The Effects of Isoflavone Supplementation Plus Combined Exercise on Lipid Levels, and Inflammatory and Oxidative Stress Markers in Postmenopausal Women



Abstract
:1. Introduction
2. Materials and Methods
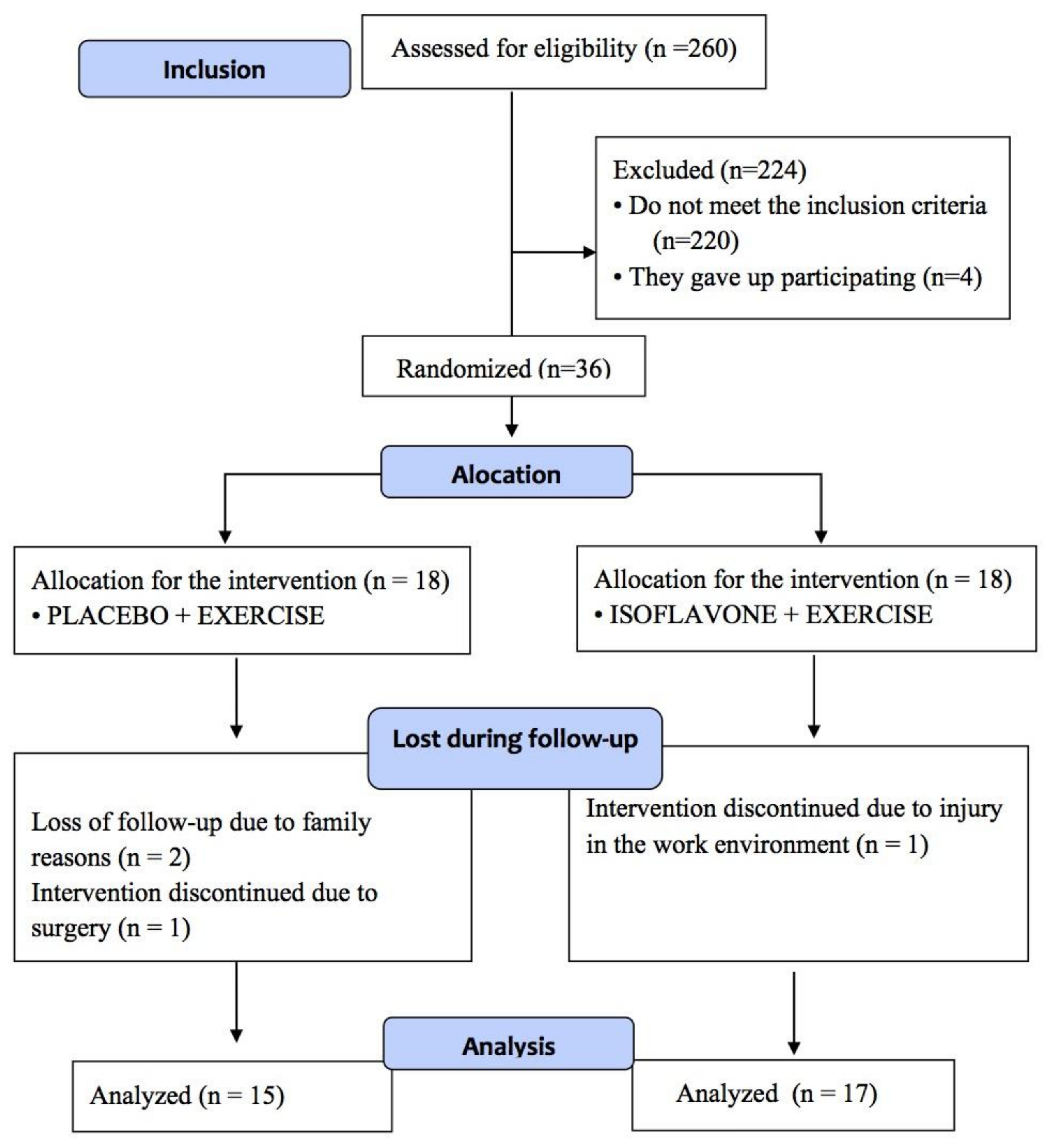
2.1. Participants
2.2. Supplementation
2.3. Body Composition and Anthropometric Measures
2.4. Dietary Assessment
2.5. Exercise Training
2.6. Blood Samples Collection and Analysis
2.7. Statistics
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alvehus, M.; Simonyte, K.; Andersson, T.; Söderström, I.; Burén, J.; Rask, E.; Mattsson, C.; Olsson, T. Adipose tissue IL-8 is increased in normal weight women after menopause and reduced after gastric bypass surgery in obese women: IL-8 levels in normal weight and obese women. Clin. Endocrinol. 2012, 77, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, S.S.; Neri, S.; Sciacchitano, S.; Pino, L.D.; Costa, M.P.; Marchese, G.; Celotta, G.; Cassibba, N.; Pennisi, G.; Caschetto, S. Behaviour of some indicators of oxidative stress in postmenopausal and fertile women. Maturitas 2006, 53, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Pusparini; Dharma, R.; Suyatna, F.D.; Mansyur, M.; Hidajat, A. Effect of soy isoflavone supplementation on vascular endothelial function and oxidative stress in postmenopausal women: A community randomized controlled trial. Asia Pac. J. Clin. Nutr. 2013, 22, 357–364. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef]
- Sarıfakıoğlu, B.; Güzelant, A.Y.; Güzel, E.Ç.; Güzel, S.; Kızıler, A.R. Effects of 12-week combined exercise therapy on oxidative stress in female fibromyalgia patients. Rheumatol. Int. 2014, 34, 1361–1367. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-K.; Park, J.-H.; Kwon, Y.-C.; Kim, H.-S.; Yoon, M.-S.; Park, H.-T. The effect of combined aerobic and resistance exercise training on abdominal fat in obese middle-aged women. J. Physiol. Anthropol. Appl. Hum. Sci. 2003, 22, 129–135. [Google Scholar] [CrossRef]
- Nielsen, A.R.; Pedersen, B.K. The biological roles of exercise-induced cytokines: IL-6, IL-8, and IL-15. Appl. Physiol. Nutr. MeTable 2007, 32, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, F.; Ernst, E. Alternative and complementary therapies for the menopause. Maturitas 2010, 66, 333–343. [Google Scholar] [CrossRef] [PubMed]
- DiSilvestro, R.A.; Goodman, J.; Dy, E.; LaValle, G. Soy isoflavone supplementation elevates erythrocyte superoxide dismutase, but not plasma ceruloplasmin in postmenopausal breast cancer survivors. Breast Cancer Res. Treat. 2005, 89, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.Y.; Lim, S.; Lee, J.M.; Kim, D.-Y.; Ann, E.