Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
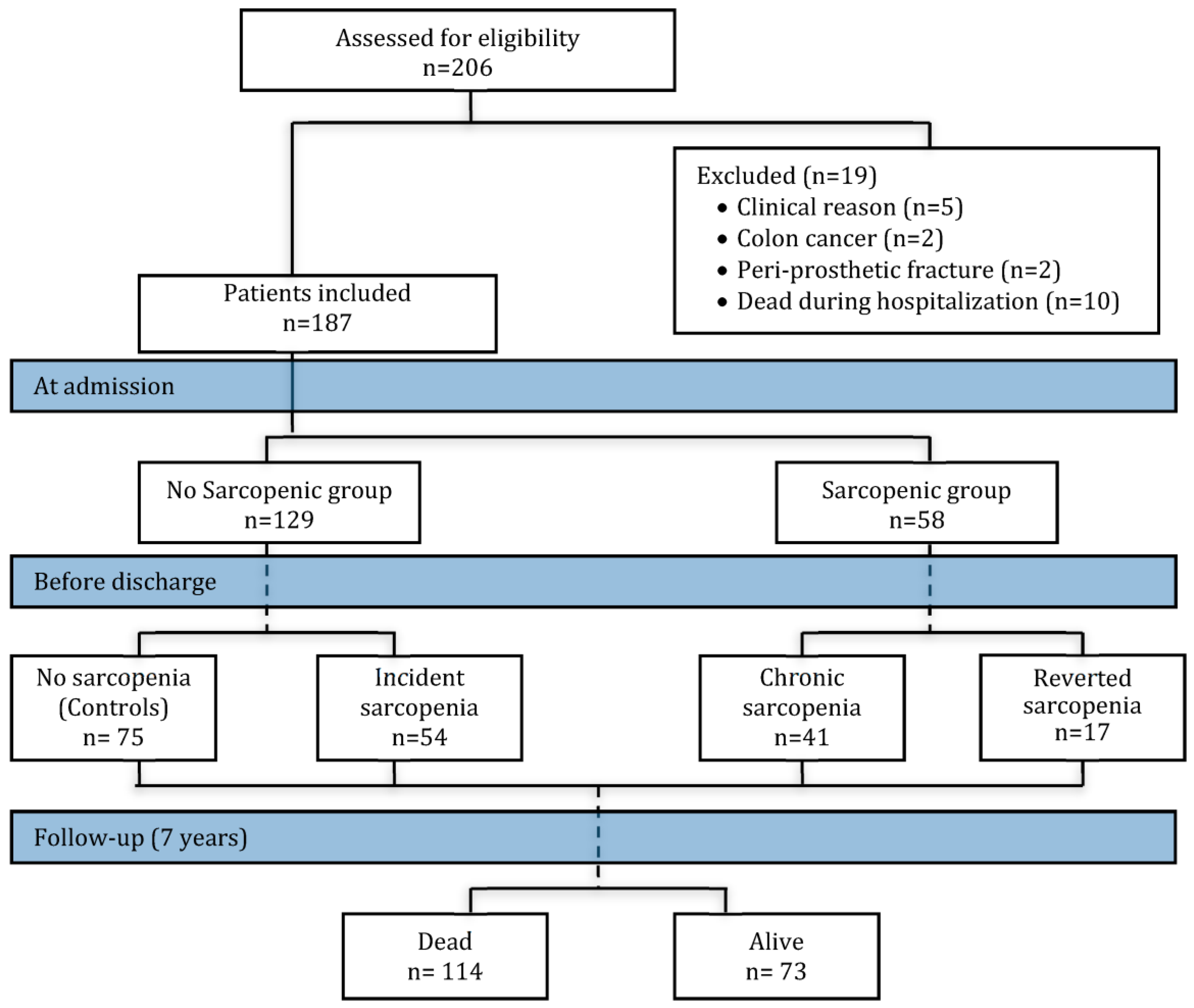
2.1. Study Population
2.2. Sarcopenia Assessment
2.3. Patients Assessment
2.4. Statistical Analysis
3. Results
3.1. Discharge Differences
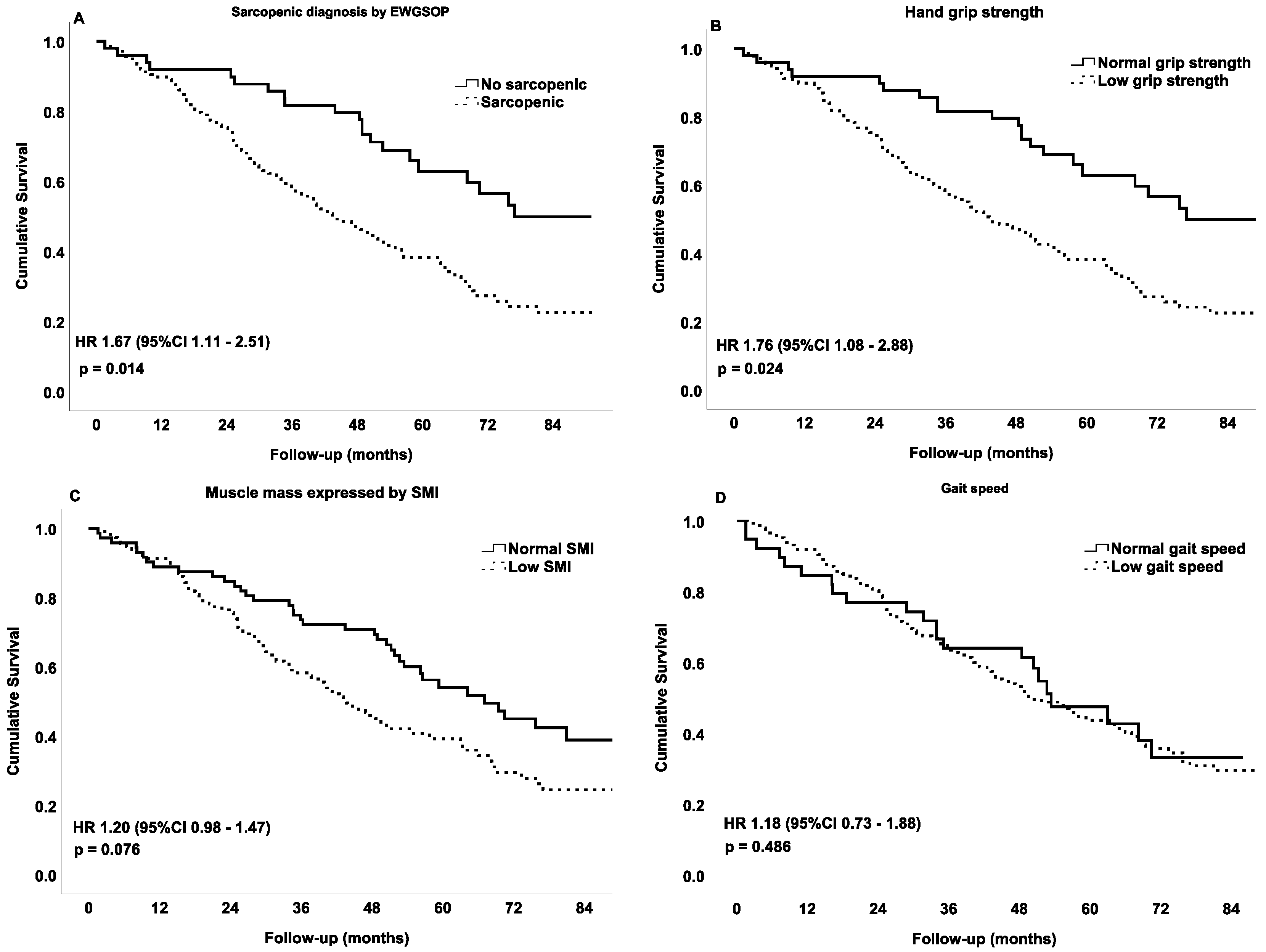
3.2. Mortality
4. Discussion
5. Conclusions and Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sloane, P.D.; Marzetti, E.; Landi, F.; Zimmerman, S. Understanding and Addressing Muscle Strength, Mass, and Function in Older Persons. J. Am. Med. Dir. Assoc. 2019, 20, 4. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Morley, J.E. Sarcopenia Is Recognized as an Independent Condition by an International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) Code. J. Am. Med. Dir. Assoc. 2016, 17, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Morley, J.E.; von Haehling, S. Welcome to the ICD-10 code for sarcopenia. J. Cachexia Sarcopenia Muscle 2016, 7, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, H.P.; Kinsella, R.; Duque, G. Osteosarcopenia: Where bone, muscle, and fat collide. Osteoporos Int. 2017, 28, 2781–2790. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, S.-V.; Fischer, K.; Dawson-Hughes, B.; Freystaetter, G.; Beuschlein, F.; Schietzel, S.; Egli, A.; Bischoff-Ferrari, H. Association between 25-Hydroxyvitamin D Status and Components of Body Composition and Glucose Metabolism in Older Men and Women. Nutrients 2018, 10, 1826. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Vaz, C. The role of sarcopenia in the risk of osteoporotic hip fracture. Clin. Rheumatol. 2015, 34, 1673–1680. [Google Scholar] [CrossRef]
- Pérez-Ros, P.; Martinez-Arnau, F.M.; Malafarina, V.; Tarazona-Santabalbina, F.J. A one-year proprioceptive exercise programme reduces the incidence of falls in community-dwelling elderly people: A before–after non-randomised intervention study. Maturitas 2016, 94, 155–160. [Google Scholar] [CrossRef]
- Uriz-Otano, F.; Uriz-Otano, J.I.; Malafarina, V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence of cognitive impairment. J. Am. Med. Dir. Assoc. 2015, 16, 215–220. [Google Scholar] [CrossRef]
- Steihaug, O.M.; Gjesdal, C.G.; Bogen, B.; Kristoffersen, M.H.; Lien, G.; Hufthammer, K.O.; Ranhoff, A.H. Does sarcopenia predict change in mobility after hip fracture? a multicenter observational study with one-year follow-up. BMC Geriatr. 2018, 18, 10. [Google Scholar] [CrossRef]
