Effects of Supplementation with the Fat-Soluble Vitamins E and D on Fasting Flow-Mediated Vasodilation in Adults: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Experimental Section
2.1. Search Strategy
2.2. Selection of Trials
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
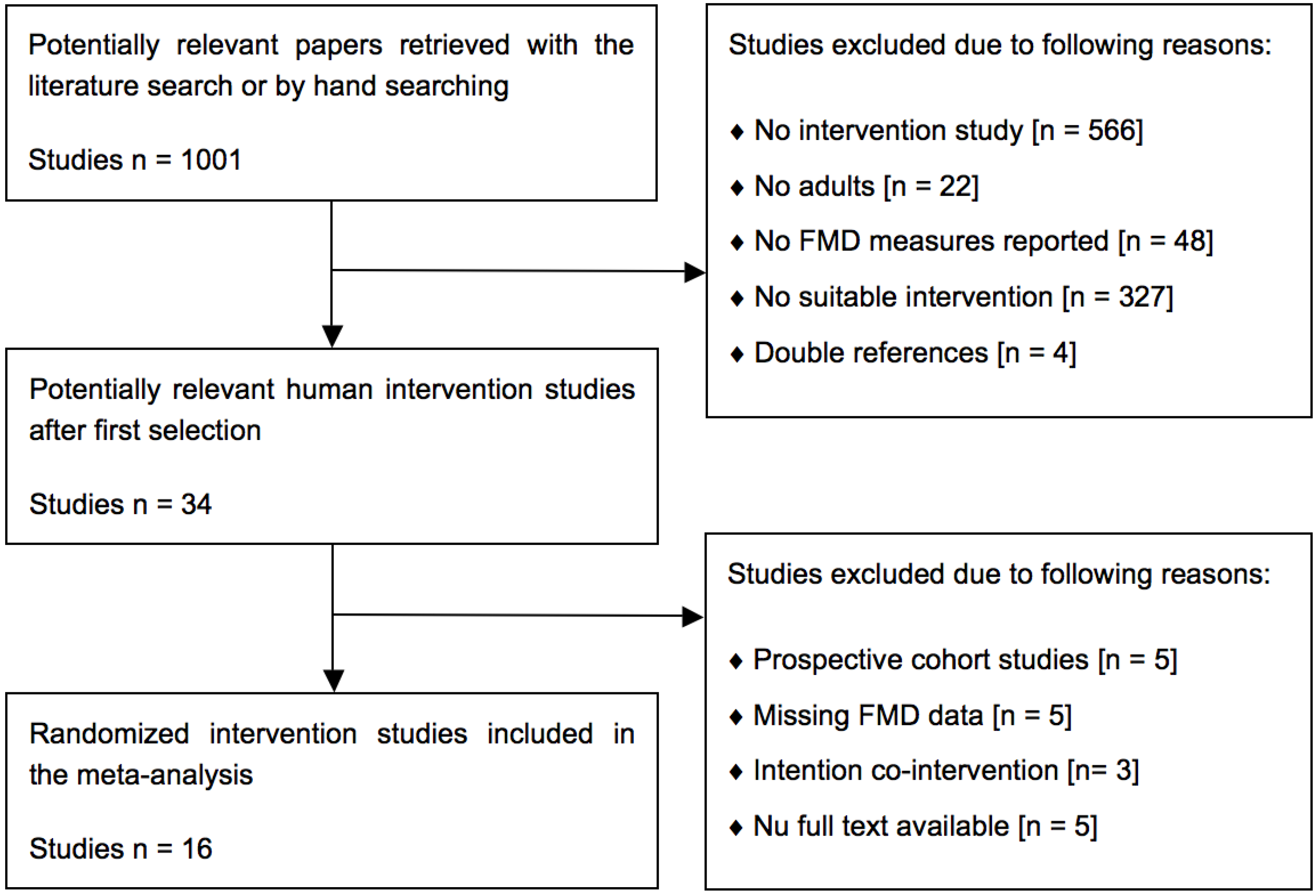
3.1. Search Results and Study Selection
3.2. Study Characteristics


{kind=link}
{kind=link}
{kind=link}
| First Author and Year | Subject Characteristics | Treatment Characteristics | FMD Measurement Characteristics | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Design 1 | Number | Male (%) | Age (Y) | BMI (kg/m2) | Health Status | Treatment 2 | Dose 3 | Duration | Cuff | Occlusion | Baseline (%) | |||||||
| Randomized controlled trials (RCTs) with vitamin E supplements as experimental variable 4 | ||||||||||||||||||
| Borovničar, 2000 (31) | P | 22/22 | 100/100 | 45.0/45.0 | -/- | High cholesterol | Toco-acetate | 889 IU/day | 6 months | Distal | 4.0 min | 6.20/6.50 | ||||||
| Economides, 2005 (32) | P | 32/31 | 53.9/53.9 | 53.0/53.0 | 29.2/29.2 | Type I/II diabetes | All-racemic α-Toc | 1800 IU/day | 12 months | - | - | 5.80/5.80 | ||||||
| Economides, 2005 (32) | P | 34/32 | 53.9/53.9 | 53.0/53.0 | 29.2/29.2 | Type I/II diabetes | All-racemic α-Toc | 1800 IU/day | 6 months | - | - | 5.70/5.70 | ||||||
| Kugiyama, 1999 (35) | P | 35/35 | 40.0/45.7 | 59.8/60.1 | 23.1/23.1 | Chest pain | α-Toco-acetate | 300 IU/day | 4 weeks | Distal | 5.0 min | 5.04/5.02 | ||||||
| Neunteufl, 2000 (37) | P | 11/11 | 100/100 | 28.0/27.0 | -/- | Smokers | All-racemic α-Toc | 600 IU/day | 4 weeks | Proximal | 4.5 min | 5.30/6.40 | ||||||
| Paolisso, 2000 (38) | P | 20/20 | 45.0/60.0 | 58.3/56.7 | 27.6/27.4 | Type II diabetes | Vitamin E | 1333 IU/day | 8 weeks | Proximal | 5.5 min | 1.83/1.71 | ||||||
| Simons, 1999 (46) | CO | 20/- | 65.0/- | 57.0/- | 27.5/- | Healthy | RRR D-α-Toco | 1000 IU/day | 10 weeks | Distal | 4.5 min | 2.70/- | ||||||
| Skyrme-Jones, 2000 (39) | P | 20/21 | 47.6/45.0 | 23.0/28.0 | 24.3/25.5 | Type I diabetes | All-racemic α-Toc | 1000 IU/day | 3 months | - | 5.0 min | 2.60/2.40 | ||||||
| Randomized controlled trials (RCTs) with vitamin D supplements as experimental variable 5 | ||||||||||||||||||
| Gepner, 2012 (33) | P | 55/55 | 00.0/00.0 | 64.1/63.6 | 27.1/25.3 | Post-menopausal | Vitamin D3 | 2500 IU/day | 4 months | Distal | 5.0 min | 5.05/4.57 | ||||||
| Harris, 2011 (34) | P | 22/23 | 41.0/52.0 | 29.0/31.0 | 30.4/29.1 | African American | Vitamin D3 | 2000 IU/day | 16 weeks | Distal | 5.0 min | 7.23/6.55 | ||||||
| Longenecker, 2012 (36) | P | 30/15 | 83.3/66.7 | 47.0/10.0 | 28.0/27.0 | HIV-infected | Vitamin D3 | 4000 IU/day | 12 weeks | Distal | 5.0 min | 2.87/2.46 | ||||||
| Sugden, 2008 (40) | P | 17/17 | 58.8/47.1 | 64.9/63.5 | 31.7/31.7 | Type II diabetes | Vitamin D2 | 100K IU (0) | 8 weeks | Distal | 5.0 min | 6.38/7.28 | ||||||
