Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. Intake of Energy, Nutrients and Foods
2.3. Regularity of Breakfast Consumption
- Breakfast on each of the three study days: Regular consumer
- Breakfast on two of the study days: Irregular consumer
- Breakfast on just one or none of the days of the study: Skippers & no breakfast
2.4. Calculation of Dietary Quality of the Diet by NRF 9.3
2.5. Statistical Analysis
3. Results
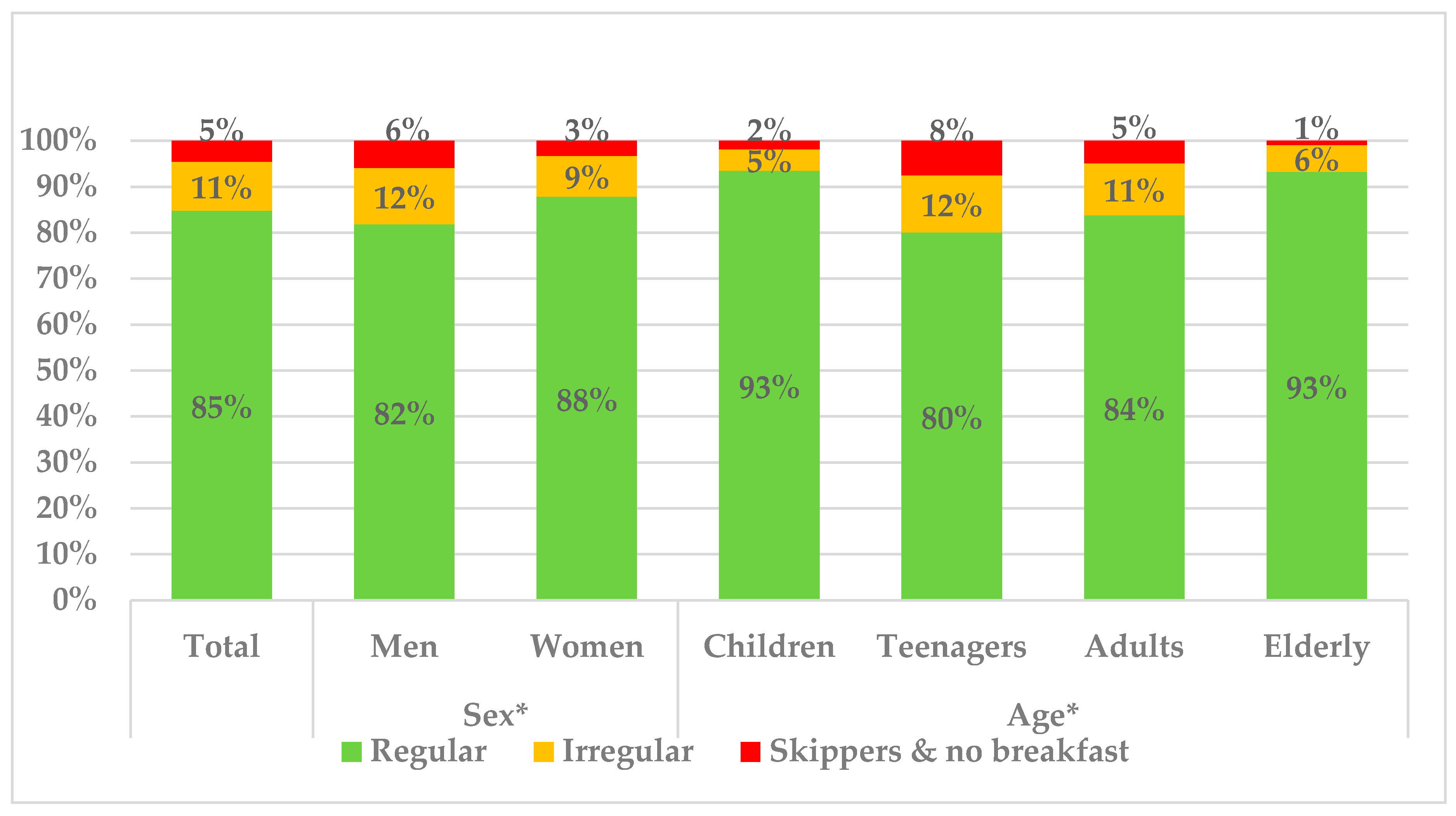
3.1. Regularity of Breakfast Consumption
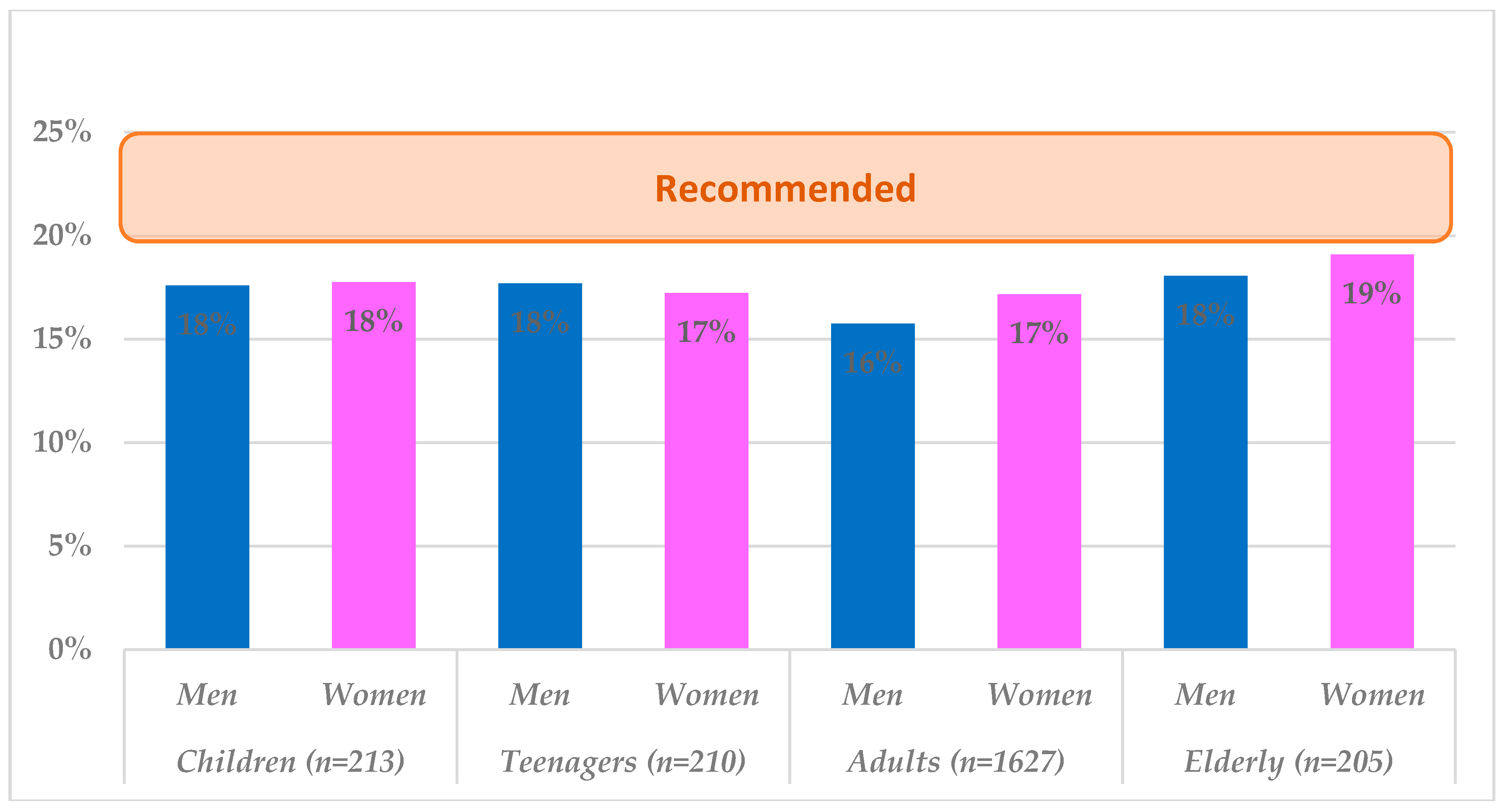
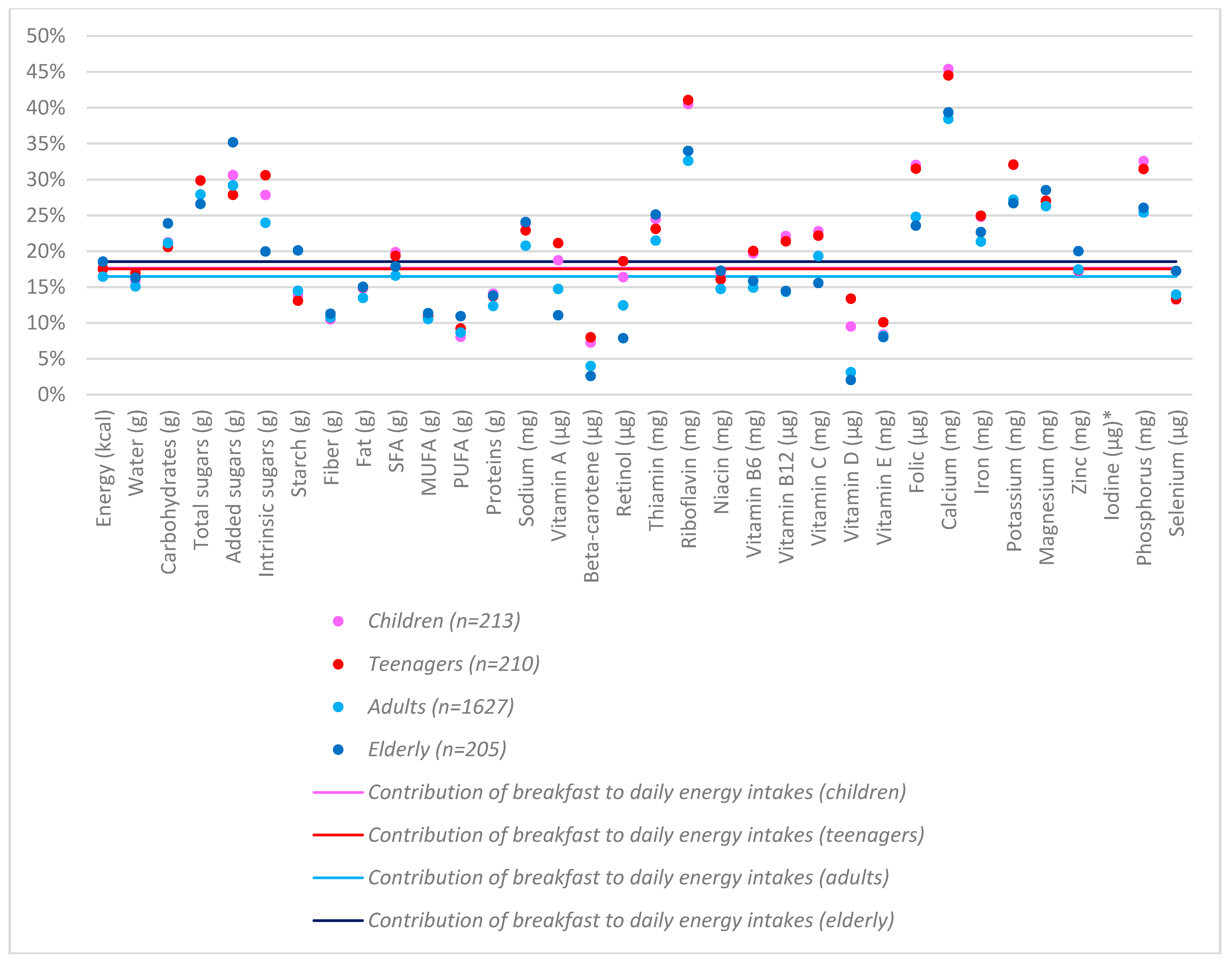
3.2. Contribution of Breakfast to Daily Energy and Nutrient Intakes
3.3. Contribution of Breakfast to Daily Food Groups Intakes in Spain
3.4. Diet Quality (DQ): Nutrient and Food Group Intakes at Breakfast by Tertiles of Daily Dietary Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pérez-Rodrigo, C.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of dietary patterns, lifestyles and overweight among spanish children and adolescents in the ANIBES study. Nutrients 2016, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- López-Sobaler, A.M.; Aparicio, A.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G. Overweight and general and abdominal obesity in a representative sample of Spanish adults: Findings from the anibes study. Biomed. Res. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud. España 2017; Ministerio de Sanidad, Consumo y Bienestar Social: Madrid, Spain, 2018.
