Resveratrol Increases Nephrin and Podocin Expression and Alleviates Renal Damage in Rats Fed a High-Fat Diet

Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Research Design, Diet and Resveratrol Treatment
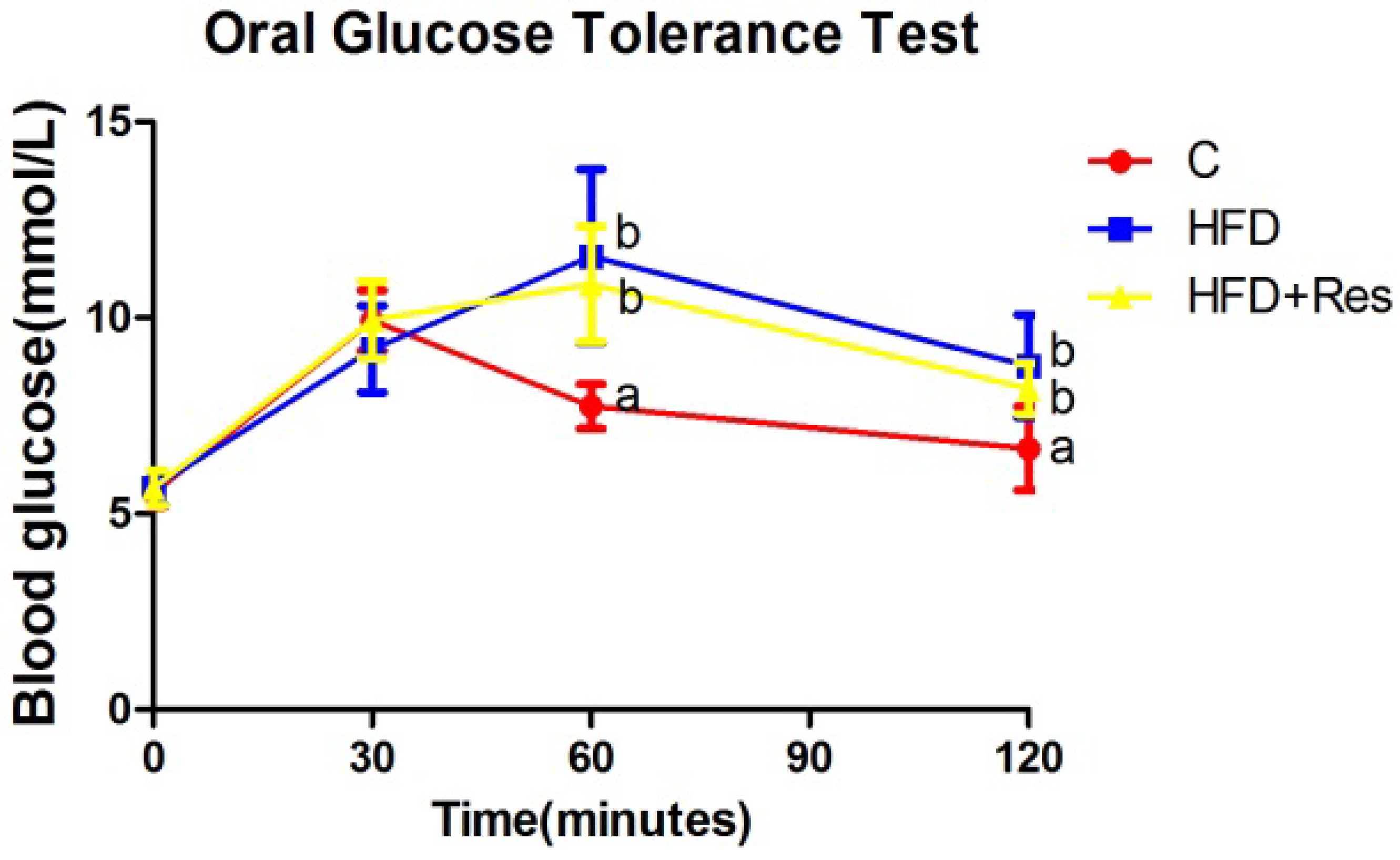
2.3. Oral Glucose Tolerance Test (OGTT)
2.4. Biochemical Analysis
2.5. Assessment of Renal Function
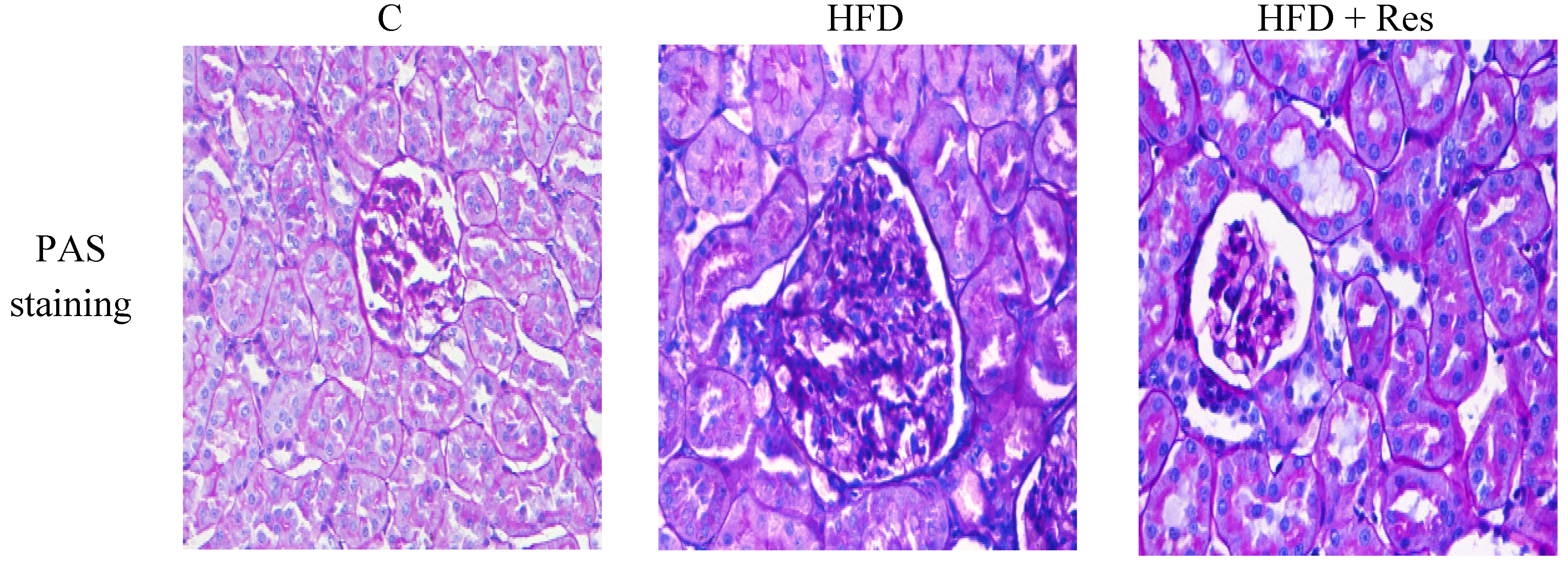
2.6. Renal Histological Analysis
2.7. NF-κB DNA-Binding Activity, SOD Activity, and MDA Level in Kidney
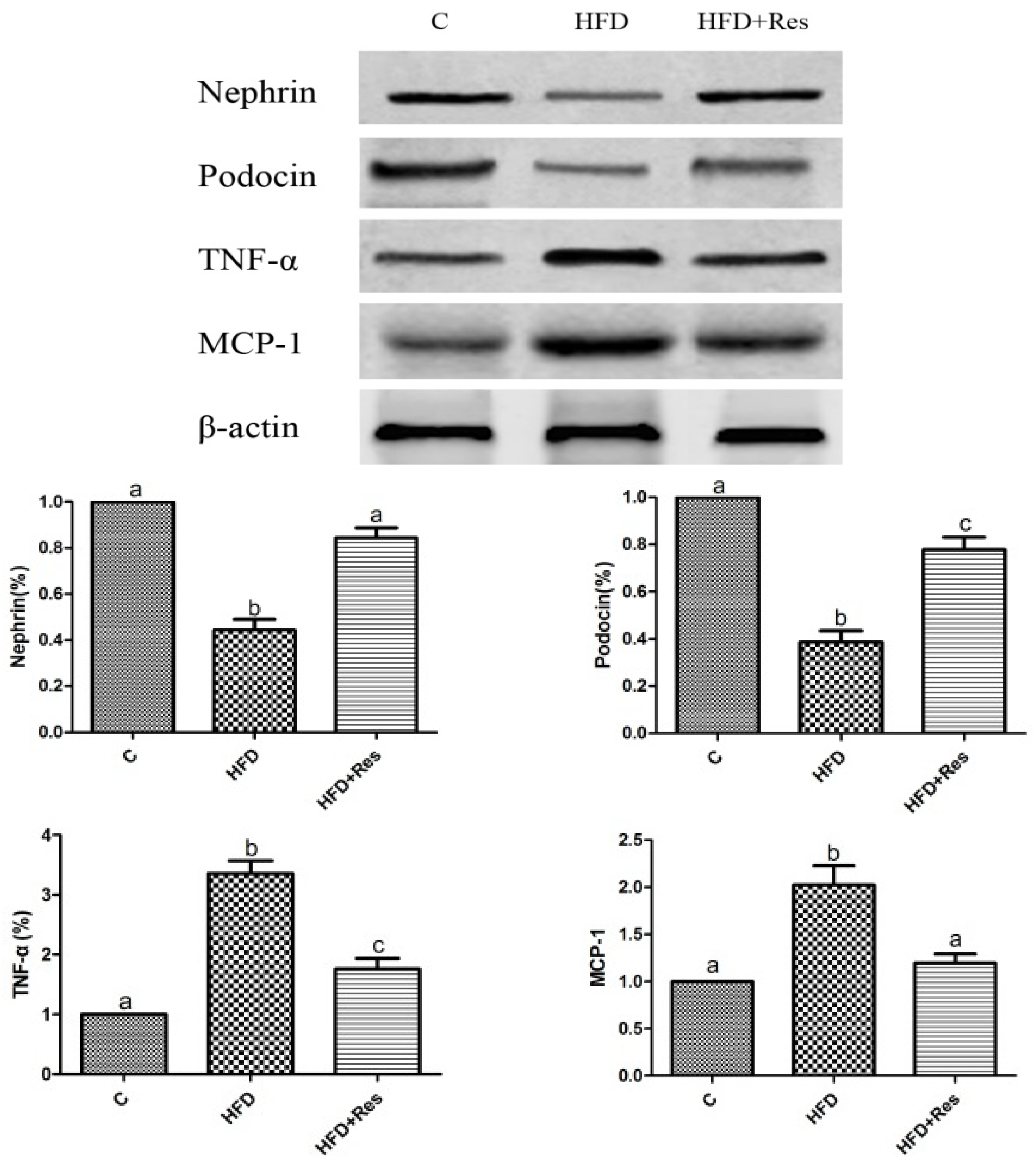
2.8. Western Blot
2.9. Statistical Analyses
3. Results
3.1. Effects of Resveratrol on Body Weight, Kidney Weight, and Omental and Epididymal Fat Weights

{kind=link}
{kind=link}
{kind=link}
| Parameters | C | HFD | HFD + Res | p value | |
|---|---|---|---|---|---|
| HFD vs. C | HFD + Res vs. HFD | ||||
| Initial body weight (g) | 189.98 ± 6.58 | 187.89 ± 7.69 | 189.2 ± 7.71 | 0.53 | 0.69 |
| Final body weight (g) | 519.16 ± 31.75 a | 652.8 ± 29.66 b | 628.6 ± 17.28 b | <0.001 | 0.055 |
| Food intake at 12 weeks (g/day) | 27.2 ± 3.0 | 29.9 ± 3.3 | 28.6 ± 3.8 | 0.09 | 0.40 |
| Energy intake at 12 weeks (kcal/day) | 104.72 ± 11.55 a | 141.43 ± 15.61 b | 135.28 ± 14.97 b | <0.001 | 0.81 |
| Kidney weight (g) | 2.95 ± 0.30 a | 3.52 ± 0.41 b | 3.22 ± 0.28 b | 0.001 | 0.053 |
| Relative kidney weight (mg/mm tibial length) | 55.02 ± 2.44 a | 64.41 ± 4.46 b | 60.54 ± 4.45 b | <0.001 | 0.61 |
| Epididymal fat weight (g) | 6.20 ± 0.48 a | 15.53 ± 1.01 b | 13.74 ± 1.64 c | <0.001 | 0.002 |
| Relative epididymal fat weight (mg/mm tibial length) | 117.14 ± 11.08 a | 267.91 ± 17.05 b | 232.93 ± 24.62 c | <0.001 | 0.001 |
| Omental fat weight (g) | 3.74 ± 0.26 a | 8.06 ± 0.22 b | 7.72 ± 0.20 c | <0.001 | 0.02 |
| Relative omental fat weight (mg/mm tibial length) | 65.59 ± 3.07 a | 139.94 ± 2.4 b | 136.21 ± 3.3 c | <0.001 | 0.04 |