| Witham, 2010 (42) | P | 19/21 | 84.2/54.5 | 65.3/66.7 | 31.1/33.3 | Type II diabetes | Vitamin D3 | 100K IU (0) | 16 weeks | Distal | - | 5.10/5.40 | ||||||
| Witham, 2010 (42) | P | 18/21 | 65.0/54.5 | 63.3/66.7 | 29.7/33.3 | Type II diabetes | Vitamin D3 | 200K IU (0) | 16 weeks | Distal | - | 6.40/5.40 | ||||||
| Witham, 2010 (42) | P | 19/22 | 84.2/54.5 | 65.3/66.7 | 31.1/33.3 | Type II diabetes | Vitamin D3 | 100K IU (0) | 8 weeks | Distal | - | 5.10/5.40 | ||||||
| Witham, 2010 (42) | P | 17/22 | 65.0/54.5 | 63.3/66.7 | 29.7/33.3 | Type II diabetes | Vitamin D3 | 200K IU (0) | 8 weeks | Distal | - | 6.40/5.40 | ||||||
| Witham, 2012 (43) | P | 28/27 | 60.0/85.7 | 66.2/67.7 | 27.3/26.1 | History stroke | Vitamin D2 | 100K IU (0) | 16 weeks | Distal | 5.0 min | 6.90/5.60 | ||||||
| Witham, 2012 (43) | P | 29/27 | 60.0/85.7 | 66.2/67.7 | 27.3/26.1 | History stroke | Vitamin D2 | 100K IU (0) | 8 weeks | Distal | 5.0 min | 6.90/5.60 | ||||||
| Witham, 2013 (44) | P | 80/79 | 50.0/53.2 | 76.9/76.7 | 28.5/27.9 | High systolic BP | Vitamin D3 | 100K IU (3) | 12 months | Distal | 5.0 min | 5.10/5.10 | ||||||
| Witham, 2013 (44) | P | 80/79 | 50.0/53.2 | 76.9/76.7 | 28.5/27.9 | High systolic BP | Vitamin D3 | 100K IU (0) | 3 months | Distal | 5.0 min | 5.10/5.10 | ||||||
| Witham, 2013 (41) | P | 25/25 | 00.0/00.0 | 41.7/39.4 | 24.9/28.7 | South Asian | Vitamin D3 | 100K IU (0) | 8 weeks | Distal | 5.0 min | 8.20/8.70 | ||||||
| Witham, 2013 (41) | P | 25/25 | 00.0/00.0 | 41.7/39.4 | 24.9/28.7 | South Asian | Vitamin D3 | 100K IU (0) | 4 weeks | Distal | 5.0 min | 8.20/8.70 | ||||||
| Yiu, 2013 (45) | P | 50/50 | 54.0/46.0 | 65.8/64.9 | 25.8/25.1 | Type II diabetes | Vitamin D3 | 5000 IU/day | 12 weeks | Distal | 5.0 min | 3.39/3.40 | ||||||
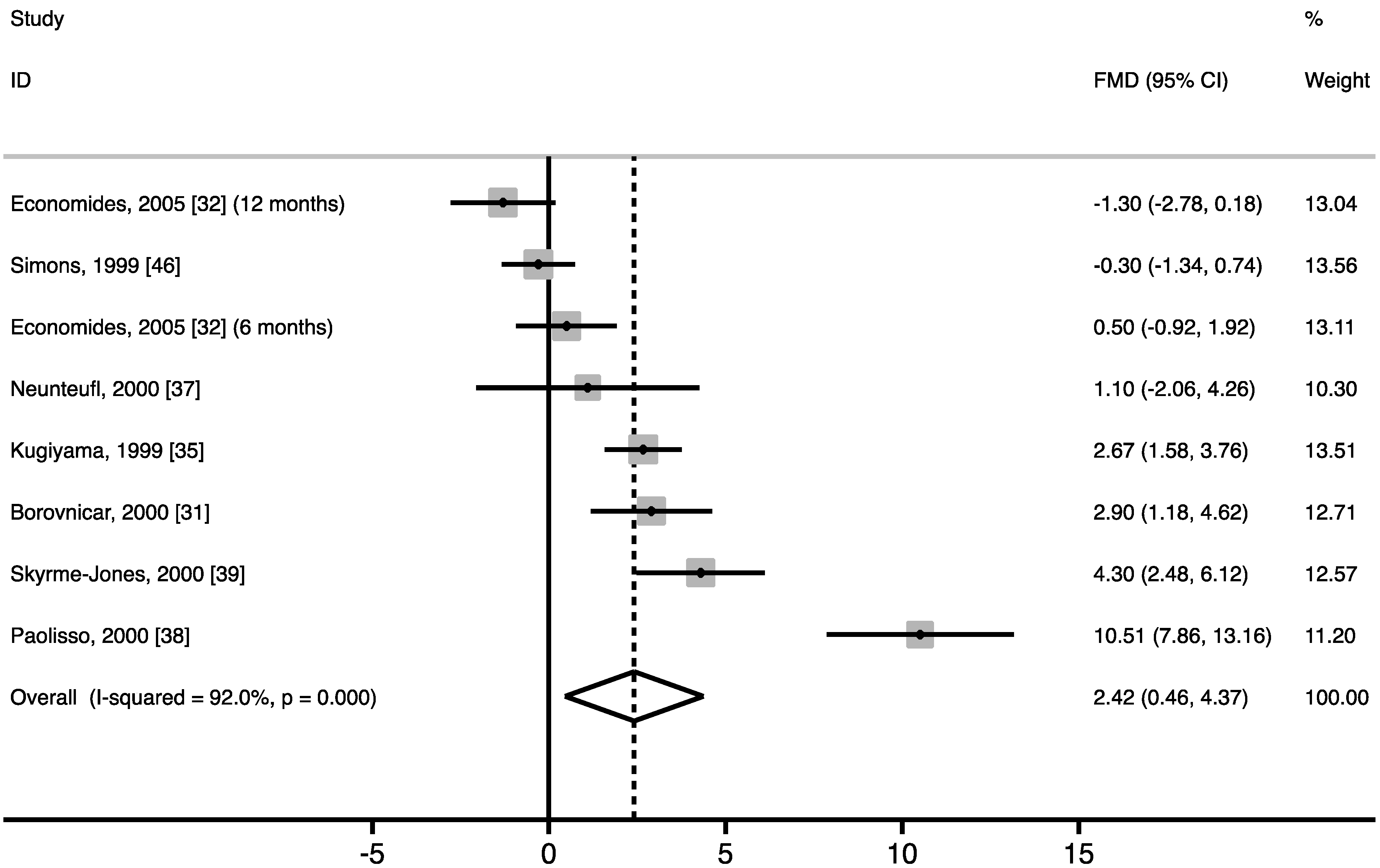
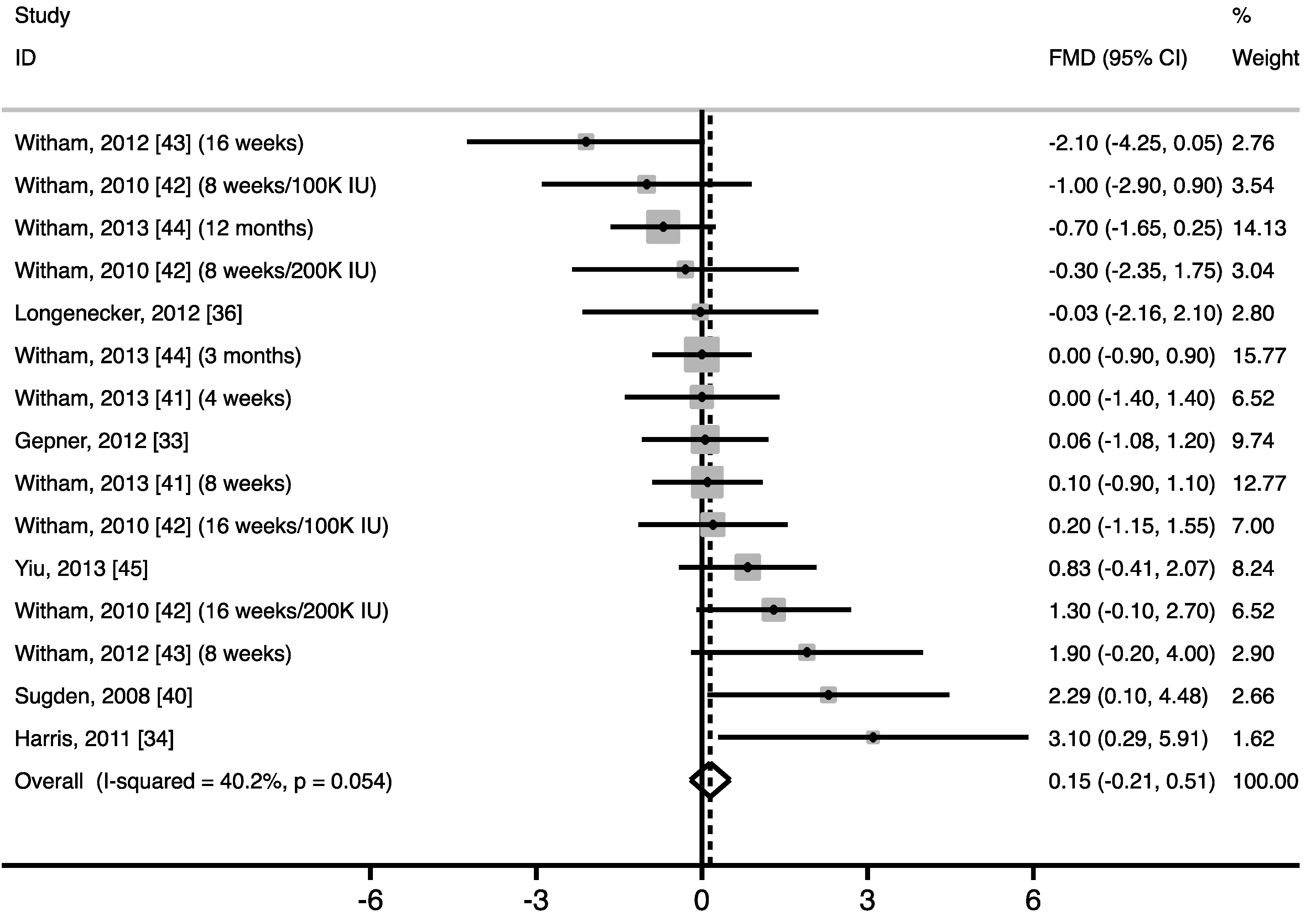
3.3. Effect of Vitamin Supplementation on FMD


3.4. Subgroup Analyses
3.5. Publication Bias
| Study Characteristic | Mean | Stratification Variable | No of Study Arms | WMD (%) 1 | 95% CI (%) | p-value Difference |
|---|---|---|---|---|---|---|
| Study arms with vitamin E supplements as experimental variable 2 | ||||||
| Mean age (years) 3 | 47.1 | ≤53.0 | 5 | 1.48 | −0.59 to 3.55 | 0.372 |
| >53.0 | 3 | 4.08 | −0.25 to 8.41 | |||
| Gender (% male) 3 | 63.2 | ≤53.9 | 5 | 3.17 | 0.25 to 6.10 | 0.500 |
| >53.9 | 3 | 1.17 | −1.14 to 3.49 | |||
| Baseline BMI (kg/m2) 3 | 26.8 | ≤27.5 | 3 | 2.15 | −0.43 to 4.72 | 0.828 |
| >27.5 | 3 | 3.11 | −2.39 to 8.60 | |||
| Baseline FMD (%) 3 | 4.40 | ≤5.17 | 4 | 4.10 | 0.71 to 7.50 | 0.219 |
| >5.17 | 4 | 0.74 | −1.16 to 2.63 | |||
| Health status | - | Healthy | 2 | −0.16 | −1.15 to 0.82 | 0.390 |
| Diseased | 6 | 3.10 | 0.67 to 5.54 | |||
| Dose (100 IU/day) 3 | 10.9 | ≤10.0 | 5 | 2.14 | 0.35 to 3.93 | 0.764 |