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The role of breakfast in health: Definition and criteria for a quality breakfast. J. Acad. Nutr. Diet 2014, 114, S8–S26. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J. Defining nutritious breakfasts and their benefits. J. Acad. Nutr. Diet 2014, 114 (Suppl. 12), S5–S7. [Google Scholar] [CrossRef]
- Corder, K.; van Sluijs, E.M.; Ridgway, C.L.; Steele, R.M.; Prynne, C.J.; Stephen, A.M.; Bamber, D.J.; Dunn, V.J.; Goodyer, I.M.; Ekelund, U. Breakfast consumption and physical activity in adolescents: Daily associations and hourly patterns. Am. J. Clin. Nutr. 2014, 99, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Moreno, E.; Valero Gaspar, T.; Rodríguez Alonso, P.; Díaz-Roncero González, A.; Gómez Carús, A.; Ávila Torres, J.M.; Varela-Moreiras, G. Estado de Situación Sobre el Desayuno en Espana; Fundación Española de la Nutrición: Madrid, Spain, 2018. [Google Scholar]
- Dye, L. The Importance of Breakfast in Europe. A Review of National Policies and Health Campaigns: European Breakfast Cereal Association 2017. Available online: http://www.breakfastisbest.eu/docs/102017/BIB_Report_Executive_Summary_Importance_of_Breakfast_in_Europe_2017.pdf (accessed on 21 July 2018).
