Maternal Zinc Intakes and Homeostatic Adjustments during Pregnancy and Lactation

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Zinc Homeostasis during Pregnancy


- • Plasma zinc declines during pregnancy with a larger decline seen in women with habitual intakes ≤9 mg/day.
- • Renal zinc conservation increases among women with low intakes, ≤9 mg/day, but the net increase in zinc retention is very small (≤0.3 mg/day).
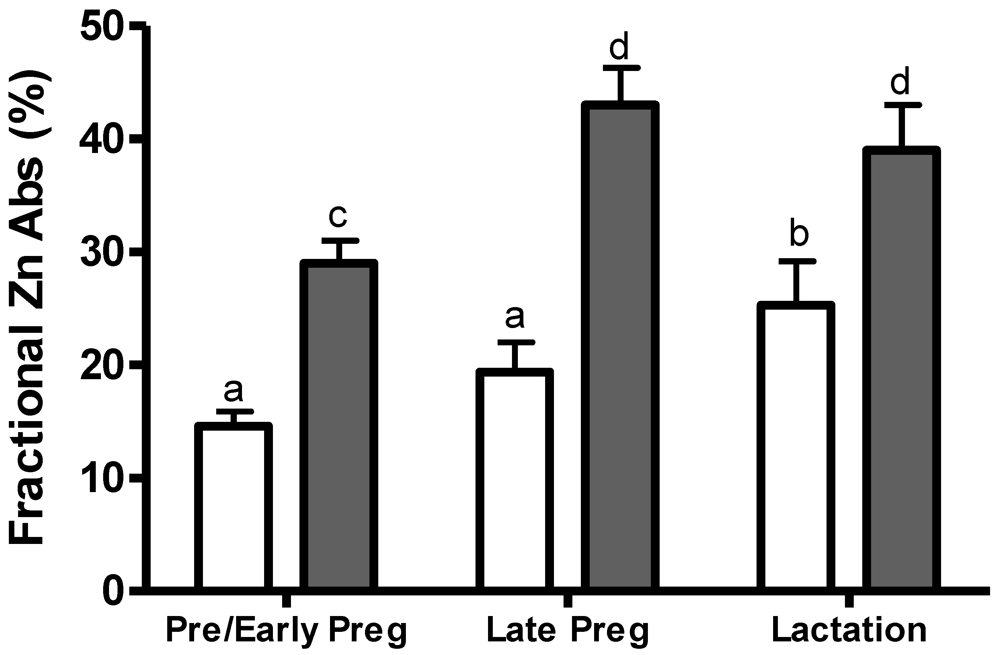
- • Fractional zinc absorption appears to increase when the maternal zinc intake falls below 9 mg/day, but the net increase in absorbed zinc does not appear to be sufficient to meet the increased zinc needs for pregnancy when dietary zinc is very low (≤6 mg/day).
- • Endogenous fecal zinc losses have not been measured in human pregnancy, thus it is not known if these losses vary with dietary zinc.
- • Preliminary kinetic data suggest that the flux of zinc from the exchangeable zinc pools to other tissues may increase in pregnancy.
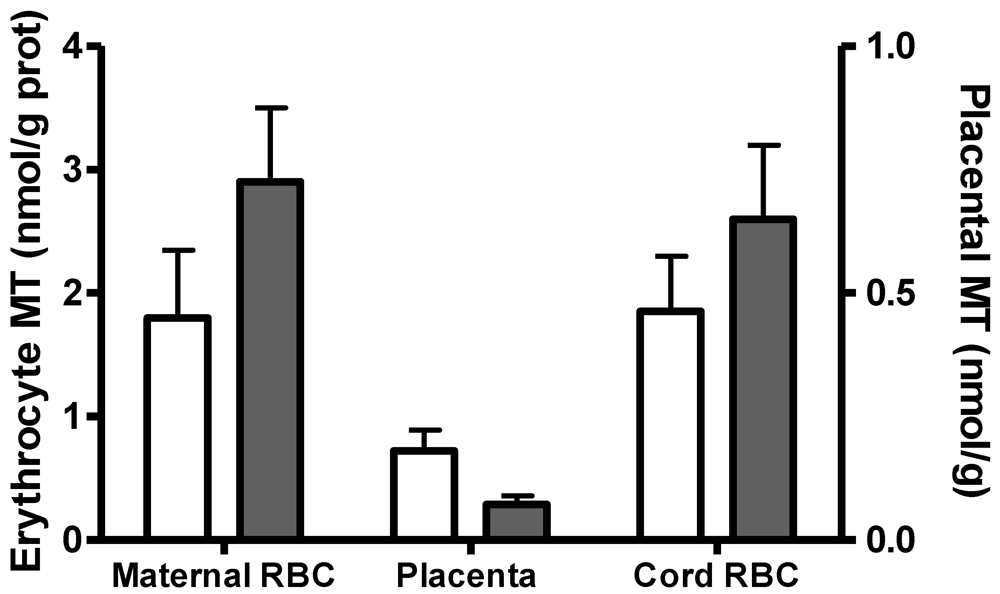
- • The regulatory role of zinc transporter proteins and metallothioneins in the placental zinc transfer needs further investigation.
