Nutrition of Preterm Infants and Raw Breast Milk-Acquired Cytomegalovirus Infection: French National Audit of Clinical Practices and Diagnostic Approach


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Outcome Measures
2.3. Data Management
2.4. Statistical Analysis
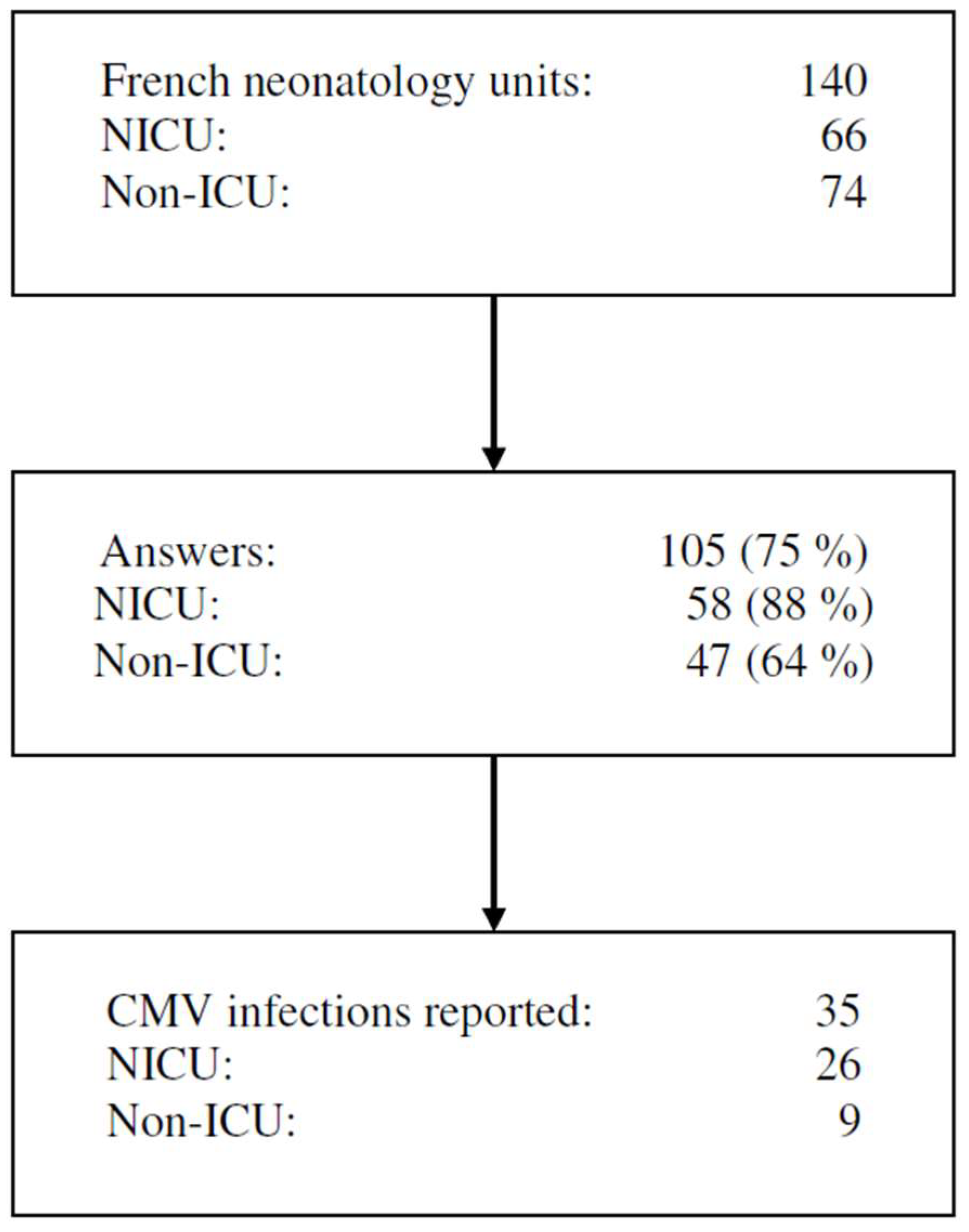
3. Results
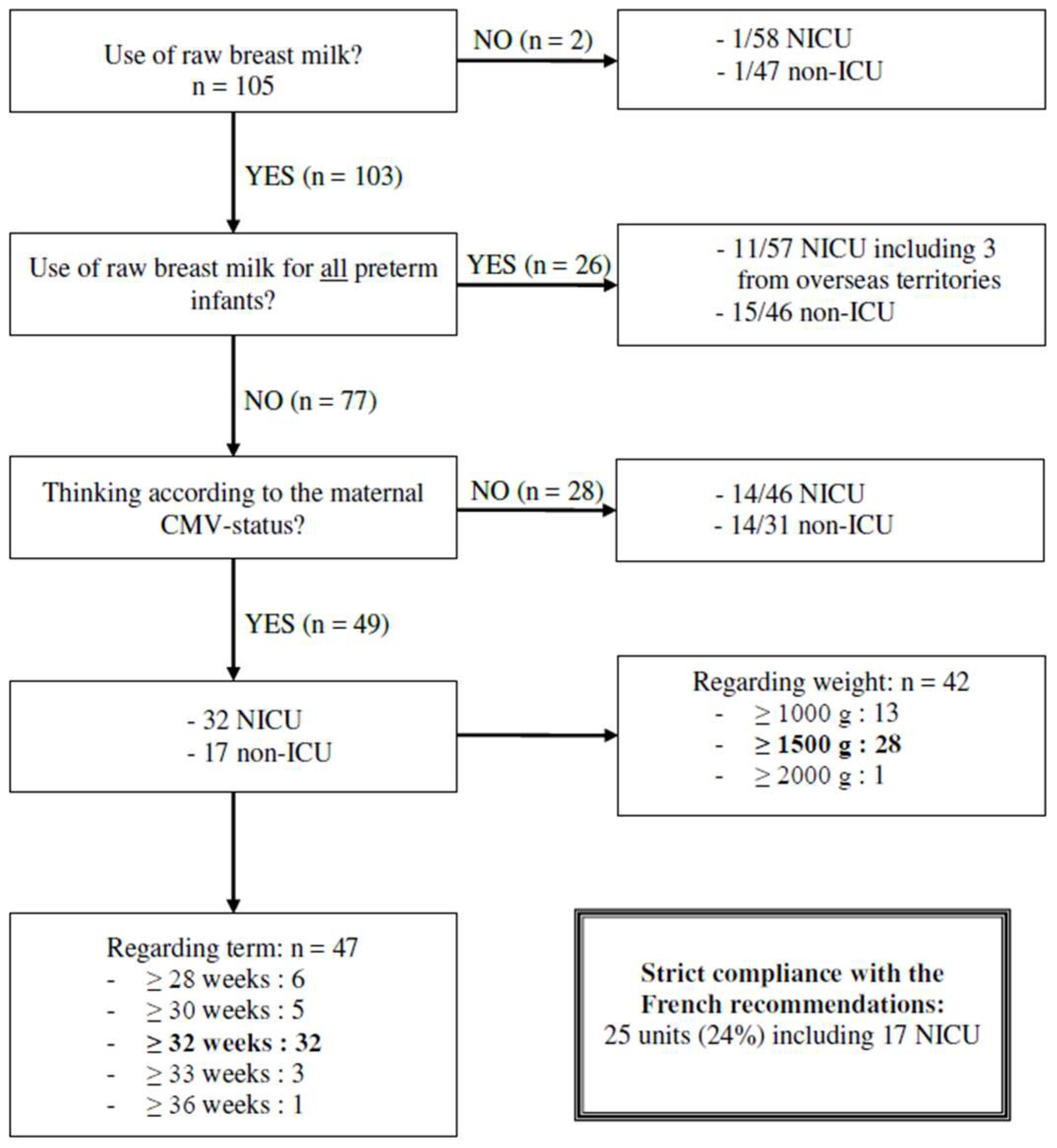
3.1. Current Clinical Practices
3.2. Raw Breast Milk Use
3.3. Reported Postnatal CMV Infection Attributed to Raw Breast Milk Nutrition
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Torchin, H.; Ancel, P.-Y.; Jarreau, P.-H.; Goffinet, F. Epidemiology of preterm birth: Prevalence, recent trends, short- and long-term outcomes. J. Gynecol. Obstet. Biol. Reprod. 2015, 44, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Ancel, P.-Y.; Goffinet, F.; EPIPAGE-2 Writing Group; Kuhn, P.; Langer, B.; Matis, J.; Hernandorena, X.; Chabanier, P.; Joly-Pedespan, L.; Lecomte, B.; et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: Results of the EPIPAGE-2 cohort study. JAMA Pediatr. 2015, 169, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Vidyasagar, D. Half a Century of Evolution of Neonatology: A Witness’s Story. Indian J. Pediatr. 2015, 82, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Cleminson, J.S.; Zalewski, S.P.; Embleton, N.D. Nutrition in the preterm infant: What’s new? Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.D.; Richard, C.; Larsen, B.M.; Field, C.J. The Importance of Human Milk for Immunity in Preterm Infants. Clin. Perinatol. 2017, 44, 23–47. [Google Scholar] [CrossRef] [PubMed]
- Araújo, E.D.; Gonçalves, A.K.; da Cornetta, M.C.; Cunha, H.; Cardoso, M.L.; Morais, S.S.; Giraldo, P.C. Evaluation of the secretory immunoglobulin A levels in the colostrum and milk of mothers of term and pre-term newborns. Braz. J. Infect. Dis. 2005, 9, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Petrova, A. Biologically active breast milk proteins in association with very preterm delivery and stage of lactation. J. Perinatol. 