Assessing the Nutritional Quality of Diets of Canadian Adults Using the 2014 Health Canada Surveillance Tool Tier System


Abstract
:1. Introduction
2. Experimental Section
2.1. Data Collection and Preparation
2.2. Application of the HCST Tier System to Dietary Recalls
2.2.1. Foods Recommended in the EWCFG
2.2.2. Foods Not Recommended in the EWCFG
2.3. Definition of Compliance to the HCST Tier System
2.4. Identification of Implausible Reporters
2.5. Statistical Analyses
3. Results
3.1. Quantity of Food Consumption
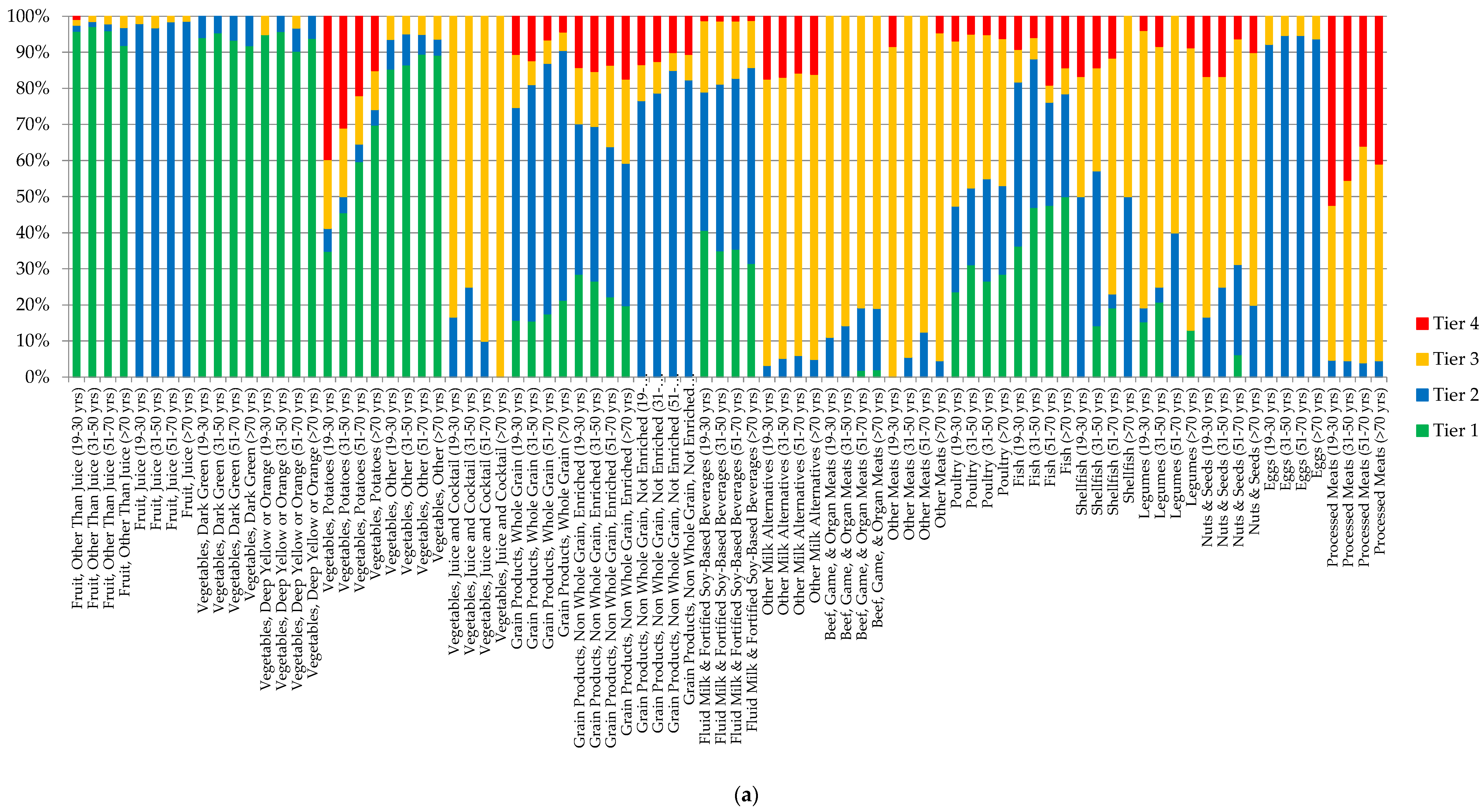
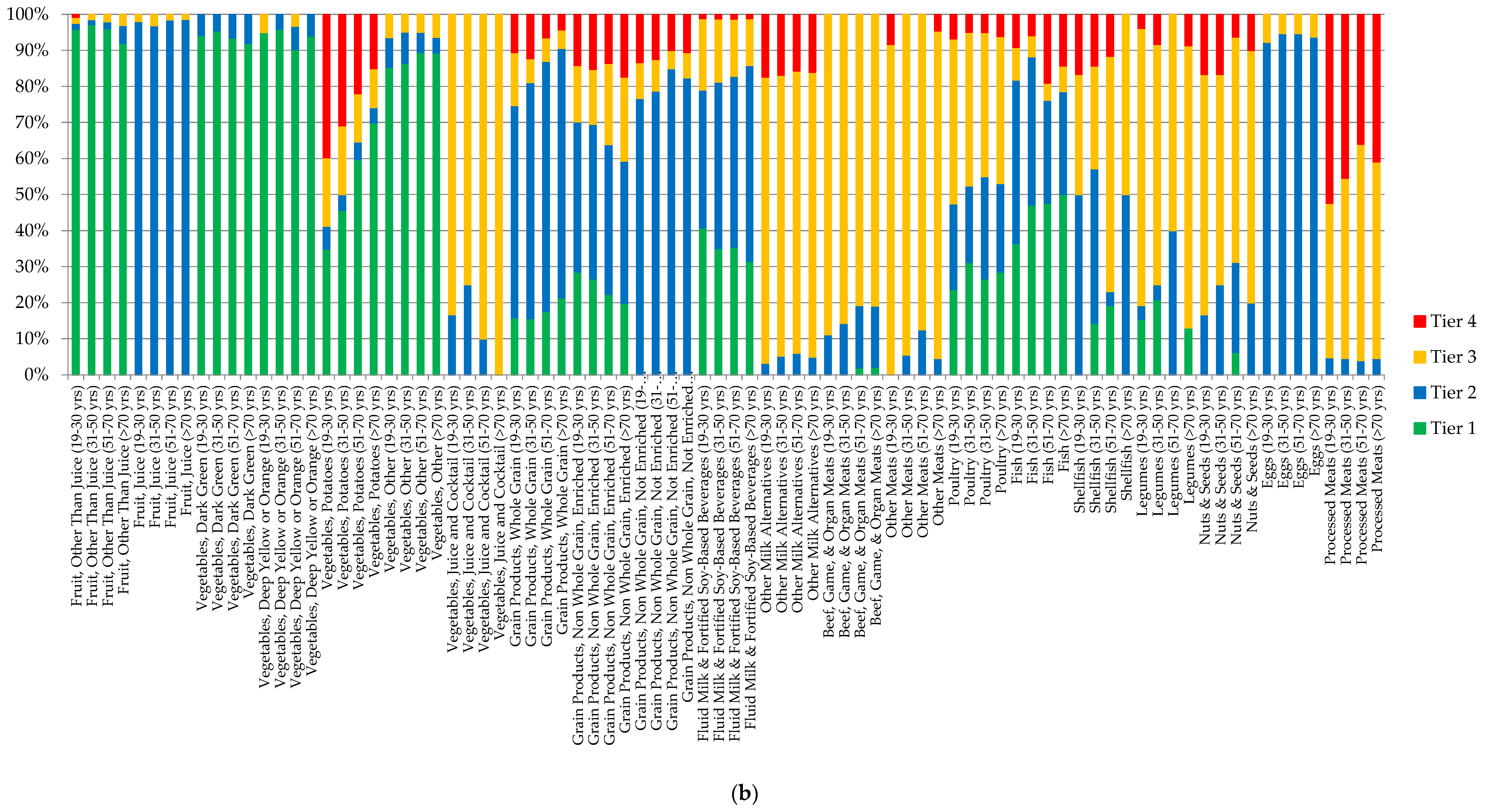
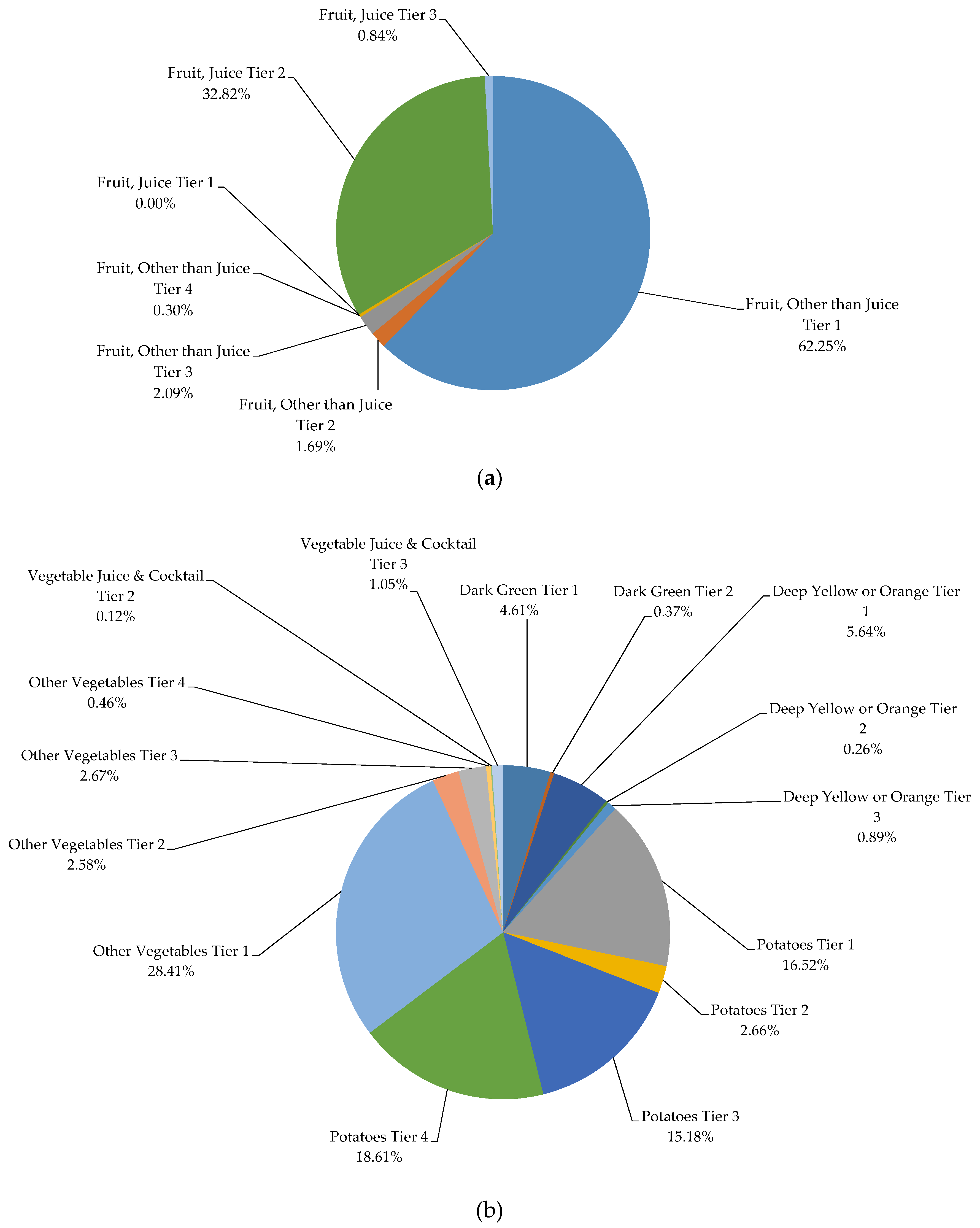
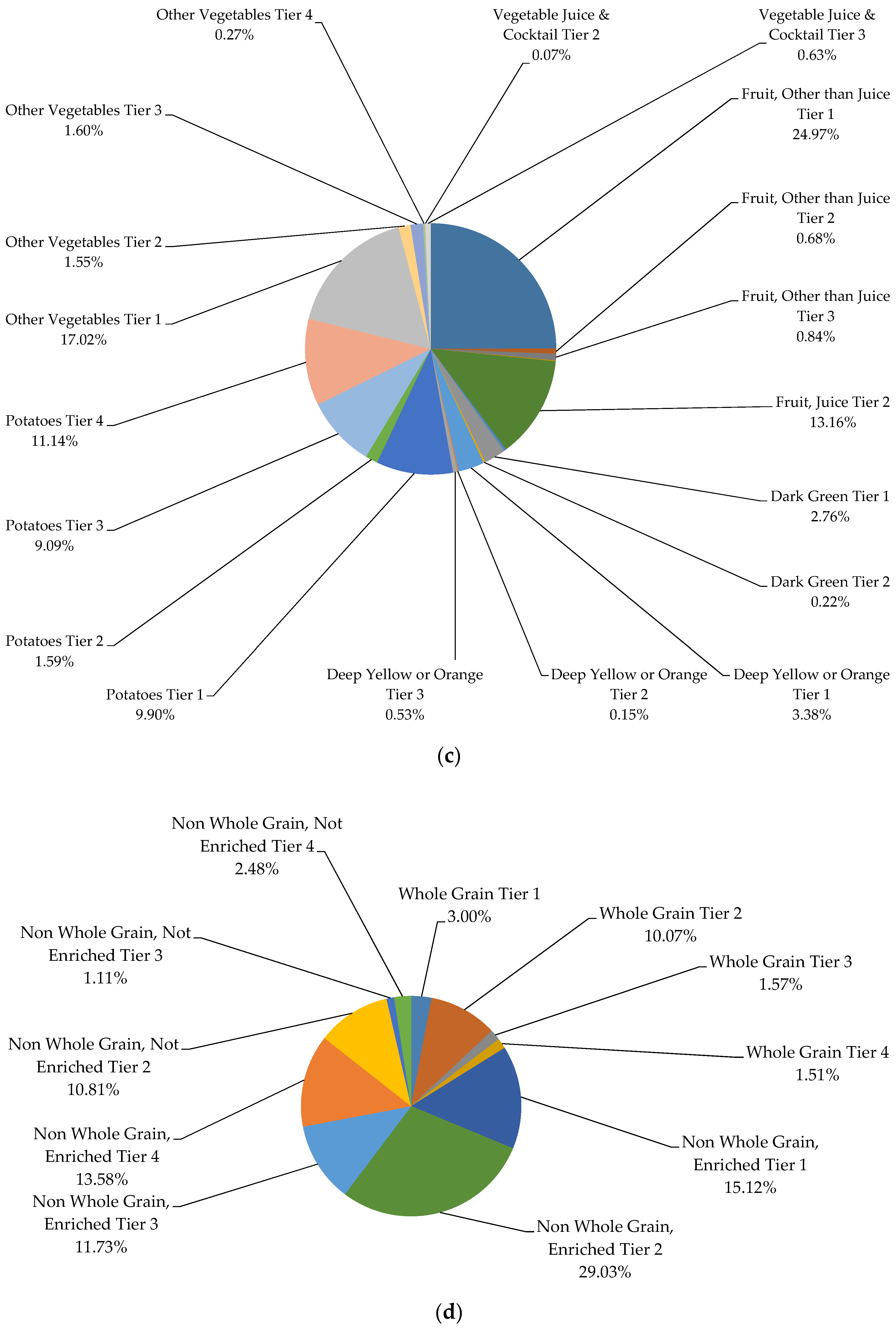
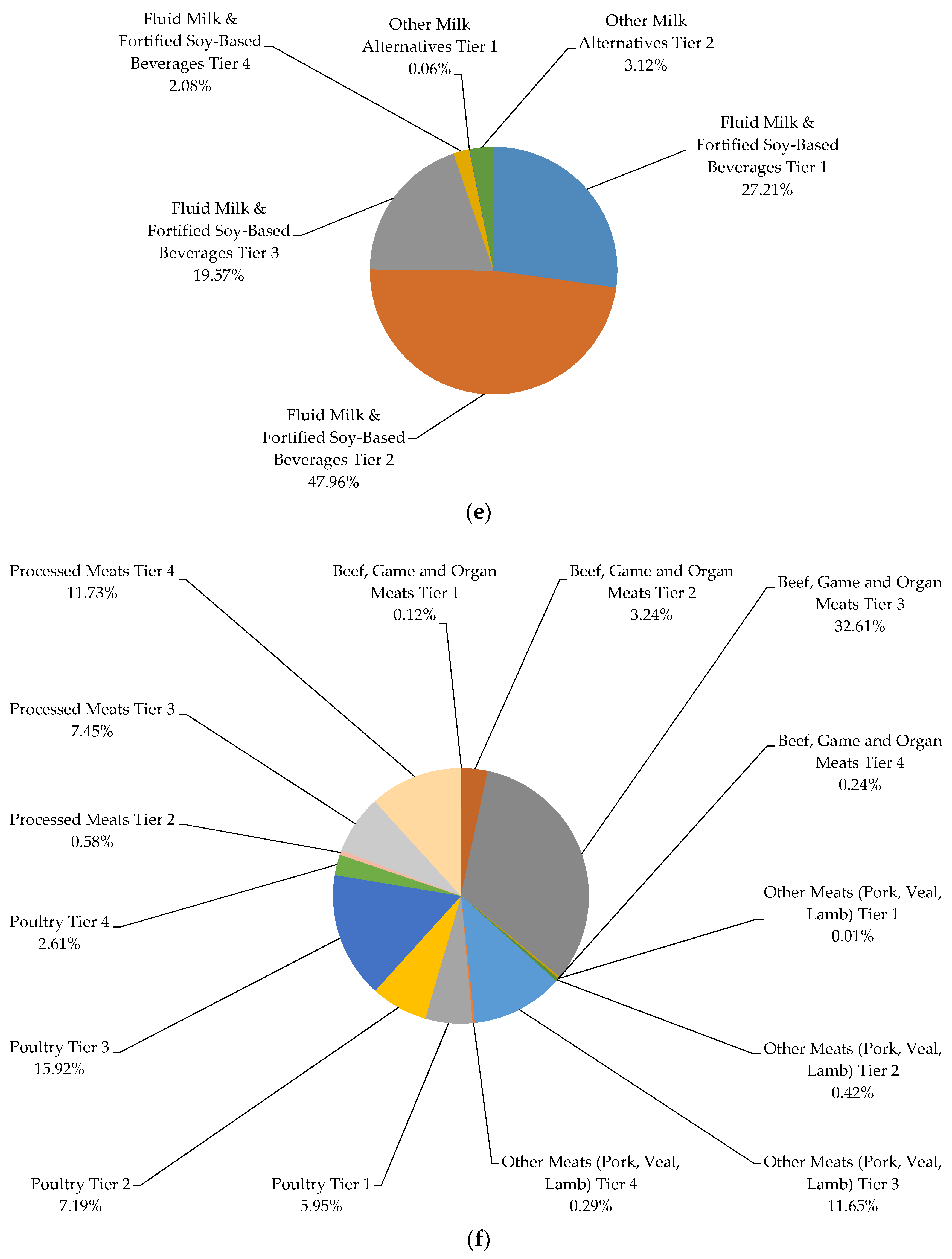
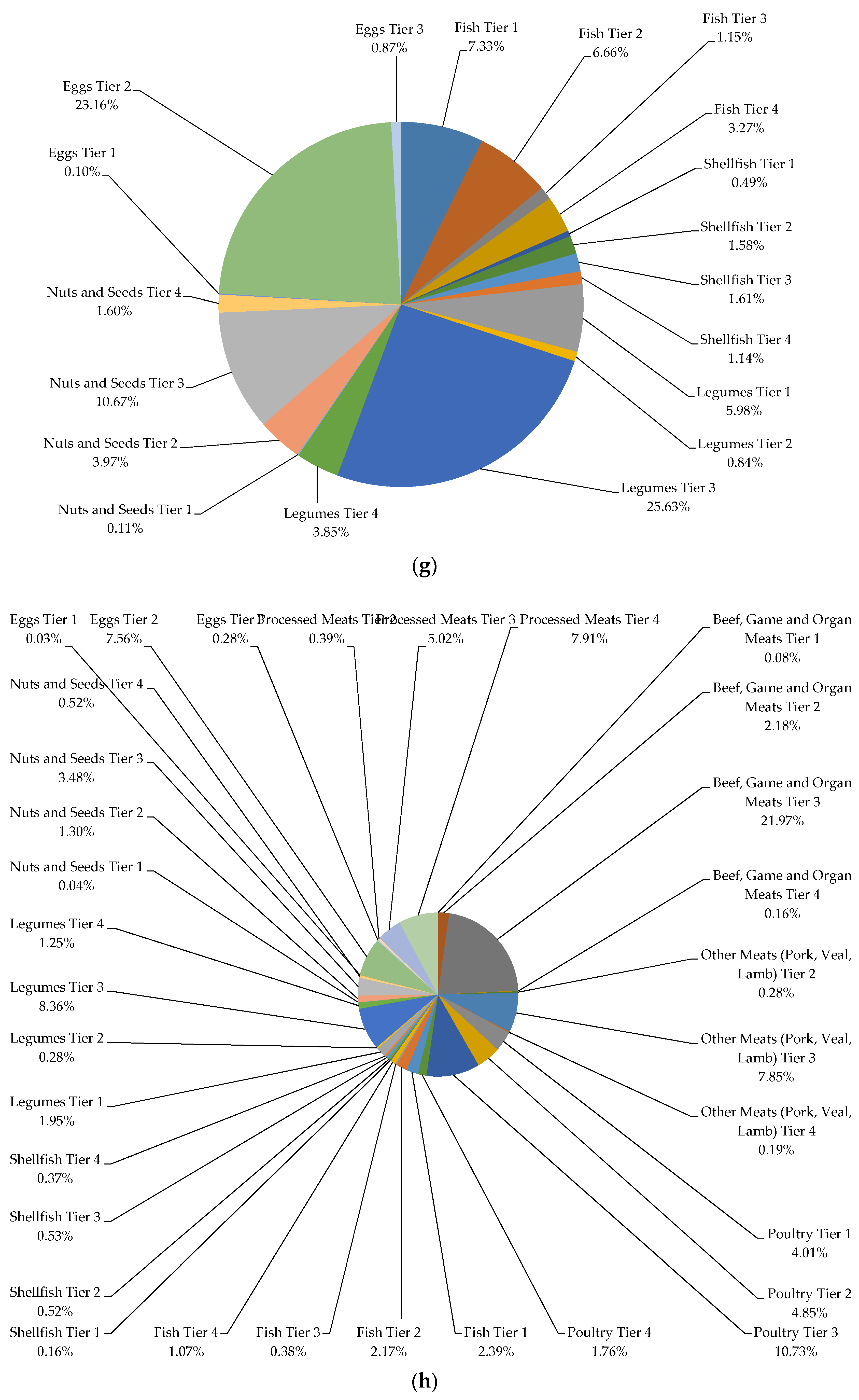
3.2. Quality of Food Consumption

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men, 19–30 Years | Women, 19–30 Years | Men, 31–50 Years | Women, 31–50 Years | Men, 51–70 Years | Women, 51–70 Years | Men, >70 Years | Women, >70 Years | |
|---|---|---|---|---|---|---|---|---|
| Food Groups (Servings/Day) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) |
| Vegetables and Fruits | ||||||||
| Tiers 1–3 | 4.35 (0.26) | 4.76 (0.19) | 4.64 (0.23) | 5.12 (0.18) | 5.56 (0.21) | 5.70 (0.14) | 5.37 (0.20) | 5.52 (0.15) |
| Tiers 1–4 | 4.57 (0.26) | 5.01 (0.18) | 4.86 (0.23) | 5.33 (0.18) | 5.71 (0.21) | 5.88 (0.14) | 5.49 (0.19) | 5.67 (0.15) |
| EWCFG Rec. | 8–10 | 7–8 | 8–10 | 7–8 | 7 | 7 | 7 | 7 |
| Grain Products | ||||||||
