Breastfeeding Promotion, Support and Protection: Review of Six Country Programmes

Abstract
:1. Introduction
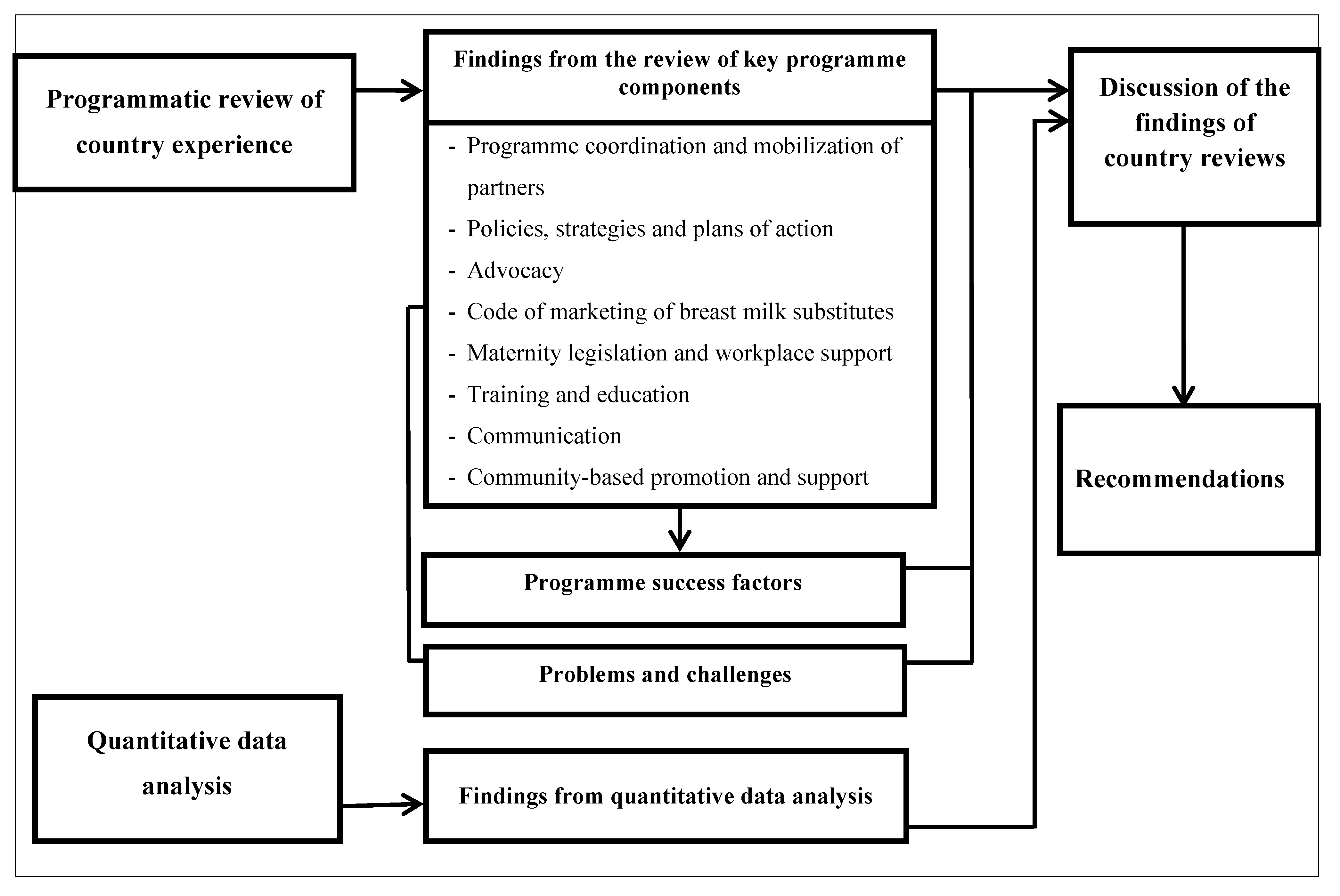
2. Method
2.1. Country Selection and Context

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selected Indicators | Bangladesh | Benin | Philippines | Sri Lanka + | Uganda | Uzbekistan ++ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographic indicators # | 1995 | 2005 | 1995 | 2005 | 1995 | 2005 | 1995 | 2005 | 1995 | 2005 | 1995 | 2005 |
| Total population (millions) | 118 | 141 | 5.65 | 7.63 | 69.3 | 85.6 | 18.2 | 19.8 | 20.8 | 28.4 | 22.9 | 26.0 |
| Population children under 5 years (millions) | 16.6 | 16.0 | 1.04 | 1.33 | 9.99 | 11.4 | 1.70 | 1.77 | 4.13 | 5.61 | 3.31 | 2.58 |
| Urban population (%) | 23.7 | 28.0 | 37.2 | 41.2 | 48.8 | 48.1 | 17.2 | 14.5 | 11.7 | 12.7 | 38.4 | 37.2 |
| Child mortality indicators * | ||||||||||||
| Under 5 mortality rate | 114 | 64.2 | 160 | 129 | 47.7 | 34.5 | 26.7 | 19.5 | 167 | 120 | 69.7 | 56.7 |
| Infant mortality rate | 80.8 | 49.1 | 97.5 | 80.5 | 34.8 | 26.6 | 22.5 | 16.7 | 99.7 | 74.7 | 57.5 | 47.8 |
| Nutrition indicators ** | 1996/1997 | 2007 | 1996 | 2006 | 1996 | 2003 | 1993 | 2006 | 1995 | 2006 | 1996 | 2006 |
| Stunting prevalence among children <5 years (%) | 55 | 36 | 29 | 38 | 30 | 30 | 24 | 18 | 40 | 32 | 34 | 15 |
| Underweight prevalence among children <5 years (%) | 56 | 46 | 29 | 23 | 28 | 28 | 38 | 22 | 25 | 20 | 17 | 5 |
| Health indicators ¶ | 2007 | 2006 | 2008 | 2006/2007 | 2006 | 2006 | ||||||
| Antenatal care coverage, at least once (%) | 51 | 84 | 91 | 99 | 94 | 99 | ||||||
| Antenatal coverage, 4 times or more (%) | 21 | 61 | 70 | - | 47 | - | ||||||
| Health facility deliveries (%) | 15 | 78 | 38 | 98 | 41 | 97 | ||||||