3.2. Effects of Resveratrol on Blood Glucose Level, Serum Lipid Level, and Insulin Resistance

| Parameters | C | HFD | HFD + Res | p value | |
|---|---|---|---|---|---|
| HFD vs. C | HFD + Res vs. HFD | ||||
| Fasting blood glucose (mmol/L) | 6.39 ± 0.42 | 6.76 ± 0.42 | 6.69 ± 0.48 | 0.07 | 0.74 |
| Fasting serum insulin (ng/mL) | 0.84 ± 0.07 a | 1.29 ± 0.11 b | 1.24 ± 0.27 b | <0.001 | 0.53 |
| HOMA-IR | 5.15 ± 0.99 a | 8.20 ± 0.33 b | 8.03 ± 0.32 b | <0.001 | 0.57 |
| OGTT(AUC) | 663.7 ± 15.97 a | 688.2 ± 16.14 b | 692.5 ± 19.31 b | 0.004 | 0.58 |
| TG (mmol/L) | 0.82 ± 0.13 a | 5.15 ± 1.23 b | 2.32 ± 0.40 c | <0.001 | <0.001 |
| TC (mmol/L) | 1.91 ± 0.17 a | 3.08 ± 0.43 b | 1.93 ± 0.24 a | <0.001 | <0.001 |
| Serum creatinine (μmol/L) | 29.69 ± 3.99 a | 36.93 ± 5.69 b | 34.53 ± 5.03 b | 0.003 | 0.29 |
| Ccr (mL/min/kg body weight) | 52.19 ± 3.72 a | 44.62 ± 2.65 b | 47.67 ± 2.07 c | <0.001 | 0.03 |
| Urinary protein excretionμg (per 24 h) | 457.55 ± 127.77 a | 1430.88 ± 359.80 b | 909.32 ± 80.07 c | <0.001 | 0.001 |
3.3. Protective Effects of Resveratrol on Proteinuria and Renal Damage Induced by HFD

| Parameters | C | HFD | HFD + Res | p value | |
|---|---|---|---|---|---|
| HFD vs. C | HFD + Res vs. HFD | ||||
| Glomerular volume (106 μm3) | 0.92 ± 0.19 a | 1.47 ± 0.31 b | 1.13 ± 0.27 c | 0.01 | 0.02 |
| ECM Accumulation (arbitrary units) | 0.074 ± 0.003 a | 0.113 ± 0.004 b | 0.098 ± 0.002 c | 0.01 | 0.01 |
3.4. Resveratrol Restored the Protein levels of Nephrin and Podocin in Kidney

3.5. Resveratrol Reduced Renal NF-κB Activity, TNF-α and MCP-1 Levels, and Alleviated Renal Oxidative Stress Induced by HFD
| Parameters | C | HFD | HFD + Res | p value | |
|---|---|---|---|---|---|
| HFD vs. C | HFD + Res vs. HFD | ||||