- Uriz-Otano, F.; Pla-Vidal, J.; Tiberio-Lopez, G.; Malafarina, V. Factors associated to institutionalization and mortality over three years, in elderly people with a hip fracture-An observational study. Maturitas 2016, 89, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Reginster, J.Y.; Rizzoli, R.; Shaw, S.C.; Kanis, J.A.; Bautmans, I.; Bischoff-Ferrari, H.; Bruyère, O.; Cesari, M.; Dawson-Hughes, B.; et al. Does nutrition play a role in the prevention and management of sarcopenia? Clin. Nutr. 2018, 37, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Argilés, J.M.; Campos, N.; Lopez-pedrosa, J.M.; Rueda, R.; Rodriguez-mañas, L. Skeletal Muscle Regulates Metabolism via Interorgan Crosstalk: Roles in Health and Disease. J. Am. Med. Dir. Assoc. 2016, 17, 789–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, D.; Zeppa, S.D.; Lucertini, F.; Annibalini, G.; Gervasi, M.; Marini, C.F.; Piccoli, G.; Stocchi, V.; Barbieri, E.; Sestili, P. Muscle and Bone Health in Postmenopausal Women: Role of Protein and Vitamin D Supplementation Combined with Exercise Training. Nutrients 2018, 10, 1103. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Malafarina, C.; Martinez, J.A.; Zulet, M.A. Effectiveness of nutritional supplementation on sarcopenia and recovery in hip fracture patients. A multi-centre randomized trial. Maturitas 2017, 101, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Reginster, J.-Y.; Cabrerizo, S.; Bruyère, O.; Kanis, J.A.; Martinez, J.A.; Zulet, M.A. Nutritional Status and Nutritional Treatment Are Related to Outcomes and Mortality in Older Adults with Hip Fracture. Nutrients 2018, 10, 555. [Google Scholar] [CrossRef] [PubMed]
- González-Montalvo, J.I.; Alarcón, T.; Gotor, P.; Queipo, R.; Velasco, R.; Hoyos, R.; Pardo, A.; Otero, A. Prevalence of sarcopenia in acute hip fracture patients and its influence on short-term clinical outcome. Geriatr. Gerontol. Int. 2016, 16, 1021–1027. [Google Scholar] [CrossRef]
- Steihaug, O.M.; Gram Gjesdal, C.; Bogen, B.; Kristoffersen, M.H.; Lien, G.; Ranhoff, A.H. Sarcopenia in patients with hip fracture: A multicenter cross-sectional study. PLoS ONE 2017, 12, e0184780. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Ortolani, E.; Salini, S.; Martone, A.M.; Santoro, L.; Santoliquido, A.; Sisto, A.; Picca, A.; Marzetti, E. The association between sarcopenia and functional outcomes among older patients with hip fracture undergoing in-hospital rehabilitation. Osteoporos Int. 2017, 28, 1569–1576. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Wakabayashi, H.; Bise, T.; Tanoue, M. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients. Clin. Nutr. 2018, 37, 2022–2028. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Landi, F.; Volpato, S.; Corsonello, A.; Meloni, E.; Bernabei, R.; Onder, G. Association of sarcopenia with short- and long-term mortality in older adults admitted to acute care wards: Results from the CRIME study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Cerri, A.P.; Bellelli, G.; Mazzone, A.; Pittella, F.; Landi, F.; Zambon, A.; Annoni, G. Sarcopenia and malnutrition in acutely ill hospitalized elderly: Prevalence and outcomes. Clin. Nutr. 2015, 34, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Alessa, A. Sarcopenia: Prevalence and prognostic significance in hospitalized patients. Clin. Nutr. 2013, 32, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Hu, X.; Wang, H.; Zhang, L.; Hao, Q.; Dong, B. Sarcopenia predicts readmission and mortality in elderly patients in acute care wards: A prospective study. J. Cachexia Sarcopenia Muscle 2017, 8, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Mody, L.; Miller, D.K.; McGloin, J.M.; Freeman, M.; Marcantonio, E.R.; Magaziner, J.; Studenski, S. Recruitment and retention of older adults in aging research. J. Am. Geriatr. Soc. 2008, 56, 2340–2348. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.H.; Hamel, M.B. Pragmatic trials—Guides to better patient care? N. Engl. J. Med. 2011, 364, 1685–1687. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.; Sloane, P.D. Making Pragmatic Trials Pragmatic in Post-acute and Long-term Care Settings. J. Am. Med. Dir. Assoc. 2019, 20, 107–109. [Google Scholar] [CrossRef]
- Thorpe, K.E.; Zwarenstein, M.; Oxman, A.D.; Treweek, S.; Furberg, C.D.; Altman, D.G.; Tunis, S.; Bergel, E.; Harvey, I.; Magid, D.J.; et al. A pragmatic-explanatory continuum indicator summary (PRECIS): A tool to help trial designers. J. Clin. Epidemiol. 2009, 62, 464–475. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Kyle, U.G.; Kondrup, J. Assessment of adult malnutrition and prognosis with bioelectrical impedance analysis: Phase angle and impedance ratio. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 330–339. [Google Scholar] [CrossRef]
- Wirth, R.; Volkert, D.; Rösler, A.; Sieber, C.C.; Bauer, J.M. Bioelectric impedance phase angle is associated with hospital mortality of geriatric patients. Arch. Gerontol. Geriatr. 2010, 51, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Steihaug, O.M.; Gjesdal, C.G.; Bogen, B.; Ranhoff, A.H. Identifying Low Muscle Mass in Patients with Hip Fracture: Validation of Biolectrical Impedance Analysis and Anthropometry Compared to Dual Energy X-ray Absorptiometry. J. Nutr. Health Aging 2016, 20, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Short, K.R.; Bigelow, M.L.; Kahl, J.; Singh, R.; Coenen-Schimke, J.; Raghavakaimal, S.; Nair, K.S. Decline in skeletal muscle mitochondrial function with aging in humans. Proc. Natl. Acad. Sci. USA 2005, 102, 5618–5623. [Google Scholar] [CrossRef] [Green Version]