| Deliveries attended by skilled health personnel (%) | 18 | 74 | 62 | 99 | 42 | 100 | ||||||
| Adult HIV prevalence (15–49 years) | <0.1 | 1.2 | <0.1 | <0.1 | 5.4 | 0.1 | ||||||
| Water and sanitation indicators ¶¶ | 2008 | 2008 | 2008 | 2008 | 2008 | 2008 | ||||||
| Percentage using improved drinking water | 81 | 73 | 92 | 89 | 69 | 87 | ||||||
| Percentage using improved sanitation facilities | 53 | 12 | 72 | 91 | 34 | 100 | ||||||
| Human development indicators † | ||||||||||||
| Life expectancy at birth (years) | 68 | 54.9 | 68 | 74.5 | 52.5 | 67.6 | ||||||
| Adult literacy rate ages 15-older (%) | - | - | 95.4 | 90.6 | - | - | ||||||
| Human Development Index (HDI) value | 0.484 | 0.419 | 0.635 | 0.676 | 0.430 | 0.624 | ||||||
2.2. The Review Process: Policy and Programming Experience

2.3. Quantitative Data Analysis
3. Results
3.1. Findings from the Review of Selected Key Programme Components in 6 Countries
3.1.1. Programme Coordination and Mobilization of Partners
3.1.2. Policies, Strategies and Plans of Action
3.1.3. Advocacy
3.1.4. Implementation of the International Code of Marketing of Breastmilk Substitutes
3.1.5. Maternity Protection Legislation and Workplace Support
3.1.6. The Baby Friendly Hospital Initiative (BFHI)
3.1.7. Training and Education
- 1. In-service training updated knowledge and skills and motivated staff. The WHO 40-h breastfeeding counselling course and the WHO/UNICEF 18-h BFHI course were the primary curricula used for in-service training between 1995 and 2005, with tens of thousands of health care providers trained through these courses.
