Exercise and Nutrition Interventions in Patients with Head and Neck Cancer during Curative Treatment: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
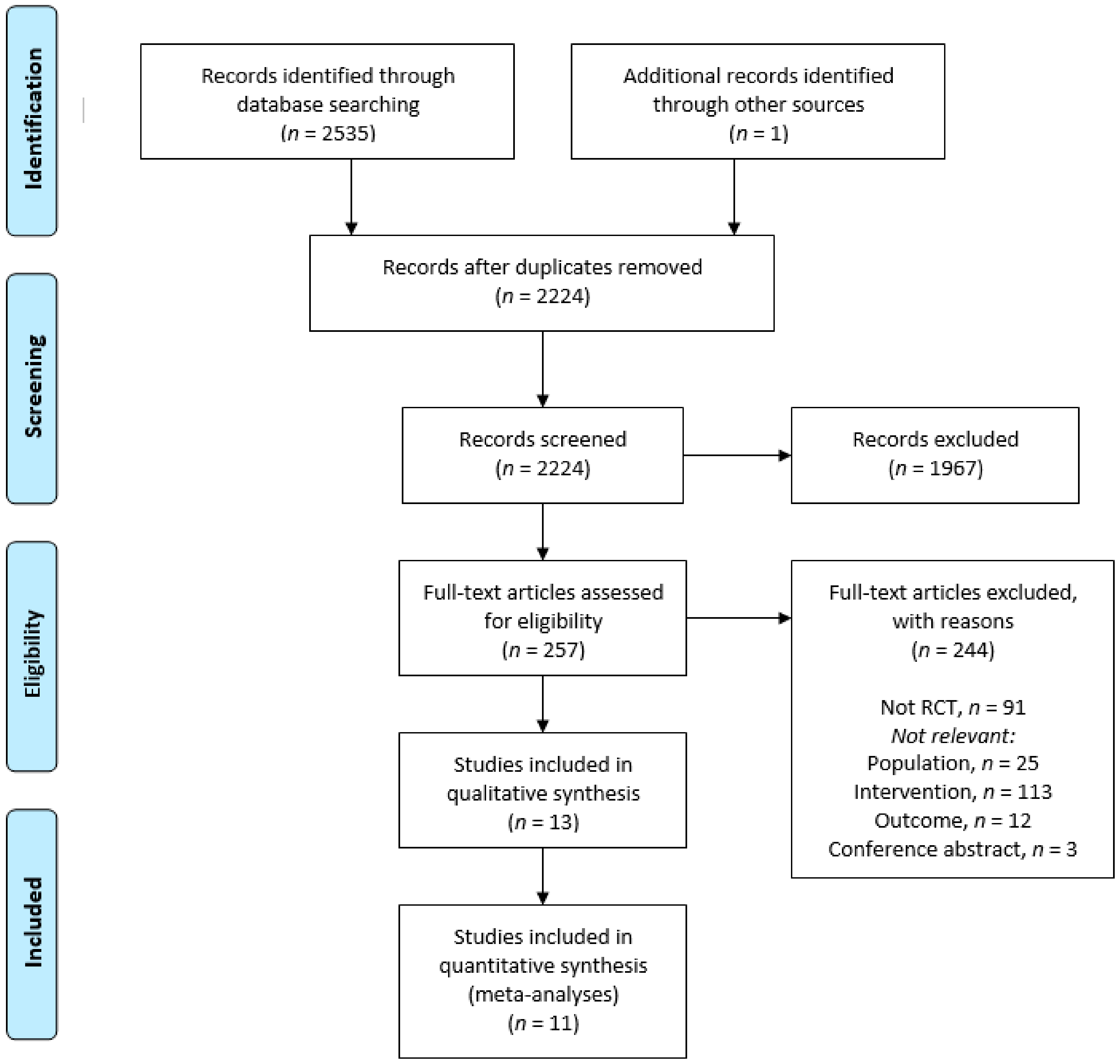
2.1. Data Sources, Search Strategy and Selection Criteria
2.1.1. Data Sources
2.1.2. Search Strategy
2.1.3. Selection Criteria
2.2. Quality Assessment
2.3. Data Extraction and Statistical Analyses
3. Results
3.1. Quality Assessment
3.2. Study Characteristics
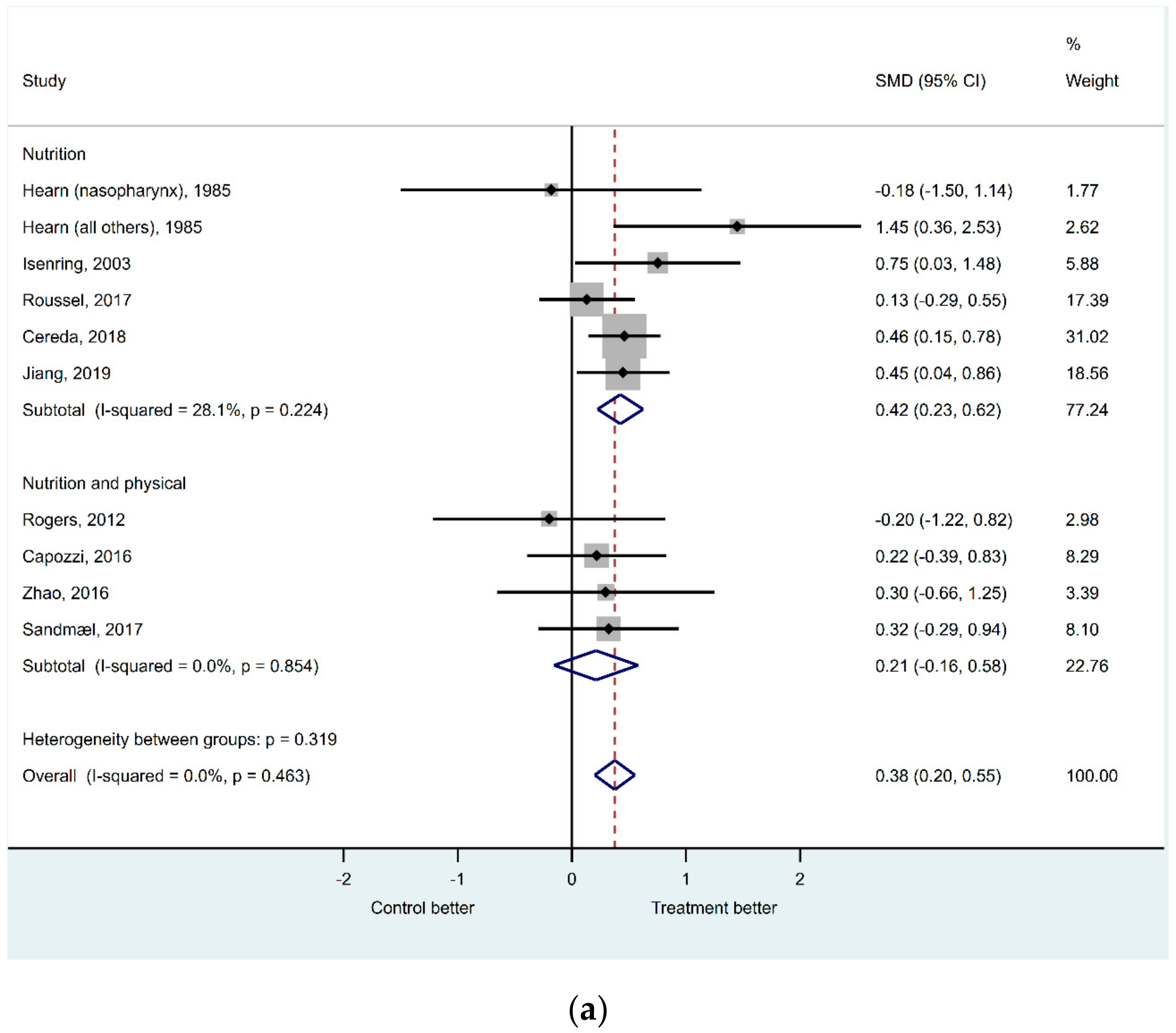
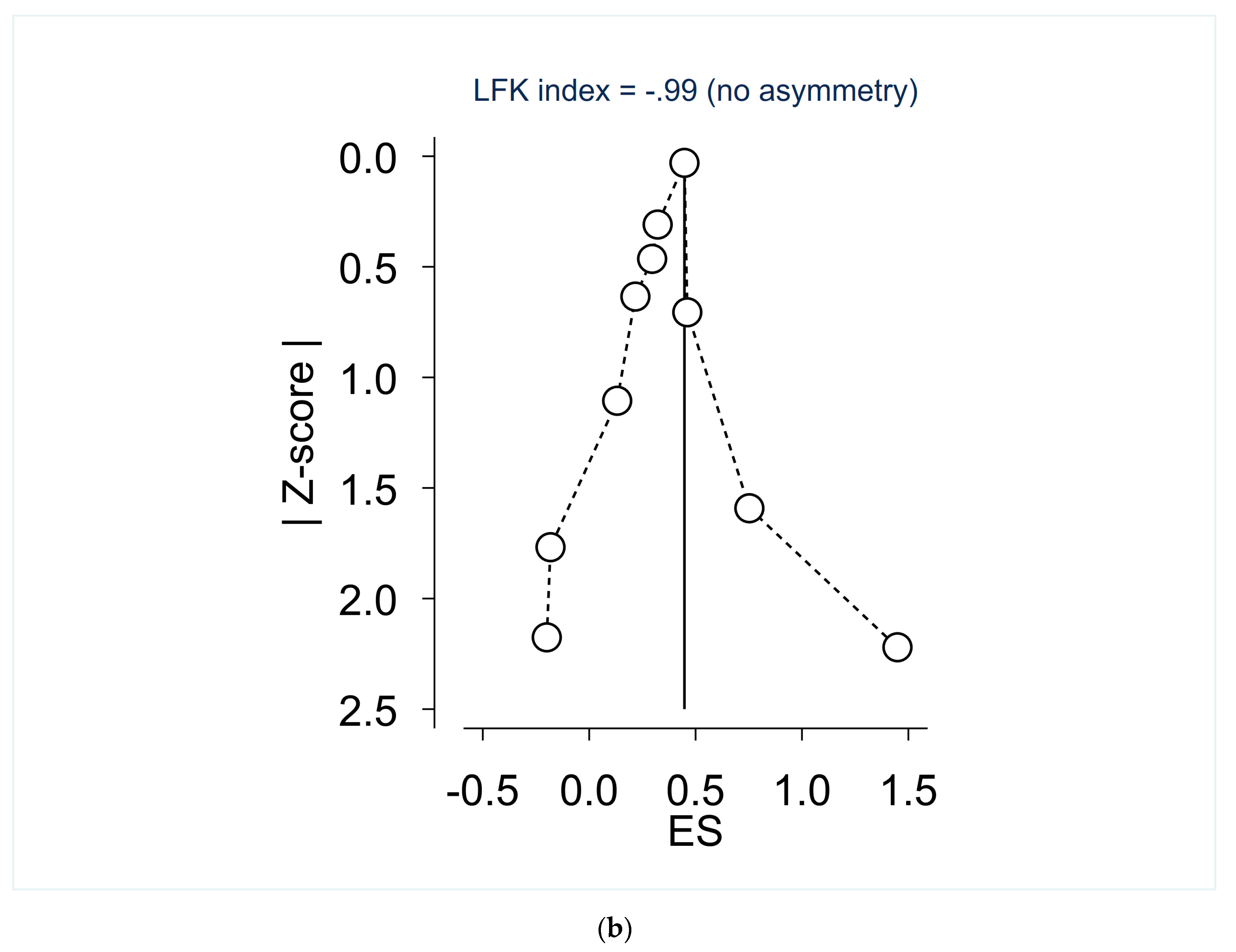
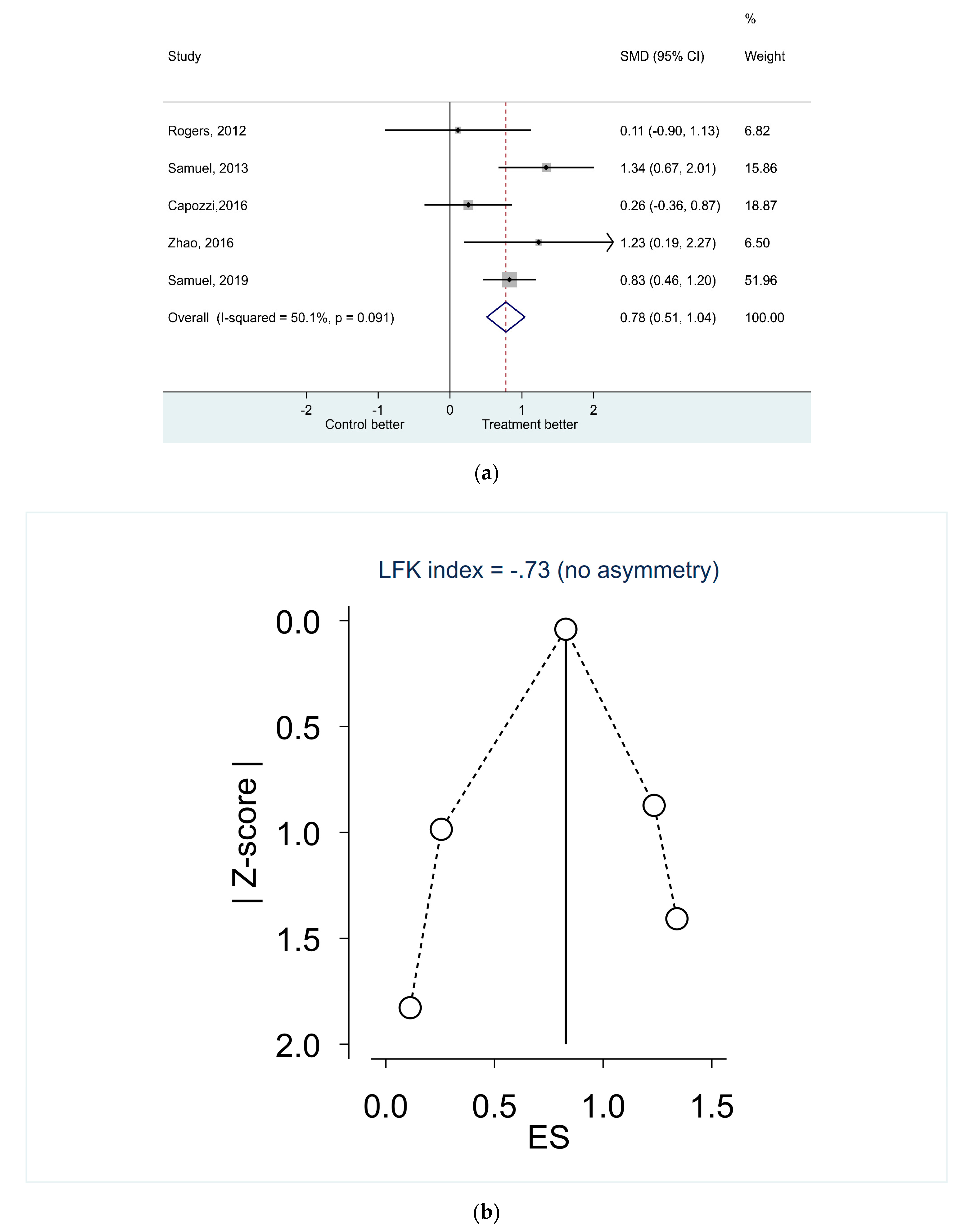
3.3. Effects on Nutritional Status, Body Composition and Physical Function
3.4. The Content of the Interventions
3.4.1. Nutrition
3.4.2. Physical Exercise
