Glycemic Response of a Carbohydrate-Protein Bar with Ewe-Goat Whey

 ,
,  and
and
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Anthropometric and Physiological Measurement

{kind=link}
| Characteristics | n = 9 |
|---|---|
| Age (years) | 23.3 ± 3.9 |
| Height (cm) | 176.4 ± 13.0 |
| Weight (kg) | 75.8 ± 17.7 |
| Body Mass Index (kg/m2) | 24.2 ± 4.1 |
| Body Fat (%) | 18.6 ± 10.0 |
| Hydration (%) | 56.3 ± 6.7 |
| Waist/Hip ratio | 0.8 ± 0.0 |
| Systolic Blood Pressure (mmHg) | 113.9 ± 13.4 |
| Diastolic Blood Pressure (mmHg) | 74.2 ± 7.1 |
| Resting Heart Rate (beats·min−1) | 71.2 ± 4.8 |
2.3. Study Design
2.4. Standard and Test Food
| Nutritional Analysis Variables | Per 100 g | Per Portion 70 g | Daily Dietary Values % (70 g) |
|---|---|---|---|
| Energy (kcal) | 409.1 | 286.3 | 14.3 |
| Protein (g) | 30.8 | 21.6 | 43.2% |
| Whey protein (g) | 14.3 | 10.01 | 43.2% |
| Total Carbohydrate (g) | 30.2 | 21.1 | 7.7% |
| Sugar (g) | 19.7 | 13.8 | 15.5% |
| Fiber (g) | 5.2 | 3.6 | 13.1% |
| Fat (g) | 15.6 | 10.9 | 15.9% |
| Saturated Fat (g) | 7.0 | 4.9 | 21.2% |
| Unsaturated Fat (g) | 8.6 | 6.0 | - |
| Polyols (g) | 6.0 | 4.2 | - |
| Sodium × 2.5 (mg) | 52 | 36.4 | 3.9% |
| Potassium (mg) | 27.5 | 19.2 | - |
2.5. Blood Collection and Analyses
2.6. Dietary Analyses
2.7. Calculation of GI-Statistical Analyses
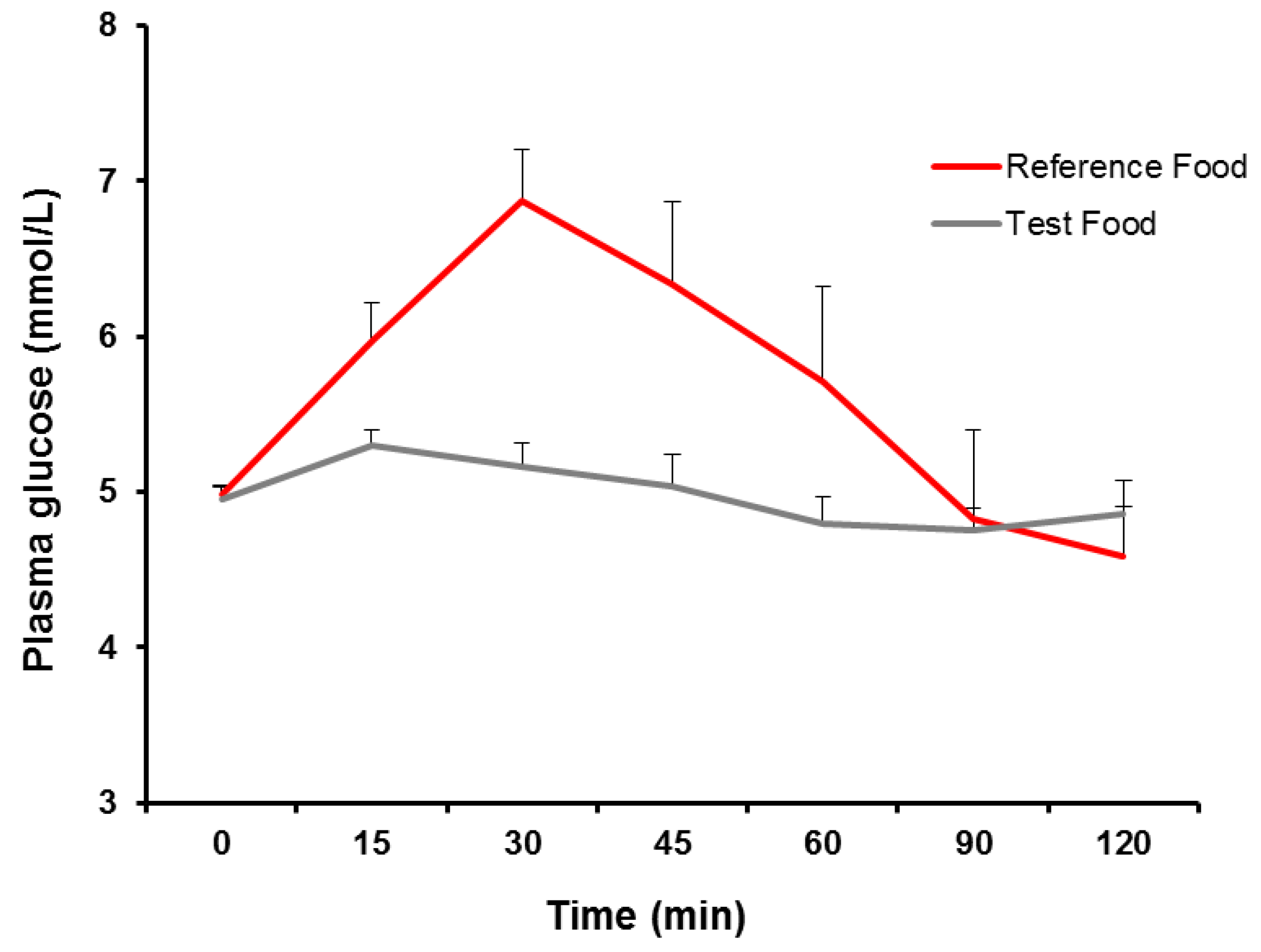
3. Results
| Complete Blood Count Variables | Standard Food | Test Food | Normal Range |
|---|---|---|---|
| White Blood Cells (103/μL) | 6.4 ± 1.4 | 6.2 ± 1.0 | 4.0–12.0 |
| Lymphocytes (103/μL) | 2.4 ± 0.7 | 2.4 ± 0.2 | 1.0–5.0 |
| Mononuclear Cells (103/μL) | 0.6 ± 0.2 | 0.6 ± 0.1 | 0.1–1.0 |
| Granulocytes (103/μL) | 3.4 ± 0.9 | 3.2 ± 0.9 | 2.0–8.0 |
| Lymphocytes (%) | 36.7 ± 6.5 | 39.4 ± 6.6 | 25.0–50.0 |
| Monocytes (%) | 10.3 ± 2.7 | 9.5 ± 1.8 | 2.0–10.0 |
| Granulocytes (%) | 53.0 ± 5.8 | 51.1 ± 7.3 | 50.0–80.0 |
| Red Blood Cells (106/μL) | 4.7 ± 0.7 | 4.7 ± 0.5 | 4.0–6.2 |
| Hemoglobin (g/dL) | 12.9 ± 1.4 | 13.5 ± 1.5 | 11.0–18.0 |
| Hematocrit (%) | 38.7 ± 3.3 | 40.1 ± 3.0 | 35.0–55.0 |
| Mean Corpuscular Volume (μm3) | 84.2 ± 12.6 | 86.8 ± 11.0 | 80.0–100.0 |
| Average Amount of Hemoglobin in Red (Pg) | 28.1 ± 4.5 | 29.3 ± 4.3 | 26.0–34.0 |
| Mean Corpuscular Hemoglobin Concentration (g/dL) | 33.3 ± 0.9 | 33.7 ± 1.4 | 31.0–3.5 |
