Assessment of Lactose-Free Diet on the Phalangeal Bone Mineral Status in Italian Adolescents Affected by Adult-Type Hypolactasia

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Anthropometric Measurements
2.3. Diet Record and Ca Intake
2.4. Quantitative Ultrasound
2.5. Breath Test
2.6. Statistical Analysis
3. Results
3.1. Subjects
3.2. Quantitative Ultrasound
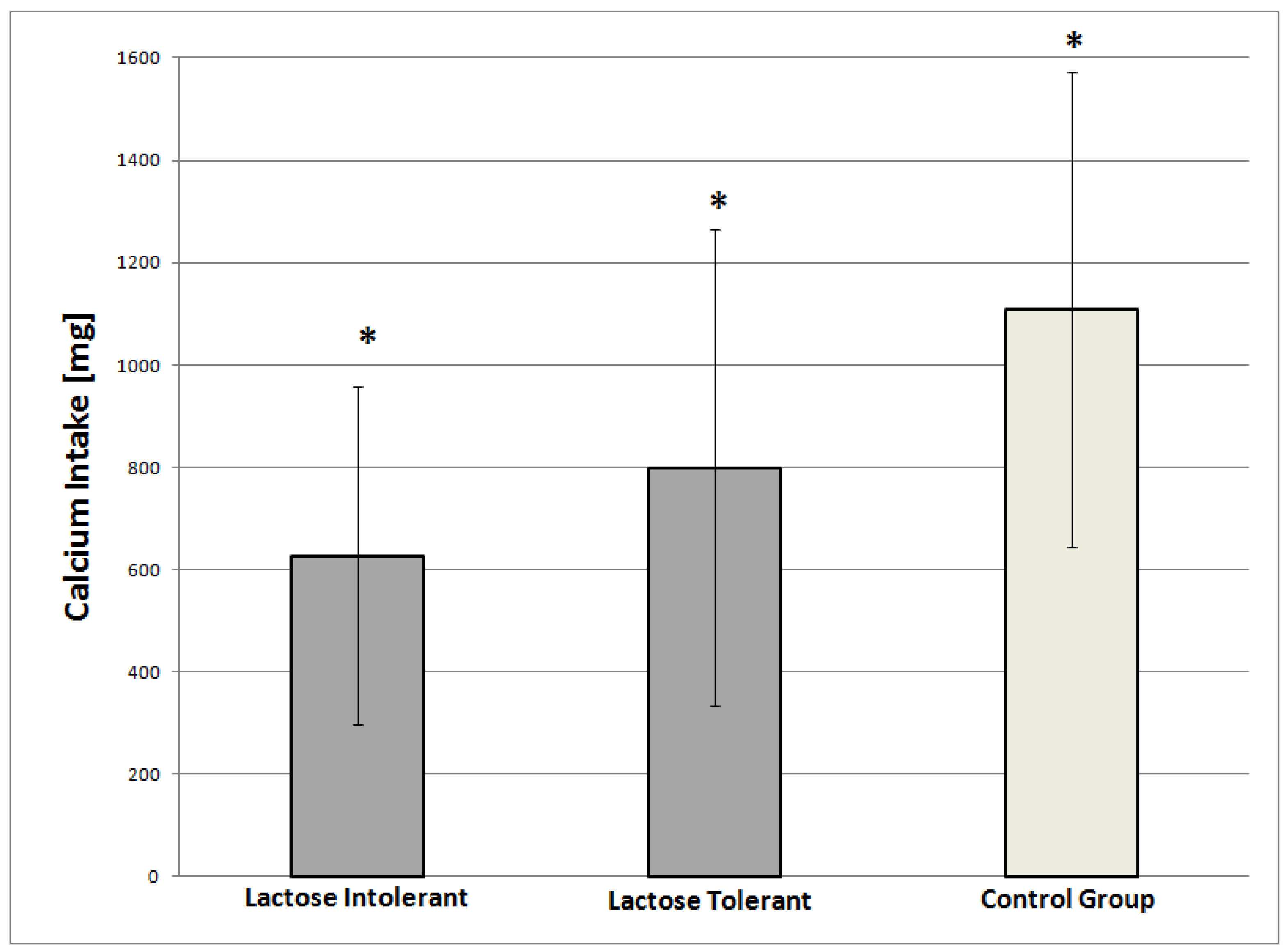
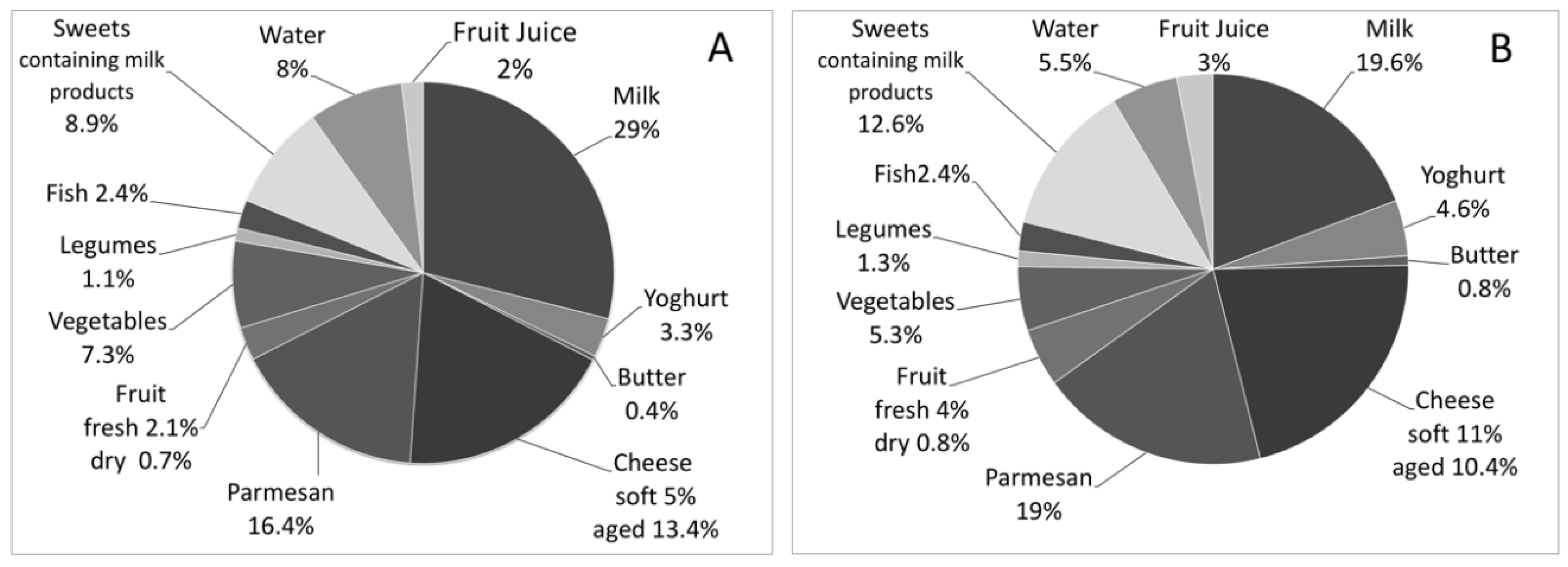
3.3. Dietary Intake of Ca and Vitamin D and Correlation to Physical Exercise
3.4. Ca Intake and BMS
4. Discussion
4.1. Ca Intake
4.2. Phalangeal BMS
4.3. Physical Activity
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Swallow, D.M. Genetics of lactase persistence and lactose intolerance. Annu. Rev. Genet. 2003, 37, 197–219. [Google Scholar] [CrossRef] [PubMed]
- Enattah, N.S.; Sahi, T.; Savilahti, E.; Terwilliger, J.D.; Peltonen, L.; Järvelä, I. Identification of a variant associated with adult-type hypolactasia. Nat. Genet. 2002, 30, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Holden, C.; Mace, R. Phylogenetic analysis of the evolution of lactose digestion in adults. Hum. Biol. 1997, 69, 605–628. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Aggarwal, R. Lactose intolerance. BMJ 2007, 334, 1331–1332. [Google Scholar] [CrossRef] [PubMed]
- Heyman, M.B. Lactose intolerance in infants, children, and adolescents. Pediatrics 2006, 118, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Greer, F.R.; Krebs, N.F. Optimizing bone health and calcium intakes of infants, children, and adolescents. Pediatrics 2006, 117, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Bonjour, J.P.; Carrie, A.L.; Ferrari, S.; Clavien, H.; Slosman, D.; Theintz, G.; Rizzoli, R. Calcium-enriched foods and bone mass growth in prepubertal girls: A randomized, double-blind, placebo-controlled trial. J. Clin. Investig. 1997, 99, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, C.; Harvey, N.; Dennison, E.; Cooper, C. Epigenetic influences in the developmental origins of osteoporosis. Osteoporos. Int. 2012, 23, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.G.; Gilchrist, N.L.; Ayling, E.M.; Hassall, A.J.; Hooke, E.A.; Sadler, W.A. Factors affecting bone mineral density in high school girls. N. Z. Med. J. 1992, 105, 95–96. [Google Scholar] [PubMed]
- Guéguen, R.; Jouanny, P.; Guillemin, F.; Kuntz, C.; Pourel, J.; Siest, G. Segregation analysis and variance components analysis of bone mineral density in healthy families. J. Bone Miner. Res. 1995, 10, 2017–2022. [Google Scholar] [CrossRef] [PubMed]
