Temporal Trends in Maternal Food Intake Frequencies and Associations with Gestational Diabetes: The Cambridge Baby Growth Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cambridge Baby Growth Study
2.2. Ethics
2.3. Pregnancy (Including Food Frequency) Questionnaire
2.4. Oral Glucose Tests and Gestational Diabetes
2.5. Assays
2.6. Calculations
2.7. Statistical Analysis and Strategy
3. Results
3.1. Characteristics of Study Participants
3.2. Associations with Food Intake Frequencies
3.2.1. Year of OGTT (Temporal Trends)
3.2.2. Gestational Diabetes, Including Attenuation of the Association with Year of OGTT
3.2.3. Indices of Insulin Secretion & Sensitivity, OGTT Glucose Concentrations
3.2.4. Index of Multiple Deprivation
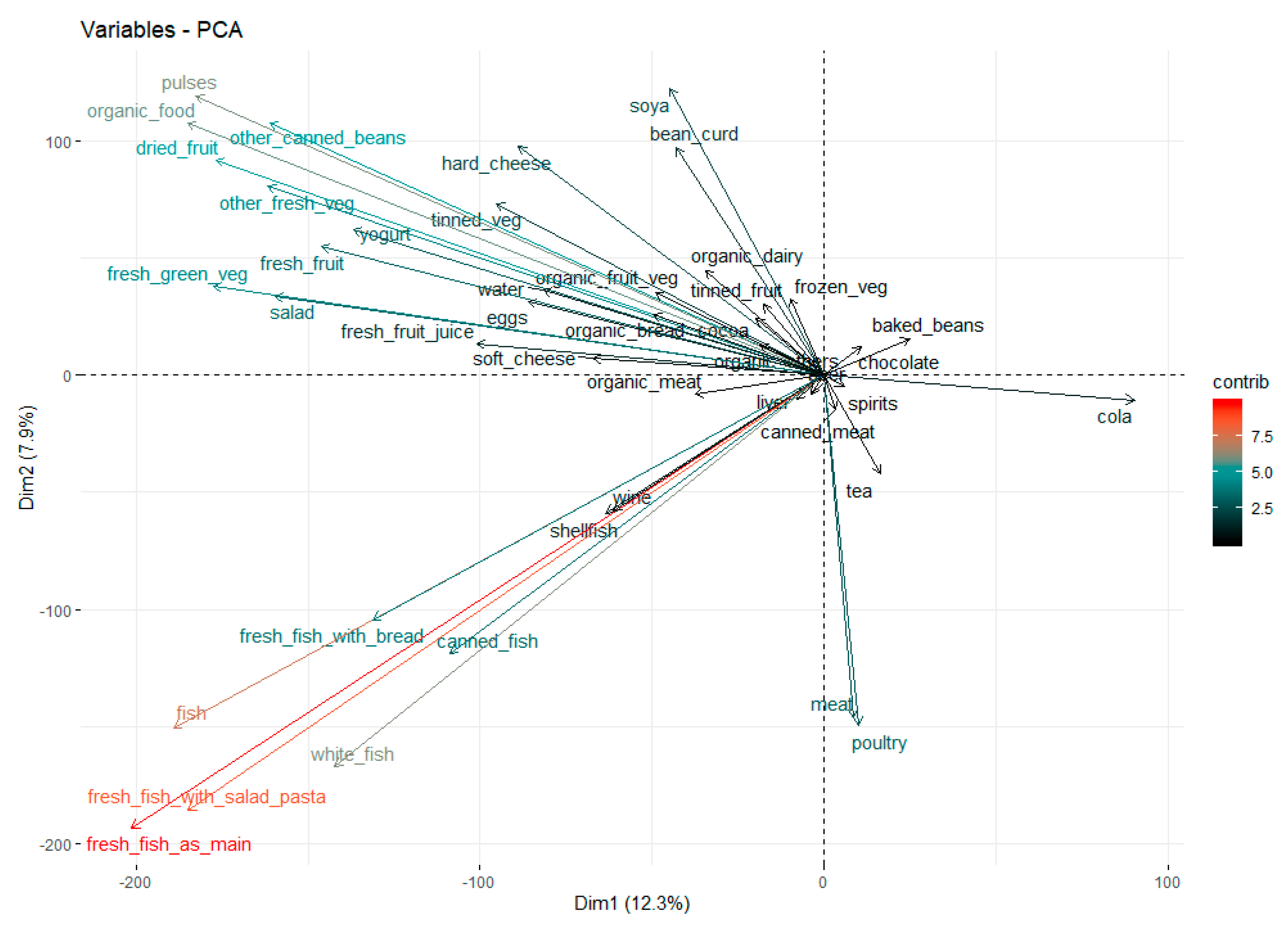
3.3. Principal Component Analysis of Food Intake Frequency Ranks
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- Heianza, Y.; Qi, L. Gene-diet interaction and precision nutrition in obesity. Int. J. Mol. Sci. 2017, 18, 787. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C.; et al. Associations of diet and physical activity with risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 698. [Google Scholar] [CrossRef] [PubMed]
- Radd-Vagenas, S.; Kouris-Blazos, A.; Singh, M.F.; Flood, V.M. Evolution of Mediterranean diets and cuisine: Concepts and definitions. Asia Pac. J. Clin. Nutr. 2017, 26, 749–763. [Google Scholar] [PubMed]
- Assaf-Balut, C.; García de la Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef] [PubMed]
- De la Torre, N.G.; Assaf-Balut, C.; Jiménez Varas, I.; Del Valle, L.; Durán, A.; Fuentes, M.; Del Prado, N.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; et al. Effectiveness of following Mediterranean diet recommendations in the real world in the incidence of Gestational Diabetes Mellitus (GDM) and adverse maternal-foetal outcomes: A prospective, universal, interventional study with a single group. The St Carlos Study. Nutrients 2019, 11, 1210. [Google Scholar]
- Assaf-Balut, C.; García de la Torre, N.; Duran, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Valerio, J.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with an enhanced consumption of extra virgin olive oil and pistachios improves pregnancy outcomes in women without Gestational Diabetes Mellitus: A Sub-analysis of the St. Carlos Gestational Diabetes Mellitus Prevention Study. Ann. Nutr. Metab. 2019, 74, 69–79. [Google Scholar] [CrossRef]