3. Zinc Homeostasis during Lactation
- • Milk zinc concentration and milk zinc output declines about 75% over the lactation period irrespective of maternal zinc intake.
- • Limited evidence suggests that milk zinc concentration is reduced with low zinc intakes.
- • Renal zinc conservation occurs during lactation, largely independent of maternal zinc intake, but the net effect on zinc conservation is small.
- • The efficiency of zinc absorption increases during lactation. The net change is further enhanced with low zinc diets (≤8 mg/day) or when maternal zinc status is marginal. Endogenous fecal zinc excretion may also decline among lactating women with low zinc intakes.
- • The effect of low maternal zinc intakes on zinc kinetics and the regulation of mammary gland zinc uptake and secretion are unknown.
4. Other Research Implications
Conflict of Interest
References
- MacDonald, R.S. The role of zinc in growth and cell proliferation. J. Nutr. 2000, 130, 1500–1508. [Google Scholar]
- Cousins, R. Zinc. In Present Knowledge in Nutrition, 9th; Bowman, B.A., Rusell, R.M., Eds.; International Life Sciences Institute: Washington, DC, USA, 2006. [Google Scholar]
- Maret, W. Molecular aspects of human cellular zinc homeostasis: Redox control of zinc potentials and zinc signals. Biometals 2009, 22, 149–157. [Google Scholar] [CrossRef]
- King, J.C. Determinants of maternal zinc status during pregnancy. Am. J. Clin. Nutr. 2000, 71, 133–143. [Google Scholar]
- Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lönnerdal, B.; Ruel, M.T.; Sandtröm, B.; Wasantwisut, E.; Hotz, C. IZiNCG. International Zinc Nutrition Consultative Group (IZiNCG) Technical Document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar]
- Caulfield, L.E.; Zavaleta, N.; Shanker, A.H.; Merialdi, M. Potential contribution of maternal zinc supplementation during pregnancy to maternal and child survival. Am. J. Clin. Nutr. 1998, 68, 499–508. [Google Scholar]
- Tamura, T.; Goldenberg, R.L. Zinc nutriture and pregnancy outcome. Nutr. Res. 1996, 16, 139–181. [Google Scholar] [CrossRef]
- Shah, D.; Sachdev, H.P.S. Effect of gestational zinc deficiency on pregnancy outcomes: Summary of observation studies and zinc supplementation trials. Br. J. Nutr. 2001, 85, S101–S108. [Google Scholar] [CrossRef]
- Tamura, T.; Goldenberg, R.L.; Johnston, K.E.; DuBard, M. Maternal plasma zinc concentrations and pregnancy outcome. Am. J. Clin. Nutr. 2000, 71, 109–113. [Google Scholar]
- Rwebembera, A.A.; Munubhi, E.K.; Manji, K.P.; Mpembeni, R.; Philip, J. Relationship between infant birth weight ≤2000 g and maternal zinc levels at Muhimbili National Hospital, Dar Es Salaam, Tanzania. J. Trop. Pediatr. 2006, 52, 118–125. [Google Scholar]
- Lee, Y.A.; Hwang, J.Y.; Kim, H.; Ha, E.H.; Park, H.; Ha, M.; Kim, Y.; Hong, Y.C.; Chang, N. Relationships of maternal zinc intake from animal foods with fetal growth. Br. J.Nutr. 2011, 22, 1–7. [Google Scholar]
- Badakhsh, M.H.; Khamseh, S.E.; Seifoddin, M.; Kashanian, M.; Malek, M.; Shafiee, G.; Baradaran, H.R. Impact of maternal zinc status on fetal growth in an Iranian pregnant population. Gynecol. Endocrinol. 2011, 27, 1074–1076. [Google Scholar] [CrossRef]
- sendarp, S.J.M.; West, C.E.; Black, R.E. The need for maternal zinc supplementation in developing countries: An unresolved issue. J. Nutr. 2003, 133, 817–827. [Google Scholar]
