The Use of Implementation Intentions to Promote Vitamin D Supplementation in Young Children

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Procedures
2.2. Questionnaires
2.3. Statistical Analyses
3. Results
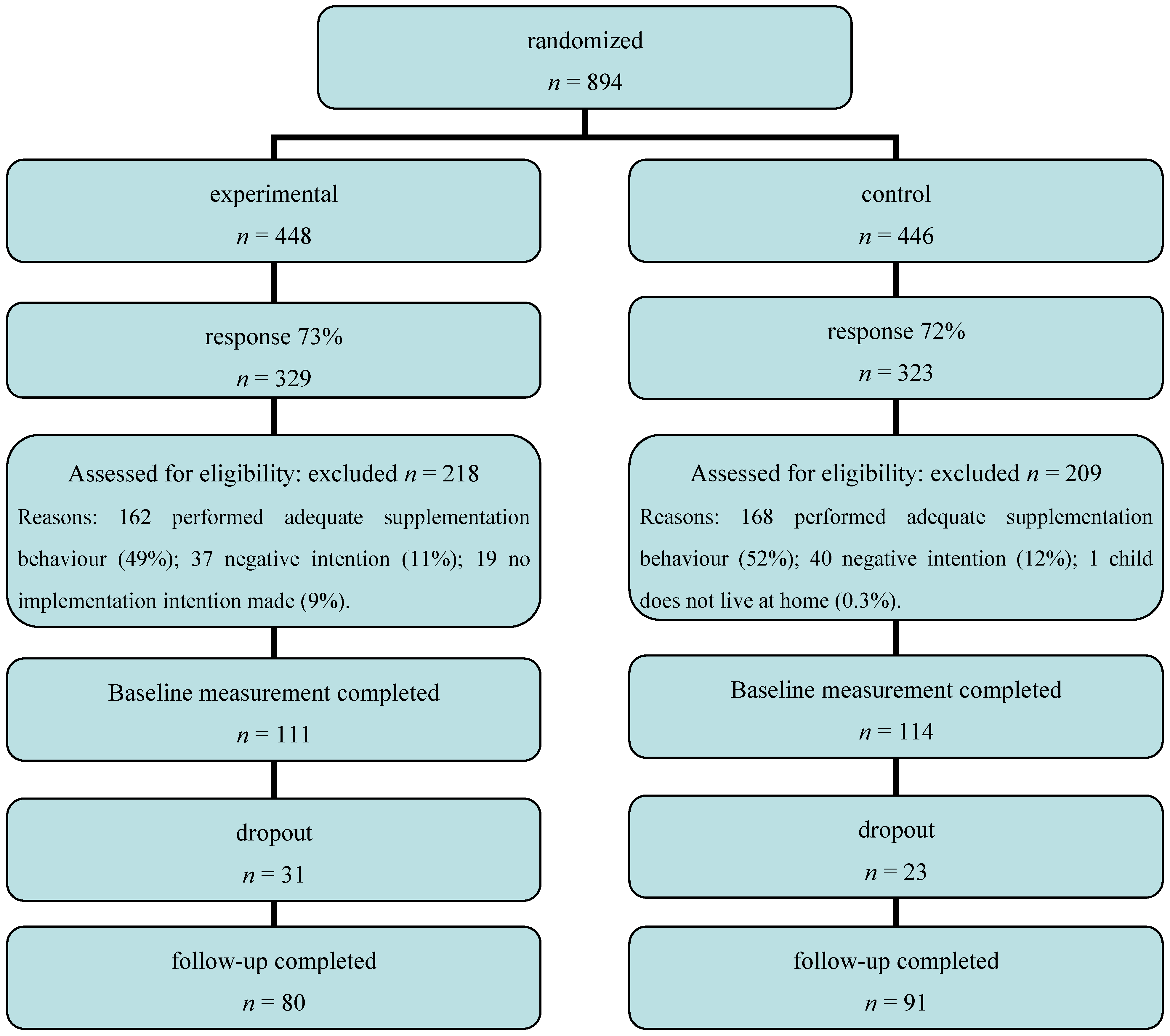
3.1. Response, Dropouts and Participants


{kind=link}
| Characteristic | % or Mean ± S.D. |
|---|---|
| Participant sex (female/male) | 78/22 |
| Participant age (years) | 34.1 ± 4.4 |
| Participant education level (low/med/high) | 4/36/60 |
| Child sex (girl/boy) | 54/46 |
| Child age (years) | 2.3 ± 0.8 |
| First-born child (yes/no) | 40/60 |
| Child ethnicity (autochthonous/allochthonous) | 91/9 |
| Intention to give vitamin D (0–2) | 1.2 ± 0.6 |
| Number of days child received vitamin D (1–5) | 2.02 ± 2.0 |
| Vitamin D at home (yes/no) | 81/19 |
3.2. Supplementation-Related Behaviour at Baseline
3.3. Effects of Implementation Intentions
| Baseline | Follow-up | |||
|---|---|---|---|---|
| Experimental group | Control group | Experimental group | Control group | |
| Number of parents performing adequate supplementation behaviour | - * | - * | 29 (36%) | 25 (27%) |
| Mean number of days parents gave vitamin D supplementation to their child ± S.D. | 2.0 ± 2.0 | 2.0 ± 2.1 | 4.1 ± 2.5 | 3.5 ± 2.7 |
| Number of parents with vitamin D supplements at home | 67 (84%) | 72 (79%) | 75 (94%) | 76 (84%) |
3.4. Evaluation by Participants
4. Discussion
5. Conclusions
Conflict of Interest
References
- Health Council of the Netherlands, Towards an Adequate Intake of Vitamin D; Health Council of the Netherlands: The Hague, The Netherlands, 2008.