| Tiers 1–3 | 5.37 (0.23) | 5.03 (0.16) | 5.06 (0.17) | 4.83 (0.14) | 4.98 (0.16) | 4.99 (0.13) | 5.23 (0.19) | 5.00 (0.12) |
| Tiers 1–4 | 5.99 (0.23) | 5.81 (0.17) | 5.70 (0.18) | 5.64 (0.14) | 5.55 (0.16) | 5.66 (0.13) | 5.99 (0.21) | 5.82 (0.12) |
| EWCFG Rec. | 8 | 6–7 | 8 | 6–7 | 7 | 6 | 7 | 6 |
| Milk and Alternatives | ||||||||
| Tiers 1–3 | 1.34 (0.10) | 1.62 (0.08) | 1.17 (0.08) b | 1.58 (0.07) b | 1.23 (0.08) | 1.46 (0.06) | 1.55 (0.13) | 1.59 (0.06) |
| Tiers 1–4 | 1.51 (0.10) | 1.79 (0.08) | 1.34 (0.08) b | 1.75 (0.07) b | 1.37 (0.08) | 1.59 (0.06) | 1.64 (0.13) | 1.72 (0.06) |
| EWCFG Rec. | 2 | 2 | 2 | 2 | 3 | 3 | 3 | 3 |
| Meat and Alternatives | ||||||||
| Tiers 1–3 | 1.86 (0.15) | 1.70 (0.10) | 2.35 (0.11) | 2.01 (0.09) | 2.40 (0.11) | 2.19 (0.09) | 2.10 (0.11) | 2.01 (0.08) |
| Tiers 1–4 | 2.12 (0.14) a | 1.88 (0.09) a | 2.60 (0.10) b | 2.20 (0.09) b | 2.65 (0.10) | 2.40 (0.09) | 2.36 (0.10) | 2.21 (0.08) |
| EWCFG Rec. | 3 | 2 | 3 | 2 | 3 | 2 | 3 | 2 |
| Men, 19–30 Years | Women, 19–30 Years | Men, 31–50 Years | Women, 31–50 Years | Men, 51–70 Years | Women, 51–70 Years | Men, >70 Years | Women, >70 Years | |
|---|---|---|---|---|---|---|---|---|
| Variable (kcal/Day) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) |
| Tiers 1 + 2 + 3 | 1539 (34) | 1089 (24) | 1468 (29) | 1103 (16) | 1353 (20) | 1086 (17) | 1217 (23) | 1014 (16) |
| Tier 4 | 269 (15) | 175 (10) | 240 (12) | 161 (9) | 178 (10) | 125 (7) | 164 (10) | 114 (6) |