- Gibney, M.J.; Barr, S.I.; Bellisle, F.; Drewnowski, A.; Fagt, S.; Livingstone, B.; Masset, G.; Varela Moreiras, G.; Moreno, L.A.; Smith, J.; et al. Breakfast in human nutrition: The International Breakfast Research Initiative. Nutrients 2018, 10, 559. [Google Scholar] [CrossRef] [PubMed]
- Aranceta, J.; Serra-Majem, L.; Arija, V.; Gil, A.; de Martínez, V.E.; Ortega, R. Objetivos nutricionales para la población española. Consenso de la Sociedad Española de Nutrición Comunitaria. Rev. Esp. Nutr. Comunitaria 2011, 17, 178–199. [Google Scholar]
- Grupo Colaborativo de la Sociedad Española de Nutrición Comunitaria (SENC); Bartrina, J.A.; Val, V.A.; Aldalur, E.M.; Muñoz, E.M.d.; Anta, R.M.O.; Pérez-Rodrigo, C.; Izquierdo, J.Q.; Martín, A.R.; Viñas, B.R.; et al. Guías alimentarias para la población española (SENC, diciembre 2016); la nueva pirámide de la alimentación saludable. Nutr. Hosp. 2016, 33 (Suppl. 8), 1–48. [Google Scholar]
- Uzhova, I.; Fuster, V.; Fernandez-Ortiz, A.; Ordovas, J.M.; Sanz, J.; Fernandez-Friera, L.; Lopez-Melgar, B.; Mendiguren, J.M.; Ibanez, B.; Bueno, H.; et al. The importance of breakfast in atherosclerosis disease: Insights from the PESA study. J. Am. Coll. Cardiol. 2017, 70, 1833–1842. [Google Scholar] [CrossRef] [PubMed]
- Navia, B.; López-Sobaler, A.M.; Villalobos, T.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Breakfast habits and differences regarding abdominal obesity in a cross-sectional study in Spanish adults: The ANIBES study. PLoS ONE 2017, 12, E0188828. [Google Scholar] [CrossRef] [PubMed]
- Hallstrom, L.; Labayen, I.; Ruiz, J.R.; Patterson, E.; Vereecken, C.A.; Breidenassel, C.; Gottrand, F.; Huybrechts, I.; Manios, Y.; Mistura, L.; et al. Breakfast consumption and cvd risk factors in european adolescents: The HELENA (healthy lifestyle in Europe by nutrition in adolescence) study. Public Health Nutr. 2013, 16, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Castillo, A.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. The ANIBES study on energy balance in spain: Design, protocol and methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos/Guía de Prácticas, 16th ed.; Ediciones Pirámide: Madrid, Spain, 2013. [Google Scholar]
- Fulgoni, V.L., III; Keast, D.R.; Drewnowski, A. Development and validation of the Nutrient-Rich Foods Index: A tool to measure nutritional quality of foods. J. Nutr. 2009, 139, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A. The Nutrient Rich Foods Index helps to identify healthy, affordable foods. Am. J. Clin. Nutr. 2010, 91, 1095S–1101S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Guideline: Sugars Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2015. [Google Scholar]
- European Food Safety Authority (EFSA). Dietary Reference Values for Nutrients: Summary Report; EFSA Supporting Publication: Parma, Italy, 2017. [Google Scholar]
- Zhang, L.; Cordeiro, L.S.; Liu, J.; Ma, Y. The association between breakfast skipping and body weight, nutrient intake and metabolic measures among participants with metabolic syndrome. Nutrients 2017, 9, 384. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh-Taskar, P.R.; Nicklas, T.A.; O’Neil, C.E.; Keast, D.R.; Radcliffe, J.D.; Cho, S. The relationship of breakfast skipping and type of breakfast consumption with nutrient intake and weight status in children and adolescents: The national health and nutrition examination survey 1999–2006. J. Am. Diet. Assoc. 2010, 110, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, E.J.; Dawson, J.; Alcorn, A.; Larsen, L.H.; Thomas, E.A.; Cardel, M.; Bourland, A.C.; Astrup, A.; St-Onge, M.P.; Hill, J.O.; et al. The effectiveness of breakfast recommendations on weight loss: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.E.; Chiuve, S.E.; Mekary, R.A.; Jensen, M.K.; Flint, A.J.; Hu, F.B.; Rimm, E.B. Prospective Study of Breakfast Eating and Incident Coronary Heart Disease in a Cohort of Male US Health Professionals Clinical Perspective. Circulation 2013, 128, 337–343. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.-P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P. Meal timing and frequency: Implications for cardiovascular disease prevention: A scientific statement from the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, E.; Aparicio, A.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Low adherence to dietary guidelines in Spain, especially in the overweight/obese population: The ANIBES Study. J. Am. Coll. Nutr. 2016, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, G.; Ahluwalia, N.; Niclasen, B.; Pammolli, A.; Vereecken, C.; Rasmussen, M.; Pedersen, P.T.; Kelly, C. Trends from 2002 to 2010 in Daily Breakfast Consumption and its Socio-Demographic Correlates in Adolescents across 31 Countries Participating in the HBSC Study. PLoS ONE. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermengildo, Y.; López-García, E.; García-Esquinas, E.; Pérez-Tasigchana, R.F.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Distribution of energy intake throughout the day and weight gain: A population-based cohort study in Spain. Br. J. Nutr. 2016, 115, 2003–2010. [Google Scholar] [CrossRef] [PubMed]
- Serra Majem, L.; Aranceta Bartrina, J.; Ribas Barba, L.; Pérez Rodrigo, C.; García Closas, R. Estudio enKid: Objetivos y metodología. In Desayuno y equilibrio alimentario. Estudio enKid; Masson: Barcelona, Spain, 2000. [Google Scholar]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Portal Estadístico del SNS. Encuesta Nacional de Salud en España 2011/2012. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2011.htm (accessed on 10 August 2018).
- Agencia, Española de Consumo, Seguridad Alimentaria y Nutrición. Ministerio de Sanidad, Servicios Sociales e Igualdad (2016). Estudio de Vigilancia del Crecimiento, Alimentación, Actividad Física, Desarrollo Infantil y Obesidad en España 2015. Madrid. Available online: http://www.aecosan.msssi.gob.es/AECOSAN/docs/documentos/nutricion/observatorio/Estudio_ALADINO_2015.pdf (accessed on 10 August 2018).
- Ruiz, E.; del Pozo, S.; Valero, T.; Avila, J.M.; Varela-Moreiras, G. Estudio de hábitos alimentarios y estilos de vida de los universitarios españoles. Fundación Española de la Nutrición (FEN), 2013. Available online: https://www.fen.org.es/storage/app/media/imgPublicaciones/30092014131915.pdf (accessed on 10 August 2018).