- Cashman, K.D. Vitamin D in childhood and adolescence. Postgrad. Med. J. 2007, 83, 230–235. [Google Scholar] [CrossRef]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678–1688. [Google Scholar]
- De Nooijer, J.; Onninck, M.; van Assema, P. Vitamin D supplementation in young children: Associations with Theory of Planned Behaviour variables, descriptive norms, moral norms and habits. Public Health Nutr. 2010, 13, 1279–1285. [Google Scholar] [CrossRef]
- Van der Linden-Kuiper, A.T.; Bunge-van Lent, F.C.G.M.; Boere-Boonekamp, M.M. Recommended vitamin D suppletion for toddlers often omitted. Ned. Tijdschr. Geneeskund. 1999, 143, 2146–2150. [Google Scholar]
- Gollwitzer, P.M. Goal achievement: The role of intentions. Eur. Rev. Soc. Psychol. 1993, 4, 141–185. [Google Scholar] [CrossRef]
- Gollwitzer, P.M. Implementation intentions. Strong effects of simple plans. Am. Psychol. 1999, 54, 493–503. [Google Scholar] [CrossRef]
- Gollwitzer, P.M.; Brandstätter, V. Implementation intentions and effective goal pursuit. J. Pers. Soc. Psychol. 1997, 73, 186–199. [Google Scholar] [CrossRef]
- Bargh, J.A.; Gollwitzer, P.M. Environmental control of goal-directed action: Automatic and strategic contingencies between situations and behavior. Neb. Symp. Motiv. 1994, 41, 71–124. [Google Scholar]
- Orbell, S.; Hodgkins, S.; Sheeran, P. Implementation intentions and the theory of planned behavior. Pers. Soc. Psychol. Bull. 1997, 23, 945–954. [Google Scholar] [CrossRef]
- Gollwitzer, P.M.; Sheeran, P. Implementation intentions and goal achievement: A meta-analysis of effects and processes. Adv. Exp. Soc. Psychol. 2006, 38, 69–119. [Google Scholar] [CrossRef]
- De Nooijer, J.; de Vet, E.; Brug, J.; de Vries, N.K. Do implementation intentions help to turn good intentions into higher fruit intake? J. Nutr. Educ. Behav. 2006, 38, 25–29. [Google Scholar] [CrossRef]
- Sheeran, P.; Orbell, S. Implementation intentions and repeated behaviour: Augmenting the predictive validity of the theory of planned behaviour. Eur. J. Soc. Psychol. 1999, 29, 349–369. [Google Scholar] [CrossRef]
- Van Osch, L.; Reubsaet, A.; Lechner, L.; de Vries, H. The formation of specific action plans can enhance sun protection behavior in motivated parents. Prev. Med. 2008, 47, 127–132. [Google Scholar] [CrossRef]
- Jansen, R.J.B. The development and evaluation of a strategy to promote vitamine D intake among 0-4 years old. Bachelor’s Thesis, Maastricht University, Maastricht, The Netherlands, 2009. [Google Scholar]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. Br. Med. J. 2000, 321, 694–696. [Google Scholar] [CrossRef]
- De Vet, E.; Oenema, A.; Sheeran, P.; Brug, J. Should implementation intentions interventions be implemented in obesity prevention: The impact of if-then plans on daily physical activity in Dutch adults. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 11. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
De Nooijer, J.; Jansen, R.; Van Assema, P. The Use of Implementation Intentions to Promote Vitamin D Supplementation in Young Children. Nutrients 2012, 4, 1454-1463. https://doi.org/10.3390/nu4101454
De Nooijer J, Jansen R, Van Assema P. The Use of Implementation Intentions to Promote Vitamin D Supplementation in Young Children. Nutrients. 2012; 4(10):1454-1463. https://doi.org/10.3390/nu4101454
Chicago/Turabian StyleDe Nooijer, Jascha, Roos Jansen, and Patricia Van Assema. 2012. "The Use of Implementation Intentions to Promote Vitamin D Supplementation in Young Children" Nutrients 4, no. 10: 1454-1463. https://doi.org/10.3390/nu4101454