Assessment of Daily Food and Nutrient Intake in Japanese Type 2 Diabetes Mellitus Patients Using Dietary Reference Intakes


Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Estimation and Assessment of Habitual Food and Nutrient Intake
2.3. Participants’ Physical Status, Medication, and Blood Constituent Values
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics

{kind=link}
{kind=link}
| Male | Female | p value | ||
|---|---|---|---|---|
| n = 77 | n = 72 | |||
| Age (years) | 65.3 ± 9.2 | 66.1 ± 9.5 | 0.74 | |
| Age classes, n (%) | 40–49 | 6 (7.8) | 6 (8.3) | 1.00 |
| 50–59 | 11 (14.3) | 10 (13.9) | ||
| 60–69 | 32 (41.6) | 29 (40.3) | ||
| over 70 | 28 (36.4) | 27 (37.5) | ||
| Diabetes medicine, yes, n (%) | 59 (77) | 60 (83) | 0.41 | |
| Dyslipidemia medicine, yes, n (%) | 26 (34) | 38 (53) | 0.02 | |
| Insulin treatment, yes, n (%) | 13 (17) | 20 (28) | 0.12 | |
| BMI (kg/m2) | 24.3 ± 3.9 | 23.7 ± 4.5 | 0.23 | |
| HbA1c (%) | 6.8 ± 0.9 | 6.9 ± 0.9 | 0.34 | |
| (≥7.0 *, %) | (58.4) | (58.3) | ||
| Plasma glucose (mg/dL) | 157 ± 50 | 152 ± 59 | 0.40 | |