| Other Foods/Beverages | ||||||||
| Alcoholic beverages | 155 (12) | 63 (9) | 127 (8) | 63 (6) | 124 (8) | 42 (3) | 62 (6) | 22 (2) |
| Beverages, higher calorie (≥40 kcal/100g) | 171 (8) | 103 (6) | 108 (6) | 61 (4) | 58 (4) | 42 (4) | 30 (3) | 26 (2) |
| Beverages, lower calorie (<40 kcal/100g) | 30 (3) | 26 (2) | 29 (2) | 26 (2) | 23 (2) | 19 (1) | 16 (1) | 15 (1) |
| High fat and/or sugar foods | 153 (8) | 130 (7) | 167 (9) | 124 (7) | 123 (5) | 105 (5) | 121 (7) | 87 (5) |
| Meal replacements | 7 (2) | 6 (2) | 4 (1) | 5 (1) | 2 (1) | 4 (1) | 0 (0) | 1 (0) |
| Saturated and/or trans fats and oils | 74 (5) | 54 (4) | 80 (5) | 59 (3) | 87 (4) | 62 (3) | 78 (4) | 64 (4) |
| Supplements | 4 (2) | 1 (0) | 3 (2) | 1 (0) | 1 (0) | 2 (1) | 2 (1) | 3 (1) |
| Uncategorized (ingredients/seasonings and unprepared foods) | 22 (3) | 15 (1) | 20 (2) | 17 (1) | 18 (1) | 16 (1) | 15 (1) | 14 (1) |
| Unsaturated fats and oils | 83 (5) | 57 (5) | 71 (4) | 62 (3) | 70 (4) | 55 (2) | 51 (3) | 47 (3) |
| Total energy from Tier 4 and “other” foods/beverages (kcal/day) | 874 (27) | 567 (19) | 771 (21) | 510 (16) | 611 (17) | 411 (11) | 487 (18) | 342 (11) |
| Total energy from Tier 4 and “other” foods/beverages (%) | 31 (1) | 29 (1) | 30 (1) | 27 (1) | 27 (1) | 23 (0) | 25 (1) | 21 (0) |






3.3. Diets High in Calories from Tier 4 and “Other” Foods/Beverages Are Not Associated with Obesity
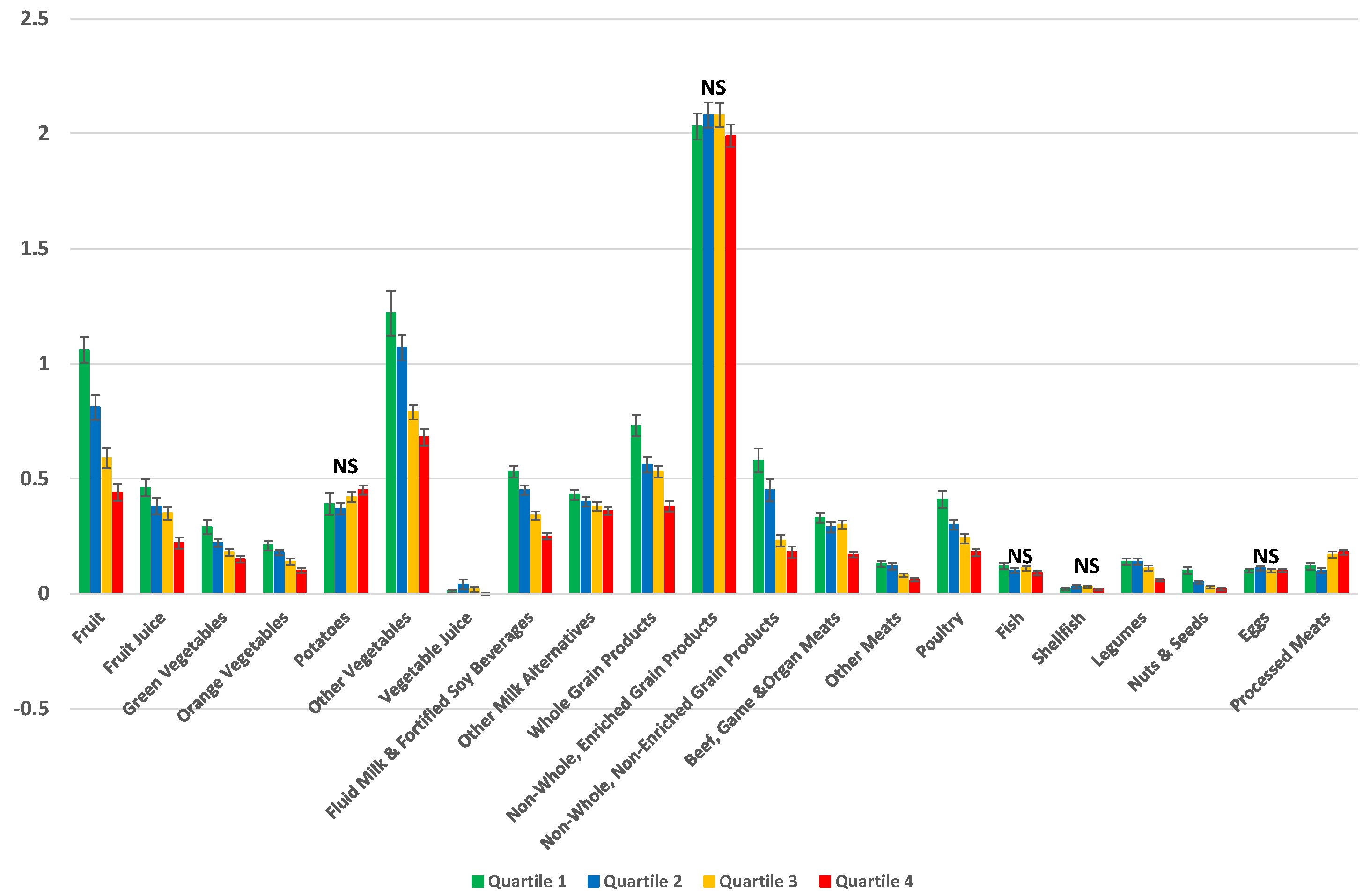
3.4. Diets High in Calories from Tier 4 and “Other” Foods/Beverages Are Associated with a Lower Nutrient Dense Diet