- Castillo-Durán, C.; Weisstaub, G. Zinc supplementation and growth of the fetus and low birth weight infant. J. Nutr. 2003, 133, 1494–1497. [Google Scholar]
- Mahomed, K.; Bhutta, Z.; Middleton, P. Zinc supplementation for improving pregnancy and infant outcome. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- Hess, S.Y.; King, J.C. Effects of maternal zinc supplementation on pregnancy and lactation outcomes. Food Nutr. Bull. 2009, 30, S60–S78. [Google Scholar]
- Gebreselassie, S.G.; Gashe, F.E. A systematic review of effect of prenatal zinc supplementation in birthweight: Meta-analysis of 17 randomized controlled trials. J. Health Popul. Nutr. 2011, 29, 134–140. [Google Scholar]
- Chaffee, B.J.; King, J.C. Effect of zinc supplementation on pregnancy and infant outcomes: A systematic review. Paediatr. Perinat. Epidemiol. 2012, 26, 118–137. [Google Scholar] [CrossRef]
- Garg, H.K.; Singhal, K.C.; Arshad, Z. A study of the effect of oral zinc supplementation during pregnancy on pregnancy outcome. Indian J. Physiol. Pharmacol. 1993, 37, 276–284. [Google Scholar]
- Xie, L.M.; Chen, X.; Pan, J. The effects of zinc supplementation to Chinese rural pregnant women and their pregnancy outcome. J. Shanghai Sec. Med. Univ. 2001, 13, 199–124. [Google Scholar]
- Goldenberg, R.L.; Tamura, T.; Neggers, Y.; Copper, R.L.; Johnston, K.E.; Dubard, M.B.; Hauth, J.C. The effect of zinc supplementation on pregnancy outcome. J. Am. Med. Assoc. 1995, 274, 463–468. [Google Scholar]
- sendarp, S.J.M.; van Raaij, J.M.A.; Arifeen, S.E.; Wahed, M.A.; Baqui, A.H.; Fuchs, G.J. A randomized, placebo-controlled trial of the effect of zinc supplementation during pregnancy on pregnancy outcome in Bangladesh urban poor. Am. J. Clin. Nutr. 2000, 71, 114–119. [Google Scholar]
- Swanson, C.A.; King, J.C. Zinc and pregnancy outcome. Am. J. Clin. Nutr. 1987, 46, 763–771. [Google Scholar]
- 24. National Academy of Sciences, Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenci, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academic Press: Washington, DC, USA, 2001.
- Swanson, C.A.; King, J.C. Reduced serum zinc concentration during pregnancy. Obstet. Gynecol. 1983, 62, 313–318. [Google Scholar] [CrossRef]
- Caulfield, L.E.; Zavaleta, N.; Figueroa, A. Adding zinc to prenatal iron and folate supplements improves maternal and neonatal zinc status in a Peruvian population. Am. J. Clin. Nutr. 1999, 69, 1257–1263. [Google Scholar]
- Hambidge, K.M.; Krebs, N.F.; Jacobs, M.A.; Favier, A.; Guyette, L.; Ikle, D.N. Zinc nutritional status during pregnancy: A longitudinal study. Am. J. Clin. Nutr. 1983, 37, 429–442. [Google Scholar]
- Moser, P.B.; Reynolds, R.D. Dietary zinc intake and zinc concentrations of plasma, erythrocytes, and breast milk in antepartum and postpartum lactating and nonlactating women: A longitudinal study. Am. J. Clin. Nutr. 1983, 38, 101–108. [Google Scholar]
- Qvist, I.; Abdulla, M.; Jagerstad, M.; Svensson, S. Iron, zinc, and folate status during pregnancy and two months after delivery. Acta Obstet. Gynecol. Scand. 1986, 65, 15–22. [Google Scholar]
- Fung, E.B.; Ritchie, L.D.; Woodhouse, L.R.; Roehl, R.; King, J.C. Zinc absorption in women during pregnancy and lactation: A longitudinal study. Am. J. Clin. Nutr. 1997, 66, 80–88. [Google Scholar]