| (≥180 *, %) | (28.6) | (25.0) | ||
| Triglycerides (mg/dL) | 149 ± 92 | 120 ± 77 | 0.03 | |
| (≥150 *, %) | (37.3) | (21.4) | ||
| LDL cholesterol (mg/dL) | 114 ± 22 | 98 ± 22 | 0.01 | |
| (≥120 *, %) | (45.5) | (15.4) | ||
| HDL cholesterol (mg/dL) | 55 ± 14 | 64 ± 16 | <0.01 | |
| (<40 *, %) | (10.7) | (1.4) | ||
| Urea nitrogen (mg/dL) | 15.8 ± 4.2 | 15.4 ± 4.4 | 0.31 | |
| Creatinine (mg/dL) | 0.84 ± 0.19 | 0.62 ± 0.23 | <0.01 | |
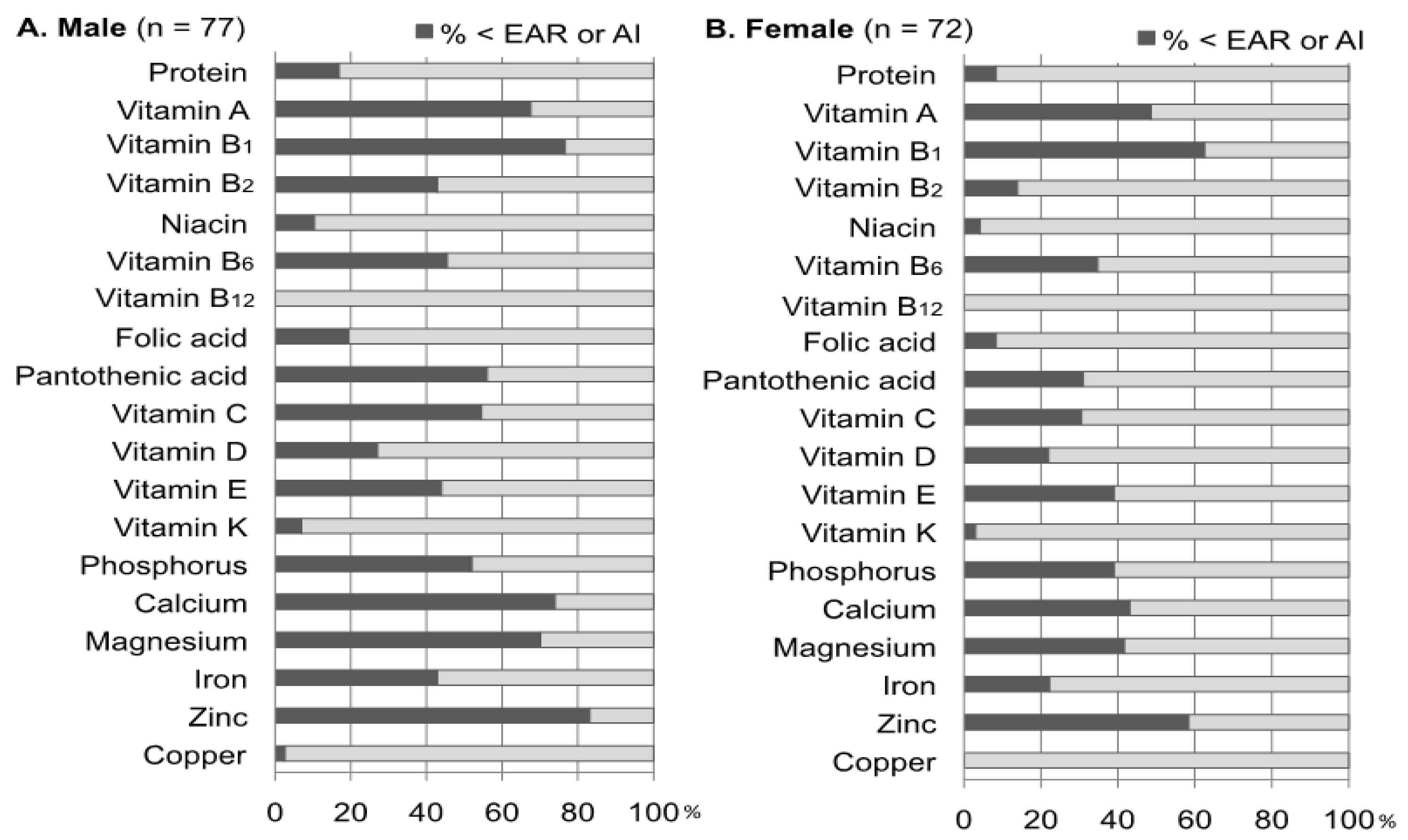
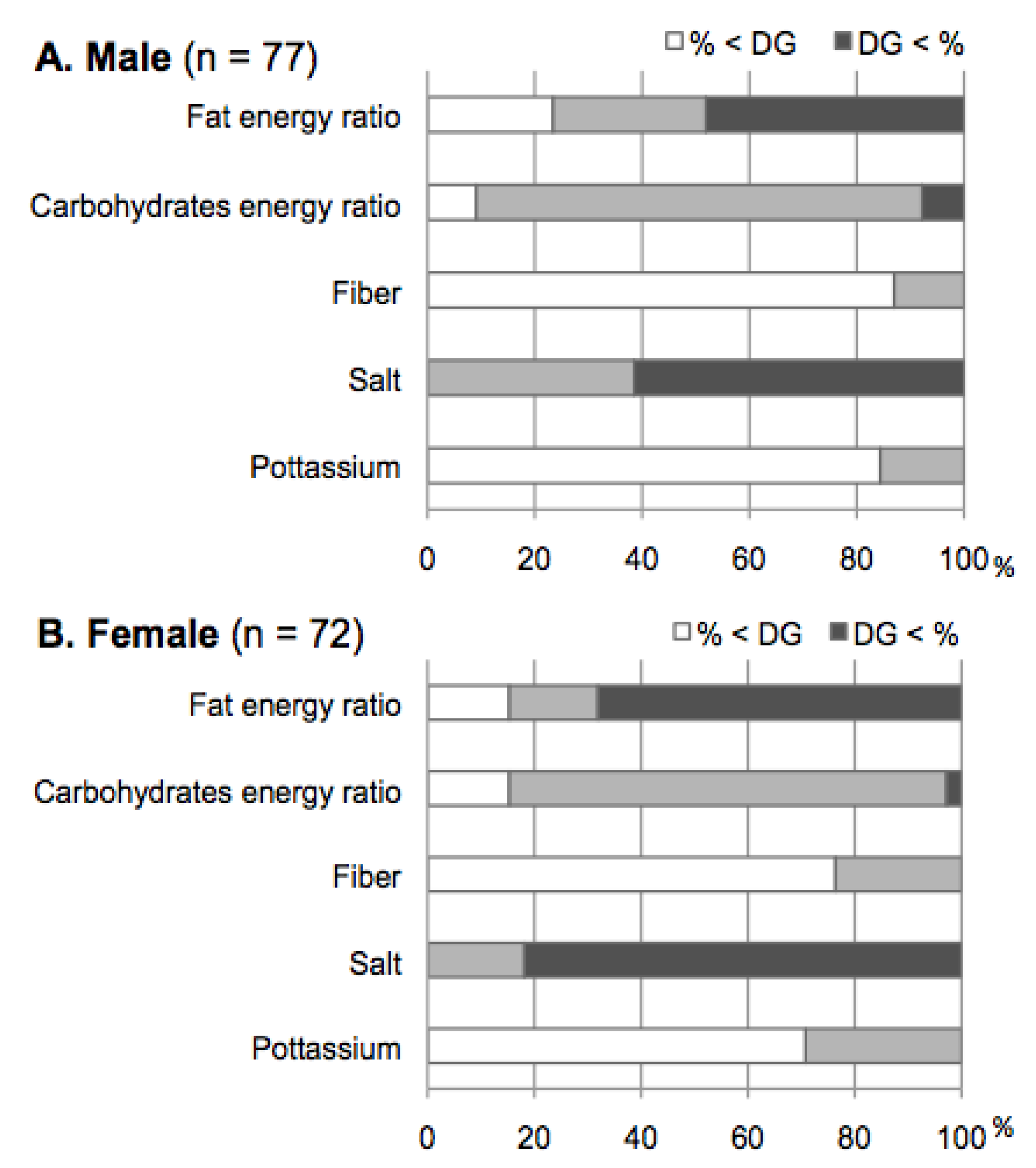
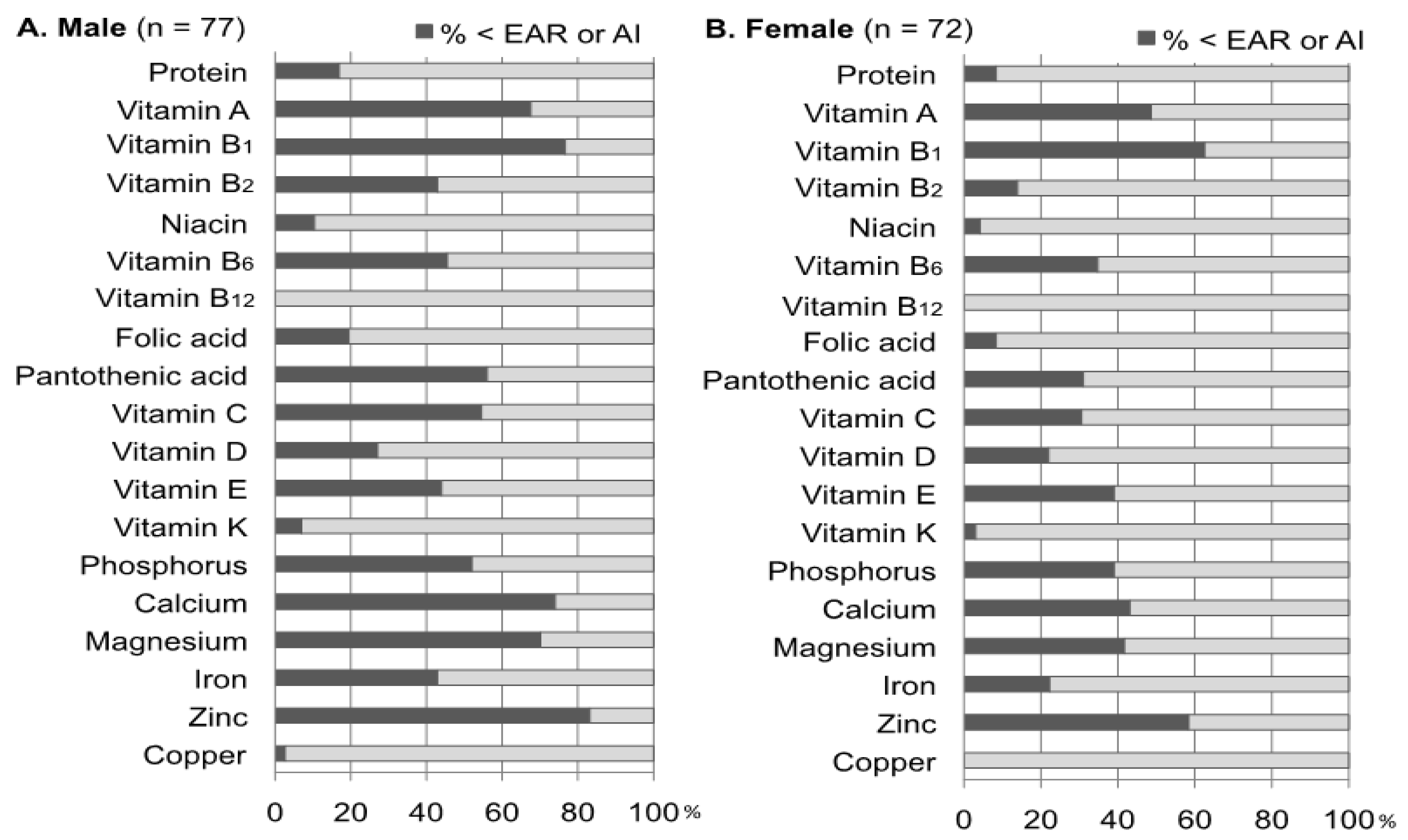
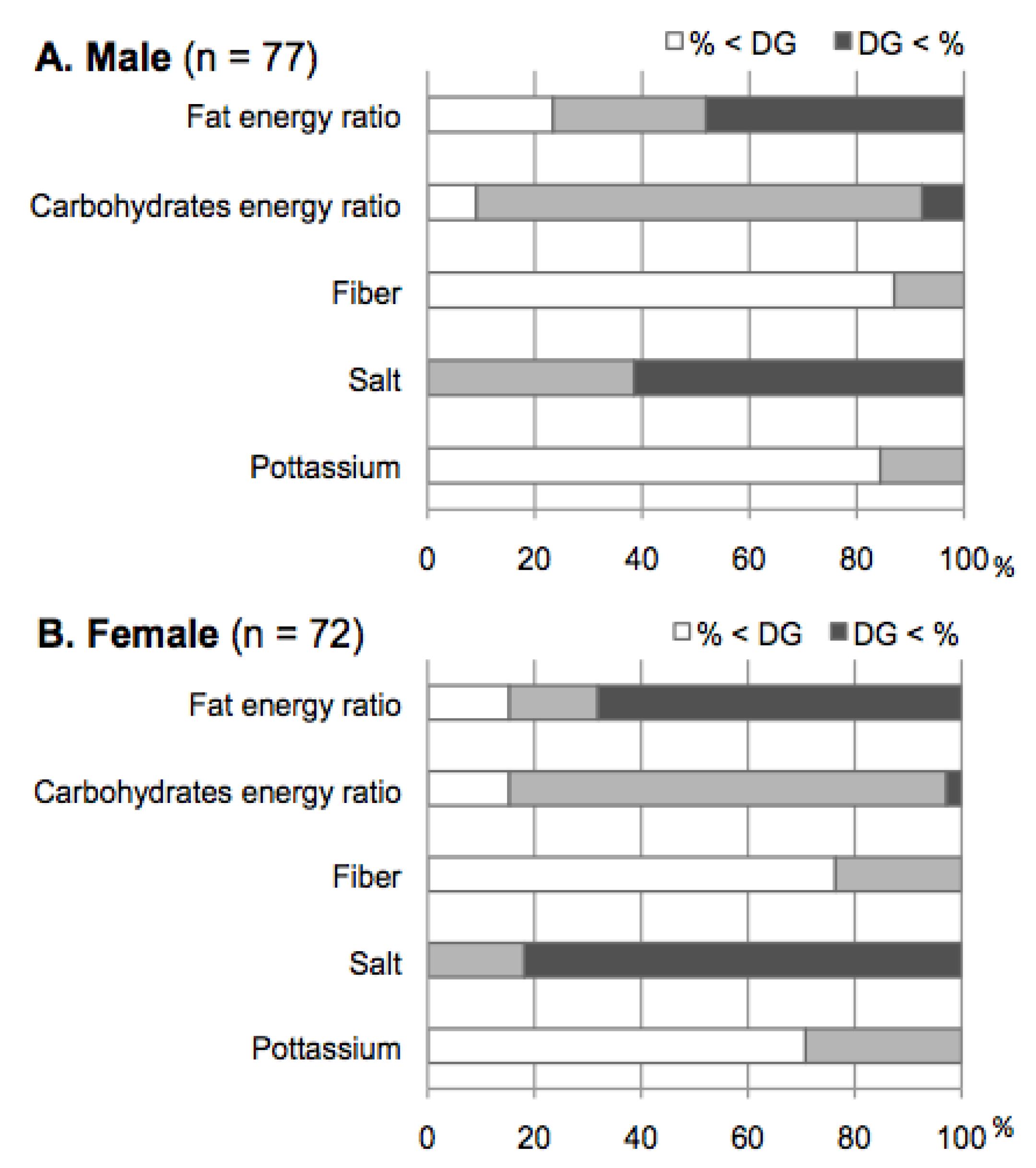
3.2. Assessment of Nutrient Intake Using the DRIs
3.3. Comparisons between Food Group or Nutrients Intake and the NNSJ
| Male | Patients (n = 77) | NNSJ (n = 726) | Difference of NNSJ from Patients | |||
|---|---|---|---|---|---|---|
| Mean | Mean | Mean | 95%CI | p value | ||
| Grains and Cereals (g) | 437 | 513 | −76 | −114.8 | −37.5 | <0.01 |
| Potatoes (g) | 27 | 57 | −30 | −48.3 | −11.2 | <0.01 |
| Sugar (g) | 13 | 8 | 5 | −1.8 | 12.7 | 0.14 |
| Pulses (g) | 4.5 | 73 | −28 | −50.0 | −6.9 | 0.01 |