-S.; Yoon, S. A combination of soy isoflavone supplementation and exercise improves lipid profiles and protects antioxidant defense-systems against exercise-induced oxidative stress in ovariectomized rats. Biofactors 2007, 29, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Lebon, J.; Riesco, E.; Tessier, D.; Dionne, I.J. Additive effects of isoflavones and exercise training on inflammatory cytokines and body composition in overweight and obese postmenopausal women: A randomized controlled trial. Menopause 2014, 21, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Oka, J.; Higuchi, M.; Tabata, I.; Toda, T.; Fujioka, M.; Fuku, N.; Teramoto, T.; Okuhira, T.; Ueno, T.; et al. Cooperative effects of isoflavones and exercise on bone and lipid metabolism in postmenopausal Japanese women: A randomized placebo-controlled trial. Metabolism 2006, 55, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Chilibeck, P.D.; Vatanparast, H.; Pierson, R.; Case, A.; Olatunbosun, O.; Whiting, S.J.; Beck, T.J.; Pahwa, P.; Biem, H.J. Effect of exercise training combined with isoflavone supplementation on bone and lipids in postmenopausal women: A randomized clinical trial. J. Bone Miner. Res. 2013, 28, 780–793. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Murphy, P.A. Isoflavone content in commercial soybean foods. J. Agric. Food Chem. 1994, 42, 1666–1673. [Google Scholar] [CrossRef]
- Anupongsanugool, E.; Teekachunhatean, S.; Rojanasthien, N.; Pongsatha, S.; Sangdee, C. Pharmacokinetics of isoflavones, daidzein and genistein, after ingestion of soy beverage compared with soy extract capsules in postmenopausal Thai women. BMC Clin. Pharmacol. 2005, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, S.; Yamaguchi, M.; Sobue, T.; Takahashi, T.; Miura, T.; Arai, Y.; Mazur, W.; Wähälä, K.; Adlercreutz, H. Pharmacokinetics of soybean isoflavones in plasma, urine and feces of men after ingestion of 60 g baked soybean powder (kinako). J. Nutr. 1998, 128, 1710–1715. [Google Scholar] [CrossRef] [PubMed]
- Kelly, G.E.; Joannou, G.E.; Reeder, A.Y.; Nelson, C.; Waring, M.A. The variable metabolic response to dietary isoflavones in humans. Proc. Soc. Exp. Biol. Med. 1995, 208, 40–43. [Google Scholar] [CrossRef] [PubMed]
- De França, N.A.G.; Callegari, A.; Gondo, F.F.; Corrente, J.E.; Mclellan, K.C.P.; Burini, R.C.; de Oliveira, E.P. Higher dietary quality and muscle mass decrease the odds of low phase angle in bioelectrical impedance analysis in Brazilian individuals: Dietary quality, muscle mass and phase angle. Nutr. Diet. 2016, 73, 474–481. [Google Scholar] [CrossRef]