- Plaza Díaz, J.; Valero, G.T.; Varela-Moreiras, G.; Gil, H.Á. La leche como vehículo de salud para la población. Calcio y sus determinantes en la salud de la población española. Fundación Española de la Nutrición (FEN) y Fundación Iberoamericana de la Nutrición (FINUT), 2017. Available online: http://www.finut.org/wp-content/uploads/2017/09/Libro-La-leche-como-veh%C3%ADculo-de-salud-version-Online.pdf (accessed on 12 August 2018).
- Olza, J.; Aranceta-Bartrina, J.; Gonza-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported dietary intake, disparity between the reported consumption and the level needed for adequacy and food sources of calcium, phosphorus, magnesium and vitamin d in the Spanish population: Findings from the anibes study. Nutrients 2017, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carvajal, A.; Cabrera, L.; Cuadrado, C. Ingestas Recomendadas de energía y nutrientes para la población española; Pirámide: Madrid, Spain, 2015; pp. 258–259. [Google Scholar]
- Partearroyo, T.; Samaniego-Vaesken, M.L.; Ruiz, E.; Olza, J.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary sources and intakes of folates and vitamin B12 in the Spanish population: Findings from the ANIBES study. PLoS ONE 2017, 12, E0189230. [Google Scholar] [CrossRef] [PubMed]
- Samaniego-Vaesken, M.; Alonso-Aperte, E.; Varela-Moreiras, G. Voluntary Folic Acid Fortification Levels and Nutrient Composition of Food Products from the Spanish Market: A 2011–2015 Update. Nutrients 2017, 9, 234. [Google Scholar] [CrossRef] [PubMed]
- Samaniego-Vaesken, M.L.; Alonso-Aperte, E.; Varela-Moreiras, G. Voluntary fortification with folic acid in Spain: An updated food composition database. Food Chem. 2016, 193, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G. The benefits of breakfast cereal consumption: A systematic review of the evidence base. Adv. Nutr. 2014, 5, 636S–673S. [Google Scholar] [CrossRef] [PubMed]
- Samaniego-Vaesken, M.; Alonso-Aperte, E.; Varela-Moreiras, G. Contribution of folic acid-fortified foods to fertile women’s folate Recommended Nutrient Intake through breakfast simulation models. Public Health Nutr. 2015, 18, 1960–1968. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Macronutrient distribution and dietary sources in the spanish population: Findings from the anibes study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, U.P.; Mazquiaran, B.L.; Rodríguez, A.P.; Valero, G.T.; Ruiz, M.E.; Ávila, T.J.M.; Varela-Moreiras, G. Informe de estado de situación sobre frutas y hortalizas: Nutrición y salud en la España del siglo XXI; Fundación Española de la Nutrición: Madrid, Spain, 2018; Available online: http://www.fen.org.es/storage/app/media/imgPublicaciones/INFORME_FRUTAS_Y_HORTALIZAS_FEN_2018.pdf (accessed on 14 August 2018).
- Estudio ENALIA 2012–2014: Encuesta Nacional de consumo de Alimentos en población Infantil y Adolescente. Agencia Española de Consumo, Seguridad Alimentaria y Nutrición. Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, 2017. Available online: http://www.aecosan.msssi.gob.es/AECOSAN/docs/documentos/seguridad_alimentaria/gestion_riesgos/Informe_ENALIA2014_FINAL.pdf (accessed on 12 August 2018).
- Poslusna, K.; Ruprich, J.; de Vries, J.H.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 h recalls, control and adjustment methods in practice. Br. J. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total | Sex | Age | |||||
|---|---|---|---|---|---|---|---|
| Men | Women | Children | Teenagers | Adults | Elderly | ||
| Regular | 1704 | 829 | 875 | 199 | 169 | 1387 | 192 |
| Irregular | 212 | 124 | 88 | 10 | 26 | 186 | 12 |
| Skippers | 64 | 39 | 25 | 4 | 15 | 54 | 1 |
| TOTAL | 1980 | 992 | 988 | 213 | 210 | 1627 | 205 |
| Total Population (n = 1980) | Children (n = 213) | Teenagers (n = 210) | Adults (n = 1627) | Elderly (n = 205) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breakfast | Daily | % Daily Intakes | Breakfast | Daily | % Daily Intakes | Breakfast | Daily | % Daily Intakes | Breakfast | Daily | % Daily Intakes | Breakfast | Daily | % Daily Intakes | |