| Renal MDA (nmol/mg) | 4.71 ± 0.81 a | 12.20 ± 1.44 b | 7.89 ± 0.83 c | <0.001 | <0.001 |
| Renal SOD activity (U/mg) | 23.88 ± 2.74 a | 7.46 ± 1.54 b | 18.77 ± 3.23 c | <0.001 | <0.001 |
| Renal NF-κB activation assay (OD at 450 nm) | 0.35 ± 0.04 a | 1.07 ± 0.02 b | 0.64 ± 0.05 c | <0.001 | <0.001 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Vivante, A.; Golan, E.; Tzur, D.; Leiba, A.; Tirosh, A.; Skorecki, K.; Calderon-Margalit, R. Body mass index in 1.2 million adolescents and risk for end-stage renal disease. Arch. Int. Med. 2012, 172, 1644–1650. [Google Scholar] [CrossRef]
- Othman, M.; Kawar, B.; El Nahas, A.M. Influence of obesity on progression of non-diabetic chronic kidney disease: A retrospective cohort study. Nephron Clin. Pract. 2009, 113, c16–c23. [Google Scholar] [CrossRef]
- Kambham, N.; Markowitz, G.S.; Valeri, A.M.; Lin, J.; D’Agati, V.D. Obesity-related glomerulopathy: An emerging epidemic. Kidney Int. 2001, 59, 1498–1509. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Khalil, A.A. Obesity-related glomerulopathy: Another nail in the coffin of the epidemic of end-stage renal disease. J. Clin. Pathol. 2007, 60, 582. [Google Scholar] [CrossRef]
- Remuzzi, G.; Chiurchiu, C.; Ruggenenti, P. Proteinuria predicting outcome in renal disease: Nondiabetic nephropathies (REIN). Kidney Int. Suppl. 2004, 92, S90–S96. [Google Scholar]
- Gorriz, J.L.; Martinez-Castelao, A. Proteinuria: Detection and role in native renal disease progression. Transplant. Rev. (Orlando) 2012, 26, 3–13. [Google Scholar] [CrossRef]
- Miner, J.H. Glomerular basement membrane composition and the filtration barrier. Pediatr. Nephrol. 2011, 26, 1413–1417. [Google Scholar] [CrossRef]
- Wickman, L.; Afshinnia, F.; Wang, S.Q.; Yang, Y.; Wang, F.; Chowdhury, M.; Graham, D.; Hawkins, J.; Nishizono, R.; Tanzer, M.; et al. Urine podocyte mRNAs, proteinuria, and progression in human glomerular diseases. J. Am. Soc. Nephrol. 2013, 24, 2081–2095. [Google Scholar] [CrossRef]