- 2. Pre-service education helped ensure that upcoming/future health care providers were equipped with correct information and practical skills to provide IYCF counselling and support. In most of the countries reviewed, pre-service education focused primarily on theoretical knowledge, without much practical guidance for dealing with lactation management issues. Moreover, in many cases messages were not always harmonized in different curricula (e.g., the curricula for nurses and doctors).
- 3. Professional development courses provided in-depth training to individuals with major responsibilities for IYCF in health facilities, academic institutions and government agencies. A one-month course on Breastfeeding Practice and Policy at the Institute of Child Health in London and a one-month lactation management course at Wellstart International in San Diego trained a generation of professionals who remained breastfeeding advocates for decades. For instance, participants from Uganda started a breastfeeding CSO and set up the first lactation clinic in sub-Saharan Africa. Professional development courses in lactation management were instrumental in training health professionals who became focal points and master trainers in lactation management in the Philippines, Sri Lanka, and Uzbekistan.
3.1.8. Communication
3.1.9. Community-Based Promotion and Support
3.2. Key Challenges
| Levels | Main Challenges and Problems Identified | |
|---|---|---|
| Household/Individual | Lack of infant feeding knowledge and skills among caregivers | |
| - | Lack of knowledge of benefits of breastfeeding and the importance of exclusive breastfeeding. | |
| - | Assumption that breast milk is not enough to nourish infants. | |
| - | Lack of infant feeding skills, such as proper positioning and attachment and appropriate complementary feeding. | |
| - | Lack of understanding that insufficient milk is due to poor suckling techniques and not feeding frequently enough. | |