- Kutilek, S.; Bayer, M.; Dolezalova, P.; Nemcova, D. Quantitative ultrasonometry of the calcaneus in children with juvenile idiopathic arthritis. Rheumatology 2006, 45, 1273–1275. [Google Scholar] [CrossRef] [PubMed]
- Kutílek, S.; Bayer, M.; Fruhauf, P. Growth failure and decreased ultrasound parameters of bone density in children with inflammatory bowel disease. Nutrition 2001, 17, 83. [Google Scholar] [CrossRef]
- Levine, A.; Mishna, L.; Ballin, A.; Givoni, S.; Dinari, G.; Hartman, C.; Shamir, R. Use of quantitative ultrasound to assess osteopenia in children with Crohn disease. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Hartman, C.; Hino, B.; Lerner, A.; Eshach-Adiv, O.; Berkowitz, D.; Shaoul, R.; Pacht, A.; Rozenthal, E.; Tamir, A.; Shamaly, H.; et al. Bone quantitative ultrasound and bone mineral density in children with celiac disease. J. Pediatr. Gastroenterol. Nutr. 2004, 39, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Mądry, E.; Krasińska, B.; Drzymaa-Czyz, S.; Sands, D.; Lisowska, A.; Grebowiec, P.; Minarowska, A.; Oralewska, B.; Mańkowski, P.; Moczko, J.; et al. Lactose malabsorption is a risk factor for decreased bone mineral density in pancreatic insufficient cystic fibrosis patients. Eur. J. Hum. Genet. 2012, 20, 1092–1095. [Google Scholar] [CrossRef] [PubMed]
- Mottes, M.; Belpinati, F.; Milani, M.; Saccomandi, D.; Petrelli, E.; Calacoci, M.; Chierici, R.; Pignatti, P.F.; Borgna-Pignatti, C. Genetic testing for adult-type hypolactasia in Italian families. Clin. Chem. Lab. Med. 2008, 46, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Zerfas, A.J. Checking Continuous Measures: Manual for Anthropometry; Division of Epidemiology, School of Public Health, University of California: Los Angeles, CA, USA, 1985. [Google Scholar]
- Cacciari, E.; Milani, S.; Balsamo, A.; Dammacco, F.; De Luca, F.; Chiarelli, F.; Pasquino, A.M.; Tonini, G.; Vanelli, M. Italian cross-sectional growth charts for height, weight and BMI (6–20 y). Eur. J. Clin. Nutr. 2002, 56, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Società Italiana di Nutrizione Umana (SINU). Livelli di Assunzione di Riferimento di Nutrienti ed Energia per la Popolazione Italiana (LARN); Revisione 2012; SINU: New York, NY, USA, 2012. [Google Scholar]
- Genant, H.K.; Engelke, K.; Fuerst, T.; Glüer, C.C.; Grampp, S.; Harris, S.T.; Jergas, M.; Lang, T.; Lu, Y.; Majumdar, S.; et al. Noninvasive assessment of bone mineral and structure: State of the art. J. Bone Miner. Res. 1996, 11, 707–730. [Google Scholar] [CrossRef] [PubMed]
