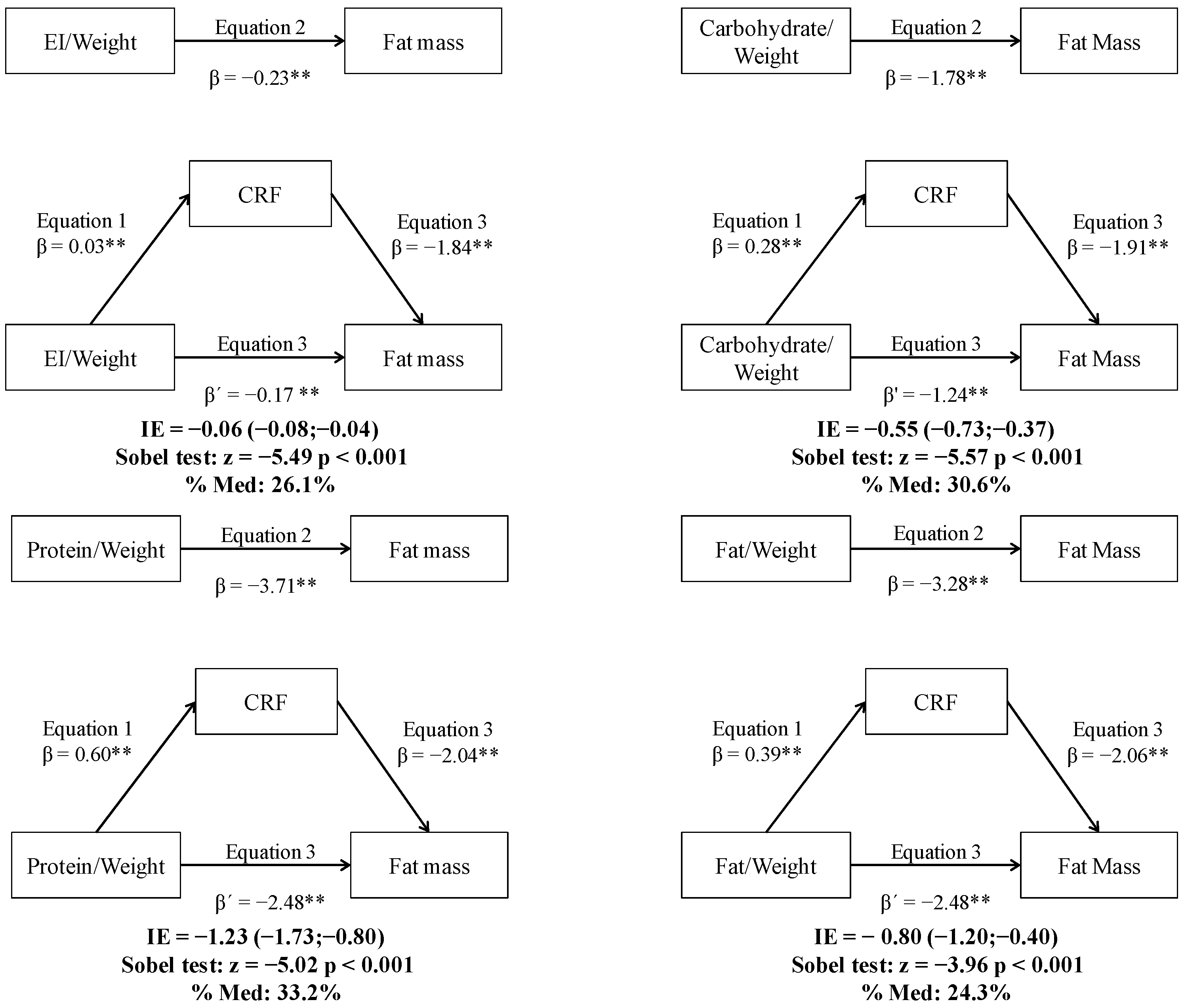
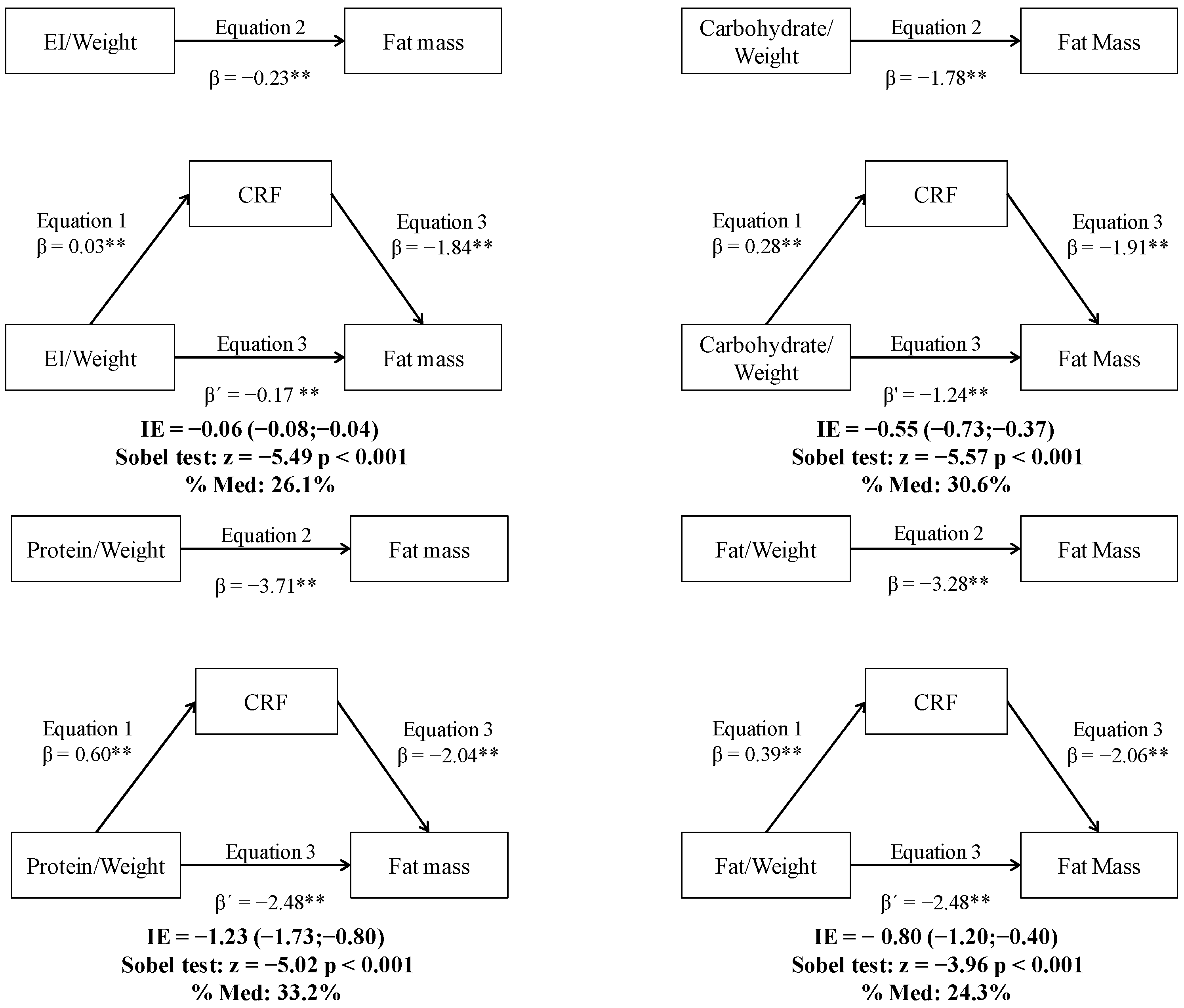
3.2. Simple Mediation Analysis
4. Discussion
4.1. Statement of Principal Findings
4.2. Direction of the Association between CRF and Obesity
4.3. Direction of the Association between Diet and Obesity
4.4. Direction of the Association between CRF and Diet
4.5. CRF as a Mediator between Diet and Obesity
4.6. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Childhood obesity, prevalence and prevention. Nutr. J. 2005, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vizcaíno, V.; Solera Martínez, M.; Notario Pacheco, B.; Sánchez López, M.; Cañete García-Prieto, J.; Torrijos Niño, C.; Arias Palencia, N.; Salcedo Aguilar, F.; Rodríguez-Artalejo, F. Trends in excess of weight, underweight and adiposity among Spanish children from 2004 to 2010: The Cuenca study. Public Health Nutr. 2012, 15, 2170–2174. [Google Scholar] [CrossRef] [PubMed]
- Brug, J.; van Stralen, M.M.; te Velde, S.J.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Lien, N.; Bere, E.; Maskini, V.; Singh, A.S.; Maes, L.; et al. Differences in weight status and energy-balance related behaviors among schoolchildren across Europe: The ENERGY-Project. PLoS ONE 2012, 7, e34742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauner, A.; Mess, F.; Woll, A. The relationship between physical activity, physical fitness and overweight in adolescents: A systematic review of studies published in or after 2000. BMC Pediatr. 2013, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- De Andrade Goncalves, E.C.; Augusto Santos Silva, D.; Gimenes Nunes, H.E. Prevalence and factors associated with low aerobic performance levels in adolescents: A systematic review. Curr. Pediatr. Rev. 2015, 11, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Martínez, A.; Victoria, F.; Pérez-Llamas, F.; Ortega, R.M.; Zamora, S. Differences in dietary intake and activity level between normal-weight and overweight or obese adolescents. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-García, M.; Ortega, F.B.; Ruiz, J.R.; Labayen, I.; Moreno, L.A.; Patterson, E.; Vicente-Rodríguez, G.; González-Gross, M.; Marcos, A.; Polito, A.; et al. More physically active and leaner adolescents have higher energy intake. J. Pediatr. 2014, 164, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Stallmann-Jorgensen, I.S.; Gutin, B.; Hatfield-Laube, J.L.; Humphries, M.C.; Johnson, M.H.; Barbeau, P. General and visceral adiposity in black and white adolescents and their relation with reported physical activity and diet. Int. J. Obes. 2007, 31, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Telford, R.D.; Cunningham, R.B.; Telford, R.M.; Riley, M.; Abhayaratna, W.P. Determinants of childhood adiposity: Evidence from the Australian LOOK Study. PLoS ONE 2012, 7, e50014. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Steiner, M.J.; Perrin, E.M. Self-reported energy intake by age in overweight and healthy-weight children in NHANES, 2001–2008. Pediatrics 2012, 130, e936–e942. [Google Scholar] [CrossRef] [PubMed]
- McGloin, A.F.; Livingstone, M.B.; Greene, L.C.; Webb, S.E.; Gibson, J.M.; Jebb, S.A.; Cole, T.J.; Coward, W.A.; Wright, A.; Prentice, A.M. Energy and fat intake in obese and lean children at varying risk of obesity. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C. Aerobic fitness, fatness and the metabolic syndrome in children and adolescents. Acta Paediatr. 2007, 96, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Watts, K.; Jones, T.W.; Davis, E.A.; Green, D. Exercise training in obese children and adolescents: Current concepts. Sports Med. 2005, 35, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, F.; Seabra, A.; Katzmarzyk, P.T.; Kraemer-Aguiar, L.G.; Bouskela, E.; Farinatti, P. Physical activity in overweight and obese adolescents: Systematic review of the effects on physical fitness components and cardiovascular risk factors. Sports Med. 2014, 44, 1139–1152. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Vizcaíno, V.; Sánchez-López, M.; Salcedo-Aguilar, F.; Notario-Pacheco, B.; Solera-Martínez, M.; Moya-Martínez, P.; Franquelo-Morales, P.; López-Martínez, S.; Rodríguez-Artalejo, F. Protocol of a randomized cluster trial to assess the effectiveness of the MOVI-2 program on overweight prevention in schoolchildren. Revista Española de Cardiología (English Version) 2012, 65, 427–433. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Fs, R.; St-Onge, M.-P.; Heymsfield, S. New bioimpedance analysis system: Improved phenotyping with whole-body analysis. Eur. J. Clin. Nutr. 2004, 58, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Sui, X.; Lavie, C.J.; Blair, S.N. Body mass index, the most widely used but also widely criticized index: Would a criterion standard measure of total body fat be a better predictor of cardiovascular disease mortality? Mayo Clin. Proc. 2016, 91, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.; De Henauw, S.; Maes, L.; Moreno, L.; Manios, Y.; Phillipp, K.; Plada, M.; De Bourdeaudhuij, I. Reliability and validity of a healthy diet determinants questionnaire for adolescents. Public Health Nutr. 2009, 12, 1830–1838. [Google Scholar] [CrossRef] [PubMed]
- Farran, A.; Zamora, R.; Cervera, P. Tablas de Composición de Alimentos del CESNID, 2nd ed.; McGraw-Hill/Interamericana: New York, NY, USA, 2004. [Google Scholar]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Little, T.D., Ed.; Guilford Press: New York, NY, USA, 2013; p. 507. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Moreno, L.A.; Rodríguez, G. Dietary risk factors for development of childhood obesity. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Elliott, S.A.; Truby, H.; Lee, A.; Harper, C.; Abbott, R.A.; Davies, P.S. Associations of body mass index and waist circumference with: Energy intake and percentage energy from macronutrients, in a cohort of Australian children. Nutr. J. 2011, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-García, M.; Ortega, F.B.; Huybrechts, I.; Ruiz, J.R.; González-Gross, M.; Ottevaere, C.; Sjöström, M.; Díaz, L.E.; Ciarapica, D.; Molnar, D.; et al. Cardiorespiratory fitness and dietary intake in European adolescents: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 1850–1859. [Google Scholar] [CrossRef] [PubMed]