- McCullough, M.L.; Feskanich, D.; Stampfer, M.J.; Giovannucci, E.L.; Rimm, E.B.; Hu, F.B.; Spiegelman, D.; Hunter, D.J.; Colditz, G.A.; Willett, W.C. Diet quality and major chronic disease risk in men and women: Moving toward improved dietary guidance. Am. J. Clin. Nutr. 2002, 76, 1261–1271. [Google Scholar] [CrossRef]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Donazar-Ezcurra, M.; López-Del Burgo, C.; Bes-Rastrollo, M. Primary prevention of gestational diabetes mellitus through nutritional factors: A systematic review. BMC Pregnancy Childbirth 2017, 17, 30. [Google Scholar] [CrossRef]
- Koivusalo, S.B.; Rönö, K.; Klemetti, M.M.; Roine, R.P.; Lindström, J.; Erkkola, M.; Kaaja, R.J.; Pöyhönen-Alho, M.; Tiitinen, A.; Huvinen, E.; et al. Gestational Diabetes Mellitus can be prevented by lifestyle intervention: The Finnish Gestational Diabetes Prevention Study (RADIEL): A randomized controlled trial. Diabetes Care 2016, 39, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Popkin, B.M. The nutrition transition: New trends in the global diet. Nutr. Rev. 1997, 55, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Foster, R.; Lunn, J. 40th Anniversary Briefing Paper: Food availability and our changing diet. Nutr. Bull. 2007, 32, 187–249. [Google Scholar] [CrossRef]
- Ferro-Luzzi, A.; Martino, L. Obesity and physical activity. Ciba Found. Symp. 1996, 201, 207–221. [Google Scholar]
- Crozier, S.R.; Robinson, S.M.; Godfrey, K.M.; Cooper, C.; Inskip, H.M. Women’s dietary patterns change little from before to during pregnancy. J. Nutr. 2009, 139, 1956–1963. [Google Scholar] [CrossRef]
- Feig, D.S.; Hwee, J.; Shah, B.R.; Booth, G.L.; Bierman, A.S.; Lipscombe, L.L. Trends in incidence of diabetes in pregnancy and serious perinatal outcomes: A large, population-based study in Ontario, Canada, 1996–2010. Diabetes Care 2014, 37, 1590–1596. [Google Scholar] [CrossRef]
- Khalifeh, A.; Breathnach, F.; Coulter-Smith, S.; Robson, M.; Fitzpatrick, C.; Malone, F. Changing trends in diabetes mellitus in pregnancy. J. Obstet. Gynaecol. 2014, 34, 135–137. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, L.; Xiao, K.; Horswell, R.; Besse, J.; Johnson, J.; Ryan, D.H.; Hu, G. Increasing incidence of gestational diabetes mellitus in Louisiana, 1997–2009. J. Women’s Health 2012, 21, 319–325. [Google Scholar] [CrossRef]
- Sella, T.; Shalev, V.; Elchalal, U.; Chovel-Sella, A.; Chodick, G. Screening for gestational diabetes in the 21st century: A population-based cohort study in Israel. J. Matern. Fetal Neonatal Med. 2013, 26, 412–416. [Google Scholar] [CrossRef]