- Martone, A.M.; Bianchi, L.; Abete, P.; Bellelli, G.; Bo, M.; Cherubini, A.; Corica, F.; Di Bari, M.; Maggio, M.; Manca, G.M.; et al. The incidence of sarcopenia among hospitalized older patients: Results from the Glisten study. J. Cachexia Sarcopenia Muscle 2017, 8, 907–914. [Google Scholar] [CrossRef]
- Masanes, F.; Culla, A.; Navarro-Gonzalez, M.; Navarro-Lopez, M.; Sacanella, E.; Torres, B.; Lopez-Soto, A. Prevalence of sarcopenia in healthy community-dwelling elderly in an urban area of Barcelona (Spain). J. Nutr. Health Aging 2012, 16, 184–187. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Barillaro, C.; Capoluongo, E.; Bernabei, R.; Onder, G. Association of anorexia with sarcopenia in a community-dwelling elderly population: Results from the ilSIRENTE study. Eur. J. Nutr. 2013, 52, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Parr, E.B.; Coffey, V.G.; Hawley, J.A. “Sarcobesity”: A metabolic conundrum. Maturitas 2013, 74, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Cabello, A.; Ara, I.; González-Agüero, A.; Casajús, J.A.; Vicente-Rodríguez, G. Fat mass influence on bone mass is mediated by the independent association between lean mass and bone mass among elderly women: A cross-sectional study. Maturitas 2013, 74, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [PubMed]
- Hita-Contreras, F. Traditional body mass index cut-offs in older people: Time for a rethink with altered fat distribution, sarcopenia and shrinking height. Maturitas 2018, 113, A1–A2. [Google Scholar] [CrossRef] [PubMed]
- Del Mar Bibiloni, M.; Karam, J.; Bouzas, C.; Aparicio-Ugarriza, R.; Pedrero-Chamizo, R.; Sureda, A.; González-Gross, M.; Tur, J. Association between Physical Condition and Body Composition, Nutrient Intake, Sociodemographic Characteristics, and Lifestyle Habits in Older Spanish Adults. Nutrients 2018, 10, 1608. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, D.; Annweiler, C.; Cederholm, T. A translational approach for the clinical application of recently updated definitions of malnutrition (GLIM) and sarcopenia (EWGSOP2). Maturitas 2019, 122, 89–90. [Google Scholar] [CrossRef]
- Landi, F.; Camprubi-Robles, M.; Bear, D.E.; Cederholm, T.; Malafarina, V.; Welch, A.A.; Cruz-Jentoft, A.J. Muscle loss: The new malnutrition challenge in clinical practice. Clin. Nutr. 2018. [Google Scholar] [CrossRef]