- Haraldsdottir, J.; Andersen, L.B. Dietary factors related to fitness in young men and women. Prev. Med. 1994, 23, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Arriscado, D.; Muros, J.J.; Zabala, M.; Dalmau, J.M. Factors associated with low adherence to a Mediterranean diet in healthy children in northern Spain. Appetite 2014, 80, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Zaqout, M.; Vyncke, K.; Moreno, L.; De Miguel-Etayo, P.; Lauria, F.; Molnar, D.; Lissner, L.; Hunsberger, M.; Veidebaum, T.; Tornaritis, M.; et al. Determinant factors of physical fitness in European children. Int. J. Public Health 2016, 61, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Nyström, C.D.; Henriksson, P.; Martínez-Vizcaíno, V.; Medrano, M.; Cadenas-Sanchez, C.; Arias-Palencia, N.M.; Löf, M.; Ruiz, J.R.; Labayen, I.; Sánchez-López, M.; et al. Does cardiorespiratory fitness attenuate the adverse effects of severe/morbid obesity on cardiometabolic risk and insulin resistance in children? A pooled analysis. Diabetes Care 2017, 40, 1580–1587. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Larizza, D.; Codrons, E.; De Silvestri, A.; Brambilla, P.; Abela, S.; Arpesella, M.; Vandoni, M. Improved metabolic and cardiorespiratory fitness during a recreational training program in obese children. J. Pediatr. Endocrinol. Metab. 2013, 26, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Prado, D.M.; Silva, A.G.; Trombetta, I.C.; Ribeiro, M.M.; Nicolau, C.M.; Guazzelli, I.C.; Matos, L.N.; Negrao, C.E.; Villares, S.M. Weight loss associated with exercise training restores ventilatory efficiency in obese children. Int. J. Sports Med. 2009, 30, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.R.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Gutin, B. The role of nutrient partitioning and stem cell differentiation in pediatric obesity: A new theory. Int. J. Pediatr. Obes. 2011, 6, 7–12. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Boys (n = 164) | Girl (n = 174) | p a | |
|---|---|---|---|
| Age (years) | 10.0 ± 0.5 | 10.0 ± 0.4 | 0.335 |
| Weight (kg) | 38.7 ± 8.7 | 39.9 ± 9.5 | 0.236 |