- Huy, C.; Loerbroks, A.; Hornemann, A.; Röhrig, S.; Schneider, S. Prevalence, Trend and determining factors of Gestational Diabetes in Germany. Geburtshilfe Frauenheilkd 2012, 72, 311–315. [Google Scholar] [CrossRef]
- Petry, C.J.; Fisher, B.G.; Ong, K.K.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Temporal trends without seasonal effects on gestational diabetes incidence relate to reductions in indices of insulin secretion: The Cambridge Baby Growth Study. Acta Diabetol. 2019, 56, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Haggarty, P.; Campbell, D.M.; Duthie, S.; Andrews, K.; Hoad, G.; Piyathilake, C.; McNeill, G. Diet and deprivation in pregnancy. Br. J. Nutr. 2009, 102, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.; Messer, L.; Evenson, K.; Kaufman, J.S. Neighborhood factors associated with physical activity and adequacy of weight gain during pregnancy. J. Urban Health 2007, 84, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Prentice, P.; Acerini, C.L.; Eleftheriou, A.; Hughes, I.A.; Ong, K.K.; Dunger, D.B. Cohort Profile: The Cambridge Baby Growth Study (CBGS). Int. J. Epidemiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Damgaard, I.N.; Jensen, T.K.; Petersen, J.H.; Skakkebaek, N.E.; Toppari, J.; Main, K.M. Cryptorchidism and maternal alcohol consumption during pregnancy. Environ. Health Perspect. 2007, 115, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Petry, C.J.; Seear, R.V.; Wingate, D.L.; Manico, L.; Acerini, C.L.; Ong, K.K.; Hughes, I.A.; Dunger, D.B. Associations between paternally transmitted fetal IGF2 variants and maternal circulating glucose concentrations in pregnancy. Diabetes 2011, 60, 3090–3096. [Google Scholar] [CrossRef]
- National Collaborating Centre for Women’s and Children’s Health. Diabetes in Pregnancy: Management of Diabetes and Its Complications from Preconception to the Postnatal Period; RCOG Press: London, UK, 2015. [Google Scholar]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; Leiva, A.D.; Hod, M.; International Association of Diabetes and Pregnancy Study Groups Consensus Panel; et al. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef]
- World Health Organization. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy: A World Health Organization Guideline. 2013. Available online: http://apps.who.int/iris/bitstream/10665/85975/1/WHO_NMH_MND_13.2_eng.pdf (accessed on 3 June 2019).