| Nuts (g) | 2.6 | 3.0 | −0.4 | −13.0 | 12.3 | 0.96 |
| Vegetables (g) | 266 | 318 | −52 | −100.7 | −3.2 | 0.04 |
| Green vegetables (g) | 115 | 105 | 11 | −16.4 | 38.0 | 0.44 |
| Write vegetables (g) | 150 | 187 | −37 | −70.2 | −3.5 | 0.03 |
| Fruits (g) | 94 | 126 | −32 | −60.9 | −3.1 | 0.03 |
| Mushrooms (g) | 11 | 22 | −10 | −25.0 | 4.2 | 0.16 |
| Algae (g) | 10 | 13 | −3 | −15.5 | 9.0 | 0.61 |
| Fishes and shellfishes (g) | 85 | 107 | −23 | −42.0 | −3.2 | 0.02 |
| Meats (g) | 55 | 77 | −22 | −38.7 | −5.2 | 0.01 |
| Eggs (g) | 38 | 37 | 1 | −12.2 | 13.3 | 0.94 |
| Milk (g) | 137 | 91 | 46 | 6.7 | 84.6 | 0.02 |
| Oils and fats (g) | 19 | 10 | 9 | 2.8 | 15.0 | <0.01 |
| Confectionery (g) | 46 | 20 | 27 | 7.6 | 45.5 | 0.01 |
| Beverages (g) | 1029 | 828 | 201 | 71.1 | 330.6 | <0.01 |
| Energy (kcal) | 1925 | 2143 | −218 | −302 | −134 | <0.01 |
| Protein (g) | 68 | 78 | −10 | −16.3 | −3.2 | <0.01 |
| Animal protein (%) | 52 | 51 | 2 | −2.8 | 5.9 | 0.48 |
| Fat (g) | 53 | 55 | −2 | −8.7 | 5.3 | 0.64 |
| Fat (E%) | 25 | 23 | 2 | −1.1 | 4.8 | 0.22 |