- Chen, H.M.; Liu, Z.H.; Zeng, C.H.; Li, S.J.; Wang, Q.W.; Li, L.S. Podocyte lesions in patients with obesity-related glomerulopathy. Am. J. Kidney Dis. 2006, 48, 772–779. [Google Scholar] [CrossRef]
- Patrakka, J.; Tryggvason, K. Nephrin—A unique structural and signaling protein of the kidney filter. Trends Mol. Med. 2007, 13, 396–403. [Google Scholar] [CrossRef]
- Patari-Sampo, A.; Ihalmo, P.; Holthofer, H. Molecular basis of the glomerular filtration: Nephrin and the emerging protein complex at the podocyte slit diaphragm. Ann. Med. 2006, 38, 483–492. [Google Scholar] [CrossRef]
- Roselli, S.; Gribouval, O.; Boute, N.; Sich, M.; Benessy, F.; Attie, T.; Gubler, M.C.; Antignac, C. Podocin localizes in the kidney to the slit diaphragm area. Am. J. Pathol. 2002, 160, 131–139. [Google Scholar] [CrossRef]
- Kelly, D.J.; Aaltonen, P.; Cox, A.J.; Rumble, J.R.; Langham, R.; Panagiotopoulos, S.; Jerums, G.; Holthofer, H.; Gilbert, R.E. Expression of the slit-diaphragm protein, nephrin, in experimental diabetic nephropathy: Differing effects of anti-proteinuric therapies. Nephrol. Dial. Transplant. 2002, 17, 1327–1332. [Google Scholar] [CrossRef]
- Jim, B.; Ghanta, M.; Qipo, A.; Fan, Y.; Chuang, P.Y.; Cohen, H.W.; Abadi, M.; Thomas, D.B.; He, J.C. Dysregulated nephrin in diabetic nephropathy of type 2 diabetes: A cross sectional study. PLoS One 2012, 7, e36041. [Google Scholar] [CrossRef]
- Agrawal, V.; Prasad, N.; Jain, M.; Pandey, R. Reduced podocin expression in minimal change disease and focal segmental glomerulosclerosis is related to the level of proteinuria. Clin. Exp. Nephrol. 2013, 17, 811–818. [Google Scholar] [CrossRef]