- World Health Organization Department of Noncommunicable Disease Surveillance Geneva. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications; WHO: Geneva, Switzerland, 1999. [Google Scholar]
- Prentice, P.M.; Olga, L.; Petry, C.J.; Simmons, D.; Murphy, H.; Hughes, I.A.; Acerini, C.L.; Ong, K.K.; Dunger, D.B. Reduced size at birth and persisting reductions in adiposity in recent compared with earlier cohorts of infants born to mothers with gestational diabetes mellitus. Diabetologia 2019, 62, 1977–1987. [Google Scholar] [CrossRef]
- Levy, J.C.; Matthews, D.R.; Hermans, M.P. Correct homeostasis model assessment (HOMA) evaluation uses the computer program. Diabetes Care 1998, 21, 2191–2192. [Google Scholar] [CrossRef]
- De Lauzon-Guillain, B.; Wijndaele, K.; Clark, M.; Acerini, C.L.; Hughes, I.A.; Dunger, D.B.; Wells, J.C.; Ong, K.K. Breastfeeding and infant temperament at age three months. PLoS ONE 2012, 7, e29326. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Tieu, J.; Crowther, C.A.; Middleton, P. Dietary advice in pregnancy for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary patterns during pregnancy are associated with risk of gestational diabetes mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, T.; Dibb, S.; Reddy, S. Looking Back, Looking forward: Sustainability and UK Food Policy 2000–2011; Sustainable Development Commission: London, UK, 2011; pp. 1–54. Available online: http://www.sd-commission.org.uk/data/files/publications/FoodPolicy10_Report_final_w.pdf (accessed on 3 June 2019).
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Pot, G.K.; Prynne, C.J.; Almoosawi, S.; Kuh, D.; Stephen, A.M.; NSHD Scientific and Data Collection Teams. Trends in food consumption over 30 years: Evidence from a British birth cohort. Eur. J. Clin. Nutr. 2015, 69, 817–823. [Google Scholar] [CrossRef] [Green Version]
- Whitton, C.; Nicholson, S.K.; Roberts, C.; Prynne, C.J.; Pot, G.K.; Olson, A.; Fitt, E.; Cole, D.; Teucher, B.; Bates, B.; et al. National Diet and Nutrition Survey: UK food consumption and nutrient intakes from the first year of the rolling programme and comparisons with previous surveys. Br. J. Nutr. 2011, 106, 1899–1914. [Google Scholar] [CrossRef]
- Qiu, C.; Frederick, I.O.; Zhang, C.; Sorensen, T.K.; Enquobahrie, D.A.; Williams, M.A. Risk of gestational diabetes mellitus in relation to maternal egg and cholesterol intake. Am. J. Epidemiol. 2011, 173, 649–658. [Google Scholar] [CrossRef] [Green Version]
- Schoenaker, D.A.; Mishra, G.D.; Callaway, L.K.; Soedamah-Muthu, S.S. The role of energy, nutrients, foods, and dietary patterns in the development of gestational diabetes mellitus: A systematic review of observational studies. Diabetes Care 2016, 39, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Milajerdi, A.; Tehrani, H.; Haghighatdoost, F.; Larijani, B.; Surkan, P.J.; Azadbakht, L. Associations between higher egg consumption during pregnancy with lowered risks of high blood pressure and gestational diabetes mellitus. Int. J. Vitam. Nutr. Res. 2018, 88, 166–175. [Google Scholar] [CrossRef]
