Fruit and Vegetable Knowledge and Intake within an Australian Population: The AusDiab Study

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
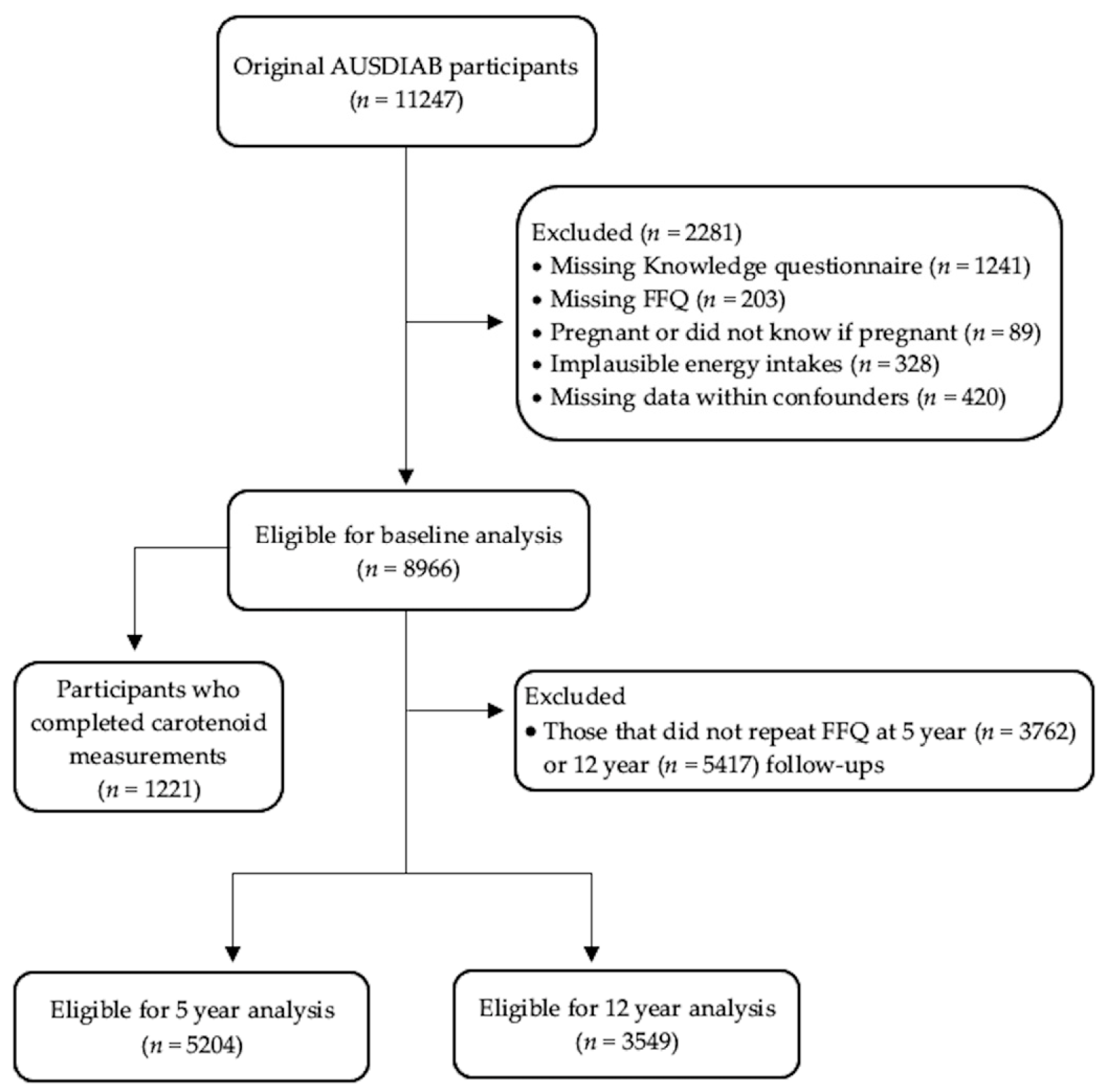
2.1. Data Collection
2.2. Variables
2.2.1. Fruit and Vegetable Knowledge
2.2.2. Fruit and Vegetable Intake
2.2.3. Serum Carotenoids
2.3. Baseline Demographics and Assessments
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Demographic Characteristics
3.2. Fruit and Vegetable Knowledge and Intake
3.3. Fruit and Vegetable Knowledge and Intake over 12 years
3.4. Fruit and Vegetable Knowledge and Serum Carotenoids
4. Discussion
4.1. The Association between Fruit and Vegetable Knowledge and Intake
4.2. Targeting Those at Risk
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- World Health Organisation. Global Health Estimates 2016: Disease Burden by Cause, Age, Sex, by Country and by Region, 2000–2016; World Health Institution: Geneva, Switzerland, 2018. [Google Scholar]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidem. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. National Health Survey: First Results, 2017-18; Commonwealth of Australia: Sydney, Australia, 2018. [Google Scholar]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global Variability in Fruit and Vegetable Consumption. Am. J. Prev. Med. 2009, 36, 402–409.e5. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bailey, R.L.; Blumberg, J.B.; Burton-Freeman, B.; Chen, C.-Y.O.; Crowe-White, K.M.; Drewnowski, A.; Hooshmand, S.; Johnson, E.; Lewis, R.; et al. Fruits, vegetables, and health: A comprehensive narrative, umbrella review of the science and recommendations for enhanced public policy to improve intake. Crit. Rev. Food Sci. Nutr. 2020, 60, 2174–2211. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation and Food and Agriculture Organization of the United Nations. Fruit and Vegetables for Health: Report of a Joint FAO/WHO Workshop on Fruit and Vegetables for Health, 1–3 September 2004, Kobe, Japan; World Health Organisation: Geneva, Switzerland, 2004. [Google Scholar]
- Habauzit, V.; Morand, C. Evidence for a protective effect of polyphenols-containing foods on cardiovascular health: An update for clinicians. Ther. Adv. Chronic Dis. 2011, 3, 87–106. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.H. Health-Promoting Components of Fruits and Vegetables in the Diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef]
- Zhu, F.; Du, B.; Xu, B. Anti-inflammatory effects of phytochemicals from fruits, vegetables, and food legumes: A review. Crit. Rev. Food Sci. Nutr. 2018, 58, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Sim, M.; Bondonno, C.P.; Bondonno, N.P.; Ward, N.C.; Prince, R.L.; Devine, A.; Lewis, J.R.; Hodgson, J.M. Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review. Nutrients 2018, 10, 595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, Y.; Tong, X.; Li, L.; Cao, S.; Yin, X.; Gao, C.; Herath, C.; Li, W.; Jin, Z.; Chen, Y.; et al. Consumption of fruit and vegetable and risk of coronary heart disease: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2015, 183, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Huang, J.; Wang, Y.; Zhang, D.; Qu, Y. Fruits and Vegetables Consumption and Risk of Stroke. Stroke 2014, 45, 1613–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Sun, D.; He, Y. Fruit and vegetables consumption and incident hypertension: Dose–response meta-analysis of prospective cohort studies. J. Hum. Hypertens. 2016, 30, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.; Bauman, A.E.; Gale, J.; Banks, E.; Kritharides, L.; Ding, D. Fruit and vegetable consumption and all-cause mortality: Evidence from a large Australian cohort study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 9. [Google Scholar] [CrossRef] [PubMed]
- Chapman, K.; Havill, M.; Watson, W.L.; Wellard, L.; Hughes, C.; Bauman, A.; Allman-Farinelli, M. Time to address continued poor vegetable intake in Australia for prevention of chronic disease. Appetite 2016, 107, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Erinosho, T.O.; Parks, C.A.; Nebeling, L.C.; Moser, R.P.; Shaikh, A.R.; Resnicow, K.; Oh, A.Y.; Yaroch, A.L. Development and Implementation of the National Cancer Institute’s Food Attitudes and Behaviors Survey to Assess Correlates of Fruit and Vegetable Intake in Adults. PLoS ONE 2015, 10, e0115017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Morrow, L.; Ludbrook, A.; MacDiarmid, J.; Olajide, D. Perceived barriers towards healthy eating and their association with fruit and vegetable consumption. J. Public Health 2016, 39, fdw038-338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinho, M.G.M.; MacKenbach, J.D.; Charreire, H.; Oppert, J.-M.; Bárdos, H.; Glonti, K.; Rutter, H.; Compernolle, S.; De Bourdeaudhuij, I.; Beulens, J.W.J.; et al. Exploring the relationship between perceived barriers to healthy eating and dietary behaviours in European adults. Eur. J. Nutr. 2018, 57, 1761–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, A.R.; Yaroch, A.L.; Nebeling, L.; Yeh, M.-C.; Resnicow, K. Psychosocial Predictors of Fruit and Vegetable Consumption in Adults. Am. J. Prev. Med. 2008, 34, 535–543.e11. [Google Scholar] [CrossRef]
- Backholer, K.; Spencer, E.; Gearon, E.; Magliano, D.J.; McNaughton, S.A.; E Shaw, J.; Peeters, A. The association between socio-economic position and diet quality in Australian adults. Public Health Nutr. 2015, 19, 477–485. [Google Scholar] [CrossRef] [Green Version]