2011, 31, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Koenig, A.; de Albuquerque Diniz, E.M.; Barbosa, S.F.C.; Vaz, F.A.C. Immunologic factors in human milk: The effects of gestational age and pasteurization. J. Hum. Lact. 2005, 21, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Spiegler, J.; Preuß, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Göpel, W.; German Neonatal Network (GNN). Does Breastmilk Influence the Development of Bronchopulmonary Dysplasia? J. Pediatr. 2016, 169, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Bharwani, S.K.; Green, B.F.; Pezzullo, J.C.; Bharwani, S.S.; Dhanireddy, R. Systematic review and meta-analysis of human milk intake and retinopathy of prematurity: A significant update. J. Perinatol. 2016, 36, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.M. The Role of Lactoferrin in Gastrointestinal and Immune Development and Function: A Preclinical Perspective. J. Pediatr. 2016, 173, S16–S28. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Breastfeeding and intelligence: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Belfort, M.B.; Rifas-Shiman, S.L.; Kleinman, K.P.; Guthrie, L.B.; Bellinger, D.C.; Taveras, E.M.; Gillman, M.W.; Oken, E. Infant feeding and childhood cognition at ages 3 and 7 years: Effects of breastfeeding duration and exclusivity. JAMA Pediatr. 2013, 167, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Horta, B.L.; de Mola, C.L.; Quevedo, L.; Pinheiro, R.T.; Gigante, D.P.; Gonçalves, H.; Barros, F.C. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: A prospective birth cohort study from Brazil. Lancet Glob. Health 2015, 3, e199–e205. [Google Scholar] [CrossRef]
