Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials

Abstract
:1. Introduction
2. Methods
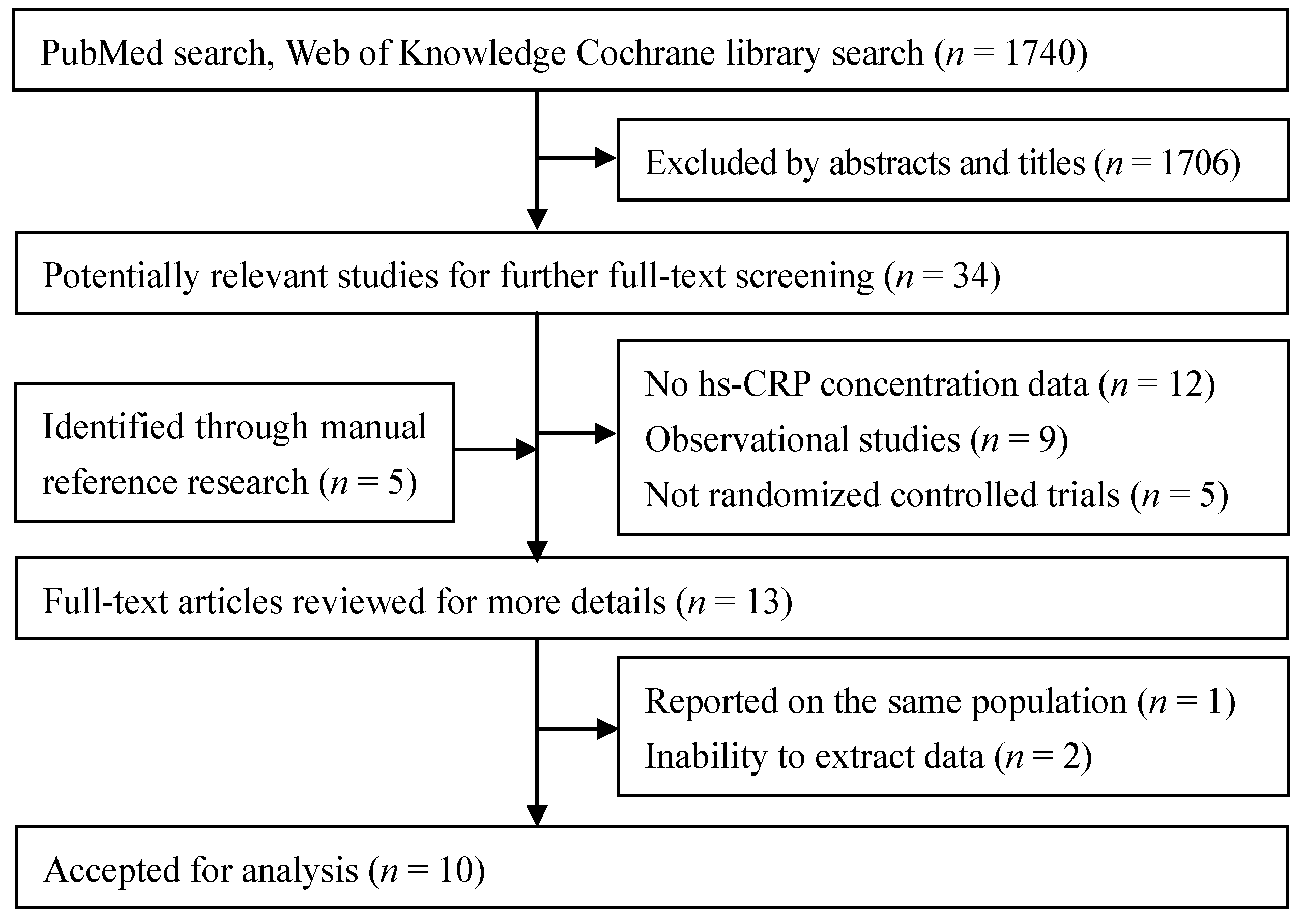
2.1. Search Strategy and Study Selection
2.2. Data Calculation and Quality Assessment
2.3. Data Synthesis and Statistical Analysis
3. Results
3.1. Search Results and Study Selection

3.2. Study Characteristics
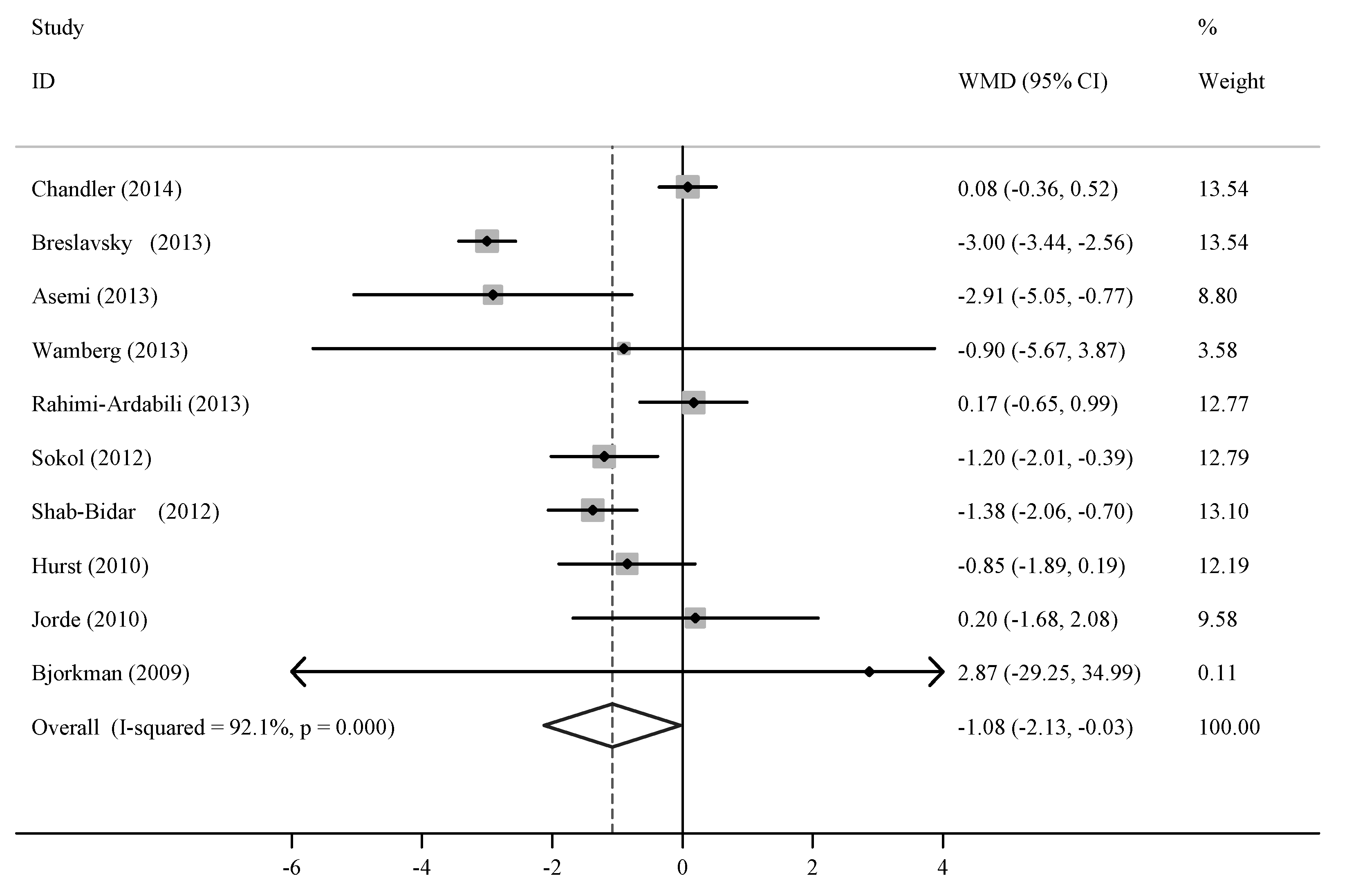
3.3. Main Analysis

{kind=link}
{kind=link}
| Author | Year | Country | Status | Age (years) | BMI (kg/m2) | Sample Size | Baseline Serum Level | Vitamin D (IU/day) | Duration (week) | Jadad Scores | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | 25(OH) D (nmol/L) | hs-CRP (mg/L) | |||||||||
| Chandler [13] | 2014 | USA | Healthy black adults | 51.0 (30–80) | 31.0 | 78 | 71 | NR | 2.48 | 4000 | 12 | 4 |
| Asemi [14] | 2013 | Iran | Healthy pregnant women | 25.1 (18–35) | 25.2 | 24 | 24 | 40.5 | 5.75 | 400 | 9 | 5 |
| Breslavsky [15] | 2013 | Israel | Type 2 diabetes patients | 66.3 | 29.3 | 19 | 13 | 29.8 | 5.00 | 1000 | 48 | 4 |
| Rahimi-Ardabili [16] | 2013 | Iran | Polycystic ovary syndrome women | 26.9 (20–40) | 28.7 | 24 | 26 | 18.5 | 1.71 | 2500 | 8 | 5 |
| Wamberg [17] | 2013 | Denmark | Obese adults | 40.4 (18–50) | 35.5 (>30) | 22 | 21 | <50 | 7.29 | 7000 | 26 | 5 |
| Shab-Bidar [18] | 2012 | Iran | Type 2 diabetes patients | 30–60 | NR | 50 | 50 | NR | 1.80 | 1000 | 12 | 2 |
| Sokol [19] | 2012 | USA | Coronary artery disease patients | 56.0 | 30.3 | 45 | 45 | <50 | 22.00 | 7143 | 12 | 5 |
| Jorde [20] | 2010 | Norway | Overweight outpatients | 47.0 | 34.3 (28–47) | 104 | 105 | 56.0 | 2.50 | 5741 | 48 | 2 |
| Von Hurst [21] | 2010 | New Zealand | Insulin-resistant women | 41.7 | 27.5 | 42 | 39 | <50 | 2.45 | 4000 | 24 | 5 |
| Bjorkman [22] | 2009 | Finland | Bedridden elderly inpatients | 84.5 (>65) | NR | 63 | 59 | 23.0 | 10.86 | 1200 | 24 | 4 |

3.4. Subgroup and Sensitivity Analyses
| Group | No | Net Change (95% CI) | P-heterogeneity | I2 (%) | P-intergroup |
|---|---|---|---|---|---|
| Total | 10 | −1.08 (−2.13, −0.03) | <0.001 | 92.1 | - |