| Compliers (Q1) ‡ ≤19.42% Energy | Intermediates (Q2) § 19.42%–31.78% Energy | Intermediates (Q3) § 31.78%–45.73% Energy | Non–compliers (Q4) ‖ >45.73% Energy | ||
|---|---|---|---|---|---|
| Characteristics | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | p-Trend |
| Age (years) | 49.82 (0.57) | 47.38 (0.72) | 46.05 (0.54) | 42.57 (0.49) | <0.0001 |
| Sex (%) | |||||
| Males | 44.10 (3.57) | 48.84 (3.73) | 51.76 (2.47) | 53.48 (2.24) | |
| Females | 55.90 (3.57) | 51.16 (3.73) | 48.24 (2.47) | 46.52 (2.24) | 0.0175 |
| BMI (kg/m2) | 27.62 (0.28) | 27.18 (0.19) | 27.42 (0.19) | 27.69 (0.21) | 0.3214 |
| Misreporting Status (%) | |||||
| Under Reporters | 42.87 (2.03) | 34.35 (2.54) | 26.87 (1.52) | 22.66 (1.64) | |
| Over Reporters | 9.02 (1.39) | 7.97 (1.05) | 9.94 (1.21) | 14.29 (1.49) | <0.0001 |
| Physical Activity (%) | |||||
| Inactive | 55.86 (2.48) | 56.83 (1.96) | 57.54 (1.85) | 62.93 (1.84) | |
| Active | 18.97 (1.53) | 18.86 (1.41) | 15.80 (1.24) | 15.87 (1.28) | 0.0342 |
| Smoking Status (%) | |||||
| Daily Smoker | 13.07 (1.32) | 14.56 (1.17) | 24.61 (1.76) | 30.33 (1.68) | |
| Never Smoked | 57.68 (1.97) | 48.33 (2.07) | 41.89 (1.88) | 34.10 (1.53) | <0.0001 |
| Compliers (Q1) † ≤19.42% Energy | Intermediates (Q2) ‡ 19.42%–31.78% Energy | Intermediates (Q3) ‡ 31.78%–45.73% Energy | Non–compliers (Q4) § >45.73% Energy | p-Trend | |
|---|---|---|---|---|---|
| Nutrients | Mean (SEM) | Mean (SEM) | Mean (SEM) | Mean (SEM) | |