- Malafarina, V.; Uriz-Otano, F.; Gil-Guerrero, L.; Iniesta, R. The anorexia of ageing: Physiopathology, prevalence, associated comorbidity and mortality. A systematic review. Maturitas 2013, 74, 293–302. [Google Scholar] [CrossRef]
- Malafarina, V.; Uriz-Otano, F.; Iniesta, R.; Gil-Guerrero, L. Effectiveness of nutritional supplementation on muscle mass in treatment of sarcopenia in old age: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 10–17. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet (Lond. Engl.) 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Lorenzo-López, L.; López-López, R.; Maseda, A.; Buján, A.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Changes in frailty status in a community-dwelling cohort of older adults: The VERISAÚDE study. Maturitas 2019, 119, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Mendonça, N.; Hill, T.; Jagger, C.; Stevenson, E.; Mathers, J.; Sayer, A. Nutrition in the Very Old. Nutrients 2018, 10, 269. [Google Scholar] [CrossRef] [PubMed]
- Clegg, M.E.; Williams, E.A. Optimizing nutrition in older people. Maturitas 2018, 112, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Paris, A.; Camprubi-Robles, M.; Lopez-Pedrosa, J.M.; Pereira, S.L.; Rueda, R.; Ballesteros-Pomar, M.D.; Garcia Almeida, J.M.; Cruz-Jentoft, A.J. Role of Oral Nutritional Supplements Enriched with B-hydroxy-B-Methylbutyrate in Maintaining Muscle Function and Improving Clinical Outcomes in Various Clinical Settings. J. Nutr. Health Aging 2018, 22, 664–675. [Google Scholar] [CrossRef] [Green Version]
- Trouwborst, I.; Verreijen, A.; Memelink, R.; Massanet, P.; Boirie, Y.; Weijs, P.; Tieland, M. Exercise and nutrition strategies to counteract sarcopenic obesity. Nutrients 2018, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Aquilani, R.; Zuccarelli, G.; Condino, A.; Catani, M.; Rutili, C.; Del Vecchio, C.; Pisano, P.; Verri, M.; Iadarola, P.; Viglio, S.; et al. Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures. Nutrients 2017, 9, 637. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Bueno-Notivol, J.; Martínez-Amat, A.; Cruz-Díaz, D.; Hernandez, A.V.; Pérez-López, F.R. Effect of exercise alone or combined with dietary supplements on anthropometric and physical performance measures in community-dwelling elderly people with sarcopenic obesity: A meta-analysis of randomized controlled trials. Maturitas 2018, 116, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Amat, A.; Aibar-Almazán, A.; Fábrega-Cuadros, R.; Cruz-Díaz, D.; Jiménez-García, J.D.; Pérez-López, F.R.; Achalandabaso, A.; Barranco-Zafra, R.; Hita-Contreras, F. Exercise alone or combined with dietary supplements for sarcopenic obesity in community-dwelling older people: A systematic review of randomized controlled trials. Maturitas 2018, 110, 92–103. [Google Scholar] [CrossRef]