| Lack of family support | ||
| - | Extended family members encouraging mothers to give other liquids and foods early. | |
| - | Family members not able to support mothers through help with household tasks or other children. | |
| Cultural beliefs and practices | ||
| Health facility/Community | - | Prelacteal feeds, delayed initiation, and discarding of colostrum. |
| - | Giving water, herbal teas, watery porridges, and other drinks within the first six months. | |
| - | Using feeding bottles and various breastmilk substitutes. | |
| - | Poor complementary feeding practices such as delaying introduction beyond six months of age and/or giving foods with insufficient variety, energy density, or feeding frequency. | |
| Unsupportive health facility and community-based services | ||
| - | Health facility practices not conducive to the establishment of good breastfeeding practices. | |
| - | Limited knowledge on IYCF and lactation management, complementary feeding, and counseling skills among health providers and community volunteers. | |
| - | Lack of time to provide the needed IYCF support by the health providers and community volunteers. | |
| - | Poor supervision and monitoring of staff and volunteers trained to provide IYCF support. | |
| National/Sub-National | Unsupportive work environment | |
| - | Limited or no maternity leave. | |
| - | Inflexible working hours and lack of breastfeeding breaks. | |
| - | No breastfeeding rooms or space for expressing and storing breast milk. | |
| Commercial pressures | ||
| - | Widespread advertising of breastmilk substitutes through print media, radio, television, and billboard advertisements. | |
| - | Provision of gifts and incentives to influence health workers to promote formula products. | |