- Njeh, C.F.; Boivin, C.M.; Langton, C.M. The role of ultrasound in the assessment of osteoporosis: A review. Osteoporos. Int. 1997, 7, 7–22. [Google Scholar] [CrossRef] [PubMed]
- Baroncelli, G.I.; Federico, G.; Bertelloni, S.; Sodini, F.; De Terlizzi, F.; Cadossi, R.; Saggese, G. Assessment of bone quality by quantitative ultrasound of proximal phalanges of the hand and fracture rate in children and adolescents with bone and mineral disorders. Pediatr. Res. 2003, 54, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Lewiecki, E.M.; Watts, N.B.; McClung, M.R.; Petak, S.M.; Bachrach, L.K.; Shepherd, J.A.; Downs, R.W., Jr. Official positions of the international society for clinical densitometry. J. Clin. Endocrinol. Metab. 2004, 89, 3651–3655. [Google Scholar] [CrossRef] [PubMed]
- Baroncelli, G.I.; Federico, G.; Vignolo, M.; Valerio, G.; del Puente, A.; Maghnie, M.; Baserga, M.; Farello, G.; Saggese, G. Cross-sectional reference data for phalangeal quantitative ultrasound from early childhood to young-adulthood according to gender, age, skeletal growth, and pubertal development. Bone 2006, 39, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Baroncelli, G.I.; Federico, G.; Bertelloni, S.; De Terlizzi, F.; Cadossi, R.; Saggese, G. Bone quality assessment by quantitative ultrasound of proximal phalanxes of the hand in healthy subjects aged 3–21 years. Pediatr. Res. 2001, 49, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Bond, J.H.; Levitt, M.D. Use of breath hydrogen (H2) in the study of carbohydrate absorption. Am. J. Dig. Dis. 1977, 22, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Pampaloni, B.; Bartolini, E.; Brandi, M.L. Parmigiano Reggiano cheese and bone health. Clin. Cases Miner. Bone Metab. 2011, 8, 33–36. [Google Scholar] [PubMed]
- Baldan, A.; Tagliatti, S.; Saccomandi, D.; Brusaferro, A.; Busoli, L.; Scala, A.; Malaventura, C.; Maggiore, G.; Borgna-Pignatti, C. Effect of lactose-free diet on phalangeal bone mineral status of Italian adolescents with adult type hypolactasia. Dig. Liver Dis. 2017, 49, e280. [Google Scholar] [CrossRef]
- Wiley, A.S. Does milk make children grow? Relationships between milk consumption and height in NHANES 1999–2002. Am. J. Hum. Biol. 2005, 17, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, A.; Garzon, P.; Eisenberg, M.J. Comparison of the mineral content of tap water and bottled waters. J. Gen. Intern. Med. 2001, 16, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Absorbability and utility of calcium in mineral waters. Am. J. Clin. Nutr. 2006, 84, 371–374. [Google Scholar] [PubMed]