- Puga, G.M.; Novais, I.D.P.; Katsanos, C.S.; Zanesco, A. Combined effects of aerobic exercise and L-arginine ingestion on blood pressure in normotensive postmenopausal women: A crossover study. Life Sci. 2016, 151, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K. The anaerobic threshold measurement to evaluate exercise performance. Am. Rev. Respir. Dis. 1984, 129, S35–S40. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, W.J.; Gordon, S.E.; Fleck, S.J.; Marchitelli, L.J.; Mello, R.; Dziados, J.E.; Friedl, K.; Harman, E.; Maresh, C.; Fry, A.C. Endogenous anabolic hormonal and growth factor responses to heavy resistance exercise in males and females. Int. J. Sports Med. 1991, 12, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Justino, A.B.; Pereira, M.N.; Peixoto, L.G.; Vilela, D.D.; Caixeta, D.C.; de Souza, A.V.; Teixeira, R.R.; Silva, H.C.G.; de Moura, F.B.R.; Moraes, I.B.; et al. Hepatoprotective Properties of a Polyphenol-Enriched Fraction from Annona crassiflora Mart. Fruit Peel against Diabetes-Induced Oxidative and Nitrosative Stress. J. Agric. Food Chem. 2017, 65, 4428–4438. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.; Dhaliwal, S.S.; Hills, A.P.; Pal, S. Effects of Chronic Exercise Training on Inflammatory Markers in Australian Overweight and Obese Individuals in a Randomized Controlled Trial. Inflammation 2013, 36, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Forti, L.N.; Van Roie, E.; Njemini, R.; Coudyzer, W.; Beyer, I.; Delecluse, C.; Bautmans, I. Effects of resistance training at different loads on inflammatory markers in young adults. Eur. J. Appl. Physiol. 2017, 117, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; Zanuso, S.; Nicolucci, A.; Fernando, F.; Cavallo, S.; Cardelli, P.; Fallucca, S.; Alessi, E.; Letizia, C.; Jimenez, A.; et al. Anti-inflammatory effect of exercise training in subjects with type 2 diabetes and the metabolic syndrome is dependent on exercise modalities and independent of weight loss. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.Y.; Chae, J.S.; Paik, J.K.; Seo, H.S.; Jang, Y.; Cavaillon, J.-M.; Lee, J.H. Effects of aging and menopause on serum interleukin-6 levels and peripheral blood mononuclear cell cytokine production in healthy nonobese women. AGE 2012, 34, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Izzicupo, P.; D’Amico, M.A.; Di Blasio, A.; Napolitano, G.; Nakamura, F.Y.; Di Baldassarre, A.; Ghinassi, B. Aerobic Training Improves Angiogenic Potential Independently of Vascular Endothelial Growth Factor Modifications in Postmenopausal Women. Front. Endocrinol. 2017, 8, 363. [Google Scholar] [CrossRef] [PubMed]
- Gomes, E.C.; Silva, A.N.; de Oliveira, M.R. Oxidants, Antioxidants, and the Beneficial Roles of Exercise-Induced Production of Reactive Species. Oxid. Med. Cell. Longev. 2012, 2012, 756132. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-M.; Ho, S.C.; Chen, Y.-M.; Woo, J. Effect of soy protein and isoflavones on blood pressure and endothelial cytokines: A 6-month randomized controlled trial among postmenopausal women. J. Hypertens. 2013, 31, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Taleb-Belkadi, O.; Chaib, H.; Zemour, L.; Fatah, A.; Chafi, B.; Mekki, K. Lipid profile, inflammation, and oxidative status in peri- and postmenopausal women. Gynecol. Endocrinol. 