| - | Lack of monitoring and enforcement of marketing regulations for breastmilk substitutes. | |
| Administrative and political challenges | ||
| - | Weak national commitment to IYCF and nutrition and inadequate resources. | |
| - | Poor coordination among government offices and partners. | |
| - | Lack of integrated, cost-effective and sustained approaches to address health and nutrition needs. | |
| - | Rapid turnover of administrative, health service, as well as, community staff and volunteers with IYCF skills. | |
| - | Small-scale and fragmented community-based services. | |
3.3. Success Factors
| Levels | Main Programme Success Factors Identified |
|---|---|
| Community |
|
| Health facility |
|
| Sub-national/National |
|
| International | - International leadership through policy and programmatic guidance (e.g., Innocenti Declaration on the Protection, Promotion and Support of Breastfeeding, the Baby Friendly Hospital Initiative, and the Global Strategy for IYCF). |
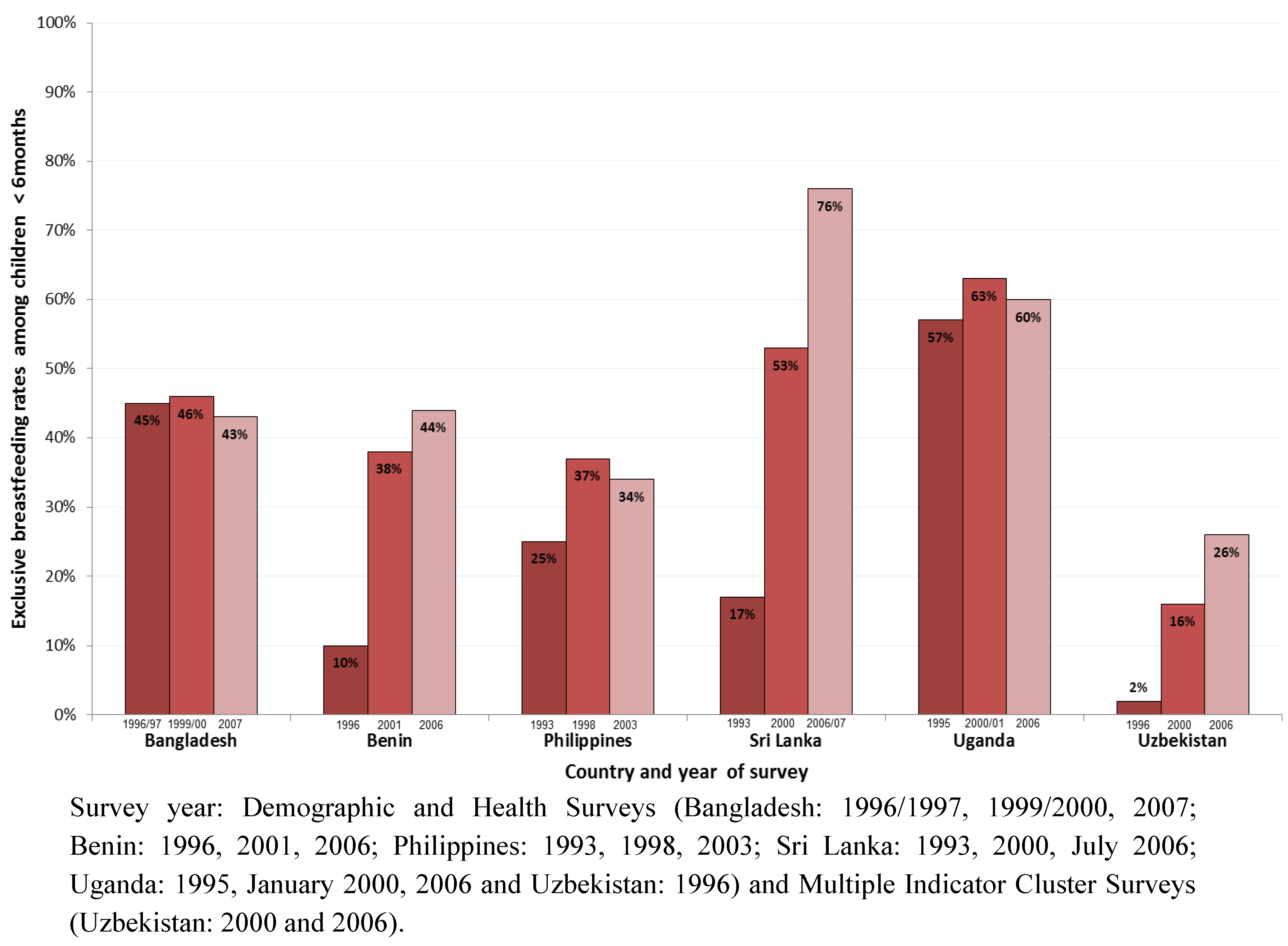
3.4. Effect of Programme on Trends in Exclusive Breastfeeding

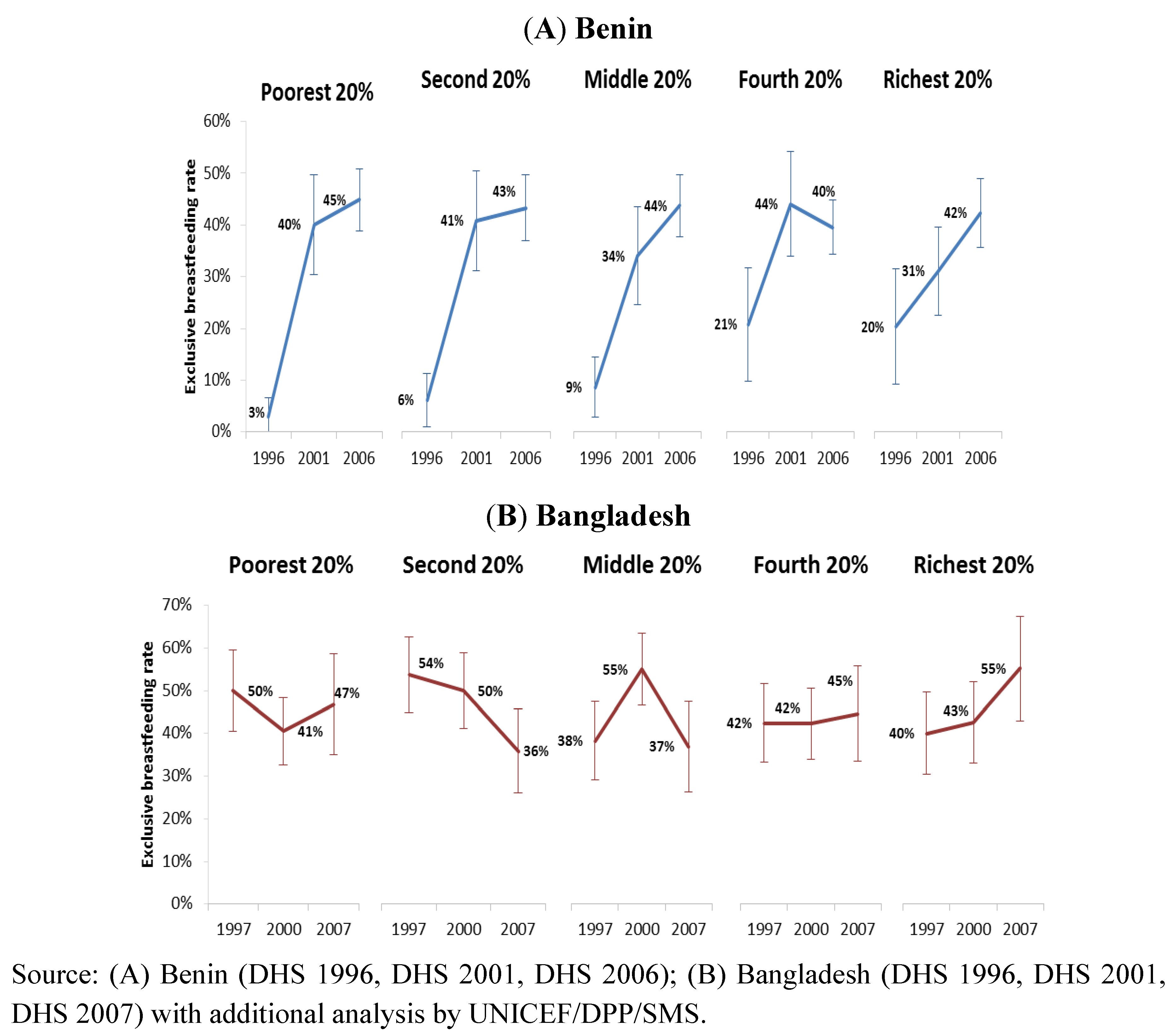
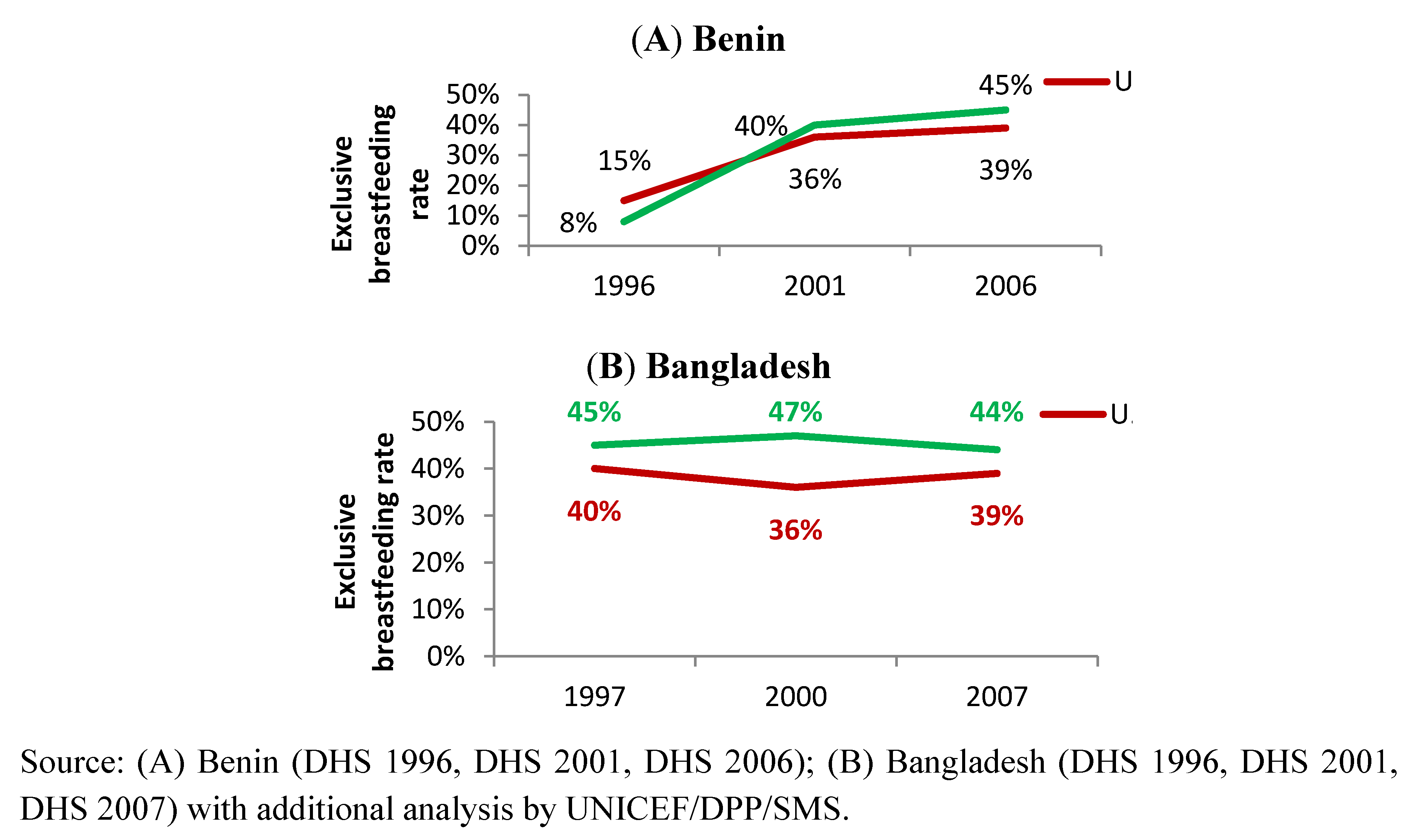
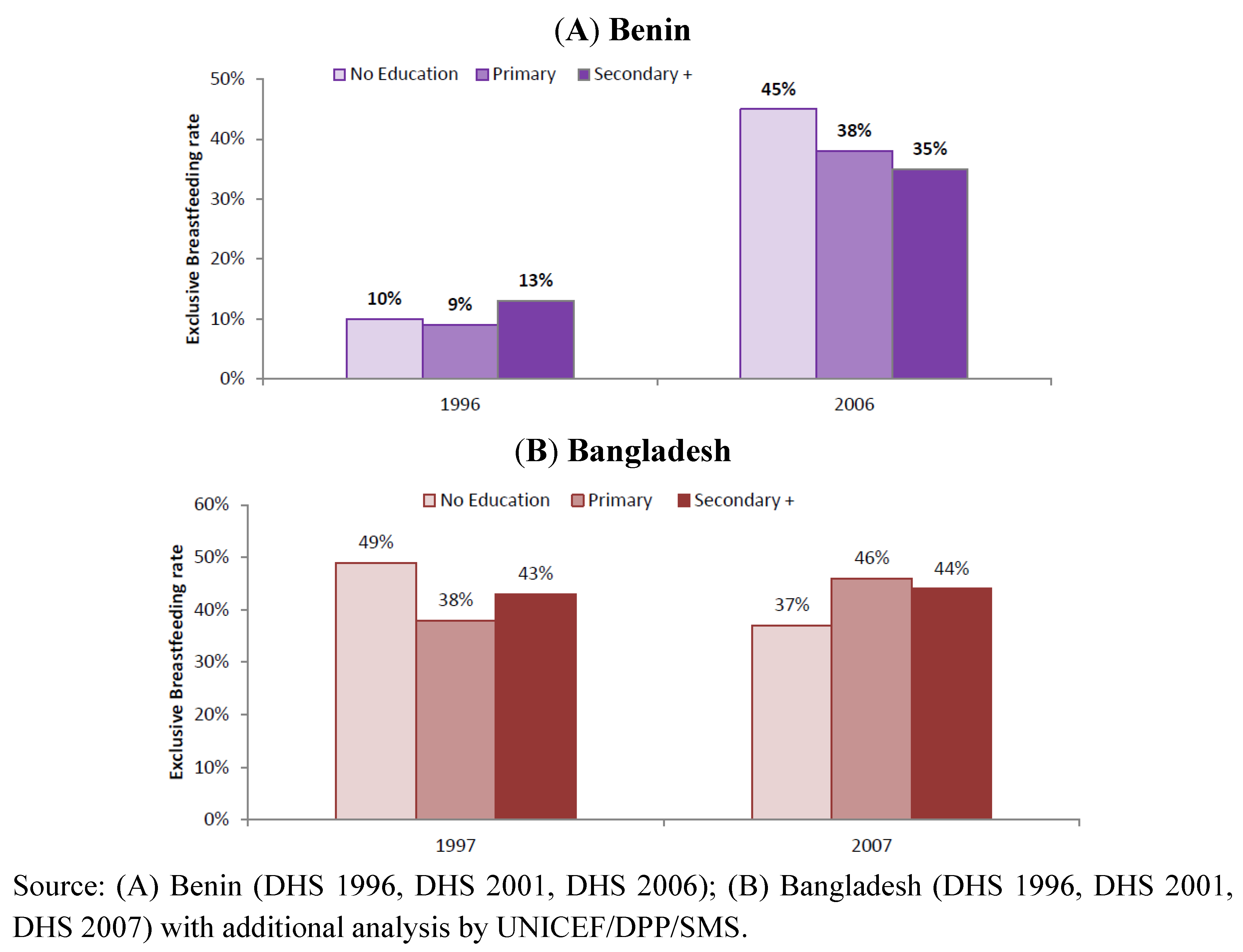
3.5. Effect of Programme on Exclusive Breastfeeding Trends by Selected Population Subgroups in Benin and Bangladesh




4. Discussion and Recommendations
“Exclusive breastfeeding goes a long way towards cancelling out the health difference between being born into poverty or being born into affluence. It is almost as if breastfeeding takes the infant out of poverty for those few vital months in order to give the child a fairer start in life and compensate for the injustices of the world into which it was born.”