- Van Odijk, J.; Kull, I.; Borres, M.P.; Brandtzaeg, P.; Edberg, U.; Hanson, L.A.; Høst, A.; Kuitunen, M.; Olsen, S.F.; Skerfving, S.; et al. Breastfeeding and allergic disease: A multidisciplinary review of the literature (1966–2001) on the mode of early feeding in infancy and its impact on later atopic manifestations. Allergy 2003, 58, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Dogaru, C.M.; Nyffenegger, D.; Pescatore, A.M.; Spycher, B.D.; Kuehni, C.E. Breastfeeding and childhood asthma: Systematic review and meta-analysis. Am. J. Epidemiol. 2014, 179, 1153–1167. [Google Scholar] [CrossRef] [PubMed]
- Amitay, E.L.; Keinan-Boker, L. Breastfeeding and Childhood Leukemia Incidence: A Meta-analysis and Systematic Review. JAMA Pediatr. 2015, 169, e151025. [Google Scholar] [CrossRef] [PubMed]
- Pudla, K.J.; Gonzaléz-Chica, D.A.; Vasconcelos, F.D.A.G.D. Effect of breastfeeding on obesity of schoolchildren: Influence of maternal education. Rev. Paul. Pediatr. 2015, 33, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Loret de Mola, C.; Victora, C.G. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Van Gysel, M.; Cossey, V.; Fieuws, S.; Schuermans, A. Impact of pasteurization on the antibacterial properties of human milk. Eur. J. Pediatr. 2012, 171, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Berens, P.; Eglash, A.; Malloy, M.; Steube, A.M. ABM Clinical Protocol #26: Persistent Pain with Breastfeeding. Breastfeed. Med. 2016, 11, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Little, K.M.; Hu, D.J.; Dominguez, K.L. HIV-1 and breastfeeding in the United States. Adv. Exp. Med. Biol. 2012, 743, 261–270. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. UNICEF Update on HIV and Infant Feeding; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Kurath, S.; Halwachs-Baumann, G.; Müller, W.; Resch, B. Transmission of cytomegalovirus via breast milk to the prematurely born infant: A systematic review. Clin. Microbiol. Infect. 2010, 16, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Hamprecht, K.; Maschmann, J.; Vochem, M.; Dietz, K.; Speer, C.P.; Jahn, G. Epidemiology of transmission of cytomegalovirus from mother to preterm infant by breastfeeding. Lancet 2001, 357, 513–518. [Google Scholar] [CrossRef]