2016, 32, 982–985. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Beedie, C.; Jimenez, A. Differential Effects of Aerobic Exercise, Resistance Training and Combined Exercise Modalities on Cholesterol and the Lipid Profile: Review, Synthesis and Recommendations. Sports Med. 2014, 44, 211–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, S.; Ho, S.C. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am. J. Clin. Nutr. 2005, 81, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Rios, D.R.A.; Rodrigues, E.T.; Cardoso, A.P.Z.; Montes, M.B.A.; Franceschini, S.A.; Toloi, M.R.T. Lack of effects of isoflavones on the lipid profile of Brazilian postmenopausal women. Nutrition 2008, 24, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Garrido, A.; De la Maza, M.P.; Hirsch, S.; Valladares, L. Soy isoflavones affect platelet thromboxane A2 receptor density but not plasma lipids in menopausal women. Maturitas 2006, 54, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Maesta, N.; Nahas, E.A.P.; Nahas-Neto, J.; Orsatti, F.L.; Fernandes, C.E.; Traiman, P.; Burini, R.C. Effects of soy protein and resistance exercise on body composition and blood lipids in postmenopausal women. Maturitas 2007, 56, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Choquette, S.; Riesco, É.; Cormier, É.; Dion, T.; Aubertin-Leheudre, M.; Dionne, I.J. Effects of soya isoflavones and exercise on body composition and clinical risk factors of cardiovascular diseases in overweight postmenopausal women: A 6-month double-blind controlled trial. Br. J. Nutr. 2011, 105, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Setchell, K.D.; Clerici, C.; Lephart, E.D.; Cole, S.J.; Heenan, C.; Castellani, D.; Wolfe, B.E.; Nechemias-Zimmer, L.; Brown, N.M.; Lund, T.D. S-Equol, a potent ligand for estrogen receptor β, is the exclusive enantiomeric form of the soy isoflavone metabolite produced by human intestinal bacterial flora. Am. J. Clin. Nutr. 2005, 81, 1072–1079. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pre | Post | Δ | p | p | p | |
|---|---|---|---|---|---|---|
| Mean ± SE | Mean ± SE | (Groups) | (Moments) | (Groups * Moments) | ||
| Total Cholesterol (mg/dL) | ||||||
| PLA | 210 ± 8 | 197 ± 7 | −13.07 ± 3.72 | 0.34 | 0.04 | 0.07 |
| ISO | 215 ± 9 | 214 ± 9 | −1.13 ± 5.03 | |||
| LDL (mg/dL) | ||||||
| PLA | 126 ± 9 | 118 ± 6 | −7.54 ± 4.29 | 0.34 | 0.24 | 0.21 |
| ISO | 133 ± 8 | 133 ± 8 | 0.25 ± 4.21 | |||
| HDL (mg/dL) | ||||||
| PLA | 55.4 ± 3.6 | 50.5 ± 3.0 | −4.54 ± 1.27 | 0.25 | 0.07 | 0.16 |
| ISO | 58.1 ± 3.4 | 57.5 ± 2.6 | −0.59 ± 2.16 | |||
| VLDL (mg/dL) | ||||||
| PLA | 24.7 ± 3.1 | 23.5 ± 3.0 | −1.20 ± 1.60 | 0.77 | 0.91 | 0.47 |
| ISO | 22.7 ± 2.1 | 23.6 ± 2.0 | 0.88 ± 2.17 | |||