5. Conclusions
- 1. Develop and implement a comprehensive strategy that aims from the outset to achieve scale with specific tailored approaches to reach higher risk groups.
- 2. Establish and support a functional and sustainable coordination mechanism.
- 3. Foster an enabling environment by developing an evidence-based advocacy strategy; strengthening Code legislation and enforcement; extending maternity protection, and improving conditions in the workplace for breastfeeding women.
- 4. Strengthen the organizational and technical capacity for IYCF to ensure sustained ownership of IYCF programming and integrate IYCF within pre-service curricula and continuing and in-service education programmes.
- 5. Make the Ten Steps of the BFHI an integral component of the norms and standard operating procedures of facilities and incorporate them in accreditation procedures.
- 6. Extend IYCF counselling and support beyond maternity services and ensure that IYCF is addressed at appropriate contact points during pregnancy and throughout the first two years of life both within the health system and the community.
- 7. Scale up community-based interventions by building coalitions to achieve scale, using multiple platforms at the community level, equipping community workers with IYCF counselling and problem-solving skills and providing supportive supervision and mentoring.
- 8. Implement comprehensive communication strategies based on formative research on enablers and barriers to improved practices including lack of information and support, engrained detrimental cultural practices and social norms, workplace restrictions, and limited decision-making authority by women.
Implications
Acknowledgments
Conflict of Interest
Disclaimer
References
- Pelletier, D.L.; Frongillo, E.A.; Habicht, J.P. Epidemiologic evidence for a potentiating effect of malnutrition on child mortality. Am. J. Public Health 1993, 83, 1130–1133. [Google Scholar] [CrossRef]
- Caulfield, L.E.; de Onis, M.; Blossner, M.; Black, R.E. Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. Am. J. Clin. Nutr. 2004, 80, 193–198. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–360. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.; Shekar, M. Maternal and Child Undernutrition Study Group. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar]
- You, D.; Jones, G.; Hill, K.; Wardlaw, T.; Chopra, M. Levels and trends in child mortality, 1990–2009. Lancet 2010, 376, 931–933. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kakuma, R. The Optimal Duration of Exclusive Breastfeeding: A Systematic Review; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Villalpando, S.; Lopez-Alarcon, M. Growth faltering is prevented by breast-feeding in underprivileged infants from Mexico City. J. Nutr. 2000, 130, 546–552. [Google Scholar]
- Up to What Age Can a Baby Stay Well Nourished by Just Being Breastfed? Available online: http://www.who.int/features/qa/21/en/index.html (accessed on 2 February 2012).
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S. Bellagio Child Survival Study Group. How many child deaths can we prevent this year? Lancet 2003, 362, 65–71. [Google Scholar]
- Bhandari, N.; Bahl, R.; Mazumdar, S.; Martines, J.; Black, R.E.; Bhan, M.K. Infant Feeding Study Group. Effect of community-based promotion of exclusive breastfeeding on diarrhoeal illness and growth: A cluster randomised controlled trial. Lancet 2003, 361, 1418–1423. [Google Scholar]
- Engle, P.L.; Black, M.M.; Behrman, J.R.; Cabral de Mello, M.; Gertler, P.J.; Kapiriri, L.; Martorell, R.; Young, M.E. International Child Development Steering Group. Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet 2007, 369, 229–242. [Google Scholar]
- Horta, B.L.; Bahl, R.; Martines, J.C.; Victora, C.G. Evidence on the Long-Term Effects of Breastfeeding: Systematic Reviews and Meta-analysis; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Walker, S.P.; Wachs, T.D.; Grantham-McGregor, S.; Black, M.M.; Nelson, C.A.; Huffman, S.L.; Baker-Henningham, H.; Chang, S.M.; Hamadani, J.D.; Lozoff, B.; et al. Inequality in early childhood: Risk and protective factors for early child development. Lancet 2011, 378, 1325–1338. [Google Scholar]
- United Nations Children’s Fund, The State of the World’s Children 2011: Adolescence—An Age of Opportunity; UNICEF: New York, NY, USA, 2011.
- Lutter, C.K.; Chaparro, C.M.; Grummer-Strawn, L.M. Increases in breastfeeding in Latin America and the Caribbean: An analysis of equity. Health Policy Plan. 2011, 26, 257–265. [Google Scholar] [CrossRef]
- Lamberti, L.M.; Fischer-Walker, C.L.; Noiman, A.; Victora, C.; Black, R.E. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health 2011, 11, S15. [Google Scholar]
- Celebrating the Innocenti Declaration on the Protection, Promotion and Support of Breastfeeding. Available online: http://www.unicef-irc.org/publications/pdf/1990-2005-gb.pdf (accessed on 5 September 2011).
- Innocenti Declaration on The Protection, Promotion and Support for Breastfeeding. Available online: http://www.unicef.org/programme/breastfeeding/innocenti.htm (accessed on 15 February 2011).