- Olstad, D.L.; Leech, R.M.; Livingstone, K.M.; Ball, K.; Thomas, B.; Potter, J.; Cleanthous, X.; Reynolds, R.; McNaughton, S.A. Are dietary inequalities among Australian adults changing? A nationally representative analysis of dietary change according to socioeconomic position between 1995 and 2011–13. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Sui, Z.; Wong, W.K.; Louie, J.C.Y.; Rangan, A. Discretionary food and beverage consumption and its association with demographic characteristics, weight status, and fruit and vegetable intakes in Australian adults. Public Health Nutr. 2017, 20, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Aaby, A.; Friis, K.; Christensen, B.; Rowlands, G.; Maindal, H.T. Health literacy is associated with health behaviour and self-reported health: A large population-based study in individuals with cardiovascular disease. Eur. J. Prev. Cardiol. 2017, 24, 1880–1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Beauchamp, A.; Dodson, S.; O’Hara, J.; McPhee, C.; Fulton, A.; Wildey, C.; Osborne, R. Health literacy and fruit and vegetable intake in rural Australia. Public Health Nutr. 2017, 20, 2680–2684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appleton, K.M.; Krumplevska, K.; Smith, E.; Rooney, C.; McKinley, M.C.; Woodside, J.V. Low fruit and vegetable consumption is associated with low knowledge of the details of the 5-a-day fruit and vegetable message in the UK: Findings from two cross-sectional questionnaire studies. J. Hum. Nutr. Diet. 2017, 31, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Dickson-Spillmann, M.; Siegrist, M. Consumers’ knowledge of healthy diets and its correlation with dietary behaviour. J. Hum. Nutr. Diet. 2010, 24, 54–60. [Google Scholar] [CrossRef]
- Worsley, A. Nutrition knowledge and food consumption: Can nutrition knowledge change food behaviour? Asia Pac. J. Clin. Nutr. 2002, 11, S579–S585. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, L.B.; Vasconcelos, S.M.L.; Correia, L.O.D.S.; Ferreira, R.C. Nutrition knowledge assessment studies in adults: A systematic review. Ciên. Saúde Colet. 2016, 21, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Aaction: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef]
- Wallace, R.; Lo, J.; Devine, A. Tailored nutrition education in the elderly can lead to sustained dietary behaviour change. J. Nutr. Health Aging 2016, 20, 8–15. [Google Scholar] [CrossRef]
- Kothe, E.J.; Mullan, B. A randomised controlled trial of a theory of planned behaviour to increase fruit and vegetable consumption. Fresh Facts. Appetite 2014, 78, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.; Zimmet, P.Z.; A Welborn, T.; Cameron, A.J.; Shaw, J.; De Courten, M.; Jolley, D.; Mccarty, D.J. The Australian Diabetes, Obesity and Lifestyle Study (AusDiab)—methods and response rates. Diabetes Res. Clin. Pr. 2002, 57, 119–129. [Google Scholar] [CrossRef] [Green Version]
- AusDiab. The Australian Diabetes, Obesity and Lifestyle Study: Health Knowledge, Attitudes & Practices Questionnaire. Available online: https://baker.edu.au/-/media/documents/impact/ausdiab/questionnaires/ausdiab-health-knowledge-questionnaire-1999.pdf?la=en (accessed on 6 June 2019).