| Erythrocyte Distribution Width (%) | 12.4 ± 1.4 | 11.9 ± 1.3 | 10.0–16.0 |
| Platelets (103/μL) | 243.1 ± 34.2 | 232.4 ± 47.5 | 150–400 |
| Mean Platelet Volume (μm3) | 8.8 ± 0.3 | 8.8 ± 0.3 | 7.0–11.0 |
| Platelet Count (%) | 0.2 ± 0.0 | 0.2 ± 0.0 | 0.2–0.5 |
| Platelet Distribution Width (%) | 16.1 ± 4.6 | 16.4 ± 4.7 | 10.0–18.0 |

4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Diplock, A.T.; Aggett, P.J.; Ashwell, M.; Bornet, F.; Fern, E.B.; Roberfroid, M.B. Scientific concepts of functional foods in Europe: Concensus document. Br. J. Nutr. 1999, 81, S1–S27. [Google Scholar] [CrossRef]
- Hasler, C.M.; Brown, A.C.; American Dietetic Association. Position of the American dietetic association: Functional foods. J. Am. Diet. Assoc. 2009, 109, 735–746. [Google Scholar] [CrossRef]
- Mitchell, H.L. The glycemic index concept in action. Am. J. Clin. Nutr. 2008, 87, 244S–246S. [Google Scholar]
- Blaak, E.E.; Antoine, J.M.; Benton, D.; Björck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; et al. Impact of postprandial glycaemia on health and prevention of disease. Obes. Rev. 2012, 13, 923–984. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Hulshof, T.; Howlett, J. Glycemic response and health—A systematic review and meta-analysis: Relations between dietary glycemic properties and health outcomes. Am. J. Clin. Nutr. 2008, 87, 258S–268S. [Google Scholar]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar]
- De Rougemont, A.; Normand, S.; Nazare, J.A.; Skilton, M.R.; Sothier, M.; Vinoy, S.; Laville, M. Beneficial effects of a 5-week low-glycaemic index regimen on weight control and cardiovascular risk factors in overweight non-diabetic subjects. Br. J. Nutr. 2007, 98, 1288–1298. [Google Scholar]
- Thomas, D.; Elliot, E.J.; Baur, L. Low glycaemic index or low glycaemic load diets for overweight and obesity. Cochrane Database Syst. Rev. 2007, 18, CD005105. [Google Scholar]
- Brand-Miller, J.C.; Hayne, S.; Petocz, P.; Colagiuri, S. Low glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Gandini, S.; la Vechia, C.; Maisonneuve, P. Glycemic index, glycemic load, and cancer risk: A meta-analysis. Am. J. Clin. Nutr. 2008, 87, 1793–1801. [Google Scholar]
- Roberts, S.B. High-glycemic index foods, hunger, and obesity: Is there a connection? Nut. Rev. 2000, 58, 163–169. [Google Scholar] [CrossRef]