| Energy (kcal/day) | 2355 (28) | 2426 (24) | 2427 (22) | 2478 (30) | <0.0001 |
| Fat (%Energy) | 28.90 (0.43) | 31.70 (0.34) | 33.91 (0.32) | 33.73 (0.39) | <0.0001 |
| Saturated fat (%Energy) | 9.02 (0.15) | 10.02 (0.16) | 11.23 (0.18) | 11.29 (0.19) | <0.0001 |
| Monounsaturated fat (%Energy) | 11.37 (0.22) | 12.74 (0.18) | 13.59 (0.15) | 13.64 (0.19) | <0.0001 |
| Polyunsaturated fat (%Energy) | 5.35 (0.13) | 5.76 (0.10) | 5.96 (0.10) | 5.91 (0.11) | 0.00 |
| Carbohydrates (%Energy) | 50.83 (0.56) | 48.77 (0.55) | 47.13 (0.46) | 47.29 (0.47) | <0.0001 |
| Added sugar (%Energy) | 5.45 (0.23) | 7.71 (0.31) | 10.40 (0.29) | 14.00 (0.36) | <0.0001 |
| Dietary fiber (g/1000 kcal) | 10.99 (0.30) | 9.37 (0.16) | 7.99 (0.13) | 6.86 (0.11) | <0.0001 |
| Protein (%Energy) | 19.63 (0.32) | 17.46 (0.30) | 15.78 (0.22) | 12.82 (0.16) | <0.0001 |
| Alcohol (%Energy) | 0.64 (0.13) | 2.07 (0.13) | 3.17 (0.24) | 6.16 (0.41) | <0.0001 |
| Vitamin A (RE/1000 kcal) | 454.94 (37.78) | 377.34 (37.78) | 339.23 (11.48) | 287.96 (10.65) | <0.0001 |
| Vitamin D (ug/1000 kcal) | 3.23 (0.16) | 3.18 (0.15) | 2.84 (0.19) | 2.45 (0.16) | <0.0001 |
| Thiamin (mg/1000 kcal) | 1.01 (0.02) | 0.91 (0.01) | 0.81 (0.01) | 0.66 (0.01) | <0.0001 |
| Riboflavin (mg/1000 kcal) | 1.09 (0.02) | 0.99 (0.01) | 0.90 (0.01) | 0.80 (0.01) | <0.0001 |
| Niacin (NE/1000 kcal) | 23.09 (0.40) | 20.45 (0.27) | 18.66 (0.26) | 16.03 (0.31) | <0.0001 |
| Vitamin B6 (ug/1000 kcal) | 1.18 (0.02) | 0.98 (0.01) | 0.86 (0.02) | 0.71 (0.01) | <0.0001 |