- Khurana, S.; Venkataraman, K.; Hollingsworth, A.; Piche, M.; Tai, T.C. Polyphenols: Benefits to the cardiovascular system in health and in aging. Nutrients 2013, 5, 3779–3827. [Google Scholar] [CrossRef]
- Tang, J.; Yan, H.; Zhuang, S. Inflammation and oxidative stress in obesity-related glomerulopathy. Int. J. Nephrol. 2012, 2012, 608397. [Google Scholar] [CrossRef]
- Meydani, M.; Hasan, S.T. Dietary polyphenols and obesity. Nutrients 2010, 2, 737–751. [Google Scholar] [CrossRef]
- Szkudelski, T.; Szkudelska, K. Anti-diabetic effects of resveratrol. Ann. N. Y. Acad. Sci. 2011, 1215, 34–39. [Google Scholar] [CrossRef]
- Kim, M.Y.; Lim, J.H.; Youn, H.H.; Hong, Y.A.; Yang, K.S.; Park, H.S.; Chung, S.; Ko, S.H.; Shin, S.J.; Choi, B.S.; et al. Resveratrol prevents renal lipotoxicity and inhibits mesangial cell glucotoxicity in a manner dependent on the AMPK-SIRT1-PGC1alpha axis in db/db mice. Diabetologia 2013, 56, 204–217. [Google Scholar] [CrossRef]
- Kitada, M.; Kume, S.; Imaizumi, N.; Koya, D. Resveratrol improves oxidative stress and protects against diabetic nephropathy through normalization of Mn-SOD dysfunction in AMPK/SIRT1-independent pathway. Diabetes 2011, 60, 634–643. [Google Scholar] [CrossRef]
- Dube, M.G.; Beretta, E.; Dhillon, H.; Ueno, N.; Kalra, P.S.; Kalra, S.P. Central leptin gene therapy blocks high-fat diet-induced weight gain, hyperleptinemia, and hyperinsulinemia: Increase in serum ghrelin levels. Diabetes 2002, 51, 1729–1736. [Google Scholar] [CrossRef]
- Shetty, A.K.; Kumar, G.S.; Sambaiah, K.; Salimath, P.V. Effect of bitter gourd (Momordica charantia) on glycaemic status in streptozotocin induced diabetic rats. Plant Foods Hum. Nutr. 2005, 60, 109–112. [Google Scholar] [CrossRef]
- Kanetsuna, Y.; Hirano, K.; Nagata, M.; Gannon, M.A.; Takahashi, K.; Harris, R.C.; Breyer, M.D.; Takahashi, T. Characterization of diabetic nephropathy in a transgenic model of hypoinsulinemic diabetes. Am. J. Physiol. Renal Physiol. 2006, 291, F1315–F1322. [Google Scholar] [CrossRef]