| Triglycerides (mg/dL) | ||||||
| PLA | 124 ± 16 | 118 ± 15 | −6.00 ± 7.98 | 0.77 | 0.91 | 0.47 |
| ISO | 113 ± 11 | 118 ± 10 | 4.38 ± 10.86 | |||
| Glucose (mg/dL) | ||||||
| PLA | 86.6 ± 1.7 | 86.8 ± 1.6 | 0.17 ± 1.33 | 0.92 | 0.27 | 0.20 |
| ISO | 87.5 ± 1.0 | 85.5 ± 1.4 | −2.08 ± 1.09 | |||
| Glycated Hemoglobin (%) | ||||||
| PLA | 5.50 ± 0.07 | 5.52 ± 0.10 | 0.02 ± 0.06 | 0.24 | 0.53 | 0.92 |
| ISO | 5.60 ± 0.05 | 5.63 ± 0.03 | 0.03 ± 0.05 | |||
| Uric Acid (mg/dL) | ||||||
| PLA | 4.5 ± 0.3 | 4.6 ± 0.3 | 0.04 ± 0.13 | 0.79 | 0.68 | 0.40 |
| ISO | 4.5 ± 0.2 | 4.4 ± 0.1 | −0.12 ± 0.14 | |||
| Pre | Post | Δ | p | p | p | |
|---|---|---|---|---|---|---|
| Mean ± SE | Mean ± SE | (Groups) | (Moments) | (Groups * Moments) | ||
| Interleukin-8 (pg/mL) | ||||||
| PLA | 13.70 ± 1.91 | 21.31 ± 2.23 | 7.61 ± 2.50 | 0.92 | 0.001 | 0.55 |
| ISO | 14.52 ± 1.10 | 20.13 ± 1.79 | 5.61 ± 2.23 | |||
| Interleukin-6 (pg/mL) | ||||||
| PLA | 1.54 ± 0.39 | 1.30 ± 0.32 | −0.24 ± 0.27 | 0.76 | 0.22 | 0.98 |
| ISO | 1.42 ± 0.21 | 1.19 ± 0.26 | −0.23 ± 0.25 | |||
| FRAP (umol/L eq. Trolox) | ||||||
| PLA | 124.31 ± 5.24 | 123.18 ± 5.67 | −1.13 ± 3.48 | 0.65 | 0.39 | 0.73 |
| ISO | 122.47 ± 2.83 | 119.85 ± 3.03 | -2.63 ± 2.58 | |||
| TBARS (umol/L TBA-RS) | ||||||
| PLA | 24.65 ± 1.08 | 24.42 ± 1.17 | −0.23 ± 0.72 | 0.72 | 0.38 | 0.70 |
| ISO | 24.40 ± 0.61 | 23.82 ± 0.66 | −0.58 ± 0.56 | |||
| SOD (SOD/mg prot) | ||||||
| PLA | 0.190 ± 0.007 | 0.194 ± 0.008 | 0.003 ± 0.010 | 0.20 | 0.24 | 0.50 |
| ISO | 0.176 ± 0.007 | 0.193 ± 0.008 | 0.012 ± 0.008 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giolo, J.S.; Costa, J.G.; Da Cunha-Junior, J.P.; Pajuaba, A.C.A.M.; Taketomi, E.A.; De Souza, A.V.; Caixeta, D.C.; Peixoto, L.G.; De Oliveira, E.P.; Everman, S.; et al. The Effects of Isoflavone Supplementation Plus Combined Exercise on Lipid Levels, and Inflammatory and Oxidative Stress Markers in Postmenopausal Women. Nutrients 2018, 10, 424. https://doi.org/10.3390/nu10040424
Giolo JS, Costa JG, Da Cunha-Junior JP, Pajuaba ACAM, Taketomi EA, De Souza AV, Caixeta DC, Peixoto LG, De Oliveira EP, Everman S, et al. The Effects of Isoflavone Supplementation Plus Combined Exercise on Lipid Levels, and Inflammatory and Oxidative Stress Markers in Postmenopausal Women. Nutrients. 2018; 10(4):424. https://doi.org/10.3390/nu10040424
Chicago/Turabian StyleGiolo, Jéssica S., Juliene G. Costa, Jair P. Da Cunha-Junior, Ana Cláudia A. M. Pajuaba, Ernesto A. Taketomi, Adriele V. De Souza, Douglas C. Caixeta, Leonardo G. Peixoto, Erick P. De Oliveira, Sarah Everman, and et al. 2018. "The Effects of Isoflavone Supplementation Plus Combined Exercise on Lipid Levels, and Inflammatory and Oxidative Stress Markers in Postmenopausal Women" Nutrients 10, no. 4: 424. https://doi.org/10.3390/nu10040424