- Baroncelli, G.I. Quantitative ultrasound methods to assess bone mineral status in children: Technical characteristics, performance, and clinical application. Pediatr. Res. 2008, 63, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Pluskiewicz, W.; Adamczyk, P.; Drozdzowska, B.; Szprynger, K.; Szczepanska, M.; Halaba, Z.; Karasek, D. Skeletal status in children, adolescents and young adults with end-stage renal failure treated with hemo- or peritoneal dialysis. Osteoporos. Int. 2002, 13, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Cadossi, R.; Canè, V. Pathways of transmission of ultrasound energy through the distal metaphysis of the second phalanx of pigs: An in vitro study. Osteoporos. Int. 1996, 6, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Barkmann, R.; Rohrschneider, W.; Vierling, M.; Tröger, J.; De Terlizzi, F.; Cadossi, R.; Heller, M.; Glüer, C.C. German pediatric reference data for quantitative transverse transmission ultrasound of finger phalanges. Osteoporos. Int. 2002, 13, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Halaba, Z.P.; Pluskiewicz, W. Quantitative ultrasound in the assessment of skeletal status in children and adolescents. Ultrasound Med. Biol. 2004, 30, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Marín, F.; González-Macías, J.; Díez-Pérez, A.; Palma, S.; Delgado-Rodríguez, M. Relationship between bone quantitative ultrasound and fractures: A meta-analysis. J. Bone Miner. Res. 2006, 21, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Aceto, G.; D’Addato, O.; Messina, G.; Carbone, V.; Cavallo, L.; Brunetti, G.; Faienza, M.F. Bone health in children and adolescents with steroid-sensitive nephrotic syndrome assessed by DXA and QUS. Pediatr. Nephrol. 2014, 29, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Krieg, M.A.; Barkmann, R.; Gonnelli, S.; Stewart, A.; Bauer, D.C.; Barquero, L.D.; Kaufman, J.J.; Lorenc, R.; Miller, P.D.; Olszynski, W.P.; et al. Quantitative ultrasound in the management of osteoporosis: The 2007 ISCD Official Positions. J. Clin. Densitom. 2008, 11, 163–187. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.L. Osteoporosis in children and adolescents. Bone 2007, 41, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, L.C.D.S.; Lederman, H.M.; de Morais, M.B. Lactose malabsorption, calcium intake, and bone mass in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Matlik, L.; Savaiano, D.; McCabe, G.; VanLoan, M.; Blue, C.L.; Boushey, C.J. Perceived milk intolerance is related to bone mineral content in 10- to 13-year-old female adolescents. Pediatrics 2007, 120, e669–e677. [Google Scholar] [CrossRef] [PubMed]