| Energy (kcal) | 296 | 1777 | 17% | 342 | 1936 | 18% | 349 | 1989 | 18% | 293 | 1782 | 16% | 295 | 1591 | 19% |
| Water (g) | 240.1 | 1573.3 | 15% | 215.3 | 1353.3 | 16% | 221.3 | 1303.7 | 17% | 243.2 | 1608.7 | 15% | 251.9 | 1544.3 | 16% |
| Carbohydrates (g) | 38.4 | 180.8 | 21% | 44.7 | 210.5 | 21% | 45.3 | 219.9 | 21% | 37.9 | 179.4 | 21% | 38.2 | 159.7 | 24% |
| Total sugars (g) | 20.2 | 72.8 | 28% | 26.5 | 88.5 | 30% | 25.7 | 86.2 | 30% | 19.9 | 71.4 | 28% | 18.5 | 69.5 | 27% |
| Added sugars (g) | 8.5 | 29.1 | 29% | 14.0 | 45.8 | 31% | 13.3 | 47.6 | 28% | 8.3 | 28.6 | 29% | 6.2 | 17.6 | 35% |
| Intrinsic sugars (g) | 9.5 | 39.9 | 24% | 11.4 | 40.8 | 28% | 11.0 | 36.0 | 31% | 9.4 | 39.2 | 24% | 9.8 | 49.2 | 20% |
| Starch (g) | 15.5 | 105.3 | 15% | 16.6 | 119.8 | 14% | 17.2 | 131.1 | 13% | 15.3 | 105.3 | 15% | 17.6 | 87.5 | 20% |
| Fibre (g) | 1.3 | 12.1 | 11% | 1.2 | 11.5 | 11% | 1.2 | 11.3 | 11% | 1.3 | 12.1 | 11% | 1.6 | 14.0 | 11% |
| Total Fat (g) | 10.4 | 76.0 | 14% | 12.4 | 83.7 | 15% | 12.6 | 84.1 | 15% | 10.3 | 76.5 | 13% | 9.9 | 65.8 | 15% |
| SFA (g) | 3.9 | 23.1 | 17% | 5.6 | 28.1 | 20% | 5.3 | 27.5 | 19% | 3.8 | 23.2 | 17% | 3.3 | 18.6 | 18% |
| MUFA (g) | 3.5 | 32.8 | 11% | 3.8 | 34.2 | 11% | 3.7 | 34.3 | 11% | 3.5 | 33.0 | 11% | 3.4 | 29.9 | 11% |
| PUFA (g) | 1.1 | 12.8 | 9% | 1.1 | 13.7 | 8% | 1.3 | 14.1 | 9% | 1.1 | 13.0 | 9% | 1.2 | 10.7 | 11% |
| Protein (g) | 9.2 | 73.0 | 13% | 10.8 | 76.5 | 14% | 10.8 | 78.6 | 14% | 9.1 | 73.4 | 12% | 9.2 | 66.3 | 14% |
| Vitamin A (µg) | 34.3 | 236.3 | 15% | 51.5 | 274.9 | 19% | 50.6 | 239.5 | 21% | 34.8 | 236.2 | 15% | 24.6 | 222.0 | 11% |
| Beta-carotene (µg) | 18.0 | 445.1 | 4% | 26.2 | 360.4 | 7% | 26.8 | 335.2 | 8% | 18.1 | 450.8 | 4% | 14.0 | 532.9 | 3% |
| Retinol (µg) | 13.9 | 115.7 | 12% | 27.1 | 165.4 | 16% | 25.8 | 138.5 | 19% | 14.2 | 114.2 | 12% | 7.5 | 95.4 | 8% |
| Thiamine (mg) | 0.17 | 0.75 | 22% | 0.20 | 0.82 | 25% | 0.20 | 0.85 | 23% | 0.16 | 0.76 | 22% | 0.17 | 0.67 | 25% |
| Riboflavin (mg) | 0.33 | 0.98 | 33% | 0.46 | 1.13 | 41% | 0.43 | 1.06 | 41% | 0.32 | 0.98 | 33% | 0.32 | 0.94 | 34% |
| Niacin (mg) | 3.1 | 20.7 | 15% | 3.5 | 20.6 | 17% | 3.5 | 21.9 | 16% | 3.1 | 21.0 | 15% | 3.2 | 18.2 | 17% |
| Vitamin B6 (mg) | 0.14 | 0.94 | 15% | 0.19 | 0.95 | 20% | 0.20 | 0.98 | 20% | 0.14 | 0.94 | 15% | 0.14 | 0.90 | 16% |
| Vitamin B12 (µg) | 0.45 | 3.01 | 15% | 0.66 | 2.97 | 22% | 0.59 | 2.75 | 21% | 0.43 | 3.03 | 14% | 0.43 | 2.96 | 14% |
| Vitamin C (mg) | 5.2 | 28.1 | 19% | 5.7 | 24.9 | 23% | 4.9 | 22.0 | 22% | 5.5 | 28.3 | 19% | 5.4 | 34.5 | 16% |
| Vitamin D (µg) | 0.0 | 1.4 | 3% | 0.1 | 1.1 | 10% | 0.1 | 1.1 | 13% | 0.0 | 1.4 | 3% | 0.0 | 1.4 | 2% |
| Vitamin E (mg) | 0.3 | 3.7 | 8% | 0.3 | 4.0 | 8% | 0.4 | 4.1 | 10% | 0.3 | 3.8 | 8% | 0.2 | 3.1 | 8% |
| Folates (µg) | 21.5 | 85.8 | 25% | 29.4 | 91.7 | 32% | 27.9 | 88.6 | 32% | 21.3 | 85.8 | 25% | 19.7 | 83.5 | 24% |
| Calcium (mg) | 196.9 | 502.0 | 39% | 285.0 | 627.6 | 45% | 260.1 | 584.2 | 45% | 189.6 | 493.0 | 38% | 186.9 | 474.5 | 39% |
| Iron (mg) | 1.5 | 6.7 | 22% | 1.8 | 7.1 | 25% | 1.8 | 7.2 | 25% | 1.4 | 6.7 | 21% | 1.4 | 6.3 | 23% |
| Potassium (mg) | 410.4 | 1491.6 | 28% | 503.5 | 1570.7 | 32% | 482.7 | 1504.0 | 32% | 404.3 | 1487.1 | 27% | 405.5 | 1517.6 | 27% |
| Magnesium (mg) | 37.8 | 142.8 | 26% | 38.7 | 146.8 | 26% | 38.8 | 143.4 | 27% | 37.7 | 143.2 | 26% | 40.1 | 140.4 | 29% |
| Zinc (mg) | 1.0 | 5.9 | 18% | 1.1 | 6.1 | 17% | 1.1 | 6.3 | 17% | 1.0 | 6.0 | 17% | 1.1 | 5.4 | 20% |
| Iodine (µg) | 115.6 | 135.9 | 85% | 160.2 | 188.0 | 85% | 148.2 | 158.7 | 93% | 110.7 | 131.2 | 84% | 114.2 | 144.0 | 79% |
| Selenium (µg) | 7.9 | 55.6 | 14% | 7.6 | 57.2 | 13% | 7.9 | 59.4 | 13% | 7.8 | 55.8 | 14% | 8.8 | 50.9 | 17% |
| Phosphorus (mg) | 217.7 | 835.5 | 26% | 302.8 | 929.6 | 33% | 282.9 | 898.9 | 31% | 211.7 | 833.5 | 25% | 203.0 | 779.6 | 26% |
| Sodium (mg) | 295.2 | 1383.6 | 21% | 369.7 | 1548.7 | 24% | 363.2 | 1584.0 | 23% | 288.0 | 1385.5 | 21% | 284.9 | 1182.8 | 24% |