| >10.0 | 3 | 3.11 | −2.39 to 8.60 | |||
| Study duration (weeks) 3 | 16.8 | ≤11.0 | 4 | 3.39 | −0.19 to 6.97 | 0.523 |
| >11.0 | 4 | 1.56 | −0.83 to 3.94 | |||
| Position cuff | - | Distal | 3 | 1.40 | 0.71 to 2.09 | 0.341 |
| Proximal | 2 | 6.63 | 4.60 to 8.66 | |||
| Occlusion duration (min) 4 | 4.67 | ≤4.50 | 3 | 1.17 | −1.14 to 3.49 | 0.158 |
| >4.50 | 3 | 5.65 | 1.77 to 9.54 | |||
| Study arms with vitamin D supplements as experimental variable 4 | ||||||
| Mean age (years) 3 | 59.8< 44.9 | ≤64.9 | 8 | 0.45 | −0.09 to 0.98 | 0.263 |
| >64.9 | 7 | −0.10 | −0.59 to 0.38 | |||
| Gender (% male) 3 | 50.4 | ≤58.8 | 8 | 0.14 | −0.28 to 0.56 | 0.805 |
| >58.8 | 7 | 0.18 | −0.49 to 0.85 | |||
| Baseline BMI (kg/m2) 3 | 28.4 | ≤28.5 | 9 | −0.02 | −0.43 to 0.39 | 0.226 |
| >28.5 | 6 | 0.68 | −0.05 to 1.40 | |||
| Baseline FMD (%) 3 | 5.89 | ≤6.38 | 8 | 0.02 | −0.43 to 0.47 | 0.550 |
| >6.38 | 7 | 0.38 | −0.22 to 0.97 | |||
| Health status | - | Healthy | 4 | 0.23 | −0.42 to 0.87 | 0.820 |
| Diseased | 11 | 0.12 | −0.31 to 0.55 | |||
| Type of vitamin 5 | - | Vitamin D2 | 3 | 0.70 | −0.54 to 1.94 | 0.521 |
| Vitamin D3 | 12 | 0.10 | −0.27 to 0.47 | |||
| Study duration (weeks) 3 | 13.9 | ≤12.0 | 9 | 0.26 | −0.21 to 0.73 | 0.675 |
| >12.0 | 6 | −0.01 | −0.56 to 0.55 | |||
| Position cuff | - | Distal | 15 | 0.15 | −0.21 to 0.51 | - |
| Proximal | 0 | - | - | |||
| Occlusion duration (min) 4 | 5.00 | ≤5.00 | 11 | 0.12 | −0.28 to 0.52 | - |
| >5.00 | 0 | - | - | |||
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lichtenstein, A.H. Nutrient supplements and cardiovascular disease: A heartbreaking story. J. Lipid Res. 2009, 50, S429–S433. [Google Scholar] [CrossRef] [PubMed]
- Widlansky, M.E.; Gokce, N.; Keaney, J.F., Jr.; Vita, J.A. The clinical implications of endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Schachinger, V.; Britten, M.B.; Zeiher, A.M. Prognostic impact of coronary vasodilator dysfunction on adverse long-term outcome of coronary heart disease. Circulation 2000, 101, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.N.; Quyyumi, A.A.; Hollenberg, N.K.; Jamerson, K.A. Surrogate markers for cardiovascular disease: Functional markers. Circulation 2004, 109, 31–46. [Google Scholar] [CrossRef]
- Ellins, E.A.; Halcox, J.P. Where are we heading with noninvasive clinical vascular physiology? Why and how should we assess endothelial function? Cardiol. Res. Pract. 2011, 2011, 870132. [Google Scholar] [CrossRef]
- Montero, D.; Walther, G.; Stehouwer, C.D.; Houben, A.J.; Beckman, J.A.; Vinet, A. Effect of antioxidant vitamin supplementation on endothelial function in type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Obes Rev. 2014, 15, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Ashor, A.W.; Lara, J.; Mathers, J.C.; Siervo, M. Effect of vitamin C on endothelial function in health and disease: A systematic review and meta-analysis of randomised controlled trials. Atherosclerosis 2014, 235, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Min, B. Effects of vitamin D on blood pressure and endothelial function. Korean J. Physiol. Pharmacol. 