- World Health OrganizationUnited Nations Children’s FundGlobal Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2003.
- World Health OrganizationUnited Nations Children’s FundPlanning Guide for National Implementation of the Global Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2007.
- Horton, S.; Sanghvi, T.; Phillips, M.; Fiedler, J.; Perez-Escamilla, R.; Lutter, C.; Rivera, A.; Segall-Correa, A.M. Breastfeeding promotion and priority setting in health. Health Policy Plan. 1996, 11, 156–168. [Google Scholar] [CrossRef]
- Riordan, J.M. The cost of not breastfeeding: A commentary. J. Hum. Lact. 1997, 13, 93–97. [Google Scholar] [CrossRef]
- Darmstadt, G.L.; Bhutta, Z.A.; Cousens, S.; Adam, T.; Walker, N.; de Bernis, L. Lancet Neonatal Survival Steering Team. Evidence-based, cost-effective interventions: How many newborn babies can we save? Lancet 2005, 365, 977–988. [Google Scholar]
- Edmond, K.M.; Zandoh, C.; Quigley, M.A.; Amenga-Etego, S.; Owusu-Agyei, S.; Kirkwood, B.R. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics 2006, 117, e380–e386. [Google Scholar] [CrossRef]
- Mullany, L.C.; Katz, J.; Li, Y.M.; Khatry, S.K.; LeClerq, S.C.; Darmstadt, G.L.; Tielsch, J.M. Breast-feeding patterns, time to initiation, and mortality risk among newborns in southern Nepal. J. Nutr. 2008, 138, 599–603. [Google Scholar]
- Bartick, M.; Reinhold, A. The burden of suboptimal breastfeeding in the United States: A pediatric cost analysis. Pediatrics 2010, 125, e1048–e1056. [Google Scholar] [CrossRef]
- Levels and Trends in Child Mortality: 2011 Report. Available online: http://www.childinfo.org/files/Child_Mortality_Report_2011.pdf (accessed on 20 January 2012).
- United Nations Children’s Fund, Progress for Children: Achieving the MDGs with Equity; UNICEF: New York, NY, USA, 2010.
- UNICEF/AED Review of Infant and Young Child Feeding Programs Published. Available online: http://www.aednutritioncenter.org/updates/detail/11 (accessed on 1 October 2011).
- World Population Prospects: The 2010 Revision. Available online: http://esa.un.org/wpp/Sorting-Tables/tab-sorting_population.htm (accessed on 10 November 2011).
- Child Mortality Estimates. Available online: http://www.childmortality.org/ (accessed on 12 December 2011).
- Demographic and Health Survey Country Reports. Available online: http://www.measuredhs.com/Data/ (accessed on 12 December 2011).
- Department of Census and Statistics—Sri Lanka. Available online: http://www.statistics.gov.lk/page.asp?page=Health (accessed on 15 November 2011).
- MICS Report from Uzbekistan. Available online: http://www.childinfo.org/mics2_uzbekistan.html (accessed on 15 November 2011).
- Childinfo. Monitoring the Situation of Children and Women. Available online: http://www.childinfo.org (accessed on 10 October 2011).
- WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation. Available online: http://www.wssinfo.org/ (accessed on 10 October 2011).
- International Human Development Indicators. Available online: http://hdr.undp.org/en/data/profiles/ (accessed 30 September 2011).
- World Health Organization, Infant and Young Child Feeding: A Tool for Assessing National Practices, Policies and Programmes; WHO: Geneva, Switzerland, 2003.
- United Nations Children’s Fund, Programming Guide: Infant and Young Child Feeding; UNICEF: New York, NY, USA, 2011.
- Ministry of Health and Family Welfare (MoHFW), Conceptual Framework of Health, Nutrition and Population Sector Programme: July 2003–June 2006; Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2003.
- Ministry of Health and Family Welfare (MoHFW), Health, Nutrition and Population Sector Programme: Revised Programme Implementation Plan (HNPSP-RPIP): July 2003–June 2010; Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2005.
- The Baby-Friendly Hospital Initiative. Available online: http://www.unicef.org/programme/breastfeeding/baby.htm#10 (accessed on 15 February 2011).
- Aguayo, V.M.; Ross, J. The monetary value of human milk in Francophone West Africa: A PROFILES analysis for nutrition policy communication. Food Nutr. Bull. 2002, 23, 153–161. [Google Scholar]
- Academy for Educational Development, PROFILES: A Process for Nutrition Policy Analysis and Advocacy. An Evaluation of PROFILES Applications in Ten African Countries; Academy for Educational Development: Washington, DC, USA, 2003.
- Black, R.E.; Morris, S.S.; Bryce, J. Where and why are 10 million children dying every year? Lancet 2003, 361, 2226–2234. [Google Scholar] [CrossRef]
- Bryce, J.; el Arifeen, S.; Pariyo, G.; Lanata, C.; Gwatkin, D.; Habicht, J.P. Multi-Country Evaluation of IMCI Study Group. Reducing child mortality: Can public health deliver? Lancet 2003, 362, 159–164. [Google Scholar]
- World Health Organization, International Code of Marketing of Breastmilk Substitutes; WHO: Geneva, Switzerland, 1981.
- Sokol, E. The Code Handbook: A Guide to Implementing the International Code of Marketing of Breastmilk Substitutes; International Code Documentation Centre/International Baby Food Action Network: Penang, Malaysia, 1997. [Google Scholar]
- C183 Maternity Protection Convention 2000. Available online: http://www.ilo.org/ilolex/cgi-lex/convde.pl?C183 (accessed on 1 March 2011).