- Brand-Miller, J.; McMillan-Price, J.; Steinbec, K.; Caterson, I. Dietary glycemic index: Health implications. J. Am. Coll. Nutr. 2009, 28, 446S–449S. [Google Scholar] [CrossRef]
- Brand-Miller, J.C.; Holt, S.H.; Pawlak, D.B.; McMillan, J. Glycemic index and obesity. Am. J. Clin. Nutr. 2002, 76, S281–S285. [Google Scholar]
- Marshall, K. Therapeutic applications of whey protein. Altern. Med. Rev. 2004, 9, 136–156. [Google Scholar]
- Madureira, A.R.; Claudia, C.I.; Gomes, A.M.P.; Pintado, M.E.; Malcata, X.F. Bovine whey proteins—Overview on their main biological properties. Food Res. Int. 2007, 40, 1197–1211. [Google Scholar] [CrossRef]
- Moatsou, G.; Hatzinaki, A.; Samolada, M.; Anifantakis, E. Major whey proteins in ovine and goat acid wheys from indigenous Greek breeds. Int. Dairy J. 2005, 15, 123–131. [Google Scholar] [CrossRef]
- Koutedakis, Y.; Bouziotas, C.; Flouris, A.D.; Nelson, P.N. Longitudinal modeling of adiposity in periadolescent Greek schoolchildren. Med. Sci. Sports Exerc. 2005, 37, 2070–2074. [Google Scholar]
- World Health Organization; Food and Agriculture Organization of the United Nations. Report of an FAO/WHO Expert Consultation on Carbohydrates:Carbohydrates in Human Nutrition; Food and Agriculture Organization: Rome, Italy, 1998. [Google Scholar]
- Brouns, F.; Bjorck, I.; Frayn, K.N.; Gibbs, A.L.; Lang, V.; Slama, G.; Wolever, T.M.S. Glycaemic index methodology. Nutr. Res. Rev. 2005, 18, 145–171. [Google Scholar]
- Nilsson, M.; Stenberg, M.; Frid, A.H.; Holst, J.J.; Björck, I.M. Glycemia and insulinemia in healthy subjects after lactose-equivalent meals of milk and other food proteins: The role of plasma amino acids and incretins. Am. J. Clin. Nutr. 2004, 80, 1246–1253. [Google Scholar]
- Gunnerud, U.J.; Ostman, E.M.; Björck, I.M. Effects of whey proteins on glycaemia and insulinaemia to an oral glucose load in healthy adults; a dose-response study. Eur. J. Clin. Nutr. 2013, 67, 749–753. [Google Scholar] [CrossRef]
- Frid, A.H.; Nilsson, M.; Holst, J.J.; Björck, I.M. Effect of whey on blood glucose and insulin responses to composite breakfast and lunch meals in type 2 diabetic subjects. Am. J. Clin. Nutr. 2005, 82, 69–75. [Google Scholar]