3.5. Adherence to the Intervention and Completion Rate
3.5.1. Adherence
3.5.2. Completion Rates
4. Discussion
4.1. Strengths and Limitations
4.2. Nutritional Interventions
4.3. Exercise Interventions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
Appendix A.1. PubMed—3 June 2019
- #1.
- “Head and Neck Neoplasms” [Mesh] AND (“Diet Therapy” [Mesh] OR “diet therapy” [Subheading] OR “Dietary Supplements”[Mesh] OR “Exercise”[Mesh] OR “Exercise Movement Techniques”[Mesh] OR “Exercise Therapy”[Mesh])
- #2.
- ((head[ti] OR neck[ti]) AND (cancer[ti] OR tumor[ti] OR tumour[ti] OR carcinoma*[ti])) AND (exercis*[ti] OR diet[ti] OR diets[ti] OR dietary OR nutrition*[ti] OR training[ti] OR physical activity[ti] OR rehabilitation[ti] OR life style[ti]) NOT medline[sb]
- #3.
- #1 OR #2 > 552 hits > EndNote PubMed in label field
Appendix A.2. Embase—1974 to 3 June 2019
- “head and neck cancer”/dm, rt, rh, si, th [Disease Management, Radiotherapy, Rehabilitation, Side Effect, Therapy]
- (diet therapy/or dietary intake/or exp exercise/or exp kinesiotherapy/or nutritional counseling/or nutritional support/or diet supplementation/or nutrition/)
- 1 and 2 > 350 hits > EndNote Embase in label field
Appendix A.3. Cochrane Library—CDSR issue 6/12, June 2019, DARE issue 2/4, April 2015, CENTRAL issue 5/12, May 2016
- #1.
- (head or neck) and (cancer or carcinom* or tumor* or tumour*): ti,ab,kw
- #2.
- (exercise or training or diet or diets or dietary or nutrition or rehabilitation or “life style” or “physical activity”): ti,ab,kw
- #3.