- International Labour Organization. C183—Maternity Protection Convention, 2000 (No. 183). Available online: http://www.ilo.org/dyn/normlex/en/f?p=1000:12100:0::NO::P12100_ILO_CODE (accessed on 5 May 2012).
- Protecting, Promoting and Supporting Breast-Feeding: The Special Role of Maternity Services. Available online: http://whqlibdoc.who.int/publications/9241561300.pdf (accessed on 2 January 2012).
- Dickin, K.; Griffiths, M.; Piwoz, E.G. Designing by Dialogue: A Program Planners’ Guide to Consultative Research for Improving Young Child Feeding; Academy for Educational Development: Washington, DC, USA, 1997. [Google Scholar]
- Philippines Demographic and Health Survey, 2003—Final Report. Available online: http://www.measuredhs.com/publications/publication-FR156-DHS-Final-Reports.cfm (accessed on 16 February 2011).
- Uganda Demographic and Health Survey, 2006—Final Report. Available online: http://www.measuredhs.com/publications/publication-FR194-DHS-Final-Reports.cfm (accessed on 16 February 2011).
- MEASURE DHS. Bangladesh: Standard DHS, 2011. Available online: http://www.measuredhs.com/what-we-do/survey/survey-display-349.cfm (accessed 30 July 2012).
- United Nations Children’s Fund, The State of the World’s Children 1985; Oxford University Press: New York, NY, USA, 1985.
- BASICS II, Country Report: Benin. Basic Support for Institutionalizing Child Survival (BASICS) Project; The United States Agency for International Development: Arlington, VA, USA, 2004.
- Promoting Exclusive Breastfeeding in Benin: A Success Story. Available online: http://www.unicef.org/wcaro/2009_2464.html (accessed on 20 January 2011).
- Venancio, S.I.; Monteiro, C.A. Individual and contextual determinants of exclusive breast-feeding in Sao Paulo, Brazil: A multilevel analysis. Public Health Nutr. 2006, 9, 40–46. [Google Scholar]
- Tiwari, R.; Mahajan, P.C.; Lahariya, C. The determinants of exclusive breast feeding in urban slums: A community based study. J. Trop. Pediatr. 2009, 55, 49–54. [Google Scholar]
- Chaparro, C.M.; Lutter, C.K. Increases in breastfeeding duration observed in Latin America and the Caribbean and the role of maternal demographic and healthcare characteristics. Food Nutr. Bull. 2010, 31, S117–S127. [Google Scholar]
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Benin; UNICEF: New York, NY, USA, 2009.
- Lauer, J.A.; Betran, A.P.; Barros, A.J.; de Onis, M. Deaths and years of life lost due to suboptimal breast-feeding among children in the developing world: A global ecological risk assessment. Public Health Nutr. 2006, 9, 673–685. [Google Scholar]
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Bangladesh; UNICEF: New York, NY, USA, 2009.
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Philippines; UNICEF: New York, NY, USA, 2009.
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Sri Lanka; UNICEF: New York, NY, USA, 2009.
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Uganda; UNICEF: New York, NY, USA, 2009.
- United Nations Children’s Fund, Infant and Young Child Feeding Programme Review. Case Study: Uzbekistan; UNICEF: New York, NY, USA, 2009.
- Heinig, M.J.; Dewey, K.G. Health advantages of breast feeding for infants: A critical review. Nutr. Res. Rev. 1996, 9, 89–110. [Google Scholar] [CrossRef]
- Cushing, A.H.; Samet, J.M.; Lambert, W.E.; Skipper, B.J.; Hunt, W.C.; Young, S.A.; McLaren, L.C. Breastfeeding reduces risk of respiratory illness in infants. Am. J. Epidemiol. 1998, 147, 863–870. [Google Scholar] [CrossRef]
- Silfverdal, S.A.; Bodin, L.; Olcen, P. Protective effect of breastfeeding: An ecologic study of Haemophilus influenzae meningitis and breastfeeding in a Swedish population. Int. J. Epidemiol. 1999, 28, 152–156. [Google Scholar] [CrossRef]
- WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality, Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: A pooled analysis. In Lancet; 2000; 355, pp. 451–455.
- Ip, S.; Chung, M.; Raman, G.; Chew, P.; Magula, N.; DeVine, D.; Trikalinos, T.; Lau, J. Breastfeeding and maternal and infant health outcomes in developed countries. Evid. Rep. Technol. Assess. 2007, 153, 1–186. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Mangasaryan, N.; Martin, L.; Brownlee, A.; Ogunlade, A.; Rudert, C.; Cai, X. Breastfeeding Promotion, Support and Protection: Review of Six Country Programmes. Nutrients 2012, 4, 990-1014. https://doi.org/10.3390/nu4080990
Mangasaryan N, Martin L, Brownlee A, Ogunlade A, Rudert C, Cai X. Breastfeeding Promotion, Support and Protection: Review of Six Country Programmes. Nutrients. 2012; 4(8):990-1014. https://doi.org/10.3390/nu4080990
Chicago/Turabian StyleMangasaryan, Nune, Luann Martin, Ann Brownlee, Adebayo Ogunlade, Christiane Rudert, and Xiaodong Cai. 2012. "Breastfeeding Promotion, Support and Protection: Review of Six Country Programmes" Nutrients 4, no. 8: 990-1014. https://doi.org/10.3390/nu4080990