- Charradi, K.; Elkahoui, S.; Karkouch, I.; Limam, F.; Hamdaoui, G.; Hassine, F.B.; El May, M.V.; El May, A.; Aouani, E. Grape seed and skin extract alleviates high-fat diet-induced renal lipotoxicity and prevents copper depletion in rat. Appl. Physiol. Nutr. Metab. 2013, 38, 259–267. [Google Scholar] [CrossRef]
- Ruotsalainen, V.; Ljungberg, P.; Wartiovaara, J.; Lenkkeri, U.; Kestila, M.; Jalanko, H.; Holmberg, C.; Tryggvason, K. Nephrin is specifically located at the slit diaphragm of glomerular podocytes. Proc. Natl. Acad. Sci. USA 1999, 96, 7962–7967. [Google Scholar] [CrossRef]
- Roselli, S.; Heidet, L.; Sich, M.; Henger, A.; Kretzler, M.; Gubler, M.C.; Antignac, C. Early glomerular filtration defect and severe renal disease in podocin-deficient mice. Mol. Cell. Biol. 2004, 24, 550–560. [Google Scholar] [CrossRef]
- Hildebrandt, F.; Heeringa, S.F. Specific podocin mutations determine age of onset of nephrotic syndrome all the way into adult life. Kidney Int. 2009, 75, 669–671. [Google Scholar] [CrossRef]
- Hunley, T.E.; Ma, L.J.; Kon, V. Scope and mechanisms of obesity-related renal disease. Curr. Opin. Nephrol. Hypertens. 2010, 19, 227–234. [Google Scholar] [CrossRef]
- Shibata, S.; Nagase, M.; Yoshida, S.; Kawachi, H.; Fujita, T. Podocyte as the target for aldosterone: Roles of oxidative stress and Sgk1. Hypertension 2007, 49, 355–364. [Google Scholar] [CrossRef]
- Impellizzeri, D.; Esposito, E.; Attley, J.; Cuzzocrea, S. Targeting inflammation: New therapeutic approaches in chronic kidney disease (CKD). Pharmacol. Res. 2014, 81C, 91–102. [Google Scholar]