- Stråvik, M.; Jonsson, K.; Hartvigsson, O.; Sandin, A.; Wold, A.E.; Sandberg, A.S.; Barman, M. Food and nutrient intake during pregnancy in relation to maternal characteristics: Results from the NICE Birth Cohort in Northern Sweden. Nutrients 2019, 11, 1680. [Google Scholar] [CrossRef] [Green Version]
- Blumfield, M.L.; Hure, A.J.; Macdonald-Wicks, L.; Smith, R.; Collins, C.E. Systematic review and meta-analysis of energy and macronutrient intakes during pregnancy in developed countries. Nutr. Rev. 2012, 70, 322–336. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Included | Not-Included | p-Value |
|---|---|---|---|
| Mother’s age at the birth of her baby (years) | 33.4 | 33.7 | 0.3 |
| (33.1, 33.7) | (33.3, 34.0) | ||
| (n = 787) | (n = 548) | ||
| Parity (n, of increasing parity and starting with 0) | 415/310/103/24/4/2 | 302/330/112/37/4/4 | 2.0 × 10−3 |
| GDM (n yes/no) | 85 yes, 780 no | 26 yes, 193 no | 0.4 |
| OGTT fasting glucose concentration (mmol/L) | 4.3 | 4.4 | 0.1 |
| (4.3, 4.4) | (4.3, 4.5) | ||
| (n = 865) | (n = 218) | ||
| OGTT fasting insulin concentration (pmol/L) | 45 | 46 | 0.8 |
| (44, 47) | (44, 49) | ||
| (n = 846) | (n = 290) | ||
| Pre-pregnancy BMI (kg/m2) | 23.5 | 23.3 | 0.4 |
| (23.2, 23.7) | (22.9, 23.6) | ||
| (n = 776) | (n = 411) | ||
| Index of multiple deprivation | 8.0 | 8.1 | 0.6 |
| (7.7, 8.3) | (7.8, 8.5) | ||
| (n = 597) | (n = 401) | ||
| Maternal highest qualification (category GCSE/A levels/degree) (n) | 75/123/337 | 38/62/155 | 0.8 |
| Sex of baby (n males/females) | 443/413 | 412/386 | 1.0 |
| Baby’s birth weight (kg) * | 3.490 | 3.449 | 0.1 |
| (3.459, 3.552) | (3.406, 3.492) | ||
| (n = 774) | (n = 408) | ||
| Gestational age at birth of baby (weeks) | 39.9 | 39.6 | 5.1 × 10−4 |
| (39.8, 40.0) | (39.5, 39.7) | ||
| (n = 857) | (n = 800) | ||
| Reported smoking during pregnancy (n yes/no) | 31/825 | 55/744 | 3.0 × 10−3 |
| Food/Drink Type | Slope (Ranks/Year) | p-Value |
|---|---|---|
| Spirits | −155.06 | 2.12 × 10−2 |
| Pulses | 95.90 | 1.37 × 10−24 |
| Tinned fruit | 69.81 | 2.33 × 10−5 |
| Other canned beans/pulses | 34.29 | 3.27 × 10−11 |
| Organic food | 33.40 | 2.51 × 10−12 |
| Beer | −32.33 | 2.75 × 10−3 |
| Soft cheese | 29.99 | 3.00 × 10−11 |
| Tinned vegetables | 29.92 | 1.07 × 10−2 |
| Wine | −26.63 | 1.40 × 10−6 |
| Tap water | 25.25 | 2.63 × 10−4 |
| Dried fruit | 23.00 | 1.36 × 10−8 |
| Organic fruit and vegetables | 22.75 | 2.19 × 10−13 |
| Organic dairy | 19.67 | 2.88 × 10−9 |
| Organic meat | 17.98 | 1.07 × 10−8 |
| Yogurt | 17.04 | 5.69 × 10−8 |
| Cola | −15.17 | 5.75 × 10−3 |
| Salad | 15.00 | 2.22 × 10−5 |
| Other fresh vegetables | 13.33 | 1.38 × 10−3 |
| Bean curd | 10.13 | 2.42 × 10−3 |
| Fresh fruit | 8.98 | 1.20 × 10−3 |
| Fresh fish with bread | 8.88 | 1.92 × 10−3 |
| Hard cheese | 8.41 | 5.54 × 10−3 |
| Soya | 7.05 | 1.68 × 10−2 |
| Fresh fish with salad pasta | 6.44 | 9.48 × 10−3 |
| Eggs | −6.19 | 3.03 × 10−2 |
| Organic others | 6.13 | 7.16 × 10−3 |
| Chocolate | 5.25 | 2.54 × 10−3 |