| n = 1980 | % of Consumers | Mean Intake (g) | Energy (kcal) | Total Sugars (g) | Added Sugars (g) | Fibre (g) | SFA (g) | Sodium (mg) | Vitamin A (µg) | Vitamin D (µg) | Folates (µg) | Calcium (mg) | Iron (mg) | Potassium (mg) | Phosphorus (mg) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MILK AND DAIRY PRODUCTS | 1716 | 87% | 155.4 | 84.5 | 8.1 | 0.7 | 0.0 | 1.9 | 98.2 | 27.3 | 0.0 | 8.1 | 208.0 | 0.2 | 237.7 | 158.2 |
| Cheeses | 201 | 10% | 17.7 | 52.5 | 0.5 | 0.0 | 0.0 | 2.4 | 164.2 | 44.0 | 0.0 | 3.2 | 93.2 | 0.1 | 29.4 | 94.5 |
| Milk | 1599 | 81% | 153.8 | 74.6 | 7.4 | 0.1 | 0.0 | 1.5 | 78.1 | 21.6 | 0.0 | 7.7 | 198.2 | 0.2 | 232.2 | 145.5 |
| Semi-skimmed milk | 854 | 43% | 131.6 | 56.6 | 5.8 | 0.0 | 0.0 | 1.1 | 65.8 | 0.0 | 0.0 | 6.6 | 173.7 | 0.1 | 197.4 | 125.0 |
| Skimmed milk | 428 | 22% | 139.0 | 48.7 | 7.0 | 0.0 | 0.0 | 0.1 | 72.3 | 0.0 | 0.0 | 7.0 | 180.7 | 0.1 | 208.5 | 132.1 |
| Whole milk | 585 | 30% | 125.2 | 82.6 | 6.3 | 0.0 | 0.0 | 2.4 | 62.6 | 57.6 | 0.0 | 6.3 | 151.5 | 0.1 | 187.8 | 115.2 |
| Other dairy products | 61 | 3% | 105.9 | 100.7 | 11.8 | 8.2 | 0.1 | 2.2 | 70.9 | 31.3 | 0.2 | 6.1 | 125.1 | 0.3 | 181.4 | 110.3 |
| Yogurt and fermented milk | 155 | 8% | 69.9 | 58.0 | 7.9 | 3.6 | 0.0 | 1.1 | 40.7 | 10.5 | 0.0 | 3.9 | 88.3 | 0.1 | 127.0 | 84.5 |
| GRAINS | 1690 | 85% | 44.7 | 159.3 | 4.3 | 3.7 | 1.6 | 1.4 | 184.7 | 9.5 | 0.2 | 14.7 | 29.0 | 1.1 | 57.4 | 56.7 |
| Bakery and pastry | 922 | 47% | 34.5 | 151.3 | 5.6 | 5.3 | 1.2 | 2.4 | 112.2 | 16.9 | 0.1 | 6.6 | 27.2 | 0.6 | 44.2 | 48.8 |
| Bread | 1012 | 51% | 33.1 | 92.5 | 0.7 | 0.2 | 1.1 | 0.1 | 175.8 | 0.0 | 0.0 | 4.7 | 14.6 | 0.6 | 41.6 | 35.1 |
| White bread | 859 | 43% | 32.0 | 89.4 | 0.7 | 0.1 | 0.8 | 0.1 | 173.6 | 0.0 | 0.0 | 3.5 | 14.3 | 0.6 | 32.7 | 28.2 |
| Whole bread | 214 | 11% | 24.1 | 62.1 | 0.5 | 0.2 | 1.8 | 0.1 | 119.2 | 0.1 | 0.0 | 7.3 | 9.8 | 0.6 | 58.7 | 47.2 |
| Breakfast cereals and cereal bars | 288 | 15% | 22.5 | 85.8 | 4.8 | 4.2 | 0.9 | 0.2 | 103.7 | 0.0 | 1.0 | 43.4 | 27.4 | 1.9 | 9.9 | 22.6 |
| Grains and flours | 158 | 8% | 18.5 | 66.5 | 0.1 | 0.0 | 1.2 | 0.1 | 5.9 | 0.1 | 0.0 | 9.1 | 7.6 | 0.7 | 46.6 | 53.1 |
| NON-ALCOHOLIC BEVERAGES | 1547 | 78% | 139.2 | 15.7 | 3.0 | 0.7 | 0.0 | 0.0 | 5.4 | 2.6 | 0.0 | 3.6 | 6.1 | 0.2 | 85.6 | 10.6 |
| Coffee and infusions | 1228 | 62% | 69.9 | 3.0 | 0.5 | 0.0 | 0.0 | 0.0 | 2.4 | 0.0 | 0.0 | 0.0 | 4.0 | 0.1 | 65.5 | 5.5 |
| Juices and nectars | 237 | 12% | 112.8 | 52.4 | 12.5 | 0.7 | 0.1 | 0.0 | 5.7 | 16.9 | 0.0 | 14.0 | 11.7 | 0.4 | 160.8 | 15.2 |
| Other drinks (non-alcohol) | 124 | 6% | 126.5 | 47.8 | 4.7 | 2.7 | 0.0 | 0.3 | 29.7 | 0.0 | 0.0 | 17.6 | 12.1 | 0.4 | 111.7 | 43.7 |
| Water | 489 | 25% | 164.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| SUGAR AND SWEETS | 1510 | 76% | 11.6 | 42.1 | 8.7 | 8.4 | 0.0 | 0.3 | 39.1 | 0.5 | 0.0 | 1.6 | 3.2 | 0.2 | 65.4 | 31.8 |
| Chocolates | 611 | 31% | 12.1 | 47.0 | 7.3 | 7.2 | 0.0 | 0.6 | 95.3 | 0.8 | 0.0 | 3.9 | 6.1 | 0.5 | 156.5 | 77.2 |
| Jams and others | 255 | 13% | 13.6 | 36.5 | 9.1 | 7.5 | 0.1 | 0.0 | 2.7 | 1.0 | 0.0 | 0.0 | 3.0 | 0.0 | 8.8 | 2.5 |
| Other sweets | 257 | 13% | 0.3 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Sugar | 863 | 44% | 7.6 | 29.5 | 7.4 | 7.4 | 0.0 | 0.0 | 0.2 | 0.0 | 0.0 | 0.0 | 0.4 | 0.0 | 1.0 | 0.1 |
| OILS AND FATS | 841 | 42% | 10.1 | 80.4 | 0.0 | 0.0 | 0.0 | 2.8 | 21.5 | 52.5 | 0.0 | 0.0 | 0.7 | 0.0 | 0.7 | 0.7 |
| Butter, margarine and shortening | 429 | 22% | 12.2 | 89.4 | 0.0 | 0.0 | 0.0 | 4.2 | 42.1 | 102.2 | 0.1 | 0.0 | 1.5 | 0.0 | 1.5 | 1.3 |
| Olive oil | 475 | 24% | 6.4 | 57.3 | 0.0 | 0.0 | 0.0 | 1.0 | 0.0 | 0.6 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| FRUITS | 415 | 21% | 123.9 | 64.5 | 11.3 | 0.0 | 1.7 | 0.2 | 3.0 | 20.8 | 0.0 | 22.3 | 19.8 | 0.4 | 225.5 | 27.7 |
| Fresh fruit | 289 | 15% | 127.9 | 55.3 | 10.9 | 0.0 | 2.1 | 0.1 | 2.8 | 25.0 | 0.0 | 13.7 | 16.4 | 0.4 | 219.4 | 20.8 |
| Fresh fruit juice | 118 | 6% | 109.1 | 46.9 | 10.9 | 0.0 | 0.1 | 0.0 | 1.1 | 10.9 | 0.0 | 40.4 | 16.9 | 0.2 | 181.1 | 20.7 |