- Winzenberg, T.M.; Shaw, K.A.; Fryer, J.; Jones, G. Calcium supplementation for improving bone mineral density in children. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef] [PubMed]
- Lanou, A.J.; Berkow, S.E.; Barnard, N.D. Calcium, dairy products, and bone health in children and young adults: A reevaluation of the evidence. Pediatrics 2005, 115, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, T.; Beck, T.J.; Lin, H.M.; Tulchinsky, M.; Eggli, D.F.; Oreskovic, T.L.; Cavanagh, P.R.; Seeman, E. Modifiable determinants of bone status in young women. Bone 2002, 30, 416–421. [Google Scholar] [CrossRef]
- Uusi-Rasi, K.; Sievänen, H.; Vuori, I.; Pasanen, M.; Heinonen, A.; Oja, P. Associations of physical activity and calcium intake with bone mass and size in healthy women at different ages. J. Bone Miner. Res. 1998, 13, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Wallace, L.S.; Ballard, J.E. Lifetime physical activity and calcium intake related to bone density in young women. J. Womens Health Gend. Based Med. 2002, 11, 389–398. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cases | Controls | ||||
|---|---|---|---|---|---|
| n | n | p-Value | |||
| Age (years ± SD) | 16.8 ± 2.5 | 102 | 17.0 ± 2.2 | 102 | |
| M | 16.7 ± 2.4 | 45 | 17.2 ± 2.0 | 48 | |
| F | 16.9 ± 2.6 | 57 | 16.8 ± 2.0 | 54 | |
| BMI (kg/m2) | 21.5 ± 3.6 | 22.4 ± 3.4 | 0.08 | ||
| M | 21.6 ± 3.8 | 45 | 23.5 ± 3.3 | 48 | 0.01 |
| F | 21.5 ± 3.5 | 57 | 21.5 ± 3.2 | 54 | 0.98 |
| Weight (Kg) | 60.0 ± 12.4 | 63.0 ± 14.2 | 0.1 | ||
| M | 64.1 ± 14.1 | 45 | 70.9 ± 14.8 | 48 | 0.01 |
| F | 56.7 ± 9.8 | 57 | 56.3 ± 9.5 | 54 | 0.92 |
| Height (m) | 1.66 ± 0.09 | 1.67 ± 0.09 | 0.21 | ||
| M | 1.71 ± 0.09 | 45 | 1.74 ± 0.08 | 48 | 0.1 |
| F | 1.62 ± 0.05 | 57 | 1.62 ± 0.06 | 54 | 0.7 |
| Cases | Controls | ||||||
|---|---|---|---|---|---|---|---|
| Ca Intake (mg/day) | Frequency | n | Ca Intake (mg/day) | Frequency | n | p-Value | |
| (Mean ± sd) | (Days/Week) | (Mean ± sd) | (Days/Week) | ||||
| Total Ca intake | 752.1 ± 433.4 | 102 | 1108.6 ± 463.8 | 102 | 7.4 × 10−8 | ||
| M | 763.4 ± 424.0 | 45 | 1289.3 ± 487.3 | 48 | 6.4 × 10−7 | ||
| F | 743.3 ± 444.3 | 57 | 964.7 ± 392.3 | 54 | 0.006 | ||
| Milk | 216.4 ± 256.2 | 4.5 ± 2.8 | 76 | 214.6 ± 181.0 | 4.6 ± 2.3 | 83 | 0.78 |
| Yoghurt | 25.2 ± 54.6 | 2.8 ± 2.3 | 48 | 51.3 ± 41.7 | 2.4 ± 1.7 | 67 | 3.4 × 10−7 |
| Butter | 2.9 ± 8.0 | 1.4 ± 1.2 | 54 | 9.2 ± 13.8 | 1.8 ± 1.3 | 67 | 7.3 × 10−6 |
| Cheese | |||||||