2013, 17, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.M.; Woo, J.; Wu, S.H.; Ho, S.C. The role of vitamin D in blood pressure, endothelial and renal function in postmenopausal women. Nutrients 2013, 5, 2590–2610. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Arab, L.; Barr, S.I.; Becking, G.C. A Report of the Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Joris, P.J.; Zeegers, M.P.; Mensink, R.P. Weight loss improves fasting flow-mediated vasodilation in adults: A meta-analysis of intervention studies. Atherosclerosis 2014, 239, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Can, M.; Gunes, M.; Haliloglu, O.A.; Haklar, G.; Inanc, N.; Yavuz, D.G.; Direskeneli, H. Effect of vitamin D deficiency and replacement on endothelial functions in Behçet's disease. Clin. Exp. Rheumatol. 2012, 30, S57–S61. [Google Scholar] [PubMed]
- Chitalia, N.; Ismail, T.; Tooth, L.; Boa, F.; Hampson, G.; Goldsmith, D.; Kaski, J.C.; Banerjee, D. Impact of vitamin D supplementation on arterial vasomotion, stiffness and endothelial biomarkers in chronic kidney disease patients. PLoS One 2014, 9, e91363. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.K.; Blum, A.; Hathaway, L.; Mincemoyer, R.; Csako, G.; Waclawiw, M.A.; Panza, J.A.; Cannon, R.O., 3rd. Vascular effects of estrogen and vitamin E therapies in postmenopausal women. Circulation 1999, 100, 1851–1857. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Carlsson, C.M.; Papcke-Benson, K.; Aeschlimann, S.E.; Bodemer, A.; Carnes, M.; McBride, P.E. The effects of lipid-lowering and antioxidant vitamin therapies on flow-mediated vasodilation of the brachial artery in older adults with hypercholesterolemia. J. Am. Coll. Cardiol. 2001, 38, 1806–1813. [Google Scholar] [CrossRef] [PubMed]
- Tarcin, O.; Yavuz, D.G.; Ozben, B.; Telli, A.; Ogunc, A.V.; Yuksel, M.; Toprak, A.; Yazici, D.; Sancak, S.; Deyneli, O.; et al. Effect of vitamin D deficiency and replacement on endothelial function in asymptomatic subjects. J. Clin. Endocrinol. Metab. 2009, 94, 4023–4030. [Google Scholar] [CrossRef] [PubMed]
- Gazis, A.; White, D.J.; Page, S.R.; Cockcroft, J.R. Effect of oral vitamin E (alpha-tocopherol) supplementation on vascular endothelial function in type 2 diabetes mellitus. Diabet Med. 1999, 16, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; OʼDriscoll, G.; Rankin, J.M.; Maiorana, A.J.; Taylor, R.R. Beneficial effect of vitamin E administration on nitric oxide function in subjects with hypercholesterolaemia. Clin. Sci. (Lond) 1998, 95, 361–367. [Google Scholar] [CrossRef]