| MEAT AND MEAT PRODUCTS | 386 | 19% | 28.4 | 68.2 | 0.1 | 0.1 | 0.0 | 1.6 | 226.1 | 85.6 | 0.0 | 0.8 | 3.5 | 0.6 | 66.1 | 45.6 |
| VEGETABLES | 242 | 12% | 19.0 | 4.2 | 0.6 | 0.0 | 0.3 | 0.0 | 3.2 | 25.1 | 0.0 | 4.7 | 2.9 | 0.1 | 50.1 | 5.2 |
| SAUCES AND CONDIMENTS | 215 | 11% | 1.2 | 3.1 | 0.0 | 0.0 | 0.0 | 0.0 | 45.6 | 2.6 | 0.0 | 2.0 | 1.8 | 0.0 | 4.0 | 9.7 |
| EGGS | 136 | 7% | 23.7 | 27.8 | 0.0 | 0.0 | 0.0 | 0.5 | 32.2 | 32.3 | 0.3 | 9.1 | 9.9 | 0.3 | 28.8 | 35.6 |
| Children/Teenagers (9–17 Years) | Adults (18–75 Years) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (Low) | T2 (Middle) | T3 (High) | p-Value | p-Value Adjusted for Daily Energy | T1 (Low) | T2 (Middle) | T3 (High) | p-Value | p-Value Adjusted for Daily Energy | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||||
| Daily NRF9.3 score | 352.5 | 51.2 | 460.0 | 24.7 | 556.3 | 42.9 | 0.000 | 0.000 | 398.5 | 54.3 | 514.2 | 26.8 | 628.3 | 52.4 | 0.000 | 0.000 |
| Energy (kcal) | 333 | 18 | 355 | 16 | 348 | 17 | 0.469 | - | 290 | 32 | 300 | 24 | 290 | 19 | 0.506 | - |
| Water (g) | 189 | 4 | 223 | 4 | 246 | 4 | 0.000 | 0.000 | 211 | 5 | 240 | 4 | 284 | 5 | 0.000 | 0.000 |
| Carbohydrates (g) | 42.6 | 2.2 | 45.7 | 2.0 | 46.9 | 2.4 | 0.177 | 0.029 | 36.3 | 3.6 | 38.3 | 3.1 | 39.2 | 2.7 | 0.059 | 0.000 |
| Total sugars (g) | 24.6 | 1.5 | 26.6 | 1.2 | 27.2 | 1.6 | 0.168 | 0.323 | 18.8 | 2.0 | 19.7 | 2.0 | 20.8 | 2.0 | 0.016 | 0.001 |
| Added sugars (g) | 14.5 | 1.6 | 14.1 | 1.4 | 12.4 | 1.6 | 0.137 | 0.008 | 9.9 | 2.3 | 8.4 | 2.3 | 6.2 | 2.0 | 0.000 | 0.000 |
| Intrinsic sugars (g) | 9.0 | 2.7 | 11.5 | 2.6 | 13.3 | 3.4 | 0.000 | 0.000 | 7.1 | 3.7 | 9.2 | 3.9 | 12.4 | 4.1 | 0.000 | 0.000 |
| Starch (g) | 15.4 | 3.4 | 17.3 | 2.5 | 18.0 | 2.5 | 0.251 | 0.168 | 14.7 | 4.5 | 15.8 | 3.8 | 16.1 | 3.0 | 0.229 | 0.008 |
| Fibre (g) | 0.95 | 0.34 | 1.37 | 0.33 | 1.34 | 0.31 | 0.007 | 0.007 | 1.01 | 0.48 | 1.27 | 0.49 | 1.76 | 0.57 | 0.000 | 0.000 |
| Fat (g) | 12.8 | 1.3 | 13.2 | 1.4 | 11.6 | 1.2 | 0.235 | 0.001 | 11.1 | 2.4 | 11.1 | 1.8 | 8.8 | 1.5 | 0.000 | 0.000 |
| Saturates (g) | 5.7 | 0.6 | 5.7 | 0.5 | 5.0 | 0.5 | 0.107 | 0.001 | 4.3 | 0.9 | 4.1 | 0.7 | 3.1 | 0.6 | 0.000 | 0.000 |
| Monounsaturates (g) | 3.8 | 0.5 | 3.9 | 0.5 | 3.6 | 0.5 | 0.640 | 0.091 | 3.7 | 0.9 | 3.8 | 0.7 | 3.0 | 0.7 | 0.000 | 0.000 |
| Polyunsaturates (g) | 1.25 | 3.20 | 1.31 | 3.48 | 1.04 | 3.01 | 0.307 | 0.128 | 1.18 | 4.15 | 1.28 | 3.71 | 0.95 | 3.47 | 0.003 | 0.000 |
| Omega 3 fatty acids | 0.08 | 2.01 | 0.09 | 2.30 | 0.07 | 2.21 | 0.556 | 0.470 | 0.07 | 2.68 | 0.07 | 2.54 | 0.05 | 2.70 | 0.008 | 0.002 |
| Omega 6 fatty acids | 1.06 | 3.18 | 1.10 | 3.51 | 0.83 | 3.00 | 0.185 | 0.055 | 0.92 | 4.28 | 0.91 | 3.88 | 0.63 | 3.45 | 0.000 | 0.000 |
| Protein (g) | 9.8 | 0.6 | 11.2 | 0.5 | 11.5 | 0.6 | 0.010 | 0.002 | 8.3 | 1.2 | 9.0 | 0.9 | 10.1 | 0.8 | 0.000 | 0.000 |
| Carbohydrates (%) | 52.2 | 9.5 | 52.6 | 9.9 | 54.7 | 10.3 | 0.081 | 0.058 | 53.0 | 15.3 | 52.6 | 13.4 | 55.3 | 13.1 | 0.001 | 0.004 |
| Total sugars (%) | 32.8 | 13.9 | 32.2 | 11.7 | 33.0 | 11.9 | 0.848 | 0.863 | 32.5 | 21.1 | 30.9 | 18.6 | 32.1 | 16.8 | 0.302 | 0.270 |
| Added sugars (%) | 19.7 | 10.5 | 17.3 | 8.0 | 15.3 | 7.6 | 0.000 | 0.000 | 18.5 | 17.2 | 14.6 | 12.9 | 11.5 | 10.9 | 0.000 | 0.000 |
| Intrinsic sugars (%) | 13.0 | 7.4 | 14.9 | 9.9 | 17.7 | 10.8 | 0.000 | 0.000 | 14.0 | 13.6 | 16.3 | 14.8 | 20.7 | 14.0 | 0.000 | 0.000 |
| Starch (%) | 19.4 | 10.8 | 20.4 | 9.8 | 21.6 | 10.1 | 0.175 | 0.208 | 20.5 | 12.4 | 21.7 | 11.6 | 23.2 | 12.1 | 0.000 | 0.000 |
| Fat (%) | 34.6 | 9.8 | 33.4 | 10.8 | 30.6 | 10.3 | 0.004 | 0.001 | 33.3 | 14.6 | 33.3 | 13.0 | 28.0 | 13.6 | 0.000 | 0.000 |
| Saturates (%) | 15.8 | 6.1 | 14.9 | 5.2 | 13.4 | 5.5 | 0.001 | 0.001 | 13.3 | 6.9 | 12.6 | 6.0 | 10.0 | 5.6 | 0.000 | 0.000 |
| Monounsaturates (%) | 10.3 | 4.1 | 10.0 | 3.9 | 9.5 | 4.2 | 0.276 | 0.131 | 11.1 | 6.1 | 11.6 | 6.5 | 10.2 | 6.7 | 0.001 | 0.002 |
| Polyunsaturates (%) | 4.8 | 5.3 | 4.7 | 5.3 | 3.9 | 4.0 | 0.204 | 0.155 | 5.5 | 6.5 | 5.7 | 6.1 | 4.6 | 5.4 | 0.005 | 0.015 |