- Donangelo, C.M.; Vargas-Zapata, C.L.; Woodhouse, L.R.; Shames, D.M.; Mukherjea, R.; King, J.C. Zinc absorption and kinetics during pregnancy and lactation in Brazilian women. Am. J. Clin. Nutr. 2005, 82, 118–124. [Google Scholar]
- King, J.C. Physiology of pregnancy and nutrient metabolism. Am. J. Clin. Nutr. 2000, 71, 1218–1225. [Google Scholar]
- Caulfield, L.E.; Donangelo, C.M.; Chen, P.; Junco, J.; Merialdi, M.; Zavaleta, N. Red blood cell metallothionein as an indicator of zinc status during pregnancy. Nutrition 2008, 24, 1081–1087. [Google Scholar] [CrossRef]
- Vargas-Zapata, C.V.; Simões, T.M.R.; Donangelo, C.M. Erythrocyte metallothionein in relation to other biochemical zinc indices in pregnant and non-pregnant women. Biol. Trace Elem. Res. 1997, 57, 115–124. [Google Scholar] [CrossRef]
- Giroux, E.; Schechter, P.J.; Schoun, J. Diminished albumin binding of zinc in serum of pregnant women. Clin. Sci. Mol. Med. 1976, 51, 545–549. [Google Scholar]
- Davis, S.R.; Cousins, R. Metallothionein expression in animals: A physiological perspective on function. J. Nutr. 2000, 130, 1085–1088. [Google Scholar]
- Maret, W. The function of zinc metallothionein: A link between cellular zinc and redox state. J. Nutr. 2000, 130, 1455–1458. [Google Scholar]
- Zapata, C.L.; Melo, M.R.; Donangelo, C.M. Maternal, placental and cord zinc components in healthy women with different levels of serum zinc. Biol. Neonate 1997, 72, 84–93. [Google Scholar] [CrossRef]
- Mas, A.; Sarkar, B. Binding, uptake and efflux of 65Zn by isoaltaed human thophoblast cells. Biochim. Biophys. Acta 1092, 35–38. [Google Scholar]
- Aslam, N.; McArdle, H.J. Mechanism of zinc uptake by microvilli isolated from human term placenta. J. Cell. Physiol. 1992, 151, 533–538. [Google Scholar] [CrossRef]
- Vargas Zapata, C.L.; Trugo, N.M.F.; Donangelo, C.M. Zinc uptake by human placental microvillous membrane vesicles: Effect of gestational age and maternal serum zinc levels. Biol. Trace Elem. Res. 2000, 73, 127–137. [Google Scholar] [CrossRef]
- Liuzzi, J.P.; Bobo, J.A.; Cui, L.; McMahon, R.J.; Cousins, R.J. Zinc transporters 1, 2 and 4 are differentially expressed and localized in rats during pregnancy and lactation. J. Nutr. 2003, 133, 342–351. [Google Scholar]
- Speich, M.; Bousquet, B.; Auget, J.L.; Gelot, S.; Laborde, O. Association between magnesium, calcium, phosphorous, copper, and zinc in umbilical cord plasma and erythrocytes, and the gestational age and growth variables of full-term newborns. Clin. Chem. 1992, 38, 141–143. [Google Scholar]
- Caulfield, L.E.; Zavaleta, N.; Figueroa, A.; Leon, Z. Maternal zinc supplementation does not affect size at birth or pregnancy duration in Peru. J. Nutr. 1999, 129, 1563–1568. [Google Scholar]
- Ianotti, L.L.; Zavaleta, N.; León, Z.; Shankar, A.H.; Caulfield, L.E. Maternal zinc supplementation and growth in Peruvian infants. Am. J. Clin. Nutr. 2008, 88, 154–160. [Google Scholar]
- Caulfield, L.E.; Putnick, D.L.; Zavaleta, N.; Lazarte, F.; Albornoz, C.; Chen, P.; DiPietro, J.A. Maternal gestational supplementation does not influence multiple aspects of child development at 54 mo of age in Peru. Am. J. Clin. Nutr. 2010, 92, 130–136. [Google Scholar] [CrossRef]
- Licheten, L.A.; Cousins, R.J. Mammalian zinc transporters: Nutritional and physiologic regulation. Ann. Rev. Nutr. 2009, 29, 153–176. [Google Scholar] [CrossRef]