- Newman, A.B.; Lee, J.S.; Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Tylavsky, F.A.; Nevitt, M.; Harris, T.B. Weight change and the conservation of lean mass in old age: The Health, Aging and Body Composition Study. Am. J. Clin. Nutr. 2005, 82, 872–878. [Google Scholar] [CrossRef]
- Di Monaco, M.; Castiglioni, C.; Vallero, F.; Di Monaco, R.; Tappero, R. Sarcopenia is more prevalent in men than in women after hip fracture: A cross-sectional study of 591 inpatients. Arch. Gerontol. Geriatr. 2012, 55, e48–e52. [Google Scholar] [CrossRef] [PubMed]
- Tay, L.; Ding, Y.Y.; Leung, B.P.; Ismail, N.H.; Yeo, A.; Yew, S.; Tay, K.S.; Tan, C.H.; Chong, M.S. Sex-specific differences in risk factors for sarcopenia amongst community-dwelling older adults. Age (Omaha) 2015, 37, 12. [Google Scholar] [CrossRef] [PubMed]
- Renoud, A.; Ecochard, R.; Marchand, F.; Chapurlat, R.; Szulc, P. Predictive parameters of accelerated muscle loss in men-MINOS study. Am. J. Med. 2014, 127, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Sipers, W.M.W.H.; de Blois, W.; Schols, J.M.G.A.; van Loon, L.J.C.; Verdijk, L.B. Sarcopenia is Related to Mortality in the Acutely Hospitalized Geriatric Patient. J. Nutr. Health Aging 2019, 23, 128–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granic, A.; Davies, K.; Jagger, C.; Dodds, R.M.; Kirkwood, T.B.L.; Sayer, A.A. Initial level and rate of change in grip strength predict all-cause mortality in very old adults. Age Ageing 2017, 46, 970–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syddall, H.E.; Westbury, L.D.; Dodds, R.; Dennison, E.; Cooper, C.; Sayer, A.A. Mortality in the Hertfordshire Ageing Study: Association with level and loss of hand grip strength in later life. Age Ageing 2017, 46, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Alonso, F.J.; Vidan-Astiz, M.; Alonso-Armesto, M.; Toledano-Iglesias, M.; Alvarez-Nebreda, L.; Branas-Baztan, F.; Serra-Rexach, J.A. The pattern of recovery of ambulation after hip fracture differs with age in elderly patients. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, Å.; Berggren, M.; Gustafson, Y.; Olofsson, B.; Lindelöf, N.; Stenvall, M. Effects of Geriatric Interdisciplinary Home Rehabilitation on Walking Ability and Length of Hospital Stay After Hip Fracture: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2016, 17, 464.e9–464.e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uemura, K.; Makizako, H.; Lee, S.; Doi, T.; Lee, S.; Tsutsumimoto, K.; Shimada, H. The impact of sarcopenia on incident homebound status among community-dwelling older adults: A prospective cohort study. Maturitas 2018, 113, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total n = 187 | |