- Pinkney, J.H.; Downs, L.; Hopton, M.; Mackness, M.I.; Bolton, C.H. Endothelial dysfunction in type 1 diabetes mellitus: Relationship with LDL oxidation and the effects of vitamin E. Diabet Med. 1999, 16, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Shab-Bidar, S.; Neyestani, T.R.; Djazayery, A.; Eshraghian, M.R.; Houshiarrad, A.; Gharavi, A.; Kalayi, A.; Shariatzadeh, N.; Zahedirad, M.; Khalaji, N.; et al. Regular consumption of vitamin D-fortified yogurt drink (Doogh) improved endothelial biomarkers in subjects with type 2 diabetes: A randomized double-blind clinical trial. BMC Med. 2011, 9, 125. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Dove, F.J.; Khan, F.; Lang, C.C.; Belch, J.J.; Struthers, A.D. Effects of vitamin D supplementation on markers of vascular function after myocardial infarction-a randomised controlled trial. Int. J. Cardiol. 2013, 167, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Mah, E.; Pei, R.; Guo, Y.; Ballard, K.D.; Barker, T.; Rogers, V.E.; Parker, B.A.; Taylor, A.W.; Traber, M.G.; Volek, J.S.; et al. γ-Tocopherol-rich supplementation additively improves vascular endothelial function during smoking cessation. Free Radic. Biol. Med. 2013, 65, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, T.; Kawano, H.; Kugiyama, K.; Hirashima, O.; Ohgushi, M.; Tsunoda, R.; Moriyama, Y.; Miyao, Y.; Yoshimura, M.; Ogawa, H.; et al. Vitamin E administration improves impairment of endothelium-dependent vasodilation in patients with coronary spastic angina. J. Am. Coll. Cardiol. 1998, 32, 1672–1679. [Google Scholar] [CrossRef] [PubMed]
- Neunteufl, T.; Kostner, K.; Katzenschlager, R.; Zehetgruber, M.; Maurer, G.; Weidinger, F. Additional benefit of vitamin E supplementation to simvastatin therapy on vasoreactivity of the brachial artery of hypercholesterolemic men. J. Am. Coll. Cardiol. 1998, 32, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Borovnicar, A.; Keber, I.; Stavljenic Rukavina, A.; Yaletel Kragelj, L. Improvement of early functional atherosclerotic changes in males with hypercholesterolemia after vitamin E supplementation. Pflugers Arch. 2000, 440, R126–R128. [Google Scholar] [CrossRef] [PubMed]
- Economides, P.A.; Khaodhiar, L.; Caselli, A.; Caballero, A.E.; Keenan, H.; Bursell, S.E.; King, G.L.; Johnstone, M.T.; Horton, E.S.; Veves, A. The effect of vitamin E on endothelial function of micro- and macrocirculation and left ventricular function in type 1 and type 2 diabetic patients. Diabetes 2005, 54, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Gepner, A.D.; Ramamurthy, R.; Krueger, D.C.; Korcarz, C.E.; Binkley, N.; Stein, J.H. A prospective randomized controlled trial of the effects of vitamin D supplementation on cardiovascular disease risk. PLoS One 2012, 7, e36617. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.A.; Pedersen-White, J.; Guo, D.H.; Stallmann-Jorgensen, I.S.; Keeton, D.; Huang, Y.; Shah, Y.; Zhu, H.; Dong, Y. Vitamin D3 supplementation for 16 weeks improves flow-mediated dilation in overweight African-American adults. Am. J. Hypertens 2011, 24, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Kugiyama, K.; Motoyama, T.; Doi, H.; Kawano, H.; Hirai, N.; Soejima, H.; Miyao, Y.; Takazoe, K.; Moriyama, Y.; Mizuno, Y.; et al. Improvement of endothelial vasomotor dysfunction by treatment with alpha-tocopherol in patients with high remnant lipoproteins levels. J. Am. Coll. Cardiol. 1999, 33, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Longenecker, C.T.; Hileman, C.O.; Carman, T.L.; Ross, A.C.; Seydafkan, S.; Brown, T.T.; Labbato, D.E.; Storer, N.; Tangpricha, V.; McComsey, G.A. Vitamin D supplementation and endothelial function in vitamin D deficient HIV-infected patients: A randomized placebo-controlled trial. Antivir. Ther. 2012, 17, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Neunteufl, T.; Priglinger, U.; Heher, S.; Zehetgruber, M.; Soregi, G.; Lehr, S.; Huber, K.; Maurer, G.; Weidinger, F.; Kostner, K. Effects of vitamin E on chronic and acute endothelial dysfunction in smokers. J. Am. Coll. Cardiol. 2000, 35, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Paolisso, G.; Tagliamonte, M.R.; Barbieri, M.; Zito, G.A.; Gambardella, A.; Varricchio, G.; Ragno, E.; Varricchio, M. Chronic vitamin E administration improves brachial reactivity and increases intracellular magnesium concentration in type II diabetic patients. J. Clin. Endocrinol. Metab. 2000, 85, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Skyrme-Jones, R.A.; O’Brien, R.C.; Berry, K.L.; Meredith, I.T. Vitamin E supplementation improves endothelial function in type I diabetes mellitus: A randomized, placebo-controlled study. J. Am. Coll. Cardiol. 2000, 36, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Sugden, J.A.; Davies, J.I.; Witham, M.D.; Morris, A.D.; Struthers, A.D. Vitamin D improves endothelial function in patients with type 2 diabetes mellitus and low vitamin D levels. Diabet Med. 2008, 25, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Adams, F.; Kabir, G.; Kennedy, G.; Belch, J.J.; Khan, F. Effect of short-term vitamin D supplementation on markers of vascular health in South Asian women living in the UK—A randomised controlled trial. Atherosclerosis 2013, 230, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Dove, F.J.; Dryburgh, M.; Sugden, J.A.; Morris, A.D.; Struthers, A.D. The effect of different doses of vitamin D(3) on markers of vascular health in patients with type 2 diabetes: A randomised controlled trial. Diabetologia 2010, 53, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Witham, M.D.; Dove, F.J.; Sugden, J.A.; Doney, A.S.; Struthers, A.D. The effect of vitamin D replacement on markers of vascular health in stroke patients—A randomised controlled trial. Nutr. Metab. Cardiovas. Dis. 2012, 22, 864–870. [Google Scholar] [CrossRef]