| Animal fat (g) | 24 | 27 | −3 | −9.2 | 3.0 | 0.31 |
| Cholesterol (mg) | 323 | 334 | −11 | −46.9 | 25.3 | 0.56 |
| Carbohydrates (g) | 260 | 295 | −35 | −51.6 | −18.0 | <0.01 |
| Carbohydrates (E%) | 54 | 62 | −8 | −10.8 | −5.5 | <0.01 |
| Fiber (g) | 13 | 17 | −4 | −7.2 | 0.0 | 0.05 |
| Salt (g) | 10.8 | 12.0 | −1.2 | −3.9 | 1.4 | 0.36 |
| Potassium (mg) | 2343 | 2591 | −248 | −416 | −80 | <0.01 |
| Calcium (mg) | 501 | 561 | −60 | −112 | −7 | 0.03 |
| Magnesium (mg) | 254 | 285 | −31 | −51.3 | −10.9 | <0.01 |
| Phosphorus (mg) | 1025 | 1104 | −79 | −145 | −13 | 0.02 |
| Iron (mg) | 6.9 | 8.9 | −2.0 | −4.2 | 0.1 | 0.07 |
| Zinc (mg) | 7.6 | 8.9 | −1.3 | −3.2 | 0.6 | 0.17 |
| Copper (mg) | 1.07 | 1.32 | −0.25 | −0.97 | 0.47 | 0.49 |
| Male | Patients (n = 72) | NNSJ (n = 815) | Difference of NNSJ from Patients | |||
|---|---|---|---|---|---|---|
| Mean | Mean | Mean | 95%CI | p value | ||
| Grains and Cereals (g) | 354 | 385 | −31 | −56.9 | −5.2 | 0.02 |
| Potatoes (g) | 28 | 58 | −29 | −58 | −11.0 | <0.01 |
| Sugar (g) | 13 | 8 | 5 | −1.7 | 12.6 | 0.14 |
| Pulses (g) | 62 | 63 | −1 | −22.0 | 19.6 | 0.91 |