- Helston, R.M.; Phillips, S.R.; McKay, J.A.; Jackson, K.A.; Mathers, J.C.; Ford, D. Zinc transporters in the mouse placenta show a coordinated regulatory response to changes in dietary zinc intake. Placenta 2007, 28, 437–444. [Google Scholar] [CrossRef]
- Asano, N.; Kondoh, M.; Ebihara, C.; Fujii, M.; Nakanishi, T.; Utoguchi, N.; Enomoto, S.; Tanaka, K.; Watanabe, Y. Induction of zinc transporters by forskolin in human trophoblast BeWo cells. Reprod. Toxicol. 2006, 21, 285–291. [Google Scholar] [CrossRef]
- Waalkes, M.P.; Poisner, A.M.; Wood, G.W.; Klassen, C.D. Metallothionein-like proteins in human placenta and fetal membranes. Toxicol. Appl. Pharmacol. 1984, 74, 179–184. [Google Scholar] [CrossRef]
- Goyer, R.A.; Haus, M.D.; Cherian, M.G. Cellular localization of metallothionein in human term placenta. Placenta 1992, 13, 349–355. [Google Scholar] [CrossRef]
- Ronco, A.M.; Garrido, F.; Llanos, M.N. Smoking specifically induces metallothionein-2 isoform in human placenta at term. Toxicology 2006, 223, 46–53. [Google Scholar] [CrossRef]
- Sorkun, H.C.; Bir, F.; Akbulut, M.; Divrikli, U.; Erken, G.; Demirhan, H.; Duzcan, E.; Elci, L.; Celik, I.; Yozgati, U. The effects of air pollution and smoking on placental cadmium, zinc concentration and metallothionein expression. Toxicology 2007, 238, 15–22. [Google Scholar] [CrossRef]
- Swanson, C.A.; King, J.C. Zinc utilization in pregnant and nonpregnant women fed controlled diets providing the zinc RDA. J. Nutr. 1982, 112, 697–707. [Google Scholar]
- O’Brien, K.O.; Zavaleta, N.; Caulfield, L.E.; Wen, J.; Abrams, S.A. Prenatal iron supplements impair zinc absorption in pregnant Peruvian women. J. Nutr. 2000, 130, 2251–2255. [Google Scholar]
- Hambidge, K.M.; Abebe, Y.; Gibson, R.S.; Westcott, J.E.; Miller, L.V.; Lei, S.; Stoecker, B.J.; Arbide, I.; Teshome, A.; Bailey, K.B.; et al. Zinc absorption during late pregnancy in rural southern Ethiopia. Am. J. Clin. Nutr. 2006, 84, 1102–1106. [Google Scholar]
- Krebs, N. Zinc supplementation during lactation. Am. J. Clin. Nutr. 1998, 68, 509–512. [Google Scholar]
- Moser-Veillon, P.B. Zinc needs and homeostasis during lactation. Analyst 1995, 120, 895–897. [Google Scholar] [CrossRef]
- Kalkwarf, H.J. Lactation and maternal bone health. Adv. Exp. Med. Biol. 2004, 554, 101–114. [Google Scholar]
- Krebs, N. Zinc transfer to the breastfed infant. J. Mammary Gland Biol. Neoplasia 1999, 4, 259–268. [Google Scholar] [CrossRef]
- Krebs, N.F.; Reidinger, C.J.; Hartley, S.; Robertson, A.D.; Hambidge, K.M. Zinc supplementation during lactation: Effects on maternal status and milk zinc concentrations. Am. J. Clin. Nutr. 1995, 61, 1030–1036. [Google Scholar]
- Beshgetoor, D.; Lönnerdal, B. Identification of an α2-macroglobulin receptor in human mammary epithelial cells. J. Nutr. 1999, 129, 152–157. [Google Scholar]
- Lönnerdal, B. Trace element transport in the mammary gland. Annu. Rev. Nutr. 2007, 27, 165–177. [Google Scholar] [CrossRef]
- Kelleher, S.L.; Lopez, V.; Lönnerdal, B.; Dufner-Beattie, J.; Andrews, G.K. Zip3 (Slc39a3) functions in zinc reuptake from the alveolar lumen in lactating mammary gland. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R194–R201. [Google Scholar] [CrossRef]
- Moser-Veillon, P.B.; Reynolds, R.D. A longitudinal study of pyrydoxin and zinc supplementation of lactating women. Am. J. Clin. Nutr. 1990, 52, 135–141. [Google Scholar]