| soft cheese | 38.2 ± 55.8 | 2.0 ± 1.5 | 79 | 122.0 ± 76.4 | 3.3 ± 1.6 | 94 | 4.0 × 10−15 |
| aged cheese | 101.0 ± 124.5 | 1.9 ± 1.6 | 68 | 115.1 ± 117.4 | 1.9 ± 1.5 | 80 | 0.0009 |
| Parmesan | 123.2 ± 112.2 | 4.9 ± 2.4 | 58 | 210.5 ± 141.0 | 5.1 ± 2.7 | 77 | 0.0001 |
| Fruit | |||||||
| fresh | 15.8 ± 40.1 | 5.9 ± 1.9 | 34 | 43.4 ± 34.5 | 5.4 ± 1.9 | 91 | 7.7 × 10−15 |
| dried | 5.5 ± 9.6 | 1.9 ± 2.2 | 40 | 9.0 ± 7.3 | 2.0 ± 1.5 | 54 | 0.008 |
| Vegetables | 55.1 ± 64.0 | 5.4 ± 2.2 | 40 | 58.2 ± 39.6 | 5.7 ± 1.8 | 95 | 0.71 |
| Legumes | 8.6 ± 8.0 | 1.5 ± 1.0 | 66 | 14.3 ± 24.3 | 1.8 ± 1.1 | 78 | 0.051 |
| Fish | 18.2 ± 26.2 | 1.3 ± 0.8 | 83 | 26.4 ± 33.8 | 1.8 ± 1.1 | 88 | 0.025 |
| Sweets containing milk products | |||||||
| cookies and snacks | 28.4 ± 18.5 | 5.0 ± 2.5 | 79 | 37.2 ± 33.8 | 4.4 ± 2.3 | 87 | 0.025 |
| Ice-cream and pudding | 39.3 ± 63.2 | 3.1 ± 2.4 | 67 | 103.1 ± 101.2 | 3.0 ± 2.0 | 87 | 3.9 × 10−7 |
| Water | 60.7 ± 97.6 | 102 | 61.4 ± 101.0 | 102 | 0.19 | ||
| very low mineral content | 15.7 ± 8.4 | 10 | 27.3 ± 17.9 | 6 | 0.12 | ||
| low mineral content | 48.0 ± 27.2 | 83 | 44.2 ± 24.9 | 87 | 0.15 | ||
| medium mineral content | 334.6 ± 160.0 | 9 | 243.7 ± 274.2 | 9 | 0.34 | ||
| Fruit Juice | 13.8 ± 5.6 | 5.0 ± 2.0 | 16 | 33.0 ± 24.7 | 4.3 ± 2.5 | 58 | 4.7 × 10−6 |
| Carbonated drinks | 31 | 52 | |||||
| Total Vitamin D intake | Vitamin D intake (µg/day) (mean ± sd) | n | Vitamin D intake (µg/day) (mean ± sd) | n | p-value | ||
| 3.6 ± 3.1 | 102 | 4.7 ± 2.7 | 102 | 0.005 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldan, A.; Tagliati, S.; Saccomandi, D.; Brusaferro, A.; Busoli, L.; Scala, A.; Malaventura, C.; Maggiore, G.; Borgna-Pignatti, C. Assessment of Lactose-Free Diet on the Phalangeal Bone Mineral Status in Italian Adolescents Affected by Adult-Type Hypolactasia. Nutrients 2018, 10, 558. https://doi.org/10.3390/nu10050558
Baldan A, Tagliati S, Saccomandi D, Brusaferro A, Busoli L, Scala A, Malaventura C, Maggiore G, Borgna-Pignatti C. Assessment of Lactose-Free Diet on the Phalangeal Bone Mineral Status in Italian Adolescents Affected by Adult-Type Hypolactasia. Nutrients. 2018; 10(5):558. https://doi.org/10.3390/nu10050558
Chicago/Turabian StyleBaldan, Alessandro, Sylvie Tagliati, Daniela Saccomandi, Andrea Brusaferro, Laura Busoli, Andrea Scala, Cristina Malaventura, Giuseppe Maggiore, and Caterina Borgna-Pignatti. 2018. "Assessment of Lactose-Free Diet on the Phalangeal Bone Mineral Status in Italian Adolescents Affected by Adult-Type Hypolactasia" Nutrients 10, no. 5: 558. https://doi.org/10.3390/nu10050558