| Nuts (g) | 2.6 | 2.4 | 0.2 | −9.0 | 9.5 | 0.96 |
| Vegetables (g) | 335 | 320 | 15 | −49.7 | 80.0 | 0.65 |
| Green vegetables (g) | 169 | 111 | 58 | 8.3 | 106.9 | 0.02 |
| Write vegetables (g) | 166 | 185 | −18 | −50.0 | 13.1 | 0.25 |
| Fruits (g) | 128 | 155 | −27 | −60.7 | 7.6 | 0.13 |
| Mushrooms (g) | 13 | 20 | −7 | −20.2 | 5.6 | 0.27 |
| Algae (g) | 10 | 13 | −3 | −16.2 | 10.4 | 0.67 |
| Fishes and shellfishes (g) | 81 | 86 | −4 | −23.4 | 14.8 | 0.66 |
| Meats (g) | 51 | 61 | −10 | −26.9 | 6.8 | 0.24 |
| Eggs (g) | 39 | 33 | 6 | −12.5 | 25.0 | 0.51 |
| Milk (g) | 144 | 110 | 35 | 3.4 | 65.8 | 0.03 |
| Oils and fats (g) | 18 | 9 | 9 | 3.0 | 15.9 | <0.01 |
| Confectionery (g) | 67 | 25 | 41 | 19.2 | 63.4 | <0.01 |
| Beverages (g) | 1110 | 654 | 456 | 302.6 | 608.8 | <0.01 |
| Energy (kcal) | 1171 | 1732 | −21 | −119 | 7.6 | 0.67 |
| Protein (g) | 66 | 67 | −1 | −7.4 | 5.6 | 0.78 |
| Animal protein (%) | 52 | 50 | 2 | −2.0 | 6.6 | 0.30 |
| Fat (g) | 53 | 49 | 4 | −3.4 | 12.0 | 0.28 |
| Fat (E%) | 27 | 25 | 2 | −0.8 | 5.4 | 0.14 |