- Vochem, M.; Hamprecht, K.; Jahn, G.; Speer, C.P. Transmission of cytomegalovirus to preterm infants through breast milk. Pediatr. Infect. Dis. J. 1998, 17, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Hamprecht, K.; Goelz, R. Postnatal Cytomegalovirus Infection through Human Milk in Preterm Infants: Transmission, Clinical Presentation, and Prevention. Clin. Perinatol. 2017, 44, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.A.; Ahmed, A.; Palmer, A.L.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; Tolan, R.W.; Novak, Z.; Chowdhury, N.; Fowler, K.B.; et al. Detection of congenital cytomegalovirus infection by real-time polymerase chain reaction analysis of saliva or urine specimens. J. Infect. Dis. 2014, 210, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Boppana, S.B.; Ross, S.A.; Shimamura, M.; Palmer, A.L.; Ahmed, A.; Michaels, M.G.; Sánchez, P.J.; Bernstein, D.I.; Tolan, R.W.; Novak, Z.; et al. Saliva polymerase-chain-reaction assay for cytomegalovirus screening in newborns. N. Engl. J. Med. 2011, 364, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Romero-Gómez, M.P.; Cabrera, M.; Montes-Bueno, M.T.; Cendejas-Bueno, E.; Segovia, C.; Pastrana, N.; Mingorance, J.; Omeñaca, F. Evaluation of cytomegalovirus infection in low-birth weight children by breast milk using a real-time polymerase chain reaction assay. J. Med. Virol. 2015, 87, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Agence française de sécurité sanitaire des aliments. Recommandations d’hygiène pour la préparation et la conservation des biberons. Available online: https://www.anses.fr/fr/system/files/MIC-Ra-BIB.pdf (accessed on 4 July 2015).