- Witham, M.D.; Price, R.J.; Struthers, A.D.; Donnan, P.T.; Messow, C.M.; Ford, I.; McMurdo, M.E. Cholecalciferol treatment to reduce blood pressure in older patients with isolated systolic hypertension: The VitDISH randomized controlled trial. JAMA Intern. Med. 2013, 173, 1672–1679. [Google Scholar] [PubMed]
- Yiu, Y.F.; Yiu, K.H.; Siu, C.W.; Chan, Y.H.; Li, S.W.; Wong, L.Y.; Lee, S.W.; Tam, S.; Wong, E.W.; Lau, C.P.; et al. Randomized controlled trial of vitamin D supplement on endothelial function in patients with type 2 diabetes. Atherosclerosis 2013, 227, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.A.; von Konigsmark, M.; Simons, J.; Stocker, R.; Celermajer, D.S. Vitamin E ingestion does not improve arterial endothelial dysfunction in older adults. Atherosclerosis 1999, 143, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Shab-Bidar, S.; Mazloum, Z.; Mousavi-Shirazifard, Z. Daily vitamin E supplementation does not improve metabolic and glycemic control in type 2 diabetic patients: A double blinded randomized controlled trial. J. Diabetes 2013, 5, 57–58. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, A.M.; Rondo, P.H.; Luzia, L.A.; DʼAbronzo, F.H.; Illison, V.K. The effects of lipoic acid and alpha-tocopherol supplementation on the lipid profile and insulin sensitivity of patients with type 2 diabetes mellitus: A randomized, double-blind, placebo-controlled trial. Diabetes Res. Clin. Pract. 2011, 92, 253–260. [Google Scholar]
- Paolisso, G.; DʼAmore, A.; Giugliano, D.; Ceriello, A.; Varricchio, M.; DʼOnofrio, F. Pharmacologic doses of vitamin E improve insulin action in healthy subjects and non-insulin-dependent diabetic patients. Am. J. Clin. Nutr. 1993, 57, 650–656. [Google Scholar] [PubMed]
- Paolisso, G.; di Maro, G.; Galzerano, D.; Cacciapuoti, F.; Varricchio, G.; Varricchio, M.; D’Onofrio, F. Pharmacological doses of vitamin E and insulin action in elderly subjects. Am. J. Clin. Nutr. 1994, 59, 1291–1296. [Google Scholar] [PubMed]
- Monsen, E.R. Dietary reference intakes for the antioxidant nutrients: Vitamin C, vitamin E, selenium, and carotenoids. J. Am. Diet. Assoc. 2000, 100, 637–640. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.R., 3rd; Pastor-Barriuso, R.; Dalal, D.; Riemersma, R.A.; Appel, L.J.; Guallar, E. Meta-analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann. Intern. Med. 2005, 142, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Nikolova, D.; Gluud, L.L.; Simonetti, R.G.; Gluud, C. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: Systematic review and meta-analysis. JAMA 2007, 297, 842–857. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; Benjamin, E.J.; DʼAgostino, R.B.; Wolf, M.; Vasan, R.S. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008, 117, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Dobnig, H.; Pilz, S.; Scharnagl, H.; Renner, W.; Seelhorst, U.; Wellnitz, B.; Kinkeldei, J.; Boehm, B.O.; Weihrauch, G.; Maerz, W. Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 2008, 168, 1340–1349. [Google Scholar] [CrossRef] [PubMed]