- Karra, M.V.; Kirksey, A.; Galal, O.; Bassily, N.S.; Harrisson, G.G.; Jerome, N.W. Zinc, calcium, and magnesium concentrations in milk from American and Egyptian women throughout the first 6 months of lactation. Am. J. Clin. Nutr. 1988, 47, 642–648. [Google Scholar]
- Lamounier, J.A.; Danelluzzi, J.C.; Vannucchi, H. Zinc concentration in human milk during lactation: A 6-month longitudinal study in southern Brazil. J. Trop. Pediatr. 1989, 35, 31–34. [Google Scholar]
- Salmenpera, L.; Perheentupa, J.; Nanto, V.; Siimes, M.A. Low zinc intake during exclusive breast-feeding does not impair growth. J. Pediatr. Gastroenterol. Nutr. 1994, 18, 361–370. [Google Scholar] [CrossRef]
- Bates, C.J.; Tsuchiya, H. Zinc in breast milk during prolonged lactation: Comparison between the UK and The Gambia. Eur. J. Clin. Nutr. 1990, 44, 61–69. [Google Scholar]
- Arnaud, J.; Prual, A.; Preziosi, P.; Cherouvrier, F.; Favier, A.; Galan, P.; Hercberg, S. Effect of iron supplementation during pregnancy on trace elements (Cu, Se, Zn) concentration in serum and breast milk from Nigerian women. Ann. Nutr. Metab. 1993, 37, 262–271. [Google Scholar] [CrossRef]
- Sazawal, S.; Jlla, S.; Dhingra, P.; Krebs, N.; Black, R.E.; Bhan, M.K. Impact of zinc supplementation on breast milk zinc levels among low socioeconomic Indian women. FASEB J. 1996, 10, A554. [Google Scholar]
- Domellöf, M.; Lönnerdal, B.; Dewey, K.G.; Cohen, R.J.; Hernell, O. Iron, zinc, and copper concentrations in breast milk are independent of maternal mineral status. Am. J. Clin. Nutr. 2004, 79, 111–115. [Google Scholar]
- Dempsey, C.; McCormick, N.H.; Croxford, T.P.; Seo, Y.A.; Grider, A.; Kelleher, S.L. Marginal maternal zinc deficiency in lactating ,ice reduces secretory capacity and alters milk composition. J. Nutr. 2012, 655–660. [Google Scholar]
- Krebs, N.F.; Hambidge, K.M.; Jacobs, M.A.; Rasbach, J.O. The effects of a dietary zinc supplement during lactation on longitudinal changes in maternal zinc status and milk concentrations. Am. J. Clin. Nutr. 1985, 41, 560–570. [Google Scholar]
- Moser, P.B.; Reynolds, R.D.; Acharya, S.; Howard, M.P.; Andon, M.B.; Lewis, S.A. Copper, iron, zinc, and selenium dietary intake and status in Nepalese lactating women and their breast-fed infant. Am. J. Clin. Nutr. 1988, 47, 729–734. [Google Scholar]
- Donangelo, C.M.; Trugo, N.M.F.; Koury, J.C.; Barreto Silva, M.I.; Freitas, L.A.; Feldheim, W.; Barth, C. Iron, zinc, folate and vitamin B12 nutritional status and milk composition of low income Brazilian mother. Eur. J. Clin. Nutr. 1989, 43, 253–266. [Google Scholar]
- Kelleher, S.L.; Lönnerdal, B. Long-term marginal intakes of zinc and retinol affect retinol homeostasis without compromising circulating levels during lactation in rats. J. Nutr. 2001, 131, 3237–3242. [Google Scholar]
- Klein, C.J.; Moser-Veillon, P.B.; Douglass, L.W.; Ruben, K.A.; Trocki, O. A longitudinal study of urinary calcium, magnesium, and zinc excretion in lactating and nonlactating postpartum women. Am. J. Clin. Nutr. 1995, 61, 779–786. [Google Scholar]
- Jackson, M.J.; Giugliano, R.; Giugliano, L.G.; Oliveira, E.F.; Shrimpton, R.; Swainbank, I.G. Stable isotope metabolic studies of zinc nutrition in slum-dwelling lactating women in the Amazon valley. Br. J. Nutr. 1988, 59, 193–203. [Google Scholar] [CrossRef]