| Fresh fruit juice | −3.37 | 7.46 × 10−3 |
| Canned fish | −3.28 | 1.64 × 10−2 |
| Baked beans | −1.36 | 1.21 × 10−4 |
| Shellfish | −1.28 × 10−5 | 2.44 × 10−2 |
| Food/Drink Type | Slope (Ranks/Diagnosis of GDM) | p-Value | Association between Year of OGTT Testing and GDM in These Women | Association between Year of OGTT Testing and GDM in These Women (Adjusted for Food/Drink Type) | ||
|---|---|---|---|---|---|---|
| OR | p-Value | OR | p-Value | |||
| Bean curd | −2.00 × 10−3 | 6.42 × 10−13 | 1.2 | 1.3 × 10−3 | 1.2 | 1.3 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 890) | (n = 890) | |||||
| Eggs | −1.86 × 10−3 | 3.03 × 10−8 | 1.2 | 1.7 × 10−3 | 1.2 | 1.6 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 893) | (n = 893) | |||||
| White fish | −1.83 × 10−3 | 3.88 × 10−6 | 1.2 | 1.5 × 10−3 | 1.2 | 1.6 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 888) | (n = 888) | |||||
| Soya | −1.66 × 10−3 | 9.02 × 10−9 | 1.2 | 1.9 × 10-3 | 1.2 | 2.1 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 890) | (n = 888) | |||||
| Meat | 1.63 × 10−3 | 4.86 × 10−8 | 1.2 | 1.5 × 10−3 | 1.2 | 1.6 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 893) | (n = 893) | |||||
| Spirits | −1.63 × 10−3 | 1.20 × 10−17 | 1.2 | 3.1 × 10−3 | 1.2 | 3.0 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 857) | (n = 857) | |||||
| Beer | −1.62 × 10−3 | 1.97 × 10−12 | 1.2 | 3.3 × 10−3 | 1.2 | 4.5 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 856) | (n = 856) | |||||
| Liver | −1.57 × 10−3 | 1.50 × 10−15 | 1.2 | 1.3 × 10−3 | 1.2 | 1.2 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 889) | (n = 889) | |||||
| Canned meat | −1.57 × 10−3 | 4.49 × 10−14 | 1.2 | 1.5 × 10−3 | 1.2 (1.1, 1.3) (n = 892) | 1.1 × 10−3 |
| (1.1, 1.3) | ||||||
| (n = 892) | ||||||
| Poultry | 1.56 × 10−3 | 7.14 × 10−5 | 1.2 | 1.5 × 10−3 | 1.3 | 1.1 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 892) | (n = 892) | |||||
| Cocoa | −1.50 × 10−3 | 1.46 × 10−6 | 1.2 | 2.7 × 10−3 | 1.2 | 2.8 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 856) | (n = 856) | |||||
| Fresh fish with salad pasta | −5.22 × 10−4 | 4.43 × 10−6 | 1.2 | 1.5 × 10−3 | 1.2 | 1.3 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 877) | (n = 877) | |||||
| Salad | 3.54 × 10−4 | 2.57 × 10−2 | 1.2 | 1.1 × 10−3 | 1.2 | 1.2 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 881) | (n = 881) | |||||
| Fresh fruit | 3.01 × 10−4 | 8.53 × 10−6 | 1.2 | 1.5 × 10−3 | 1.2 | 1.7 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 895) | (n = 895) | |||||
| Wine | −2.99 × 10−4 | 1.74 × 10−4 | 1.2 | 2.0 × 10−3 | 1.2 | 3.9 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 867) | (n = 867) | |||||
| Organic bread | −2.83 × 10−4 | 7.89 × 10−3 | 1.2 | 4.4 × 10−3 | 1.2 | 4.9 × 10−3 |
| (1.1, 1.4) | (1.1, 1.4) | |||||
| (n = 603) | (n = 603) | |||||
| Fresh fish with bread | −2.53 × 10−4 | 2.00 × 10−3 | 1.2 | 1.2 × 10−3 | 1.2 | 1.2 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 864) | (n = 864) | |||||