|---|---|
| Age, years | 85.2 ± 6.3 |
| Sex n (%) | |
| Female | 138 (73.8%) |
| Male | 49 (26.2%) |
| BMI kg/m2 | 25.4 ± 4.6 |
| Fracture type | |
| Intracapsular | 89 (47.6%) |
| Extracapsular | 98 (52.4%) |
| Type of surgery | |
| Replacement | 69 (36.9%) |
| Internal fixation | 118 (63.1%) |
| Time to surgery | 2 (2–4) |
| Non-weight bearing | 29 (15.5%) |
| LoS orthopedics (days) | 10 (8–12) |
| LoS rehabilitation (days) | 41 (29–57) |
| ONS & | 73 (42.6%) |
| Previous Barthel index | 85 (60–100) |
| MMSE | 22 (16–26) |
| MNA-SF ‡ | 10 (8–12) |
| SMI kg/m2 | |
| Female | 13.6 ± 2.3 |
| Male | 17.2 ± 3.4 |
| Grip strength kg | |
| Female | 11.9 ± 5.0 |
| Male | 19.6 ± 9.6 |
| No Sarcopenic (Controls) n = 75 | Incident Sarcopenia n = 54 | Chronic Sarcopenia n = 41 | Reverted Sarcopenia n = 17 | p-Value | |
|---|---|---|---|---|---|
| Age (year) | 83.9 ± 5.6 | 86.1 ± 6.8 | 88.2 ± 4.6 ‡ | 81.1 ± 7.6 | <0.0001 |
| Sex n (M/W) | 9/66 | 35/19 | 0/41 | 5/12 | <0.0001 |
| BMI, Kg/m2 | 28.6 ± 4.7 | 23.9 ± 3.1 ‡ | 22.2 ± 2.8 ‡ | 23.6 ± 3.0 ‡ | <0.0001 |
| Weight, Kg | 70.9 ± 15.0 | 62.1 ± 10.4 ‡ & | 53.3 ± 7.4 ‡ # | 59.0 ± 11.4 ‡ | 0.0001 |
| SMI, Kg/m2 | |||||
| Men | 7.4 ± 0.4 #-$ | 5.9 ± 0.6 | NA * | 6.4 ± 0.3 | <0.0001 |
| Women | 6.1 ± 0.6 &-$ | 5.8 ± 0.7 &-$ | 4.9 ± 0.4 | 5.2 ± 0.3 | <0.0001 |
| Hand grip, kg | |||||
| Men | 28.2 ± 11.3 | 15.6 ± 6.0 ‡ $ | NA * | 33.7 ± 3.3 | <0.0001 |
| Women | 13.5 ± 5.9 & | 12.3 ± 5.0 | 9.4 ± 3.0 | 12.4 ± 2.4 | 0.0008 |
| Low hand-grip n (%) | 42 (56%) | 12 (22.2%) | 41 (100%) | 17 (100%) | <0.0001 |
| Gait speed (m/s) | 0.41 ± 0.22 | 0.36 ± 0.27 | 0.33 ± 0.22 | 0.54 ± 0.26 & | 0.040 |
| Phase Angle | 4.5 ± 1.1 & | 4.3 ± 1.4 | 3.7 ± 0.6 | 4.2 ± 1.1 | 0.010 |
| Previous BI | 85 (69–100) | 85 (55–100) | 80 (60–97) | 100 (85–100) | 0.090 |
| Discharge BI | 60 (30–80) | 50 (30–75) | 55 (25–70) | 75 (70–80) | 0.069 |
| MMSE | 22 (16–27) | 23 (16–27) | 20 (15–25) | 23 (17–26) | 0.507 |
| MNA-SF | 11 (10–13) | 12 (10–13) | 10 (10–11) ‡ | 12 (10–12) & | 0.005 |
| Weight difference ¥, kg | −1.9 ± 3.4 | −2.8 ± 3.4 | −1.5 ± 2.6 | −0.5 ± 3.0 | 0.054 |
| SMI difference ¥, kg/m2 | |||||
| Men | −1.4 ± 2.0 | −0.8 ± 1.7 | NA * | −0.8 ± 1.7 | 0.872 |
| Women | −0.6 ± 1.2 #-$ | −1.8 ± 2.2 &-$ | −0.2 ± 0.7 $ | 0.9 ± 1.2 | <0.0001 |
| Grip strength difference ¥, Kg | |||||