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O’Hare, D.; Schanler, R.J.; Eidelman, A.I. Breastfeeding and the Use of Human Milk. Pediatrics 2005, 115, 496–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omarsdottir, S.; Casper, C.; Akerman, A.; Polberger, S.; Vanpée, M. Breastmilk handling routines for preterm infants in Sweden: A national cross-sectional study. Breastfeed. Med. 2008, 3, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Lanzieri, T.M.; Dollard, S.C.; Josephson, C.D.; Schmid, D.S.; Bialek, S.R. Breast milk-acquired cytomegalovirus infection and disease in VLBW and premature infants. Pediatrics 2013, 131, e1937–e1945. [Google Scholar] [CrossRef] [PubMed]
- Eidelman, A.I.; Schanler, R.J.; Johnston, M.; Landers, S.; Noble, L.; Szucs, K.; Viehmann, L. Se Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef]
- Cheong, J.L.Y.; Cowan, F.M.; Modi, N. Gastrointestinal manifestations of postnatal cytomegalovirus infection in infants admitted to a neonatal intensive care unit over a five year period. Arch. Dis. Child. Fetal Neonatal Ed. 2004, 89, F367–F369. [Google Scholar] [CrossRef] [PubMed]
- Okulu, E.; Akin, I.M.; Atasay, B.; Ciftçi, E.; Arsan, S.; Türmen, T. Severe postnatal cytomegalovirus infection with multisystem involvement in an extremely low birth weight infant. J. Perinatol. 2012, 32, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, R.; Tagawa, M.; Sanjo, M.; Chiba, H.; Ito, T.; Yamada, M.; Nakae, S.; Suzuki, A.; Nishimura, H.; Naganuma, M.; et al. Severe postnatal cytomegalovirus infection in a very premature infant. Neonatology 2007, 92, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Fischer, C.; Meylan, P.; Bickle Graz, M.; Gudinchet, F.; Vaudaux, B.; Berger, C.; Roth-Kleiner, M. Severe postnatally acquired cytomegalovirus infection presenting with colitis, pneumonitis and sepsis-like syndrome in an extremely low birthweight infant. Neonatology 2010, 97, 339–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamele, M.; Flanagan, R.; Loomis, C.A.; Stevens, T.; Fairchok, M.P. Severe morbidity and mortality with breast milk associated cytomegalovirus infection. Pediatr. Infect. Dis. J. 2010, 29, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.-A.; Belhabri, S.; Karaoui, L. Erratum: Clinical Findings and Autopsy of a Preterm Infant with Breast Milk-Acquired Cytomegalovirus Infection. AJP Rep. 2016, 6, e367. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.S.; Benjamin, D.K.; Puopolo, K.M.; Laughon, M.M.; Clark, R.H.; Mukhopadhyay, S.; Benjamin, D.K.; Smith, P.B.; Permar, S.R. Postnatal Cytomegalovirus Infection and the Risk for Bronchopulmonary Dysplasia. JAMA Pediatr. 2015, 169, e153785. [Google Scholar] [CrossRef] [PubMed]
- Collège National des Gynécologues et Obstétriciens Français. Cytomégalovirus et grossesse. Available online: http://www.cngof.fr/actualites/403-cytomegalovirus-et-grossesse (accessed on 2 March 2016).