| Folate (ug/1000 kcal) | 140.90 (4.18) | 126.67 (2.72) | 111.50 (2.16) | 94.84 (1.86) | <0.0001 |
| Vitamin B12 (ug/1000 kcal) | 2.60 (0.17) | 2.44 (0.16) | 2.03 (0.06) | 1.69 (0.06) | <0.0001 |
| Vitamin C (mg/1000 kcal) | 77.08 (2.35) | 67.80 (2.22) | 59.87 (1.90) | 45.63 (1.76) | <0.0001 |
| Calcium (mg/1000 kcal) | 480.37 (9.83) | 437.20 (8.22) | 392.96 (6.56) | 349.48 (6.24) | <0.0001 |
| Phosphorous (mg/1000 kcal) | 772.27 (8.81) | 691.04 (7.52) | 622.08 (7.17) | 547.76 (6.62) | <0.0001 |
| Potassium (mg/1000 kcal) | 1855.09 (27.90) | 1644.51 (16.61) | 1477.51 (16.16) | 1295.64 (18.68) | <0.0001 |
| Sodium (mg/1000 kcal) | 1536.45 (30.10) | 1523.69 (25.57) | 1584.82 (24.92) | 1510.05 (35.78) | 0.11 |
| Magnesium (mg/1000 kcal) | 194.68 (3.53) | 173.05 (1.99) | 152.38 (1.57) | 140.98 (4.48) | <.0001 |
| Iron (mg/1000 kcal) | 8.04 (0.12) | 7.38 (0.10) | 6.75 (0.08) | 5.75 (0.07) | <.0001 |
| Zinc (mg/1000 kcal) | 6.63 (0.10) | 5.89 (0.13) | 5.37 (0.09) | 4.33 (0.07) | <0.0001 |
| Glycemic Index | 51.03 (0.40) | 52.40 (0.32) | 53.61 (0.32) | 53.56 (0.35) | <0.0001 |
| Glycemic Load | 151.26 (3.12) | 156.99 (2.72) | 154.48 (2.48) | 159.37 (2.94) | 0.07 |
| Energy Density (kcal/g) | 1.55 (0.02) | 1.71 (0.02) | 1.91 (0.02) | 2.15 (0.02) | <0.0001 |

4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Nutrient Profile Models. Available online: http://www.who.int/nutrition/topics/profiling/en/ (accessed on 8 October 2015).