| Height (cm) | 140.6 ± 6.6 | 142.9 ± 7.0 | 0.003 |
| BMI (kg/m2) | 19.4 ± 3.6 | 19.4 ± 3.7 | 0.908 |
| WC (cm) | 68.9 ± 9.2 | 68.9 ± 9.3 | 0.978 |
| FM (%) | 24.1 ± 7.0 | 27.0 ± 5.7 | <0.001 |
| FMI (kg/m2) | 4.9 ± 2.4 | 5.4 ± 2.2 | <0.001 |
| Tanner stage * | 1.6 ± 0.7 | 1.6 ± 0.6 | 0.345 |
| Tanner stage (I–II/III–V) (%) * | 85.6/14.4 | 87.7/12.3 | 0.721 |
| CRF (mL/kg/min) | 44.33 ± 4.7 | 41.51 ± 3.3 | <0.001 |
| EI (kcal) | 1648.1 ± 516.9 | 1582.0 ± 497.7 | 0.245 |
| Carbohydrate (% EI) | 42.0 ± 9.4 | 43.2 ± 9.6 | 0.251 |
| Protein (% EI) | 18.4 ± 4.9 | 17.6 ± 4.5 | 0.131 |
| Fat (% EI) | 39.7 ± 8.5 | 39.2 ± 8.7 | 0.611 |
| EI/weight (kcal/kg) | 45.1 ± 18.0 | 42.1 ± 16.8 | 0.132 |
| Carbohydrate/weight (g/kg) | 4.7 ± 2.0 | 4.5 ± 2.0 | 0.426 |
| Protein/weight (g/kg) | 2.0 ± 0.8 | 1.8 ± 0.8 | 0.042 |
| Fat/weight (g/kg) | 2.0 ± 1.1 | 1.9 ± 0.9 | 0.140 |
| Underweight (%) | 8.2 | 8.6 | 0.770 |
| Normal weight (%) | 54.1 | 55.7 | |
| Overweight (%) | 30.8 | 26.4 | |
| Obese (%) | 6.8 | 9.2 |
| WC | FM | FMI | CRF | EI | Carbohydrate | Protein | Fat | EI/Weight | Carbohydrate/Weight | Protein/Weight | Fat/Weight | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BMI | 0.933 ** | 0.915 ** | 0.965 ** | −0.571 ** | −0.096 | −0.036 | 0.119 * | −0.028 | −0.583 ** | −0.552 ** | −0.469 ** | −0.463 ** |
| WC | 0.906 ** | 0.928 ** | −0.574 ** | −0.088 | −0.015 | 0.131 * | −0.056 | −0.582 ** | −0.547 ** | −0.456 ** | −0.470 ** | |
| FM | 0.975 ** | −0.602 ** | −0.179 ** | −0.005 | 0.156 * | −0.081 | −0.604 ** | −0.554 ** | −0.462 ** | −0.504 ** | ||
| FMI | −0.584 ** | −0.136 * | −0.025 | 0.135 * | −0.047 | −0.578 ** | −0.538 ** | −0.454 ** | −0.471 ** | |||
| CRF | 0.045 | 0.064 | −0.048 | −0.043 | 0.319 ** | 0.340 ** | 0.272 ** | 0.214 ** | ||||
| EI | −0.206 ** | −0.207 ** | 0.341 ** | 0.806 ** | 0.625 ** | 0.611 ** | 0.776 ** | |||||
| Carbohydrate | −0.433 ** | −0.871 ** | −0.147 * | 0.368 ** | −0.383 ** | −0.470 ** | ||||||
| Protein | −0.066 | −0.218 ** | −0.405 ** | 0.394 ** | −0.206 ** | |||||||
| Fat | 0.284 ** | −0.185 ** | 0.212 ** | 0.634 ** | ||||||||
| EI/weight | 0.838 ** | 0.781 ** | 0.900 ** | |||||||||