- Venter, C.S.; Vorster, H.H.; Cummings, J.H. Effects of dietary propionate on carbohydrate and lipid metabolism in healthy volunteers. Am. J. Gastroenterol. 1990, 85, 549–553. [Google Scholar]
- Solomon, T.P.J.; Haus, J.M.; Kelly, K.R.; Cook, M.D.; Filion, J.; Rocco, M.; Kashyap, S.R.; Watanabe, R.M.; Barkoukis, H.; Kirwan, J.P. A low-glycemic index diet combined with exercise reduces insulin resistance, postprandial hyperinsulinemia, and glucose-dependent insulinotropic polypeptide responses in obese, prediabetic humans. Am. J. Clin. Nutr. 2010, 92, 1359–1368. [Google Scholar] [CrossRef]
- Strachan, M.W.; Ewing, F.M.; Frier, B.M.; Harper, A.; Deary, I.J. Food cravings during acute hypoglycaemia in adults with type 1 diabetes. Physiol. Behav. 2004, 80, 675–682. [Google Scholar]
- Qi, L.; Hu, F.B. Dietary glycemic load, whole grains, and systemic inflammation in diabetes: The epidemiological evidence. Curr. Opin. Lipidol. 2007, 18, 3–8. [Google Scholar] [CrossRef]
- Luhovyy, B.L.; Akhavan, T.; Anderson, G.H. Whey proteins in the regulation of food intake and satiety. J. Am. Coll. Nutr. 2007, 26, 704S–712S. [Google Scholar] [CrossRef]
- Donaldson, C.M.; Perry, T.L.; Rose, M.C. Glycemic index and endurance performance. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 154–165. [Google Scholar]
- Jamurtas, A.Z.; Tofas, T.; Fatouros, I.; Nikolaidis, M.G.; Paschalis, V.; Yfanti, C.; Raptis, S.; Koutedakis, Y. The effects of low and high glycemic index foods on exercise performance and beta-endorphin responses. JISSN 2011, 8. [Google Scholar] [CrossRef]
- Stevenson, E.; McComb, G.; Oram, C.; Williams, C. Improved recovery from prolonged exercise following the consumption of low glycemic index carbohydrate meals. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 333–349. [Google Scholar]
- Watanabe, A.; Okada, K.; Shimizu, Y.; Wakabayashi, H.; Higuchi, K.; Niiya, K.; Kuwabara, Y.; Yasuyama, T.; Ito, H.; Tsukishiro, T.; et al. Nutritional therapy of chronic hepatitis by whey protein (non-heated). J. Med. 2000, 31, 283–302. [Google Scholar]
- Bounous, G. Whey protein concentrate (WPC) and glutathione modulation in cancer treatment. Anticancer Res. 2000, 20, 4785–4792. [Google Scholar]