| Animal fat (g) | 22 | 24 | −1 | −7.3 | 4.9 | 0.69 |
| Cholesterol (mg) | 293 | 291 | 2 | −34.2 | 37.6 | 0.92 |
| Carbohydrates (g) | 237 | 249 | −12 | −27.7 | 3.4 | 0.13 |
| Carbohydrates (E%) | 56 | 60 | −4 | −6.3 | −0.8 | 0.01 |
| Fiber (g) | 14 | 17 | −2 | −6.1 | 1.2 | 0.19 |
| Salt (g) | 10.3 | 10.6 | −0.3 | −3.1 | 2.4 | 0.81 |
| Potassium (mg) | 2571 | 2510 | 61 | −163 | 285 | 0.59 |
| Calcium (mg) | 569 | 555 | 14 | −38 | 65 | 0.60 |
| Magnesium (mg) | 261 | 260 | 1 | −22 | 23 | 0.95 |
| Phosphorus (mg) | 1022 | 975 | 47 | −25 | 118 | 0.20 |
| Iron (mg) | 7.3 | 8.3 | −1.0 | −3.3 | 113 | 0.41 |
| Zinc (mg) | 7.3 | 7.5 | −0.2 | −2.1 | 1.6 | 0.81 |
| Copper (mg) | 1.09 | 1.15 | −0.06 | −0.74 | 0.62 | 0.86 |
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- King, H.; Aubert, R.E.; Herman, W.H. Global burden of diabetes, 1995–2025: Prevalence, numerical estimates, and projections. Diabetes Care 1998, 21, 1414–1431. [Google Scholar] [CrossRef]
- Annual Report of the National Health and Nutrition Survey in 2007 (in Japanese); Ministry of Health Labour and Welfare: Tokyo, Japan, 2010.