- Boumahni, B.; Robillard, P.-Y. Infection post-natale à cytomégalovirus chez l’enfant prématuré: Rôle du lait de mère. Arch. Pédiatr. 2014, 21, 1060–1061. [Google Scholar] [CrossRef] [PubMed]
- Croly-Labourdette, S.; Vallet, S.; Gagneur, A.; Gremmo-Feger, G.; Legrand-Quillien, M.-C.; Ansquer, H.; Jacquemot, L.; Narbonne, V.; Lintanf, J.; Collet, N.; et al. Transmission du cytomégalovirus par le lait maternel cru aux enfants prématurés: Étude épidémiologique pilote. Arch. Pédiatr. 2006, 13, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Picaud, J.C.; Buffin, R.; Gremmo-Feger, G.; Rigo, J.; Putet, G.; Casper, C.; Working group of the French Neonatal Society on fresh human milk use in preterm infants. Review concludes that specific recommendations are needed to harmonise the provision of fresh mother’s milk to their preterm infants. Acta Paediatr. 2018, 107, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Barbi, M.; Binda, S.; Primache, V.; Caroppo, S.; Didò, P.; Guidotti, P.; Corbetta, C.; Melotti, D. Cytomegalovirus DNA detection in Guthrie cards: A powerful tool for diagnosing congenital infection. J. Clin. Virol. 2000, 17, 159–165. [Google Scholar] [CrossRef]
- Binda, S.; Caroppo, S.; Didò, P.; Primache, V.; Veronesi, L.; Calvario, A.; Piana, A.; Barbi, M. Modification of CMV DNA detection from dried blood spots for diagnosing congenital CMV infection. J. Clin. Virol. 2004, 30, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Göhring, K.; Dietz, K.; Hartleif, S.; Jahn, G.; Hamprecht, K. Influence of different extraction methods and PCR techniques on the sensitivity of HCMV-DNA detection in dried blood spot (DBS) filter cards. J. Clin. Virol. 2010, 48, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Mussi-Pinhata, M.M.; Pinto, P.C.G.; Yamamoto, A.Y.; Berencsi, K.; de Souza, C.B.S.; Andrea, M.; Duarte, G.; Jorge, S.M. Placental transfer of naturally acquired, maternal cytomegalovirus antibodies in term and preterm neonates. J. Med. Virol. 2003, 69, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Mussi-Pinhata, M.M.; Yamamoto, A.Y.; do Carmo Rego, M.A.; Pinto, P.C.G.; da Motta, M.S.F.; Calixto, C. Perinatal or early-postnatal cytomegalovirus infection in preterm infants under 34 weeks gestation born to CMV-seropositive mothers within a high-seroprevalence population. J. Pediatr. 2004, 145, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Mehler, K.; Oberthuer, A.; Lang-Roth, R.; Kribs, A. High rate of symptomatic cytomegalovirus infection in extremely low gestational age preterm infants of 22–24 weeks’ gestation after transmission via breast milk. Neonatology 2014, 105, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Remington, J.; Klein, J.; Wilson, C.; Nizet, V.; Maldonado, Y. Infectious Diseases of the Fetus and Newborn, 7th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2011. [Google Scholar]
- Vauloup-Fellous, C.; Picone, O.; Cordier, A.-G.; Parent-du-Châtelet, I.; Senat, M.-V.; Frydman, R.; Grangeot-Keros, L. Does hygiene counseling have an impact on the rate of CMV primary infection during pregnancy? Results of a 3-year prospective study in a French hospital. J. Clin. Virol. 2009, 46, S49–S53. [Google Scholar] [CrossRef] [PubMed]