- World Health Organization Regional Office for Europe. Nutrient Profile Model. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/270716/Nutrient-Profile-Model_Version-for-Web.pdf?ua=1 (accessed on 8 October 2015).
- World Health Organization. Catalogue of Nutrient Profile Models; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Department of Health. Nutrient Profiling Technical Guidance. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216094/dh_123492.pdf (accessed on 8 October 2015).
- Chiuve, S.E.; Sampson, L.; Willett, W.C. The association between a nutritional quality index and risk of chronic disease. Am. J. Prev. Med. 2011, 40, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Njike, V.Y.; Rhee, L.Q.; Reingold, A.; Ayoob, K.T. Performance characteristics of NuVal and the Overall Nutritional Quality Index (ONQI). Am. J. Clin. Nutr. 2010, 91, 1102S–1108S. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Njike, V.Y.; Faridi, Z.; Rhee, L.Q.; Reeves, R.S.; Jenkins, D.J.; Ayoob, K.T. The stratification of foods on the basis of overall nutritional quality: The overall nutritional quality index. Am. J. Health Promot. 2009, 24, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Food Standards Australia New Zealand. Short Guide for Industry to the Nutrient Profiling Scoring Criterion (NPSC) in Standard 1.2.7—Nutrition, Health and Related Claims. Available online: http://www.foodstandards.gov.au/industry/labelling/Documents/Short-guide-for-industry-to-the-NPSC.pdf (accessed on 8 October 2015).
- Health Canada. The Development and Use of a Surveillance Tool: The Classification of Foods in the Canadian Nutrient File According to Eating Well with Canada’s Food Guide, 2014. Available online: http://publications.gc.ca/collections/collection_2014/sc-hc/H164-158-2-2014-eng.pdf (accessed on 8 October 2015).
- Katamay, S.W.; Esslinger, K.A.; Vigneault, M.; Johnston, J.L.; Junkins, B.A.; Robbins, L.G.; Sirois, I.V.; Jones-Mclean, E.M.; Kennedy, A.F.; Bush, M.A.; et al. Eating well with Canada’s Food Guide (2007): Development of the food intake pattern. Nutr. Rev. 2007, 65, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. The Canadian Nutrient File; Nutrition Research Division: Ottawa, ON, Canada, 2001. [Google Scholar]
- Health Canada. Canadian Community Health Survey Cycle 2.2 Nutrition (2004)—A Guide to Accessing and Interpreting the Data. Available online: http://www.hc-sc.gc.ca/fn-an/surveill/nutrition/commun/cchs_guide_escc-eng.php (accessed on 8 October 2015).
- Béland, Y.; Dale, V.; Dufour, J.; Hamel, M. The Canadian Community Health Survey: Building on the Success from the Past. In Proceedings of the American Statistical Association Joint Statistical Meeting, Section on Survey Research Methods, American Statistical Association, Minneapolis, MN, USA, 2–6 August 2005.
- Statistics Canada. Canadian Community Health Survey (CCHS) Cycle 2.2 (2004). Nutrition—General Health (Including Vitamin & Mineral Supplements) & 24-Hour Dietary Recall Components. Available online: http://www23.statcan.gc.ca/imdb-bmdi/document/5049_D24_T9_V1-eng.pdf (accessed on 8 October 2015).
- United States Department of Agriculture Agricultural Research Service. USDA Automated Multiple-Pass Method. Available online: http://www.ars.usda.gov/Services/docs.htm?docid=7710 (accessed on 8 October 2015).
- United States Department of Agriculture, Agricultural Research Service. National Nutrient Database for Standard Reference Release 19. Available online: http://www.ars.usda.gov/ba/bhnrc/ndl (accessed on 8 October 2015).
- Atkinson, F.S.; Foster-Powell, K.; Brand-Miller, J.C. International tables of glycemic index and glycemic load values: 2008. Diabetes Care 2008, 31, 2281–2283. [Google Scholar] [CrossRef] [PubMed]
- Foster-Powell, K.; Holt, S.H.; Brand-Miller, J.C. International table of glycemic index and glycemic load values: 2002. Am. J. Clin. Nutr. 2002, 76, 5–56. [Google Scholar] [PubMed]
- Health Canada Bureau of Nutritional Sciences. Food Group Codes and Descriptions—Canadian Community Health Survey (CCHS) 2.2. Available online: http://www23.statcan.gc.ca/imdb-bmdi/pub/document/5049_D23_T9_V1-eng.pdf (accessed on 8 October 2015).
- Louie, J.C.; Flood, V.; Turner, N.; Everingham, C.; Gwynn, J. Methodology for adding glycemic index values to 24-hour recalls. Nutrition 2011, 27, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Flood, A.; Subar, A.F.; Hull, S.G.; Zimmerman, T.P.; Jenkins, D.J.; Schatzkin, A. Methodology for adding glycemic load values to the National Cancer Institute Diet History Questionnaire database. J. Am. Diet. Assoc. 2006, 106, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Perez-Escamilla, R.; Obbagy, J.E.; Altman, J.M.; Essery, E.V.; McGrane, M.M.; Wong, Y.P.; Spahn, J.M.; Williams, C.L. Dietary energy density and body weight in adults and children: A systematic review. J. Acad. Nutr. Diet. 2012, 112, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Mander, A.P.; Jones, L.R.; Emmett, P.M.; Jebb, S.A. A prospective analysis of dietary energy density at age 5 and 7 years and fatness at 9 years among UK children. Int. J. Obes. 2008, 32, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Blanck, H.M.; Kettel Khan, L.; Serdula, M.K.; Seymour, J.D.; Tohill, B.C.; Rolls, B.J. Dietary energy density is associated with energy intake and weight status in US adults. Am. J. Clin. Nutr. 2006, 83, 1362–1368. [Google Scholar] [PubMed]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1231S. [Google Scholar] [PubMed]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Black, A.E.; Goldberg, G.R.; Jebb, S.A.; Livingstone, M.B.; Cole, T.J.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 2. Evaluating the results of published surveys. Eur. J. Clin. Nutr. 1991, 45, 583–599. [Google Scholar] [PubMed]
- Nielsen, S.J.; Adair, L. An alternative to dietary data exclusions. J. Am. Diet. Assoc. 2007, 107, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Jessri, M.; Lou, Y.W.; L’Abbe, M.R. Evaluation of different methods to handle misreporting in obesity research: Evidence from the Canadian national nutrition survey. Br. J. Nutr. 2016, 115, 147–159. [Google Scholar] [CrossRef] [PubMed]
- McCrory, M.A.; McCrory, M.A.; Hajduk, C.L.; Roberts, S.B. Procedures for screening out inaccurate reports of dietary energy intake. Public Health Nutr. 2002, 5, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of screening out implausible energy intake reports on relationships between diet and BMI. Obes. Res. 2005, 13, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Impact of identifying plausible respondents on the under-reporting of energy intake in the Canadian Community Health Survey. Health Rep. 2008, 19, 47–55. [Google Scholar] [PubMed]
- Rao, J.N.K.; Wu, C.F.J.; Yue, K. Some recent work on resampling methods for complex surveys. Survey Methodol. 1992, 18, 209–217. [Google Scholar]
- Yeo, D.; Mantel, H.; Liu, T.P. Bootstrap Variance Estimation for the National Population Health Survey. In Proceedings of the Annual Meeting of the American Statistical Association: Survey Research Methods Section; American Statistical Association: Baltimore, MD, USA, 7 August 1999. [Google Scholar]
- Statistics Canada. Canadian Community Health Survey—Nutrition (CCHS). Available online: http://www.hc-sc.gc.ca/fn-an/surveill/nutrition/commun/cchs_focus-volet_escc-eng.php (accessed on 8 October 2015).