| Men | −1.2 ± 5.0 | 0.4 ± 3.8 | NA * | 0.5 ± 1.0 | 0.782 |
| Women | 0.96 ± 2.9 | −0.33 ± 2.8 $ | 0.12 ± 2.3 $ | 3.5 ± 4.8 | 0.006 |
| Variable | Incident * | p | Chronic ‡ | p Value |
|---|---|---|---|---|
| BMI | 0.73 (0.64–0.84) | <0.0001 | 0.64 (0.53–0.76) | <0.0001 |
| MNA-SF | 0.93 (0.65–1.33) | 0.696 | 0.60 (0.40–0.90) | 0.015 |
| TST $ | 0.94 (0.88–1.01) | 0.113 | 0.91 (0.85–0.98) | 0.022 |
| Hand-grip strength | 0.92 (0.85–0.99) | 0.038 | 0.85 (0.77–0.94) | 0.002 |
| SMI | 0.17 (0.07–0.43) | <0.0001 | 0.002 (0.0002–0.03) | <0.0001 |
| PA | 0.97 (0.65–1.44) | 0.896 | 0.41 (0.21–0.78) | 0.007 |
| Sarcopenia n = 95 | No Sarcopenia n = 92 | p-Value | |
|---|---|---|---|
| Sex n (M/W) | 35/60 | 14/78 | 0.001 |
| Weight, Kg | 56.1 ± 9.4 | 66.4 ± 13.9 | <0.001 |
| BMI, Kg/m2 | 22.3 ± 2.8 | 26.9 ± 4.5 | <0.001 |
| Hb, g/dL | 11.9 ± 1.2 | 11.6 ± 1.0 | 0.046 |
| Total Protein, g/dL | 6.2 ± 0.6 | 6.2 ± 0.5 | 0.616 |
| Albumin, g/dL | 3.5 ± 0.4 | 3.5 ± 0.4 | 0.921 |
| VitD ng/mL | 11 (12.7–24.9) | 16 (12–23.5) | 0.481 |
| IL-6, pg/mL | 6.2 (3.6–9.3) | 6.0 (3.9–8.4) | 0.753 |
| TNF-alpha, pg/mL | 11.3 (8.0–15.8) | 7.5 (5.0–12.4) | 0.022 |
| Barthel index | 50 (30–75) | 65 (35–80) | 0.053 |
| MNA-SF | 11.5 (10–12.7) | 11.5 (10.5–12.5) | 0.880 |
| PA | 3.9 ± 0.7 | 4.4 ± 0.8 | 0.0001 |
| Hand-grip, kg | 12.8 ± 5.4 | 16.7 ± 7.9 | 0.001 |
| Men | 17.2 ± 5.6 | 32.3 ± 4.2 | <0.001 |
| Women | 10.2 ± 3.3 | 14.8 ± 5.8 | <0.001 |
| Low grip strength n (%) | 95 (100%) | 43 (46.7%) | <0.0001 |
| SMI, Kg/m2 | |||
| Men | 5.7 ± 0.6 | 6.9 ± 0.7 | <0.001 |
| Women | 5.0 ± 0.4 | 5.9 ± 0.6 | <0.001 |
| Low SMI n (%) | 95 (100%) | 20 (21.7%) | <0.0001 |
| Gait speed, m/s | 0.3 ± 0.2 | 0.4 ± 0.2 | 0.035 |
| Low gait speed n (%) | 80 (84.2%) | 68 (73.9%) | 0.083 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malafarina, V.; Malafarina, C.; Biain Ugarte, A.; Martinez, J.A.; Abete Goñi, I.; Zulet, M.A. Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study. Nutrients 2019, 11, 2243. https://doi.org/10.3390/nu11092243
Malafarina V, Malafarina C, Biain Ugarte A, Martinez JA, Abete Goñi I, Zulet MA. Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study. Nutrients. 2019; 11(9):2243. https://doi.org/10.3390/nu11092243
Chicago/Turabian StyleMalafarina, Vincenzo, Concetta Malafarina, Arantzazu Biain Ugarte, J. Alfredo Martinez, Itziar Abete Goñi, and M. Angeles Zulet. 2019. "Factors Associated with Sarcopenia and 7-Year Mortality in Very Old Patients with Hip Fracture Admitted to Rehabilitation Units: A Pragmatic Study" Nutrients 11, no. 9: 2243. https://doi.org/10.3390/nu11092243