- #1 and #2 > 379 hits (40 CDSR/7 DARE/343 CENTRAL) > EndNote CDSR/DARE/CENTRAL in label field
Appendix A.4. CINAHL June 2019
- S1 TI ((head OR neck) AND (cancer OR tumor OR tumour OR carcinoma*))
- S2 AB ((head OR neck) AND (cancer OR tumor OR tumour OR carcinoma*))
- S3 TI (exercis* OR diet OR diets OR nutrition* OR training OR rehabilition OR “physical activity” OR lifestyle OR “life style”)
- S4 AB (exercis* OR diet OR diets OR nutrition* OR training OR rehabilition OR “physical activity” OR lifestyle OR “life style”)
- S5 TI (therap* OR treatment* OR intervention* OR management* OR radiotherap* OR chemotherap* OR chemoradiotherap*)
- S6 AB (therap* OR treatment* OR intervention* OR management* OR radiotherap* OR chemotherap* OR chemoradiotherap*)
- S7 (s1 OR s2) AND (s3 OR s4) AND (s5 or s6) > 389 hits > EndNote CINAHL in label field
References
- Forouzanfar, M.H.; Foreman, K.J.; Delossantos, A.M.; Lozano, R.; Lopez, A.D.; Murray, C.J.; Naghavi, M. Breast and cervical cancer in 187 countries between 1980 and 2010: A systematic analysis. Lancet 2011, 378, 1461–1484. [Google Scholar] [CrossRef]
- Ratko, T.A.; Douglas, G.W.; de Souza, J.A.; Belinson, S.E.; Aronson, N. Radiotherapy treatments for head and neck cancer update. In AHRQ Comparative Effectiveness Reviews; Comparative Effectiveness Review No. 144; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2014. [Google Scholar]
- Kubrak, C.; Olson, K.; Jha, N.; Jensen, L.; McCargar, L.; Seikaly, H.; Harris, J.; Scrimger, R.; Parliament, M.; Baracos, V.E. Nutrition impact symptoms: Key determinants of reduced dietary intake, weight loss, and reduced functional capacity of patients with head and neck cancer before treatment. Head Neck 2010, 32, 290–300. [Google Scholar] [CrossRef]
- Kilgour, R.D.; Vigano, A.; Trutschnigg, B.; Hornby, L.; Lucar, E.; Bacon, S.L.; Morais, J.A. Cancer-related fatigue: The impact of skeletal muscle mass and strength in patients with advanced cancer. J. Cachexia Sarcopenia Muscle 2010, 1, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [Green Version]
- Findlay, M.; Bauer, J.; Brown, T.; Davidson, W.; Hill, J.; Isenring, E.; Talwar, B.; Bell, K.; Kiss, N.; Kurmis, R. Evidence based practice guidelines for the nutritional management of patients with head and neck cancer. Clin. Guidel. Netw. 2011. [Google Scholar]
- Langius, J.A.; Zandbergen, M.C.; Eerenstein, S.E.; van Tulder, M.W.; Leemans, C.R.; Kramer, M.H.; Weijs, P.J. Effect of nutritional interventions on nutritional status, quality of life and mortality in patients with head and neck cancer receiving (chemo) radiotherapy: A systematic review. Clin. Nutr. 2013, 32, 671–678. [Google Scholar] [CrossRef]
- Garg, S.; Yoo, J.; Winquist, E. Nutritional support for head and neck cancer patients receiving radiotherapy: A systematic review. Supportive Care Cancer 2010, 18, 667–677. [Google Scholar] [CrossRef]
- Sandmael, J.A.; Bye, A.; Solheim, T.S.; Stene, G.B.; Thorsen, L.; Kaasa, S.; Lund, J.A.; Oldervoll, L.M. Feasibility and preliminary effects of resistance training and nutritional supplements during versus after radiotherapy in patients with head and neck cancer: A pilot randomized trial. Cancer 2017, 123, 4440–4448. [Google Scholar] [CrossRef]
- Capozzi, L.C.; Nishimura, K.C.; McNeely, M.L.; Lau, H.; Culos-Reed, S.N. The impact of physical activity on health-related fitness and quality of life for patients with head and neck cancer: A systematic review. Br. J. Sports Med. 2016, 50, 325–338. [Google Scholar] [CrossRef]
- Bossola, M. Nutritional Interventions in Head and Neck Cancer Patients Undergoing Chemoradiotherapy: A Narrative Review. Nutrients 2015, 7, 266–277. [Google Scholar] [CrossRef]
- Sammut, L.; Ward, M.; Patel, N. Physical activity and quality of life in head and neck cancer survivors: A literature review. Int. J. Sports Med. 2014, 35, 794–799. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macedo, L.G.; Elkins, M.R.; Maher, C.G.; Moseley, A.M.; Herbert, R.D.; Sherrington, C. There was evidence of convergent and construct validity of physiotherapy evidence database quality scale for physiotherapy trials. J. Clin. Epidemiol. 2010, 63, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Yamato, T.P.; Maher, C.; Koes, B.; Moseley, A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J. Clin. Epidemiol. 2017, 86, 176–181. [Google Scholar] [CrossRef]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef]
- Harris, R.; Bradburn, M.; Deeks, J.; Harbord, R.; Altman, D.; Steichen, T. METAN: Stata module for fixed and random effects meta-analysis. In Statistical Software Components; Boston College Department of Economics: Boston, MA, USA, 2010. [Google Scholar]
- Sterne, J. METAFUNNEL: Stata module to produce funnel plots for meta-analysis. Res. Pap. Econ. 2003. Available online: https://EconPapers.repec.org/RePEc:boc:bocode:s434101 (accessed on 6 August 2020).
- Harbord, R.; Harris, R.J.; Sterne, J.A.; Steichen, T. METABIAS: Stata module to test for small-study effects in meta-analysis. Res. Pap. Econ. 2009. Available online: https://EconPapers.repec.org/RePEc:boc:bocode:s404901 (accessed on 10 August 2020).
- Furuya-Kanamori, L. LFK: Stata module to compute LFK index and Doi plot for detection of publication bias in meta-analysis. Res. Pap. Econ. 2020. Available online: https://EconPapers.repec.org/RePEc:boc:bocode:s458762 (accessed on 14 August 2020).