- Hodge, A.M.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Ireland, P.; Jolley, D.; Giles, G.; O’Dea, K.; Powles, J.; Rutishauser, I.; Wahlqvist, M.L.; Williams, J. Development of the Melbourne FFQ: A food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pac. J. Clin. Nutr. 1994, 3, 19–31. [Google Scholar]
- National Health and Medical Research Council. National Health and Medical Research Council. Australian Dietary Guidelines (Reference N55a); National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Coyne, T.; Ibiebele, T.I.; McNaughton, S.A.; Rutishauser, I.H.E.; O’Dea, K.; Hodge, A.M.; McClintock, C.; Findlay, M.G.; Lee, A. Evaluation of brief dietary questions to estimate vegetable and fruit consumption—using serum carotenoids and red-cell folate. Public Health Nutr. 2005, 8, 298–308. [Google Scholar] [CrossRef] [Green Version]
- Talwar, D.; Ha, T.K.; Cooney, J.; Brownlee, C.; Jo’Reilly, D.S. A routine method for the simultaneous measurement of retinol, α-tocopherol and five carotenoids in human plasma by reverse phase HPLC. Clin. Chim. Acta 1998, 270, 85–100. [Google Scholar] [CrossRef]
- Dalton, M.; Cameron, A.J.; Zimmet, P.Z.; Shaw, J.E.; Jolley, D.; Dunstan, D.W.; Welborn, T.A. On behalf of the AusDiab Steering Committee Waist circumference, waist-hip ratio and body mass index and their correlation with cardiovascular disease risk factors in Australian adults. J. Intern. Med. 2003, 254, 555–563. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. The Active Australia Survey: A Guide and Manual for Implementation, Analysis and Reporting. Available online: Aihw.gov.au/reports/physical-activity/active-australia-survey/contents/table-of-contents (accessed on 18 January 2020).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000; pp. 1–253. [Google Scholar]
- Trewin, D. Information Paper—Census of Population and Housing: Socio-Economic Indexes for Areas Australia 2001; Australian Bureau of Statistics: Canberra, Australia, 2003.
- Colón-Ramos, U.; Rutten, L.J.F.; Moser, R.P.; Colón-López, V.; Martínez, A.P.O.; Yaroch, A.L. The Association Between Fruit and Vegetable Intake, Knowledge of the Recommendations, and Health Information Seeking Within Adults in the U.S. Mainland and in Puerto Rico. J. Health Commun. 2014, 20, 105–111. [Google Scholar] [CrossRef]
- Erinosho, T.O.; Moser, R.P.; Oh, A.; Nebeling, L.C.; Yaroch, A.L. Awareness of the Fruits and Veggies—More Matters campaign, knowledge of the fruit and vegetable recommendation, and fruit and vegetable intake of adults in the 2007 Food Attitudes and Behaviors (FAB) Survey. Appetite 2012, 59, 155–160. [Google Scholar] [CrossRef]
- Farragher, T.; Wang, W.C.; Worsley, A. The associations of vegetable consumption with food mavenism, personal values, food knowledge and demographic factors. Appetite 2016, 97, 29–36. [Google Scholar] [CrossRef]
- Taylor, M.K.; Sullivan, D.K.; Ellerbeck, E.F.; Gajewski, B.J.; Gibbs, H.D. Nutrition literacy predicts adherence to healthy/unhealthy diet patterns in adults with a nutrition-related chronic condition. Public Health Nutr. 2019, 22, 2157–2169. [Google Scholar] [CrossRef] [PubMed]