- Jessri, M.; L’Abbé, M.R. The Time for an Updated Canadian Food Guide Has Arrived. Appl. Physiol. Nutr. Metab. 2015, 40, 854–857. [Google Scholar] [CrossRef] [PubMed]
- Kondro, W. Proposed Canada Food Guide called “obesogenic”. CMAJ 2006, 174, 605–606. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Ayoob, K.T.; Decker, E.A.; Frank, G.C.; Jenkins, D.A.; Reeves, R.S.; Charmel, P. The ONQI is not a black box. Am. J. Prev. Med. 2011, 41, e15–e16. [Google Scholar] [CrossRef] [PubMed]
- Fogli-Cawley, J.J.; Dwyer, J.T.; Saltzman, E.; McCullough, M.L.; Troy, L.M.; Jacques, P.F. The 2005 Dietary Guidelines for Americans Adherence Index: Development and application. J. Nutr. 2006, 136, 2908–2915. [Google Scholar] [PubMed]
- Kranz, S.; Hartman, T.; Siega-Riz, A.M.; Herring, A.H. A diet quality index for American preschoolers based on current dietary intake recommendations and an indicator of energy balance. J. Am. Diet. Assoc. 2006, 106, 1594–1604. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Indexes of overall diet quality: A review. J. Am. Diet. Assoc. 1996, 96, 785–791. [Google Scholar] [CrossRef]
- Julia, C.; Touvier, M.; Mejean, C.; Ducrot, P.; Peneau, S.; Hercberg, S.; Kesse-Guyot, E. Development and validation of an individual dietary index based on the British Food Standard Agency nutrient profiling system in a French context. J. Nutr. 2014, 144, 2009–2017. [Google Scholar] [CrossRef] [PubMed]
- Estaquio, C.; Kesse-Guyot, E.; Deschamps, V.; Bertrais, S.; Dauchet, L.; Galan, P.; Hercberg, S.; Castetbon, K. Adherence to the French Programme National Nutrition Sante Guideline Score is associated with better nutrient intake and nutritional status. J. Am. Diet. Assoc. 2009, 109, 1031–1041. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An index of diet and eating patterns is a valid measure of diet quality in an Australian population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [PubMed]
- Clerfeuille, E.; Vieux, F.; Lluch, A.; Darmon, N.; Rolf-Pedersen, N. Assessing the construct validity of five nutrient profiling systems using diet modeling with linear programming. Eur. J. Clin. Nutr. 2013, 67, 1003–1005. [Google Scholar] [CrossRef] [PubMed]
- Chiolero, A.; Wietlisbach, V.; Ruffieux, C.; Paccaud, F.; Cornuz, J. Clustering of risk behaviors with cigarette consumption: A population-based survey. Prev. Med. 2006, 42, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Dallongeville, J.; Marecaux, N.; Fruchart, J.C.; Amouyel, P. Cigarette smoking is associated with unhealthy patterns of nutrient intake: A meta-analysis. J. Nutr. 1998, 128, 1450–1457. [Google Scholar] [PubMed]
- Julia, C.; Vernay, M.; Salanave, B.; Deschamps, V.; Malon, A.; Oleko, A.; Hercberg, S.; Castetbon, K. Nutrition patterns and metabolic syndrome: A need for action in young adults (French Nutrition and Health Survey—ENNS, 2006–2007). Prev. Med. 2010, 51, 488–493. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, K. The Relationship between Diet Quality and Obesity in Canadian Adults: Evidence from the 2004 Canadian Community Health Survey. Available online: http://ir.lib.uwo.ca/cgi/viewcontent.cgi?article=1570&context=etd (accessed on 6 October 2015).
- Alkerwi, A.; Sauvageot, N.; Nau, A.; Lair, M.L.; Donneau, A.F.; Albert, A.; Guillaume, M. Population compliance with national dietary recommendations and its determinants: Findings from the ORISCAV-LUX study. Br. J. Nutr. 2012, 108, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- Togo, P.; Osler, M.; Sorensen, T.I.; Heitmann, B.L. Food intake patterns and body mass index in observational studies. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Julia, C.; Peneau, S.; Andreeva, V.A.; Mejean, C.; Fezeu, L.; Galan, P.; Hercberg, S. Weight-loss strategies used by the general population: How are they perceived? PLoS ONE 2014, 9, e97834. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Waijers, P.M.; Feskens, E.J.; Ocke, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Available online: http://www.health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 8 October 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jessri, M.; Nishi, S.K.; L’Abbé, M.R. Assessing the Nutritional Quality of Diets of Canadian Adults Using the 2014 Health Canada Surveillance Tool Tier System. Nutrients 2015, 7, 10447-10468. https://doi.org/10.3390/nu7125543
Jessri M, Nishi SK, L’Abbé MR. Assessing the Nutritional Quality of Diets of Canadian Adults Using the 2014 Health Canada Surveillance Tool Tier System. Nutrients. 2015; 7(12):10447-10468. https://doi.org/10.3390/nu7125543
Chicago/Turabian StyleJessri, Mahsa, Stephanie K. Nishi, and Mary R. L’Abbé. 2015. "Assessing the Nutritional Quality of Diets of Canadian Adults Using the 2014 Health Canada Surveillance Tool Tier System" Nutrients 7, no. 12: 10447-10468. https://doi.org/10.3390/nu7125543