| Baseline hs-CRP | - | - | - | - | 0.023 |
| ≥5 mg/L | 5 | −2.21 (−3.50, −0.92) | 0.004 | 73.8 | - |
| <5 mg/L | 5 | −0.40 (−1.12, 0.31) | 0.004 | 73.7 | - |
| Vitamin D dosage | - | - | - | - | 0.195 |
| ≥4000 IU/day | 5 | −0.49 (−1.21, 0.23) | 0.060 | 55.4 | - |
| <4000 IU/day | 5 | −1.69 (−3.27, −0.12) | <0.001 | 92.1 | - |
| Intervention duration | - | - | - | - | 0.559 |
| ≥24 weeks | 5 | −1.31 (−3.08 to 0.46) | <0.001 | 82.7 | - |
| <24 weeks | 5 | −0.80 (−1.65 to 0.05) | <0.001 | 82.9 | - |
3.5. Meta-Regression Analysis
3.6. Publication Bias
4. Discussion
Acknowledgments
Conflicts of Interest
References
- McGreevy, C.; Williams, D. New insights about vitamin D and cardiovascular disease. Ann. Int. Med. 2011, 155, 820–826. [Google Scholar] [CrossRef]
- Rifai, N.; Ridker, P.M. High-Sensitivity C-reactive protein: A novel and promising marker of coronary heart disease. Clin. Chem. 2001, 47, 403–411. [Google Scholar]
- De Ferranti, S.D.; Rifai, N. C-reactive protein: A nontraditional serum marker of cardiovascular risk. Cardiovasc. Pathol. 2007, 16, 14–21. [Google Scholar] [CrossRef]
- Kaptoge, S.; di Angelantonio, E.; Pennells, L.; Wood, A.M.; White, I.R.; Gao, P.; Walker, M.; Thompson, A.; Sarwar, N.; Caslake, M.; et al. C-reactive protein, fibrinogen, and cardiovascular disease prediction. N. Eng. J. Med. 2012, 367, 1310–1320. [Google Scholar] [CrossRef] [Green Version]
- Guillot, X.; Semerano, L.; Saidenberg-Kermanac’h, N.; Falgarone, G.; Boissier, M.C. Vitamin D and inflammation. Joint Bone Spine 2010, 77, 552–557. [Google Scholar] [CrossRef]
- Zanetti, M.; Harris, S.S.; Dawson-Hughes, B. Ability of vitamin D to reduce inflammation in adults without acute illness. Nutr. Rev. 2014, 72, 95–98. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Whitlock, R.P.; Chan, S.; Devereaux, P.J.; Sun, J.; Rubens, F.D.; Thorlund, K.; Teoh, K.H. Clinical benefit of steroid use in patients undergoing cardiopulmonary bypass: A meta-analysis of randomized trials. Eur. Heart J. 2008, 29, 2592–2600. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N.P. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Chandler, P.D.; Scott, J.B.; Drake, B.F.; Ng, K.; Manson, J.E.; Rifa, N.; Chan, A.T.; Bennett, G.G.; Hollis, B.W.; Giovannucci, E.L.; et al. Impact of vitamin D supplementation on inflammatory markers in African Americans: Results of a four-arm, randomized, placebo-controlled trial. Cancer Prev. Res. 2014, 7, 218–225. [Google Scholar] [CrossRef]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Vitamin D supplementation affects serum high-sensitivity C-reactive protein, insulin resistance, and biomarkers of oxidative stress in pregnant women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef]
- Breslavsky, A.; Frand, J.; Frand, Z.; Boaz, M.; Barnea, Z.; Shargorodsky, M. Effect of high doses of vitamin D on arterial properties, adiponectin, leptin and glucose homeostasis in type 2 diabetic patients. Clin. Nutr. 2013, 32, 970–975. [Google Scholar] [CrossRef]
- Rahimi-Ardabili, H.; Pourghassem, G.B.; Farzadi, L. Effects of vitamin D on cardiovascular disease risk factors in polycystic ovary syndrome women with vitamin D deficiency. J. Endocrinol. Investig. 2013, 36, 28–32. [Google Scholar]
- Wamberg, L.; Kampmann, U.; Stødkilde-Jørgensen, H.; Rejnmark, L.; Pedersen, S.B.; Richelsen, B. Effects of vitamin D supplementation on body fat accumulation, inflammation, and metabolic risk factors in obese adults with low vitamin D levels—Results from a randomized trial. Eur. J. Int. Med. 2013, 24, 644–649. [Google Scholar] [CrossRef]
- Shab-Bidar, S.; Neyestani, T.R.; Djazayery, A.; Eshraghian, M.R.; Houshiarrad, A.; Kalayi, A.; Shariatzadeh, N.; Khalaji, N.; Gharavi, A. Improvement of vitamin D status resulted in amelioration of biomarkers of systemic inflammation in the subjects with type 2 diabetes. Diabetes Metab. Res. Rev. 2012, 28, 424–430. [Google Scholar] [CrossRef]
- Sokol, S.I.; Srinivas, V.; Crandall, J.P.; Kim, M.; Tellides, G.; Lebastchi, A.H.; Yu, Y.; Gupta, A.K.; Alderman, M.H. The effects of vitamin D repletion on endothelial function and inflammation in patients with coronary artery disease. Vasc. Med. 2012, 17, 394–404. [Google Scholar] [CrossRef]