- Thompson, O.M.; Yaroch, A.L.; Moser, R.P.; Rutten, L.J.F.; Petrelli, J.M.; Smith-Warner, S.A.; Mâsse, L.C.; Nebeling, L. Knowledge of and Adherence to Fruit and Vegetable Recommendations and Intakes: Results of the 2003 Health Information National Trends Survey. J. Health Commun. 2011, 16, 328–340. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.F.C.; Parmenter, K.; Waller, J. Nutrition knowledge and food intake. Appetite 2000, 34, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Brewer, D.; Dickens, E.; Humphrey, A.; Stephenson, T. Increased fruit and vegetable intake among older adults participating in Kentucky’s congregate meal site program. Educ. Gerontol. 2016, 42, 771–784. [Google Scholar] [CrossRef] [Green Version]
- Cannoosamy, K.; Pem, D.; Bhagwant, S.; Jeewon, R. Is a Nutrition Education Intervention Associated with a Higher Intake of Fruit and Vegetables and Improved Nutritional Knowledge among Housewives in Mauritius? Nutrients 2016, 8, 723. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.L.; Famodu, O.A.; Holásková, I.; Infante, A.M.; Murray, P.J.; Olfert, I.M.; McFadden, J.W.; Downes, M.T.; Chantler, P.D.; Duespohl, M.W.; et al. Educational intervention improves fruit and vegetable intake in young adults with metabolic syndrome components. Nutr. Res. 2019, 62, 89–100. [Google Scholar] [CrossRef]
- Hersey, J.C.; Cates, S.C.; Blitstein, J.L.; Kosa, K.M.; Rivera, O.J.S.; Contreras, D.A.; Long, V.A.; Singh, A.; Berman, D.A. Eat Smart, Live Strong Intervention Increases Fruit and Vegetable Consumption Among Low-Income Older Adults. J. Nutr. Gerontol. Geriatr. 2015, 34, 66–80. [Google Scholar] [CrossRef]
- Neville, C.E.; McKinley, M.C.; Draffin, C.R.; Gallagher, N.; Appleton, K.M.; Young, I.; Edgar, J.M.; Woodside, J.V. Participating in a fruit and vegetable intervention trial improves longer term fruit and vegetable consumption and barriers to fruit and vegetable consumption: A follow-up of the ADIT study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 158. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.G.; Rhee, Y.; Honrath, K.; Salafia, E.H.B.; Terbizan, D. Nutrition education effective in increasing fruit and vegetable consumption among overweight and obese adults. Appetite 2016, 100, 94–101. [Google Scholar] [CrossRef]
- Lara, J.; Hobbs, N.; Moynihan, P.; Meyer, T.D.; Adamson, A.J.; Errington, L.; Rochester, L.; Sniehotta, F.F.; White, M.; Mathers, J.C. Effectiveness of dietary interventions among adults of retirement age: A systematic review and meta-analysis of randomized controlled trials. BMC Med. 2014, 12, 60. [Google Scholar] [CrossRef] [Green Version]
- Parekh, N.; Jiang, J.; Buchan, M.; Meyers, M.; Gibbs, H.; Krebs, P. Nutrition Literacy among Cancer Survivors: Feasibility Results from the Healthy Eating and Living Against Breast Cancer (HEAL-BCa) Study: A Pilot Randomized Controlled Trial. J. Cancer Educ. 2017, 33, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Pem, D.; Bhagwant, S.; Jeewon, R. A Pre and Post Survey to Determine Effectiveness of a Dietitian-Based Nutrition Education Strategy on Fruit and Vegetable Intake and Energy Intake among Adults. Nutrients 2016, 8, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollard, C.M.; Miller, M.; Woodman, R.J.; Meng, X.; Binns, C. Changes in Knowledge, Beliefs, and Behaviors Related to Fruit and Vegetable Consumption among Western Australian Adults from 1995 to 2004. Am. J. Public Health 2009, 99, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, K.M.; Burton, M.; Brown, A.K.; A McNaughton, S. Exploring barriers to meeting recommendations for fruit and vegetable intake among adults in regional areas: A mixed-methods analysis of variations across socio-demographics. Appetite 2020, 153, 104750. [Google Scholar] [CrossRef] [PubMed]