- Daly, J.M.; Hearne, B.; Dunaj, J.; LePorte, B.; Vikram, B.; Strong, E.; Green, M.; Muggio, F.; Groshen, S.; DeCosse, J.J. Nutritional rehabilitation in patients with advanced head and neck cancer receiving radiation therapy. Am. J. Surg. 1984, 148, 514–520. [Google Scholar] [CrossRef]
- Samuel, S.R.; Maiya, A.G.; Fernandes, D.J.; Guddattu, V.; Saxena, P.P.; Kurian, J.R.; Lin, P.-J.; Mustian, K.M. Effectiveness of exercise-based rehabilitation on functional capacity and quality of life in head and neck cancer patients receiving chemo-radiotherapy. Supportive Care Cancer 2019, 27, 3913–3920. [Google Scholar] [CrossRef]
- Cereda, E.; Cappello, S.; Colombo, S.; Klersy, C.; Imarisio, I.; Turri, A.; Caraccia, M.; Borioli, V.; Monaco, T.; Benazzo, M.; et al. Nutritional counseling with or without systematic use of oral nutritional supplements in head and neck cancer patients undergoing radiotherapy. Radiother. Oncol. 2018, 126, 81–88. [Google Scholar] [CrossRef]
- Hearne, B.E.; Dunaj, J.M.; Daly, J.M.; Strong, E.W.; Vikram, B.; LePorte, B.J.; DeCosse, J.J. Enteral nutrition support in head and neck cancer: Tube vs. oral feeding during radiation therapy. J. Am. Diet. Assoc. 1985, 85, 669–674. [Google Scholar]
- Isenring, E.; Capra, S.; Bauer, J.; Davies, P.S. The impact of nutrition support on body composition in cancer outpatients receiving radiotherapy. Acta Diabetol. 2003, 40 (Suppl. 1), S162–S164. [Google Scholar] [CrossRef]
- Jiang, W.; Ding, H.; Li, W.; Ling, Y.; Hu, C.; Shen, C. Benefits of oral nutritional supplements in patients with locally advanced nasopharyngeal cancer during concurrent chemoradiotherapy: An exploratory prospective randomized trial. Nutr. Cancer 2018, 70, 1299–1307. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro-Grillo, I.; Marques Vidal, P.; Camilo, M.E. Impact of nutrition on outcome: A prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck J. Sci. Spec. Head Neck 2005, 27, 659–668. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Anton, P.M.; Fogleman, A.; Hopkins-Price, P.; Verhulst, S.; Rao, K.; Malone, J.; Robbs, R.; Courneya, K.S.; Nanavati, P.; et al. Pilot, randomized trial of resistance exercise during radiation therapy for head and neck cancer. Head Neck 2013, 35, 1178–1188. [Google Scholar] [CrossRef]
- Roussel, L.; Micault, E.; Peyronnet, D.; Blanchard, D.; Guarnieri, S.; Choussy, O.; Gery, B.; Bequignon, A.; Joubert, C.; Parienti, J.; et al. Intensive nutritional care for patients treated with radiotherapy in head and neck cancer: A randomized study and meta-analysis. Eur. Arch. Otorhinolaryngol. 2017, 274, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.R.; Maiva, G.A.; Babu, A.S.; Vidyasagar, M.S. Effect of exercise training on functional capacity & quality of life in head & neck cancer patients receiving chemoradiotherapy. Indian J. Med. Res. 2013, 137, 515–520. [Google Scholar] [PubMed]
- Zhao, S.G.; Alexander, N.B.; Djuric, Z.; Zhou, J.; Tao, Y.; Schipper, M.; Feng, F.Y.; Eisbruch, A.; Worden, F.P.; Strath, S.J.; et al. Maintaining physical activity during head and neck cancer treatment: Results of a pilot controlled trial. Head Neck 2016, 38 (Suppl. 1), E1086–E1096. [Google Scholar] [CrossRef] [Green Version]
- Capozzi, L.C.; McNeely, M.L.; Lau, H.Y.; Reimer, R.A.; Giese-Davis, J.; Fung, T.S.; Culos-Reed, S.N. Patient-reported outcomes, body composition, and nutrition status in patients with head and neck cancer: Results from an exploratory randomized controlled exercise trial. Cancer 2016, 122, 1185–1200. [Google Scholar] [CrossRef] [Green Version]
- Weaver, C.M.; Miller, J.W. Challenges in conducting clinical nutrition research. Nutr. Rev. 2017, 75, 491–499. [Google Scholar] [CrossRef]
- de Vries, J.; Antoine, J.-M.; Burzykowski, T.; Chiodini, A.; Gibney, M.; Kuhnle, G.; Méheust, A.; Pijls, L.; Rowland, I. Markers for nutrition studies: Review of criteria for the evaluation of markers. Eur. J. Nutr. 2013, 52, 1685–1699. [Google Scholar] [CrossRef]
- Deutz, N.E.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The underappreciated role of low muscle mass in the management of malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Prado, C.M.; Purcell, S.A.; Alish, C.; Pereira, S.L.; Deutz, N.E.; Heyland, D.K.; Goodpaster, B.H.; Tappenden, K.A.; Heymsfield, S.B. Implications of low muscle mass across the continuum of care: A narrative review. Ann. Med. 2018, 50, 675–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, T.S.; Scott, J.M.; Michalski, M.; Capaci, C.; Thomas, S.; Herndon, J.E. Novel methods for reporting of exercise dose and adherence: An exploratory analysis. Med. Sci. Sports Exerc. 2018, 50, 1134. [Google Scholar] [CrossRef]
- Fayh, A.P.T.; de Sousa, I.M.; Gonzalez, M.C. New insights on how and where to measure muscle mass. Curr. Opin. Supportive Palliat. Care 2020. [Google Scholar] [CrossRef]
- Vasiloglou, M.F.; Fletcher, J.; Poulia, K.-A. Challenges and perspectives in nutritional counselling and nursing: A narrative review. J. Clin. Med. 2019, 8, 1489. [Google Scholar] [CrossRef] [Green Version]
- McCarter, K.; Baker, A.L.; Britton, B.; Halpin, S.A.; Beck, A.; Carter, G.; Wratten, C.; Bauer, J.; Wolfenden, L.; Burchell, K. Head and neck cancer patient experience of a new dietitian-delivered health behaviour intervention: ‘you know you have to eat to survive’. Supportive Care Cancer 2018, 26, 2167–2175. [Google Scholar] [CrossRef] [Green Version]
- Endevelt, R.; Gesser-Edelsburg, A. A qualitative study of adherence to nutritional treatment: Perspectives of patients and dietitians. Patient Prefer. Adherence 2014, 8, 147. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, I.B.; Lima, E.d.N.S.; Canto, P.P.L.; Gontijo, C.A.; Maia, Y.C.d.P.; Pena, G.d.G. Oral nutritional supplementation affects the dietary intake and body weight of head and neck cancer patients during (Chemo) radiotherapy. Nutrients 2020, 12, 2516. [Google Scholar] [CrossRef]
- Sladdin, I.; Ball, L.; Bull, C.; Chaboyer, W. Patient-centred care to improve dietetic practice: An integrative review. J. Hum. Nutr. Diet. 2017, 30, 453–470. [Google Scholar] [CrossRef]