| Hard cheese | −2.31 × 10−4 | 1.49 × 10−3 | 1.2 | 1.5 × 10−3 | 1.2 | 1.5 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 894) | (n = 894) | |||||
| Soft cheese | −2.15 × 10−4 | 5.32 × 10−4 | 1.2 | 3.2 × 10−3 | 1.2 | 3.2 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 877) | (n = 877) | |||||
| Canned fish | 2.13 × 10−4 | 8.82 × 10−5 | 1.2 | 1.5 × 10−3 | 1.2 | 1.6 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 893) | (n = 893) | |||||
| Fresh fruit juice | 1.66 × 10−4 | 2.17 × 10−3 | 1.2 | 1.5 × 10−3 | 1.2 | 1.5 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 888) | (n = 888) | |||||
| Dried fruit | −1.34 × 10−4 | 5.76 × 10−4 | 1.2 | 1.4 × 10−3 | 1.2 | 7.9 × 10−4 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 892) | (n = 892) | |||||
| Shellfish | −5.92 × 10−5 | 8.47 × 10−3 | 1.2 | 1.9 × 10−3 | 1.2 | 1.8 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 886) | (n = 886) | |||||
| Tea | −5.10 × 10−5 | 1.16 × 10−3 | 1.2 | 2.2 × 10−3 | 1.2 | 2.6 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 876) | (n = 876) | |||||
| Fresh fish as main course | −3.19 × 10−5 | 3.92 × 10−4 | 1.2 | 1.4 × 10−3 | 1.2 | 9.5 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 888) | (n = 888) | |||||
| Baked beans | −1.55 × 10−5 | 6.05 × 10−3 | 1.2 | 1.5 × 10−3 | 1.2 | 1.1 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 894) | (n = 894) | |||||
| Tap water | 1.43 × 10−5 | 2.06 × 10−3 | 1.2 | 1.5 × 10−3 | 1.2 | 1.9 × 10−3 |
| (1.1, 1.3) | (1.1, 1.3) | |||||
| (n = 894) | (n = 894) | |||||
| Food/Drink Type | Slope (Ranks/Index of Multiple Deprivation Units) | p-Value |
|---|---|---|
| Bean curd | 38.24 | 9.82 × 10−4 |
| Soya | 20.07 | 1.29 × 10−2 |
| Other canned beans/pulses | 18.41 | 4.21 × 10−3 |
| Pulses | 17.83 | 5.39 × 10−5 |
| Organic food | 16.36 | 1.20 × 10−4 |
| Salad | 11.58 | 7.05 × 10−3 |
| Dried fruit | 10.82 | 1.07 × 10−2 |
| Organic dairy | 10.23 | 2.46 × 10−4 |
| Baked beans | −9.81 | 1.67 × 10−3 |
| Tea | −9.77 | 1.04 × 10−3 |
| Organic bread | 9.47 | 9.65 × 10−3 |
| Organic meat | 9.47 | 1.43 × 10−2 |
| Organic others | 8.97 | 1.42 × 10−4 |
| Hard cheese | −8.24 | 4.94 × 10−3 |
| Fish | 7.89 | 2.48 × 10−3 |
| Eggs | 6.70 | 1.56 × 10−3 |
| White fish | −6.58 | 1.49 × 10−2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petry, C.J.; Ong, K.K.; Hughes, I.A.; Acerini, C.L.; Dunger, D.B. Temporal Trends in Maternal Food Intake Frequencies and Associations with Gestational Diabetes: The Cambridge Baby Growth Study. Nutrients 2019, 11, 2822. https://doi.org/10.3390/nu11112822
Petry CJ, Ong KK, Hughes IA, Acerini CL, Dunger DB. Temporal Trends in Maternal Food Intake Frequencies and Associations with Gestational Diabetes: The Cambridge Baby Growth Study. Nutrients. 2019; 11(11):2822. https://doi.org/10.3390/nu11112822
Chicago/Turabian StylePetry, Clive J., Ken K. Ong, Ieuan A. Hughes, Carlo L. Acerini, and David B. Dunger. 2019. "Temporal Trends in Maternal Food Intake Frequencies and Associations with Gestational Diabetes: The Cambridge Baby Growth Study" Nutrients 11, no. 11: 2822. https://doi.org/10.3390/nu11112822