- Glasson, C.; Chapman, K.; James, E. Fruit and vegetables should be targeted separately in health promotion programmes: Differences in consumption levels, barriers, knowledge and stages of readiness for change. Public Health Nutr. 2010, 14, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Rekhy, R.; McConchie, R. Promoting consumption of fruit and vegetables for better health. Have campaigns delivered on the goals? Appetite 2014, 79, 113–123. [Google Scholar] [CrossRef]
- Carter, O.B.; Pollard, C.M.; Atkins, J.F.; Milliner, J.M.; Pratt, I.S. ‘We’re not told why—we’re just told’: Qualitative reflections about the Western Australian Go for 2&5® fruit and vegetable campaign. Public Health Nutr. 2010, 14, 982–988. [Google Scholar] [CrossRef] [Green Version]
- Baker, A.H.; Wardle, J.F.C. Sex differences in fruit and vegetable intake in older adults. Appetite 2003, 40, 269–275. [Google Scholar] [CrossRef]
- Hendrie, G.; Coveney, J.D.; Cox, D. Exploring nutrition knowledge and the demographic variation in knowledge levels in an Australian community sample. Public Health Nutr. 2008, 11, 1365–1371. [Google Scholar] [CrossRef] [Green Version]
- Worsley, A.; Wang, W.C.; Byrne, S.; Yeatman, H. Different patterns of Australian adults’ knowledge of foods and nutrients related to metabolic disease risk. J. Nutr. Sci. 2014, 3, e14. [Google Scholar] [CrossRef] [Green Version]
- Vasconcelos, C.; Almeida, A.; Sá, C.; Viana, J.L.; Cabral, M.; Ramos, E.; Mendes, R. Nutrition-related knowledge and its determinants in middle-aged and older patients with type 2 diabetes. Prim. Care Diabetes 2020, 14, 119–125. [Google Scholar] [CrossRef] [PubMed]
- De Vriendt, T.; Matthys, C.; Verbeke, W.; Pynaert, I.; De Henauw, S. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behaviour. Appetite 2009, 52, 788–792. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Khoramdad, M.; Vahedian-Azimi, A.; Karimi, L.; Rahimi-Bashar, F.; Amini, H.; Sahebkar, A. Association between passive smoking and cardiovascular disease: A systematic review and meta-analysis. IUBMB Life 2020, 72, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Lamb, K.E.; Costa, C.; Cutumisu, N.; Ellaway, A.; Kamphuis, C.B.M.; Mentz, G.; Pearce, J.; Santana, P.; Santos, R.; et al. Neighbourhood socioeconomic disadvantage and fruit and vegetable consumption: A seven countries comparison. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, K.M.; Olstad, D.L.; Leech, R.M.; Ball, K.; Meertens, B.; Potter, J.; Cleanthous, X.; Reynolds, R.; McNaughton, S.A. Socioeconomic Inequities in Diet Quality and Nutrient Intakes among Australian Adults: Findings from a Nationally Representative Cross-Sectional Study. Nutrients 2017, 9, 1092. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Baseline Knowledge of Fruit and Vegetable Intake | ||||
|---|---|---|---|---|
| Total Cohort | Adequate | Insufficient | Poor | |
| n (%) | 8966 | 2085 (24.1) | 6596 (73.0) | 285 (2.9) |
| Sex (men), n (%) | 4043 (49.8) | 563 (32.6) | 3291 (54.8) | 189 (67.5) |
| Age groups, n (%) | ||||
| 25–45 years | 3127 (47.8) | 970 (60.1) | 2060 (43.7) | 97 (47.6) |