- Williams, G.F.; White, H.; Sen, M.; Prestwich, R.J.D. Patients’ experience of enteral feeding following (chemo) radiotherapy for head and neck cancer: A qualitative study. Clin. Nutr. 2019, 38, 1382–1389. [Google Scholar] [CrossRef]
- Sandmæl, J.A.; Sand, K.; Bye, A.; Solheim, T.S.; Oldervoll, L.; Helvik, A.S. Nutritional experiences in head and neck cancer patients. Eur. J. Cancer Care 2019, 28, e13168. [Google Scholar] [CrossRef] [Green Version]
- Orell, H.; Schwab, U.; Saarilahti, K.; Österlund, P.; Ravasco, P.; Mäkitie, A. Nutritional counseling for head and neck cancer patients undergoing (chemo) radiotherapy—A prospective randomized trial. Front. Nutr. 2019, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H. Exercise guidelines for cancer survivors: Consensus statement from international multidisciplinary roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweegers, M.G.; Altenburg, T.M.; Chinapaw, M.J.; Kalter, J.; Verdonck-de Leeuw, I.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; Brug, J. Which exercise prescriptions improve quality of life and physical function in patients with cancer during and following treatment? A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2018, 52, 505–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Adults diagnosed with HNC, receiving RT with curative intent (± concomitant CT) | Patients <18 years of age, cancer with another origin, surgery as only treatment |
| Intervention | (1) Physical exercise or (2) nutrition or (3) a combination of exercise and nutrition. Initiated at start of RT and conducted during RT. Physical exercise is defined as sessions of muscle strength and/or aerobic exercise. Nutrition is defined as, dietary counselling, oral nutritional supplements or enteral nutrition by nasogastric tube or PEG | (1) Interventions initiated before start or after completion of RT (2) Nutritional interventions consisting only of vitamins or minerals (3) Comparisons of enteral and parenteral solutions (4) Swallowing exercise interventions alone |
| Comparator | Standard care or placebo | |
| Outcome | Nutritional status (validated assessment instruments, e.g., SGA or PG-SGA), body composition (body weight, BMI, muscle mass or lean body mass, fat mass) and/or objectively measured physical functioning (walk test, handgrip strength, physical or performance battery) | Quality of life, fatigue, feasibility, treatment tolerance or survival as only outcome measure |
| Study design | RCTs or pilot RCTs | Case series with <10 participants, qualitative studies, reviews, letters, editorials, notes |
| Setting | No restrictions | |
| Time frame | No restrictions |
| Author, Year | Country | Study Design | Type of Intervention | Sample Size | Age in Years | Clinical Info Included Patients | Cancer Treatment |
|---|---|---|---|---|---|---|---|
| Capozzi, 2016 [10] | Canada | Pilot RCT | Exercise and nutrition | 60 male 82% | Mean (SD) 56.1 (9.2) | Diagnosis (n): Larynx-hypopharynx (6), Nasopharynx (4), Oral (8), Oropharynx (29), Other (6), Unknown origin (7) Stage (n): I-III (11), IV (48) Histology: NA | RT (n = 16) CRT (n = 44) |
| Cereda, 2018 [23] | Italy | RCT | Nutrition | 159 male 72% | Mean (SD) Counselling 63.8 (12.7); counselling + ONS 66.5 (14.5) | Diagnosis (n): Hypopharynx (13), Larynx (41), Naso- oropharynx (44), Oral (29), Other (32) Stage (n): 0-II (76), III (40), IV (34) Histology (n): Squamous (124), Lymphoma (20), other (15) | RT (n = 98) and CRT (n = 61) |
| Daly, 1984 [21] | USA | RCT | Nutrition | 40 male 80% | Mean (SD), Intervention 53 (15) Control 55 (13) | Diagnosis (n): Nasopharynx (15), Other (25) Stage (n): II (2), III (9), IV (28) Histology: NA | All RT |
| Hearne, 1989 [24] | USA | RCT | Nutrition | 31 male 77% | Mean (range), Intervention 52.1 (22–74) Control 56.1 (37–83) | Diagnosis (n): Nasopharynx (9), Other (22) Stage (n): III (11), IV (20) Histology: NA | All RT |
| Isenring, 2003 [25] | Australia | RCT | Nutrition | 36 male 81% | Mean (SD), 63 (15) | Diagnosis: NA Stage: NA Histology: NA | All RT |
| Jiang, 2018 [26] | China | RCT | Nutrition | 100 male 69% | Mean (SD), Intervention 46.7 (10.9)) Control 48.2 (11.1) | Diagnosis: Nasopharynx Stage: III (43), IVa-b (57) Histology: NA | All CRT |
| Ravasco, 2005 [27] | Portugal | RCT | Nutrition | 75 male 80% | Mean (SD) 60 (11) | Diagnosis (n NA): Larynx, Oropharynx, Nasopharynx, Tongue Stage (n): I-II (30), III-IV (45) Histology: NA | All RT (all pre-vious CT) |
| Rogers, 2013 [28] | USA | Pilot RCT | Exercise and nutrition | 15 male 80% | Mean (SD) 60.5 (12.5) | Diagnosis (n): Nasopharynx, scalp and salivary glands (5), Other (10)Stage (n): I-II (7), III -IV (8) Histology: NA | RT (n = 11), CRT (n = 4) |
| Roussel, 2017 [29] | France | RCT | Nutrition | 87 male 81% | Mean (SD) 60 (10) | Diagnosis (n): Hypopharynx (11), Larynx (19), Oral (9), Oropharynx (40), Nasopharynx (2), Sinus (2), Unknown origin (4) Stage (n): I-II (14), III (14), IV-V (59) Histology: NA | RT (n = 28), CRT (n = 59) |
| Sandmaell, 2017 [9] | Norway | Pilot RCT | Exercise and nutrition | 41 male 61% | Mean (SD) 63.2 (9.3) | Diagnosis (n): Larynx (4), Nasal (1), Oral (5), Pharynx (20), Pharynx and larynx (1), Salivary glands (8), Unknown origin (2) Stage and histology: NA | RT (n = 24), CRT (n = 17) |
| Samuel, 2019 [22] | India | RCT | Exercise | 148 | Mean (SD) Intervention: 52.8 (9.7) Control: 52.8 (10.5) | Diagnosis (n): Larynx (28), Oropharynx (120) Stage (n): III (38), IVa (94), IVb (16) Histology: NA | All CRT |
| Samuel, 2013 [30] | India | RCT | Exercise | 48 male 88% | Mean (SD) Intervention: 51.7 (10) Control: 52.5 (8.27) | Diagnosis: NA Stage: NA Histology: NA | All CRT |
| Zhao, 2016 [31] | USA | Pilot RCT | Exercise and nutrition | 18 male 94% | Mean (SD) 57 (11) | Diagnosis (n): Larynx (1), Pharynx (15), Unknown origin (1) Stage (n): III (4), IV (7) Histology (n): NA | All CRT |
| Study | Intervention Type | Criteria * | Total | Quality ** | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||||
| Randomized Controlled Trials | ||||||||||||||
| Samuel, 2019 [22] | Exercise | + | + | + | + | − | − | − | + | − | + | + | 7 | Moderate |