- Franz, M.J.; Boucher, J.L.; Green-Pastors, J.; Powers, M.A. Evidence-based nutrition practice guidelines for diabetes and scope and standards of practice. J. Am. Diet. Assoc. 2008, 108, S52–S58. [Google Scholar] [CrossRef]
- Franz, M.J.; Powers, M.A.; Leontos, C.; Holzmeister, L.A.; Kulkarni, K.; Monk, A.; Wedel, N.; Gradwell, E. The evidence for medical nutrition therapy for type 1 and type 2 diabetes in adults. J. Am. Diet. Assoc. 2010, 110, 1852–1889. [Google Scholar] [CrossRef]
- Paulweber, B.; Valensi, P.; Lindstrom, J.; Lalic, N.M.; Greaves, C.J.; McKee, M.; Kissimova-Skarbek, K.; Liatis, S.; Cosson, E.; Szendroedi, J.; et al. A European evidence-based guideline for the prevention of type 2 diabetes. Horm. Metab. Res. 2010, 42, S3–S36. [Google Scholar]
- Mann, J.I.; de Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Riccardi, G.; Rivellese, A.A.; Rizkalla, S.; Slama, G.; et al. Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 373–394. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabete-2012. Diabetes Care 2012, 35, S11–S63. [CrossRef]
- The Japan Diabetes Society, Evidence-Based Practice Guideline for the Treatment of Diabetes in Japan (in Japanese); Nankodo: Tokyo, Japan, 2010; pp. 21–39.
- Japan Diabetes Society, Food Exchange Lists Dietary guidance for Persons with Diabetes; Bunkodo: Tokyo, Japan, 2003; p. 1.
- Yamada, S. Dietary therapy of type 2 diabetic mellitus (in Japanese). Naika 2011, 108, 616–620. [Google Scholar]
- Japanese Society for Dialysis Therapy. An overview of regular dialysis treatment in Japan (as of 31 December 2011) (in Japanese). J. Jpn. Soc. Dial. Ther. 2011, 43, 1–36.
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-administered diet history questionnaire developed for health education: A relative validation of the test-version by comparison with 3-day diet record in women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef]
- Kasuga, M.; Sasaki, S.; Shibata, K.; Tabata, I.; Nakamura, T.; Morita, A.; Yoshiike, N. Dietary reference intakes for Japanese 2010. J. Nutr. Sci. Vitaminol. 2013, 59, S1–S109. [Google Scholar] [CrossRef]
- Ministry of Health, Labour, and Welfare, The National Nutrition Survey in Japan in 2010 (in Japanese); Ministry of Health, Labour, and Welfare: Tokyo, Japan, 2012.
- Yoshiike, N.; Matsumura, Y.; Iwase, M.; Sugiyama, M.; Yamaguchi, M. National nutrition survey in Japan. J. Epidemiol. 1996, 6, S189–S200. [Google Scholar]
- Ford, E.S.; Mokdad, A.H. Fruit and vegetable consumption and diabetes mellitus incidence among U.S. adults. Prev. Med. 2001, 32, 33–39. [Google Scholar] [CrossRef]
- Bazzano, L.A.; Li, T.Y.; Joshipura, K.J.; Hu, F.B. Intake of fruit, vegetables, and fruit juices and risk of diabetes in women. Diabetes Care 2008, 31, 1311–1317. [Google Scholar] [CrossRef]
- Chandalia, M.; Garg, A; Lutjohann, D.; von Bergmann, K.; Grundy, S.M.; Brinkley, L.J. Beneficial effects of high dietary fiber intake in patients with type 2 diabetes mellitus. N. Engl. J. Med. 2000, 342, 1392–1398. [Google Scholar] [CrossRef]
- Giacco, R.; Parillo, M.; Rivellese, A.A.; Lasorella, G.; Giacco, A.; D’Episcopo, L.; Riccardi, G. Long-term dietary treatment with increased amounts of fiber-rich low-glycemic index natural foods improves blood glucose control and reduces the number of hypoglycemic events in type 1 diabetic patients. Diabetes Care 2000, 23, 1461–1466. [Google Scholar] [CrossRef]
- Takahashi, K.; Kamada, C.; Yoshimura, H.; Okumura, R.; Iimuro, S.; Ohashi, Y.; Araki, A.; Umegaki, H.; Sakurai, T.; Yoshimura, Y.; et al. Effects of total and green vegetable intakes on glycated hemoglobin A1c and triglycerides in elderly patients with type 2 diabetes mellitus: The Japanese Elderly Intervention Trial. Geriatr. Gerontol. Int. 2012, 12, S50–S58. [Google Scholar]