| 45–65 years | 4188 (35.7) | 930 (31.3) | 3144 (37.4) | 114 (30.4) |
| >65 years | 1651 (16.5) | 185 (8.6) | 1392 (18.9) | 74 (22.0) |
| BMI groups, n (%) | ||||
| Underweight | 85 (1.0) | 19 (1.2) | 64 (0.8) | 2 (3.5) |
| Normal | 3269 (39.4) | 864 (43.6) | 2324 (38.3) | 81 (34.0) |
| Overweight | 3621 (39.3) | 721 (35.1) | 2758 (40.6) | 142 (41.5) |
| Obese | 1991 (20.3) | 481 (20.2) | 1450 (20.3) | 60 (21.0) |
| Energy intake (MJ/day), mean ± SD | 8.8 ± 3.1 | 8.5 ± 2.9 | 8.8 ± 3.1 | 8.9 ± 3.9 |
| Physical activity, n (%) | ||||
| Sedentary | 1523 (15.8) | 269 (11.8) | 1183 (17.2) | 71 (15.2) |
| Insufficient | 2761 (32.1) | 679 (33.7) | 1997 (31.3) | 85 (38.6) |
| Sufficient | 4682 (52.1) | 1137 (54.5) | 3416 (51.5) | 129 (46.2) |
| Relationship status, n (%) | ||||
| Married | 6495 (72.6) | 1532 (70.8) | 4772 (73.5) | 191 (65.6) |
| De facto | 434 (4.5) | 115 (5.4) | 300 (4.3) | 19 (4.4) |
| Separated | 228 (2.4) | 61 (3.9) | 157 (1.8) | 10 (4.7) |
| Divorced | 534 (5.1) | 119 (5.0) | 396 (5.2) | 19 (4.7) |
| Widowed | 559 (5.3) | 82 (3.4) | 453 (5.8) | 24 (8.5) |
| Single | 716 (10.0) | 176 (11.5) | 518 (9.4) | 22 (12.1) |
| Level of education, n (%) | ||||
| Never to some high school | 3586 (35.9) | 668 (29.8) | 2773 (37.7) | 145 (40.7) |
| Completed university/equivalent | 5380 (64.1) | 1417 (70.2) | 3823 (62.3) | 140 (59.3) |
| SEIFA Disadvantage, n (%) | ||||
| Quartile 1 (least disadvantaged) | 2634 (35.1) | 695 (38.1) | 1889 (34.5) | 50 (25.8) |
| Quartile 2 | 3501 (34.3) | 860 (34.8) | 2539 (34.3) | 102 (32.0) |
| Quartile 3 | 1437 (16.1) | 283 (16.0) | 1088 (15.9) | 66 (22.0) |
| Quartile 4 (most disadvantaged) | 1394 (14.5) | 247 (11.1) | 1080 (15.4) | 67 (20.3) |
| Smoking status, n (%) | ||||
| Current | 1366 (15.7) | 207 (9.7) | 1091 (17.2) | 68 (29.1) |
| Former smoker | 2628 (25.8) | 578 (25.0) | 1951 (26.0) | 99 (29.9) |
| Non-smoker | 4972 (58.4) | 1300 (65.3) | 3554 (56.8) | 118 (41.0) |
| Self-reported CVD history, Yes, n (%) | 718 (6.8) | 89 (3.9) | 599 (7.5) | 30 (12.4) |
| Diabetes status, n (%) | ||||
| Normal glucose levels | 6620 (76.9) | 1686 (83.8) | 4745 (75.0) | 189 (67.0) |
| Known Diabetes Mellitus | 357 (3.4) | 46 (2.3) | 293 (3.6) | 18 (6.3) |
| Impaired fasting glucose | 534 (5.8) | 85 (4.2) | 423 (6.1) | 26 (10.2) |
| Impaired glucose tolerance | 1088 (10.4) | 218 (8.0) | 835 (11.2) | 35 (11.9) |
| New Diabetes Mellitus | 367 (3.5) | 50 (1.7) | 300 (4.1) | 17 (4.6) |
| Baseline Knowledge of Fruit and Vegetable Intake | |||
|---|---|---|---|
| Adequate | Insufficient | Poor | |
| FVI (grams/day) | |||
| n, (%) | 2085 (24.1) | 6596 (73.0) | 285 (2.9) |
| Unadjusted | reference | −57.5 (−73.4, −41.7) | −125.8 (−144.7, −106.9) |
| Multivariable adjusted b | reference | −67.1 (-80.0, −54.3) | −124.0 (−142.9, −105.1) |
| Fruit Intake (grams/day) | |||
| n, (%) | 3754 (42.6) | 5031 (55.6) | 181 (1.8) |
| Unadjusted | reference | −65.8 (−74.2, −57.3) | −107.1 (−130.0, −84.1) |
| Multivariable adjusted b | reference | −65.3 (−73.3, −57.3) | −96.7 (−126.9, −66.4) |
| Vegetable Intake (grams/day) | |||
| n, (%) | 2775 (32.2) | 6032 (65.9) | 159 (1.9) |
| Unadjusted | reference | −11.2 (−21.1, −1.3) | −51.9 (−68.1, −35.7) |
| Multivariable adjusted b | reference | −16.1 (−26.4, −5.8) | −58.9 (−77.6, −40.2) |
| Baseline Fruit and Vegetable Intake (grams/day) | |||