| Samuel, 2013 [30] | Exercise | + | + | − | + | − | − | − | − | − | + | + | 5 | Moderate |
| Cereda, 2018 [23] | Nutrition | + | + | + | + | − | − | − | + | + | + | + | 8 | High |
| Jiang, 2018 [26] | Nutrition | + | + | + | + | − | − | − | + | + | + | + | 8 | High |
| Roussel, 2017 [29] | Nutrition | + | + | + | + | − | − | − | − | − | + | + | 6 | Moderate |
| Ravasco, 2005 [27] | Nutrition | ? | + | + | ? | − | − | − | + | + | + | + | 6 | Moderate |
| Isenring, 2003 [25] | Nutrition | − | + | ? | + | − | − | ? | + | − | ? | + | 4 | Low |
| Hearne, 1989 [24] | Nutrition | − | ? | ? | ? | − | − | − | − | − | + | + | 2 | Low |
| Daly, 1984 [21] | Nutrition | + | − | ? | ? | − | − | − | ? | − | + | − | 2 | Low |
| Pilot and Feasibility Studies | ||||||||||||||
| Sandmael, 2017 [9] | Exercise and nutrition | + | + | + | + | − | − | − | + | − | + | + | 6 | Moderate |
| Capozzi, 2016 [10] | Exercise and nutrition | + | + | + | + | − | − | + | − | + | + | − | 7 | Moderate |
| Zhao, 2016 [31] | Exercise and nutrition | + | + | + | + | + | + | + | + | + | + | + | 10 | High |
| Rogers, 2013 [28] | Exercise and nutrition | + | + | + | + | − | − | − | + | + | + | + | 8 | High |
| Randomized Controlled Trials | |||||
| Study | Intervention Type | Description of Intervention | Length of Intervention | Intervention Adherence | Completion Rate |
| Samuel, 2019 [22] | Exercise | Intervention: Brisk walking for 15–20 min and resistance training for major muscles of upper and lower limb, 2 sets and 8−15 repetitions. Exercise sessions monitored at the hospital, five days a week followed by a monitored home-based program. Control: Physical exercise recommendation, 10 min walks during the day five days a week. | Seven weeks during RT at the hospital followed by four weeks at home | NA | 120/148 Lost: Intervention 16 Control 12 |
| Samuel, 2013 [30] | Exercise | Intervention: Brisk walking for 15−20 min at perceived exertion rate between 3−5/10, five days a week. Individually tailored program for major muscle groups of upper and lower limbs 2−3 sets and 8−10 repetitions. Exercise sessions five days a week. Control: No scheduled exercise sessions but advised to remain as physically active as possible. | Intervention during RT, 6 weeks | NA | 43/48 Lost: Intervention 4 Control 1 |
| Cereda, 2018 [23] | Nutrition | Intervention: Nutritional counseling based on estimated protein−calorie requirement (1.2 g/kg of actual body weight), personal eating patterns and preferences, chewing and swallowing abilities. Addition of 1−2 bottles/day of n−3 polyunsaturated fatty acids−enriched ONS. Follow−up during RT: once a week for 6 weeks. After RT: one month and three months Control: Nutritional counseling as described above. No n−3 ONS but for ethical reasons ONS were prescribed when food intake was too low (< 60% of estimated requirements for two consecutive weeks). EN or PN was started if intake was too low for two consecutive weeks despite the use of ONS. | During RT and 3 months follow−up | NA, but protein intake (g protein/kg/day) described: End of RT: Intervention 1.0 vs. control 0.87 1 month after RT: Intervention 1.16 vs. control 0.97 3 months after RT: Intervention 1.12 vs. control 0.96 | 112/159 Lost: Intervention 22 Control 25 |
| Jiang, 2018 [26] | Nutrition | Intervention: ONS 100g/day (402 kcal, 18 g protein) Control: No ONS General dietary advices in both groups every week PN with glucose if intake was severely compromised | During CRT | Consumed 52.1 g (29.4g)/day | 91/100 Lost: Intervention 5 Control 4 |
| Roussel, 2017 [29] | Nutrition | Intervention: Six individualized counselling meetings with a dietitian at home (two during RT and four at the end of RT). One meeting 2 months after end of RT. Energy and protein requirements individually evaluated and nutritional adjustments obtained with regular foods, ONS or EN if necessary. Education for self−monitoring weight, adapting intake and modifying food textures. Control: As described above but only two outpatient consultations with a dietitian during RT. Recalls if needed. | During RT, 3 months follow−up | NA but energy intake (kcal/kg/day) described: 1 month after RT: Intervention 34 vs. control 33 3 months after RT: Intervention 35 vs. control 31 | 87/117 Lost: Intervention 16 Control 14 |
| Ravasco, 2005 [27] | Nutrition | Group 1 (n = 25): individualized counselling with regular foods Group 2 (n = 25): usual diet plus ONS (2 × 200 mL containing 20 g protein and 200 kcal per day) Group 3 (n = 25): intake ad libitum Nutritional goal for group 1 and 2 was achievement of individually calculated energy and protein requirements | Intervention during RT, 3 months follow−up | NA, but nutritional intake was primary endpoint and reported Baseline: intake similar in all groups End of RT: group 1 increase of 521 kcal/day, p = 0.002 ONS increase of 322 kcal/day, p = 0.05 Ad lib decrease of 400 kcal/day, p ≤ 0.01 Between−group finding, p = 0.005 3 months: group 1 maintained energy intake, other groups decreased, p = 0.001 | All completed |
| Isenring, 2003 [25] | Nutrition | Intervention: Individualized counselling by using a standard protocol (American Dietetic Association Medical Nutrition Therapy Head and Neck). ONS were provided when appropriate Control: Regular care, general advice by the nursing staff with samples of ONS if felt necessary. | Intervention during RT, 3 months follow−up | NA | 32/36 Lost: Intervention 1 Control 3 |
| Hearne, 1985 [24] | Nutrition | Intervention: Intensive nasogastric feeding during RT Control: Oral intake and dietary counselling Goal for intervention in both groups: 40 kcal/kg per day and 1g protein/kg per day | Intervention during RT, 1 month follow−up | Intervention: Two of 14 (14%) refused tube feeding and converted to control Control: Two of 12 (16%) converted to intervention due to weight loss Energy intake during RT (kcal/kg): Intervention 35−42 vs. control 15−34 No p−values given. | 26/31 Lost: Intervention 4 Control 1 |