- Aoe, S.; Toba, Y.; Yamamura, J.; Kawakami, H.; Yahiro, M.; Kumegawa, M.; Itabashi, A.; Takada, Y. Controlled trial of the effects of milk basic protein (MBP) supplementation on bone metabolism in healthy adult women. Biosci. Biotechnol. Biochem. 2001, 65, 913–918. [Google Scholar] [CrossRef]
- Ha, E.; Zemel, M.B. Functional properties of whey, whey components, and essential amino acids: Mechanisms underlying health benefits for active people. J. Nutr. Biochem. 2003, 14, 251–258. [Google Scholar] [CrossRef]
- Anthony, J.C.; Anthony, T.G.; Kimball, S.R.; Jefferson, L.S. Signaling pathways involved in translational control of protein synthesis in skeletal muscle by leucine. J. Nutr. 2001, 131, 856S–860S. [Google Scholar]
- Parry-Billings, M.; Budgett, R.; Koutedakis, Y.; Blomstrand, E.; Brooks, S.; Williams, C.; Calder, P.C.; Pilling, S.; Baigrie, R.; Newsholme, E.A. Plasma amino acid concentrations in the overtraining syndrome: Possible effects on the immune system. Med. Sci. Sports Exerc. 1992, 24, 1353–1358. [Google Scholar]
- Kerasioti, E.; Kiskini, A.; Veskoukis, A.; Jamurtas, A.; Tsitsimpikou, C.; Tsatsakis, A.M.; Koutedakis, Y.; Stagos, D.; Kouretas, D.; Karathanos, V. Effect of special carbohydrate-protein cake on oxidative stress markers after exhaustive cycling in humans. Food Chem. Toxicol. 2012, 50, 2805–2810. [Google Scholar] [CrossRef]
- Kerasioti, E.; Stagos, D.; Jamurtas, A.; Kiskini, A.; Koutedakis, Y.; Goutzourelas, N.; Pournaras, S.; Tsatsakis, A.M.; Kouretas, D. Anti-inflammatory effects of special carbohydrate-protein cake after exhaustive cycling in humans. Food Chem. Toxicol. 2013, 61, 42–46. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Manthou, E.; Kanaki, M.; Georgakouli, K.; Deli, C.K.; Kouretas, D.; Koutedakis, Y.; Jamurtas, A.Z. Glycemic Response of a Carbohydrate-Protein Bar with Ewe-Goat Whey. Nutrients 2014, 6, 2240-2250. https://doi.org/10.3390/nu6062240
Manthou E, Kanaki M, Georgakouli K, Deli CK, Kouretas D, Koutedakis Y, Jamurtas AZ. Glycemic Response of a Carbohydrate-Protein Bar with Ewe-Goat Whey. Nutrients. 2014; 6(6):2240-2250. https://doi.org/10.3390/nu6062240
Chicago/Turabian StyleManthou, Eirini, Maria Kanaki, Kalliopi Georgakouli, Chariklia K. Deli, Dimitrios Kouretas, Yiannis Koutedakis, and Athanasios Z. Jamurtas. 2014. "Glycemic Response of a Carbohydrate-Protein Bar with Ewe-Goat Whey" Nutrients 6, no. 6: 2240-2250. https://doi.org/10.3390/nu6062240