- Jorde, R.; Sneve, M.; Torjesen, P.A.; Figenschau, Y.; Gøransson, L.G.; Omdal, R. No effect of supplementation with cholecalciferol on cytokines and markers of inflammation in overweight and obese subjects. Cytokine 2010, 50, 175–180. [Google Scholar] [CrossRef]
- Von Hurst, P.R.; Stonehouse, W.; Coad, J. Vitamin D supplementation reduces insulin resistance in South Asian women living in New Zealand who are insulin resistant and vitamin D deficient—A randomized, placebo-controlled trial. Br. J. Nutr. 2010, 103, 549–555. [Google Scholar] [CrossRef]
- Bjorkman, M.P.; Sorva, A.J.; Tilvis, R.S. C-reactive protein and fibrinogen of bedridden older patients in a six-month vitamin D supplementation trial. J. Nutr. Health Aging 2009, 13, 435–439. [Google Scholar] [CrossRef]
- Agrawal, A.; Cha-Molstad, H.; Samols, D.; Kushner, I. Overexpressed nuclear factor-kappaB can participate in endogenous C-reactive protein induction, and enhances the effects of C/EBPbeta and signal transducer and activator of transcription-3. Immunology 2003, 108, 539–547. [Google Scholar] [CrossRef]
- Cohen-Lahav, M.; Shany, S.; Tobvin, D.; Chaimovitz, C.; Douvdevani, A. Vitamin D decreases NFκB activity by increasing IkappaBalpha levels. Nephrol. Dial. Transplant. 2006, 21, 889–897. [Google Scholar]
- Song, Y.; Hong, J.; Liu, D.; Lin, Q.; Lai, G. 1,25-Dihydroxyvitamin D3 inhibits nuclear factor kappa B activation by stabilizing inhibitor IκBα via mRNA stability and reduced phosphorylation in passively sensitized human airway smooth muscle cells. Scand. J. Immunol. 2013, 77, 109–116. [Google Scholar]
- Wang, Q.; Li, H.; Xie, H.; Fu, M.; Guo, B.; Ding, Y.; Li, W.; Yu, H. 25-Hydroxyvitamin D3 attenuates experimental periodontitis through downregulation of TLR4 and JAK1/STAT3 signaling in diabetic mice. J. Steroid Biochem. Mol. Biol. 2013, 135, 43–50. [Google Scholar] [CrossRef]