| Daly, 1984 [21] | Nutrition | Intervention: EN Control: Oral intake and dietary counselling Goal in both groups: 40 kcal/kg per day and 1−1.5 g protein/kg per day. If weight gain did not occur after each week +5 kcal/kg per day. Both groups received enteral support throughout RT (approximately 8 weeks) and for several additional weeks until reaction to radiation subsided | Intervention during and up to 6 months follow−up | Intervention: Two of 22 (9%) converted to control due to non−compliance during the first week of RT Control: Two of 15 (11%) converted to tube feeding due to weight loss during the two first weeks of RT Energy intake (kcal/kg): Tube fed 39 vs. orally 30, p < 0.00 | 35/38 Lost: NA |
| Pilot and Feasibility Studies | |||||
| Study | Intervention Type | Description of Intervention | Length of Intervention | Intervention Adherence | Completion Rate |
| Sandmæl, 2017 [9] | Exercise and nutrition | Group 1: During treatment: Resistance exercises: 2 lower body− and 2 upper body, 3−4 sets, 6 to 12 repetitions, monitored by a physiotherapist at the hospital twice a week á 30 min (total 12 sessions). Recommended 150 min of moderate intensity exercise per week in addition. After the training sessions one bottle ONS. Recommended to take 1−2 ONS each day. Group 2: During treatment: Recommended to follow physical exercise guidelines for cancer patients. 2−4 weeks after end of RT: 3 weeks stay at rehabilitation centre. Resistance exercises: 3 sessions of 45 min of involving 3 upper body and 3 lower body exercises. 3−4 sets and 6 to 12 repetitions plus two voluntary sessions each week involving a combination of strength, aerobic and balance exercises with low intensity. Dietary counselling once a week in small groups and use of ONS. | Intervention during RT for group 1 and intervention after RT for group 2 Intervention initiated during the first week of radiotherapy lasting 6 weeks. | Adherence rates (%): Interv during RT, exercise 81 and ONS 57 After RT, exercise 94 and ONS 76 | 29/41 Lost: Intervention 2 Control 10 |
| Zhao, 2016 [31] | Exercise and nutrition | Group 1: Intervention based on guidelines for patients with cancer (American College of Sports Medicine); strengthening, cardiovascular fitness and physical exercise. Exercise during the 7 weeks CRT at a clinical research center supervised by a trainer. Up to 3 sessions per week, lasting up to 1 h including warmup, cool down, and rest periods. Resistance exercises included chest press, wall push up, military press, side arm raises, biceps curl, shoulder shrugs, and calf raises. Duration and intensity were customized to the individual, goal three 8 to 12 repetition sets. Aerobic exercise was defined as walking with a pedometer and a goal to maintain step count based on the mean step count of the previous training week. Post CRT (weeks 8 to 14), integration of exercise activities into own lifestyle. Weekly telephone calls from the trainer. Before CRT counselling by a dietician, repeated in case of decrease in BMI greater than a 5% to 10%. Group 2: Standard treatment, dietary counselling and active nutritional surveillance during RT, neither encouraged nor discouraged to exercise. | Intervention for 7 weeks 7 weeks follow up | Exercise adherence rate 72%, Completed 15.2 of 21 sessions. | 17/20 Lost: Intervention 1 Control 2 |
| Rogers, 2013 [28] | Exercise and nutrition | Group 1: Nutritional counseling and 12 weeks resistance exercise. Exercise during treatment; one hour supervised sessions twice weekly at a training facility at the hospital. Six weeks of twice weekly home−based sessions supported with telephone counseling, written materials, and DVD. Up to 10 repetitions of 9 different exercises using a resistance band for major muscle groups (chest press, leg extension, lateral row, reverse curl, triceps using wall push−up/triceps kickback, heel raise, 2−arm front raise, hamstring curl, and arm curl). Intensity: light, moderate and heavy resistance bands were used. Group 2: Nutritional counseling provided by registered dietitian according to standard counseling appropriate for head and neck cancer during radiotherapy | 12 weeks intervention | Exercise adherence: 6 weeks: 83% 6−12 weeks: 62% Both groups Face to face nutritional counselling (6 weeks): 96% completed Telephone counselling (6−12 weeks): 77% completed | 13/15 Lost: Intervention 2 Control 0 |
| Capozzi, 2016 [10] | Lifestyle interventions including exercise and nutrition | Group 1: 12 weeks lifestyle intervention during RT and Group 2: same intervention immediately after completion of RT. Components of intervention: physician referral and clinical support; health education; behavioral change support; individual exercise program (home exercises twice a week); group−based exercise (2 exercise sessions weekly) Exercise program: progressive resistance training with 2 sets of 8 repetitions at 8 to 10 repetitions maximum for 10 exercises targeting major muscle groups. In addition to exercise sessions participants were required to attend 6 education sessions biweekly | Immediate intervention during RT for group 1 and delayed intervention after RT for group 2 Total 24 weeks | NA | 36/60 Lost: Group1: 15 Group 2: 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bye, A.; Sandmael, J.A.; Stene, G.B.; Thorsen, L.; Balstad, T.R.; Solheim, T.S.; Pripp, A.H.; Oldervoll, L.M. Exercise and Nutrition Interventions in Patients with Head and Neck Cancer during Curative Treatment: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3233. https://doi.org/10.3390/nu12113233
Bye A, Sandmael JA, Stene GB, Thorsen L, Balstad TR, Solheim TS, Pripp AH, Oldervoll LM. Exercise and Nutrition Interventions in Patients with Head and Neck Cancer during Curative Treatment: A Systematic Review and Meta-Analysis. Nutrients. 2020; 12(11):3233. https://doi.org/10.3390/nu12113233
Chicago/Turabian StyleBye, Asta, Jon A. Sandmael, Guro B. Stene, Lene Thorsen, Trude R. Balstad, Tora S. Solheim, Are Hugo Pripp, and Line M. Oldervoll. 2020. "Exercise and Nutrition Interventions in Patients with Head and Neck Cancer during Curative Treatment: A Systematic Review and Meta-Analysis" Nutrients 12, no. 11: 3233. https://doi.org/10.3390/nu12113233