| Carbohydrate/weight | 0.504 ** | 0.545 ** | ||||||||||
| Protein/weight | 0.693 ** |
| FM (%) | Cardiorespiratory Fitness Categories | |||
|---|---|---|---|---|
| Low | Medium | High | p-Value | |
| Model 1 | 31.8 ± 0.6 | 25.7 ± 0.4 | 21.0 ± 0.6 | <0.001 |
| Model 2 | 30.1 ± 0.6 | 25.8 ± 0.3 | 22.1 ± 0.5 | <0.001 |
| Model 3 | 30.5 ± 0.6 | 25.7 ± 0.4 | 22.0 ± 0.5 | <0.001 |
| Model 4 | 30.7 ± 0.6 | 25.7 ± 0.4 | 21.7 ± 0.5 | <0.001 |
| Model 5 | 30.6 ± 0.6 | 25.9 ± 0.4 | 21.6 ± 0.5 | <0.001 |
| Model 1 | Model 6 | |||||||
|---|---|---|---|---|---|---|---|---|
| Low | Medium | High | p-Value | Low | Medium | High | p-Value | |
| EI/Weight Categories | ||||||||
| FM (%) | 31.2 ± 0.6 | 25.6 ± 0.4 | 20.4 ± 0.6 | <0.001 | 29.7 ± 0.5 | 25.7 ± 0.3 | 21.6 ± 0.5 | <0.001 |
| Carbohydrate/Weight Categories | ||||||||
| FM (%) | 30.2 ± 0.6 | 25.8 ± 0.4 | 20.8 ± 0.6 | <0.001 | 29.0 ± 0.5 | 25.7 ± 0.4 | 22.3 ± 0.5 | <0.001 |
| Protein/Weight Categories | ||||||||
| FM (%) | 29.6 ± 0.6 | 25.5 ± 0.5 | 22.1 ± 0.6 | <0.001 | 28.3 ± 0.5 | 25.6 ± 0.4 | 23.2 ± 0.5 | <0.001 |
| Fat/Weight Categories | ||||||||
| FM (%) | 29.6 ± 0.6 | 26.0 ± 0.4 | 21.1 ± 0.6 | <0.001 | 28.4 ± 0.5 | 26.2 ± 0.4 | 22.0 ± 0.5 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lahoz-García, N.; García-Hermoso, A.; Milla-Tobarra, M.; Díez-Fernández, A.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Cardiorespiratory Fitness as a Mediator of the Influence of Diet on Obesity in Children. Nutrients 2018, 10, 358. https://doi.org/10.3390/nu10030358
Lahoz-García N, García-Hermoso A, Milla-Tobarra M, Díez-Fernández A, Soriano-Cano A, Martínez-Vizcaíno V. Cardiorespiratory Fitness as a Mediator of the Influence of Diet on Obesity in Children. Nutrients. 2018; 10(3):358. https://doi.org/10.3390/nu10030358
Chicago/Turabian StyleLahoz-García, Noelia, Antonio García-Hermoso, Marta Milla-Tobarra, Ana Díez-Fernández, Alba Soriano-Cano, and Vicente Martínez-Vizcaíno. 2018. "Cardiorespiratory Fitness as a Mediator of the Influence of Diet on Obesity in Children" Nutrients 10, no. 3: 358. https://doi.org/10.3390/nu10030358