- Sian, L.; Krebs, N.F.; Westcott, J.E.; Fengliang, L.; Tong, L.; Mileer, L.V.; Sonko, B.; Hambidge, M. Zinc homeostasis during lactation in a population with a low zinc intake. Am. J. Clin. Nutr. 2002, 75, 99–103. [Google Scholar]
- Moser-Veillon, P.B.; Patterson, K.Y.; Veillon, C. Zinc absorption is enhanced during lactation. FASEB J. 1995, 9, A729. [Google Scholar]
- Davies, N.T. Studies on the absorption of zinc by rat intestine. Br. J. Nutr. 1980, 43, 189–203. [Google Scholar] [CrossRef]
- Ortega, R.M.; Andrés, P.; Martínez, R.M.; López-Sobaler, A.M.; Quintas, M.E. Zinc levels in maternal milk: The influence of nutritional status with respect to zinc during the third trimester of pregnancy. Eur. J. Clin. Nutr. 1997, 51, 253–258. [Google Scholar]
- Allen, L.S. Multiple micronutrients in pregnancy and lactation: An overview. Am. J. Clin. Nutr. 2005, 81, 1206–1212. [Google Scholar]
- Prentice, A. Vitamin D deficiency: A global perspective. Nutr. Rev. 2008, 66, S153–S163. [Google Scholar] [CrossRef]
- Chung, C.S.; Nagey, D.A.; Veillon, C.; Patterson, K.Y.; Jackson, R.T.; Moser-Veillon, P.B. A single 60-mg iron dose decreases zinc absorption in lactating women. J. Nutr. 2002, 132, 1903–1905. [Google Scholar]
- Tomkins, A. Nutrition and maternal morbidity and mortality. Br. J. Nutr. 2001, 85, S93–S99. [Google Scholar] [CrossRef]
- Wellinghausen, N. Immunobiology of gestational zinc deficiency. Br. J. Nutr. 2001, 85, S81–S86. [Google Scholar] [CrossRef]
- Gibson, R.S.; Abebe, Y.; Stabler, S.; Allen, R.H.; Westcott, J.E.; Stoecker, B.J.; Krebs, N.F.; Hambidge, M. Zinc, gravida, infection, and iron, but not vitamin B-12 or folate status, predict hemoglobin during pregnancy in Southern Ethiopia. J. Nutr. 2008, 138, 581–586. [Google Scholar]
- Mohamed, A.A.; Ali, A.A.; Ali, N.I.; Abusalama, E.H.; Elbashir, M.I.; Adam, I. Zinc, parity, infection, and severe anemia among pregnant women in Kassla, eastern Sudan. Biol. Trace Elem. Res. 2011, 140, 284–290. [Google Scholar] [CrossRef]
- Rink, L.; Gabriel, P. Zinc and the immune system. Proc. Nutr. Soc. 2000, 59, 541–552. [Google Scholar] [CrossRef]
- Valde-Ramos, R. Zinc: A perinatal point of view. Prog. Food Nutr. Sci. 1992, 16, 279–306. [Google Scholar]
- Lönnerdal, B.; Zavaleta, N.; Kusunoki, L.; Lanata, C.F.; Peerson, J.M.; Brown, K.H. Effect of postpartum maternal infection in proteins and trace elements in colostrum and early milk. Acta Paediatr. 1996, 85, 537–542. [Google Scholar] [CrossRef]
- Zavaleta, N.; Lanata, C.; Butron, B.; Peerson, J.M.; Brown, K.H.; Lönnerdal, B. Effect of acute maternal infection on quantity and composition of breast milk. Am. J. Clin. Nutr. 1995, 62, 559–563. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Donangelo, C.M.; King, J.C. Maternal Zinc Intakes and Homeostatic Adjustments during Pregnancy and Lactation. Nutrients 2012, 4, 782-798. https://doi.org/10.3390/nu4070782
Donangelo CM, King JC. Maternal Zinc Intakes and Homeostatic Adjustments during Pregnancy and Lactation. Nutrients. 2012; 4(7):782-798. https://doi.org/10.3390/nu4070782
Chicago/Turabian StyleDonangelo, Carmen Marino, and Janet C. King. 2012. "Maternal Zinc Intakes and Homeostatic Adjustments during Pregnancy and Lactation" Nutrients 4, no. 7: 782-798. https://doi.org/10.3390/nu4070782