- Dalan, R.; Liew, H.; Tan, A.W.; Chew, D.E.; Leow, M.K. Vitamin D and the endothelium: Basic, translational and clinical research updates. IJC Metab. Endocr. 2014, 4, 4–17. [Google Scholar] [CrossRef]
- Heaney, R.P. Vitamin D and calcium interactions: Functional outcomes. Am. J. Clin. Nutr. 2008, 88, 541S–544S. [Google Scholar] [PubMed]
- Voutilainen, S.; Nurmi, T.; Mursu, J.; Rissanen, T.H. Carotenoids and cardiovascular health. Am. J. Clin. Nutr. 2006, 83, 1265–1271. [Google Scholar] [PubMed]
- Geleijnse, J.M.; Vermeer, C.; Grobbee, D.E.; Schurgers, L.J.; Knapen, M.H.; van der Meer, I.M.; Hofman, A.; Witteman, J.C. Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: The Rotterdam Study. J. Nutr. 2004, 134, 3100–3105. [Google Scholar] [PubMed]
- Juanola-Falgarona, M.; Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Corella, D.; Estruch, R.; Ros, E.; Fito, M.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; et al. Dietary intake of vitamin K is inversely associated with mortality risk. J. Nutr. 2014, 144, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Bjorkhem, I.; Wretlind, B.; Diczfalusy, U.; Henriksson, P.; Freyschuss, A. Effect of ascorbic acid on microcirculation in patients with type II diabetes: A randomized placebo-controlled cross-over study. Clin Sci (Lond) 2005, 108, 507–513. [Google Scholar] [CrossRef]
- Sankhla, M.; Sharma, T.K.; Mathur, K.; Rathor, J.S.; Butolia, V.; Gadhok, A.K.; Vardey, S.K.; Sinha, M.; Kaushik, G.G. Relationship of oxidative stress with obesity and its role in obesity induced metabolic syndrome. Clin. Lab. 2012, 58, 385–392. [Google Scholar] [PubMed]
- De Roos, N.M.; Bots, M.L.; Schouten, E.G.; Katan, M.B. Within-subject variability of flow-mediated vasodilation of the brachial artery in healthy men and women: Implications for experimental studies. Ultrasound Med. Biol. 2003, 29, 401–406. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joris, P.J.; Mensink, R.P. Effects of Supplementation with the Fat-Soluble Vitamins E and D on Fasting Flow-Mediated Vasodilation in Adults: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 1728-1743. https://doi.org/10.3390/nu7031728
Joris PJ, Mensink RP. Effects of Supplementation with the Fat-Soluble Vitamins E and D on Fasting Flow-Mediated Vasodilation in Adults: A Meta-Analysis of Randomized Controlled Trials. Nutrients. 2015; 7(3):1728-1743. https://doi.org/10.3390/nu7031728
Chicago/Turabian StyleJoris, Peter J., and Ronald P. Mensink. 2015. "Effects of Supplementation with the Fat-Soluble Vitamins E and D on Fasting Flow-Mediated Vasodilation in Adults: A Meta-Analysis of Randomized Controlled Trials" Nutrients 7, no. 3: 1728-1743. https://doi.org/10.3390/nu7031728