|---|---|---|---|
| Model 2 b | Coefficient | (95% CI) | |
| Baseline Knowledge Score | Adequate | reference | |
| Insufficient | −67.1 | (−80.0, −54.3) | |
| Poor | −124.0 | (142.9, 105.1) | |
| Sex | Male | reference | |
| Female | 25.7 | (19.4, 32.0) | |
| Age Groups | 25–45 years | reference | |
| 45–65 years | 59.3 | (44.9, 73.6) | |
| >65 years | 84.9 | (64.4, 105.3) | |
| BMI Groups | Normal | reference | |
| Underweight | −36.6 | (−92.2, 18.9) | |
| Overweight | 1.6 | (−10.5, 13.7) | |
| Obese | 8.7 | (−14.0, 31.4) | |
| Energy Intake | (megajoules/day) | 17.8 | (16.0, 19.5) |
| Physical Activity Level | Sedentary | reference | |
| Insufficient | 2.5 | (−17.6, 22.5) | |
| Sufficient | 33.4 | (19.4, 47.4) | |
| Marital Status | Married | reference | |
| De facto | −14.5 | (−34.7, 5.7) | |
| Separated | −16.6 | (−53.8, 20.5) | |
| Divorced | −16.1 | (−42.2, 9.9) | |
| Widowed | −11.1 | (−45.4, 23.2) | |
| Single | −2.3 | (−20.8, 16.2) | |
| Education Level | Never to some high school | reference | |
| University or equivalent | −7.9 | (−17.4, 1.6) | |
| SEIFA Disadvantage | Quartile 1 (least) | reference | |
| Quartile 2 | 0.1 | (−16.3, 16.4) | |
| Quartile 3 | 8.3 | (−15.4, 31.9) | |
| Quartile 4 (most) | 10.9 | (−19.2, 41.0) | |
| Smoking Status | Current smoker | reference | |
| Former smoker | 59.1 | (38.7, 79.5) | |
| Non-smoker | 65.3 | (45.1, 85.5) | |
| Self-reported history of CVD | Yes | reference | |
| No | −18.2 | (−39.1, 2.7) | |
| Diabetes Status | Normal glucose levels | reference | |
| Known Diabetes Mellitus | 35.6 | (6.4, 64.7) | |
| New Diabetes Mellitus | −5.3 | (−44.0, 33.5) | |
| Impaired fasting glucose | 1.2 | (−22.5, 24.9) | |
| Impaired glucose tolerance | −10.5 | (−33.8, 12.8) | |
| Baseline Knowledge of Fruit and Vegetable Intake | |||
|---|---|---|---|
| Adequate | Insufficient | Poor | |
| FVI (grams/day): 5 years | |||
| n, (%) | 1298 (24.9) | 3775 (72.5) | 131 (2.5) |
| Unadjusted | reference | −45.2 (−56.1, −34.3) | −128.2 (−159.3, −97.1) |
| Multivariable adjusted b | reference | −50.4 (−61.4, −39.4) | −122.2 (−152.7, −91.6) |
| FVI (grams/day): 12 years | |||
| n, (%) | 1022 (28.8) | 2457 (69.2) | 70 (2.0) |
| Unadjusted | reference | −37.5 (−49.5, −25.6) | −92.0 (−131.7, −52.4) |
| Multivariable adjusted b | reference | −42.5 (−54.6, −30.5) | −94.6 (−133.8, −55.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hill, C.R.; Blekkenhorst, L.C.; Radavelli-Bagatini, S.; Sim, M.; Woodman, R.J.; Devine, A.; Shaw, J.E.; Hodgson, J.M.; Daly, R.M.; Lewis, J.R. Fruit and Vegetable Knowledge and Intake within an Australian Population: The AusDiab Study. Nutrients 2020, 12, 3628. https://doi.org/10.3390/nu12123628
Hill CR, Blekkenhorst LC, Radavelli-Bagatini S, Sim M, Woodman RJ, Devine A, Shaw JE, Hodgson JM, Daly RM, Lewis JR. Fruit and Vegetable Knowledge and Intake within an Australian Population: The AusDiab Study. Nutrients. 2020; 12(12):3628. https://doi.org/10.3390/nu12123628
Chicago/Turabian StyleHill, Caroline R., Lauren C. Blekkenhorst, Simone Radavelli-Bagatini, Marc Sim, Richard J. Woodman, Amanda Devine, Jonathan E. Shaw, Jonathan M. Hodgson, Robin M. Daly, and Joshua R. Lewis. 2020. "Fruit and Vegetable Knowledge and Intake within an Australian Population: The AusDiab Study" Nutrients 12, no. 12: 3628. https://doi.org/10.3390/nu12123628