- Gao, G.; Zhang, B.; Ramesh, G.; Betterly, D.; Tadagavadi, R.K.; Wang, W.; Reeves, W.B. TNF-alpha mediates increased susceptibility to ischemic AKI in diabetes. Am. J. Physiol. Renal Physiol. 2013, 304, F515–F521. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, Z.; Xiang, Z.; Zeng, C.; Chen, Z.; Ma, X.; Li, L. Obesity-related glomerulopathy: Insights from gene expression profiles of the glomeruli derived from renal biopsy samples. Endocrinology 2006, 147, 44–50. [Google Scholar] [CrossRef]
- Matoba, K.; Kawanami, D.; Ishizawa, S.; Kanazawa, Y.; Yokota, T.; Utsunomiya, K. Rho-kinase mediates TNF-alpha-induced MCP-1 expression via p38 MAPK signaling pathway in mesangial cells. Biochem. Biophys. Res. Commun. 2010, 402, 725–730. [Google Scholar] [CrossRef]
- Chow, F.Y.; Nikolic-Paterson, D.J.; Ma, F.Y.; Ozols, E.; Rollins, B.J.; Tesch, G.H. Monocyte chemoattractant protein-1-induced tissue inflammation is critical for the development of renal injury but not type 2 diabetes in obese db/db. Diabetologia 2007, 50, 471–480. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pan, Q.-R.; Ren, Y.-L.; Zhu, J.-J.; Hu, Y.-J.; Zheng, J.-S.; Fan, H.; Xu, Y.; Wang, G.; Liu, W.-X. Resveratrol Increases Nephrin and Podocin Expression and Alleviates Renal Damage in Rats Fed a High-Fat Diet. Nutrients 2014, 6, 2619-2631. https://doi.org/10.3390/nu6072619
Pan Q-R, Ren Y-L, Zhu J-J, Hu Y-J, Zheng J-S, Fan H, Xu Y, Wang G, Liu W-X. Resveratrol Increases Nephrin and Podocin Expression and Alleviates Renal Damage in Rats Fed a High-Fat Diet. Nutrients. 2014; 6(7):2619-2631. https://doi.org/10.3390/nu6072619
Chicago/Turabian StylePan, Qing-Rong, Yan-Long Ren, Jia-Jia Zhu, Yan-Jin Hu, Jin-Su Zheng, Hui Fan, Yuan Xu, Guang Wang, and Wen-Xian Liu. 2014. "Resveratrol Increases Nephrin and Podocin Expression and Alleviates Renal Damage in Rats Fed a High-Fat Diet" Nutrients 6, no. 7: 2619-2631. https://doi.org/10.3390/nu6072619