- Kimberlin, D.W.; Jester, P.M.; Sánchez, P.J.; Ahmed, A.; Arav-Boger, R.; Michaels, M.G.; Ashouri, N.; Englund, J.A.; Estrada, B.; Jacobs, R.F.; et al. National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group Valganciclovir for symptomatic congenital cytomegalovirus disease. N. Engl. J. Med. 2015, 372, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Omarsdottir, S.; Agnarsdottir, M.; Casper, C.; Orrego, A.; Vanpée, M.; Rahbar, A.; Söderberg-Nauclér, C. High prevalence of cytomegalovirus infection in surgical intestinal specimens from infants with necrotizing enterocolitis and spontaneous intestinal perforation: A retrospective observational study. J. Clin. Virol. 2017, 93, 57–64. [Google Scholar] [CrossRef] [PubMed]
- You, D.M.; Johnson, M.D. Cytomegalovirus infection and the gastrointestinal tract. Curr. Gastroenterol. Rep. 2012, 14, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Skeath, T.; Stewart, C.; Waugh, S.; Embleton, N.; Cummings, S.; Berrington, J. Cytomegalovirus and other common enteric viruses are not commonly associated with NEC. Acta Paediatr. 2016, 105, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Goelz, R.; Hamprecht, K.; Klingel, K.; Poets, C.F. Intestinal manifestations of postnatal and congenital cytomegalovirus infection in term and preterm infants. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2016, 83, 29–36. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| “Proven” Infections | Term at Birth | Weight at Birth | Age at Diagnosis (Day) | Symptoms | Missing Information | Source of Reference |
| 1 | 27 weeks 4 days | 550 g | 50 | “Sepsis-like”, NEC, death | / | Lopes et al., 2016 |
| 2 | 27 weeks 4 days | 1000 g | 50 | Asymptomatic | / | Lopes et al., 2016 |
| 3 | 26 weeks | 810 g | 70 | “Sepsis-like”, NEC, | / | This study |
| 4 | 27 weeks | 900 g | 60 | “Sepsis-like”, NEC | / | This study |
| 5 | 29 weeks | 1200 g | 53 | Asymptomatic | / | Croly-Labourlette et al., 2006 |
| “Highly probable” infections | ||||||
| 6 | 25 weeks 5 days | 900 g | 36 | Thrombocytopenia, hyperleukocytosis | CMV PCR on residual blood from transfusions | This study |
| 7 | 27 weeks | / | 30 | “Sepsis-like” | Elimination of congenital origin | This study |
| 8 | 27 weeks 5 days | 950 g | 41 | “Sepsis-lik”, thrombocytopenia NEC, death | Elimination of congenital origin | This study |
| 9 | 28 weeks | 1125 g | 60 | Thrombocytopenia | CMV reactivation in breast milk (stopped before) | Boumahni et al., 2014 |
| 10 | 30 weeks | 1500 g | 15 and 40 | Cholestasis “Sepsis-like” | CMV reactivation in breast milk | Radi et al., 2007 |
| 11 | 33 weeks | >2000 g | 20 | “Sepsis-like”, NEC | Elimination of congenital origin | This study |
| 12 | 33 weeks | >2000 g | 20 | Adenopathies | Elimination of congenital origin | This study |
| “Probable” infections | ||||||
| 13 | 25 weeks | 570 g | 90 | Unconfirmed hearing loss |  | This study |
| 14 | 32 weeks | >2000 | 35 | “Sepsis-like” | This study | |
| 15 | 32 weeks | 1950 | 60 | Severe leukopenia | This study |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, A.-A.; Champion, V.; Mitanchez, D. Nutrition of Preterm Infants and Raw Breast Milk-Acquired Cytomegalovirus Infection: French National Audit of Clinical Practices and Diagnostic Approach. Nutrients 2018, 10, 1119. https://doi.org/10.3390/nu10081119
Lopes A-A, Champion V, Mitanchez D. Nutrition of Preterm Infants and Raw Breast Milk-Acquired Cytomegalovirus Infection: French National Audit of Clinical Practices and Diagnostic Approach. Nutrients. 2018; 10(8):1119. https://doi.org/10.3390/nu10081119
Chicago/Turabian StyleLopes, Anne-Aurelie, Valerie Champion, and Delphine Mitanchez. 2018. "Nutrition of Preterm Infants and Raw Breast Milk-Acquired Cytomegalovirus Infection: French National Audit of Clinical Practices and Diagnostic Approach" Nutrients 10, no. 8: 1119. https://doi.org/10.3390/nu10081119