- Iimuro, S.; Yoshimura, Y.; Umegaki, H.; Sakurai, T.; Araki, A.; Ohashi, Y.; Iijima, K.; Ito, H. Dietary pattern and mortality in Japanese elderly patients with type 2 diabetes mellitus: Does a vegetable- and fish-rich diet improve mortality? An explanatory study. Geriatr. Gerontol. Int. 2012, 12, S59–S67. [Google Scholar]
- Nanri, A.; Mizoue, T.; Yoshida, D.; Takahashi, R.; Takayanagi, R. Dietary patterns and A1C in Japanese men and women. Diabetes Care 2008, 31, 1568–1573. [Google Scholar] [CrossRef]
- Sakuma, M.; Yamanaka-Okumura, H.; Naniwa, Y.; Matsumoto, D.; Tsunematsu, M.; Yamamoto, H.; Taketani, Y.; Takeda, E. Dose-dependent effects of barley cooked with white rice on postprandial glucose and desacyl ghrelin levels. J. Clin. Biochem. Nutr. 2009, 44, 151–159. [Google Scholar] [CrossRef]
- Nanri, A.; Mizoue, T.; Noda, M.; Takahashi, Y.; Kato, M.; Inoue, M.; Tsugane, S. Rice intake and type 2 diabetes in Japanese men and women: The Japan Public Health Center-based Prospective Study. Am. J. Clin. Nutr. 2010, 92, 1468–1477. [Google Scholar] [CrossRef]
- Hu, E.A.; Pan, A.; Malik, V.; Sun, Q. White rice consumption and risk of type 2 diabetes: Meta-analysis and systematic review. BMJ 2012, 15, 344. [Google Scholar]
- Wheeler, M.L.; Dunbar, S.A.; Jaacks, L.M.; Karmally, W.; Mayer-Davis, E.J.; Wylie-Rosett, J.; Yancy, W.S., Jr. Macronutrients, food groups, and eating patterns in the management of diabetes: A systematic review of the literature, 2010. Diabetes Care 2012, 35, 434–445. [Google Scholar] [CrossRef]
- Cornier, M.A.; Donahoo, W.T.; Pereira, R.; Gurevich, I.; Westergren, R.; Enerback, S.; Eckel, P.J.; Goalstone, M.L.; Hill, J.O.; Eckel, R.H.; et al. Insulin sensitivity determines the effectiveness of dietary macronutrient composition on weight loss in obese women. Obes. Res. 2005, 13, 703–709. [Google Scholar] [CrossRef]
- Ebbeling, C.B.; Leidig, M.M.; Feldman, H.A.; Lovesky, M.M.; Ludwig, D.S. Effects of a low-glycemic load vs. low-fat diet in obese young adults: A randomized trial. JAMA 2007, 16, 2092–2102. [Google Scholar]
- McNaughton, S.A.; Mishra, G.D.; Brunner, E.J. Dietary patterns, insulin resistance, and incidence of type 2 diabetes in the Whitehall II Study. Diabetes Care 2008, 31, 1343–1348. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Willett, W.C.; Hu, F.B. Sugarsweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef]
- Imamura, F.; Lichtenstein, A.H.; Dallal, G.E.; Meigs, J.B.; Jacques, P.F. Confounding by dietary patterns of the inverse association between alcohol consumption and type 2 diabetes risk. Am. J. Epidemiol. 2009, 170, 37–45. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kobayashi, Y.; Hattori, M.; Wada, S.; Iwase, H.; Kadono, M.; Tatsumi, H.; Kuwahata, M.; Fukui, M.; Hasegawa, G.; Nakamura, N.; et al. Assessment of Daily Food and Nutrient Intake in Japanese Type 2 Diabetes Mellitus Patients Using Dietary Reference Intakes. Nutrients 2013, 5, 2276-2288. https://doi.org/10.3390/nu5072276
Kobayashi Y, Hattori M, Wada S, Iwase H, Kadono M, Tatsumi H, Kuwahata M, Fukui M, Hasegawa G, Nakamura N, et al. Assessment of Daily Food and Nutrient Intake in Japanese Type 2 Diabetes Mellitus Patients Using Dietary Reference Intakes. Nutrients. 2013; 5(7):2276-2288. https://doi.org/10.3390/nu5072276
Chicago/Turabian StyleKobayashi, Yukiko, Mikako Hattori, Sayori Wada, Hiroya Iwase, Mayuko Kadono, Hina Tatsumi, Masashi Kuwahata, Michiaki Fukui, Goji Hasegawa, Naoto Nakamura, and et al. 2013. "Assessment of Daily Food and Nutrient Intake in Japanese Type 2 Diabetes Mellitus Patients Using Dietary Reference Intakes" Nutrients 5, no. 7: 2276-2288. https://doi.org/10.3390/nu5072276