- Ngo, D.T.; Sverdlov, A.L.; McNeil, J.J.; Horowitz, J.D. Does vitamin D modulate asymmetric dimethylarginine and C-reactive protein concentrations? Am. J. Med. 2010, 123, 335–341. [Google Scholar] [CrossRef]
- Bellia, A.; Garcovich, C.; D’Adamo, M.; Lombardo, M.; Tesauro, M.; Donadel, G.; Gentileschi, P.; Lauro, D.; Federici, M.; Lauro, R.; et al. Serum 25-hydroxyvitamin D levels are inversely associated with systemic inflammation in severe obese subjects. Int. Emerg. Med. 2013, 8, 33–40. [Google Scholar] [CrossRef]
- Amer, M.; Qayyum, R. Relation between serum 25-hydroxyvitamin D and C-reactive protein in asymptomatic adults (from the continuous National Health and Nutrition Examination Survey 2001 to 2006). Am. J. Cardiol. 2012, 109, 226–230. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A global perspective for health. Dermatoendocrinology 2013, 5, 51–108. [Google Scholar] [CrossRef]
- DRI Tables Food and Nutrition Information Center. Available online: https://fnic.nal.usda.gov/dietary-guidance/dietary-reference-intakes/dri-tables (accessed on 17 March 2014).
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Romagnoli, E.; Pepe, J.; Piemonte, S.; Cipriani, C.; Minisola, S. Management of endocrine disease: Value and limitations of assessing vitamin D nutritional status and advised levels of vitamin D supplementation. Eur. J. Endocrinol. 2013, 169, R59–R69. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chen, N.; Wan, Z.; Han, S.-F.; Li, B.-Y.; Zhang, Z.-L.; Qin, L.-Q. Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2014, 6, 2206-2216. https://doi.org/10.3390/nu6062206
Chen N, Wan Z, Han S-F, Li B-Y, Zhang Z-L, Qin L-Q. Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2014; 6(6):2206-2216. https://doi.org/10.3390/nu6062206
Chicago/Turabian StyleChen, Neng, Zhongxiao Wan, Shu-Fen Han, Bing-Yan Li, Zeng-Li Zhang, and Li-Qiang Qin. 2014. "Effect of Vitamin D Supplementation on the Level of Circulating High-Sensitivity C-Reactive Protein: A Meta-Analysis of Randomized Controlled Trials" Nutrients 6, no. 6: 2206-2216. https://doi.org/10.3390/nu6062206