| Protein (%) | 12.4 | 4.4 | 13.0 | 3.4 | 13.8 | 5.2 | 0.024 | 0.011 | 12.3 | 6.1 | 12.7 | 5.4 | 15.0 | 7.3 | 0.000 | 0.000 |
| Children/Teenagers (9–17 years) | Adults (18–75 years) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (Low) | T2 (Middle) | T3 (High) | p-Value | p-Value Adjusted for Daily Energy | T1 (Low) | T2 (Middle) | T3 (High) | p-Value | p-Value Adjusted for Daily Energy | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||||
| Daily NRF9.3 score | 352.5 | 51.2 | 460.0 | 24.7 | 556.3 | 42.9 | 0.000 | 0.000 | 398.5 | 54.3 | 514.2 | 26.8 | 628.3 | 52.4 | 0.000 | 0.000 |
| Vitamin A (µg) | 43.4 | 21.4 | 53.9 | 26.4 | 56.6 | 25.4 | 0.359 | 0.460 | 32.8 | 28.4 | 41.3 | 29.1 | 27.7 | 29.3 | 0.002 | 0.002 |
| Beta-carotene (µg) | 20.1 | 15.5 | 23.7 | 18.8 | 37.9 | 19.7 | 0.013 | 0.011 | 11.3 | 29.8 | 18.6 | 27.9 | 24.8 | 43.0 | 0.000 | 0.000 |
| Retinol (µg) | 23.9 | 29.4 | 29.8 | 34.1 | 26.0 | 36.4 | 0.740 | 0.946 | 17.2 | 33.1 | 19.4 | 36.8 | 6.5 | 33.6 | 0.000 | 0.000 |
| Thiamine (mg) | 0.15 | 1.39 | 0.20 | 1.40 | 0.25 | 1.49 | 0.000 | 0.000 | 0.13 | 1.54 | 0.16 | 1.49 | 0.21 | 1.58 | 0.000 | 0.000 |
| Riboflavin (mg) | 0.35 | 1.42 | 0.48 | 1.40 | 0.52 | 1.49 | 0.000 | 0.000 | 0.25 | 1.51 | 0.32 | 1.51 | 0.40 | 1.57 | 0.000 | 0.000 |
| Niacin (mg) | 2.9 | 2.0 | 3.6 | 2.0 | 4.1 | 2.2 | 0.000 | 0.000 | 2.6 | 2.4 | 3.0 | 2.3 | 3.7 | 2.5 | 0.000 | 0.000 |
| Vitamin B6 (mg) | 0.14 | 1.51 | 0.20 | 1.58 | 0.26 | 1.73 | 0.000 | 0.000 | 0.09 | 1.84 | 0.14 | 1.76 | 0.21 | 1.95 | 0.000 | 0.000 |
| Vitamin B12 (µg) | 0.47 | 0.09 | 0.67 | 0.08 | 0.74 | 0.08 | 0.000 | 0.000 | 0.35 | 0.10 | 0.45 | 0.12 | 0.51 | 0.10 | 0.000 | 0.000 |
| Vitamin C (mg) | 3.0 | 5.3 | 5.3 | 4.8 | 8.5 | 7.4 | 0.000 | 0.000 | 2.8 | 7.5 | 5.2 | 7.8 | 10.0 | 9.2 | 0.000 | 0.000 |
| Vitamin D (µg) | 0.07 | 3.17 | 0.10 | 3.54 | 0.24 | 3.42 | 0.000 | 0.000 | 0.03 | 3.33 | 0.05 | 3.78 | 0.05 | 4.36 | 0.164 | 0.190 |
| Vitamin E (mg) | 0.40 | 2.86 | 0.34 | 2.69 | 0.38 | 2.46 | 0.642 | 0.307 | 0.26 | 3.28 | 0.35 | 2.97 | 0.30 | 3.06 | 0.022 | 0.029 |
| Folates (µg) | 19.5 | 5.1 | 30.4 | 5.4 | 38.3 | 5.8 | 0.000 | 0.000 | 14.4 | 7.8 | 21.1 | 7.2 | 29.4 | 8.6 | 0.000 | 0.000 |
| Calcium (mg) | 224 | 20 | 294 | 15 | 304 | 19 | 0.000 | 0.000 | 161 | 25 | 187 | 23 | 221 | 19 | 0.000 | 0.000 |
| Iron (mg) | 1.50 | 1.82 | 1.85 | 1.90 | 2.01 | 2.00 | 0.000 | 0.000 | 1.22 | 2.15 | 1.42 | 2.12 | 1.66 | 2.20 | 0.000 | 0.000 |
| Potassium (mg) | 426 | 26 | 516 | 27 | 541 | 29 | 0.000 | 0.000 | 337 | 30 | 404 | 31 | 477 | 33 | 0.000 | 0.000 |
| Magnesium (mg) | 33.7 | 3.4 | 40.5 | 3.6 | 42.3 | 3.4 | 0.000 | 0.000 | 31.2 | 4.7 | 36.8 | 4.6 | 46.6 | 5.0 | 0.000 | 0.000 |
| Zinc (mg) | 0.97 | 0.10 | 1.10 | 0.08 | 1.15 | 0.10 | 0.046 | 0.035 | 0.93 | 0.19 | 1.06 | 0.15 | 1.17 | 0.14 | 0.000 | 0.000 |
| Iodine (µg) | 127 | 85 | 167 | 88 | 169 | 84 | 0.000 | 0.000 | 93 | 77 | 112 | 82 | 128 | 81 | 0.000 | 0.000 |
| Phosphorus (mg) | 261 | 16 | 314 | 18 | 305 | 17 | 0.003 | 0.003 | 185 | 23 | 212 | 21 | 236 | 18 | 0.000 | 0.000 |
| Selenium (µg) | 7.3 | 1.0 | 7.9 | 0.9 | 8.1 | 1.1 | 0.488 | 0.644 | 7.2 | 1.8 | 8.2 | 1.7 | 8.3 | 1.4 | 0.008 | 0.000 |
| Sodium (mg) | 343 | 34 | 372 | 27 | 385 | 32 | 0.227 | 0.254 | 277 | 62 | 293 | 49 | 293 | 36 | 0.414 | 0.139 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz, E.; Ávila, J.M.; Valero, T.; Rodriguez, P.; Varela-Moreiras, G. Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative. Nutrients 2018, 10, 1324. https://doi.org/10.3390/nu10091324
Ruiz E, Ávila JM, Valero T, Rodriguez P, Varela-Moreiras G. Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative. Nutrients. 2018; 10(9):1324. https://doi.org/10.3390/nu10091324
Chicago/Turabian StyleRuiz, Emma, José Manuel Ávila, Teresa Valero, Paula Rodriguez, and Gregorio Varela-Moreiras. 2018. "Breakfast Consumption in Spain: Patterns, Nutrient Intake and Quality. Findings from the ANIBES Study, a Study from the International Breakfast Research Initiative" Nutrients 10, no. 9: 1324. https://doi.org/10.3390/nu10091324