Maternal Dietary Patterns during Pregnancy in Relation to Offspring Forearm Fractures: Prospective Study from the Danish National Birth Cohort

Abstract
:1. Introduction
2. Materials and Methods
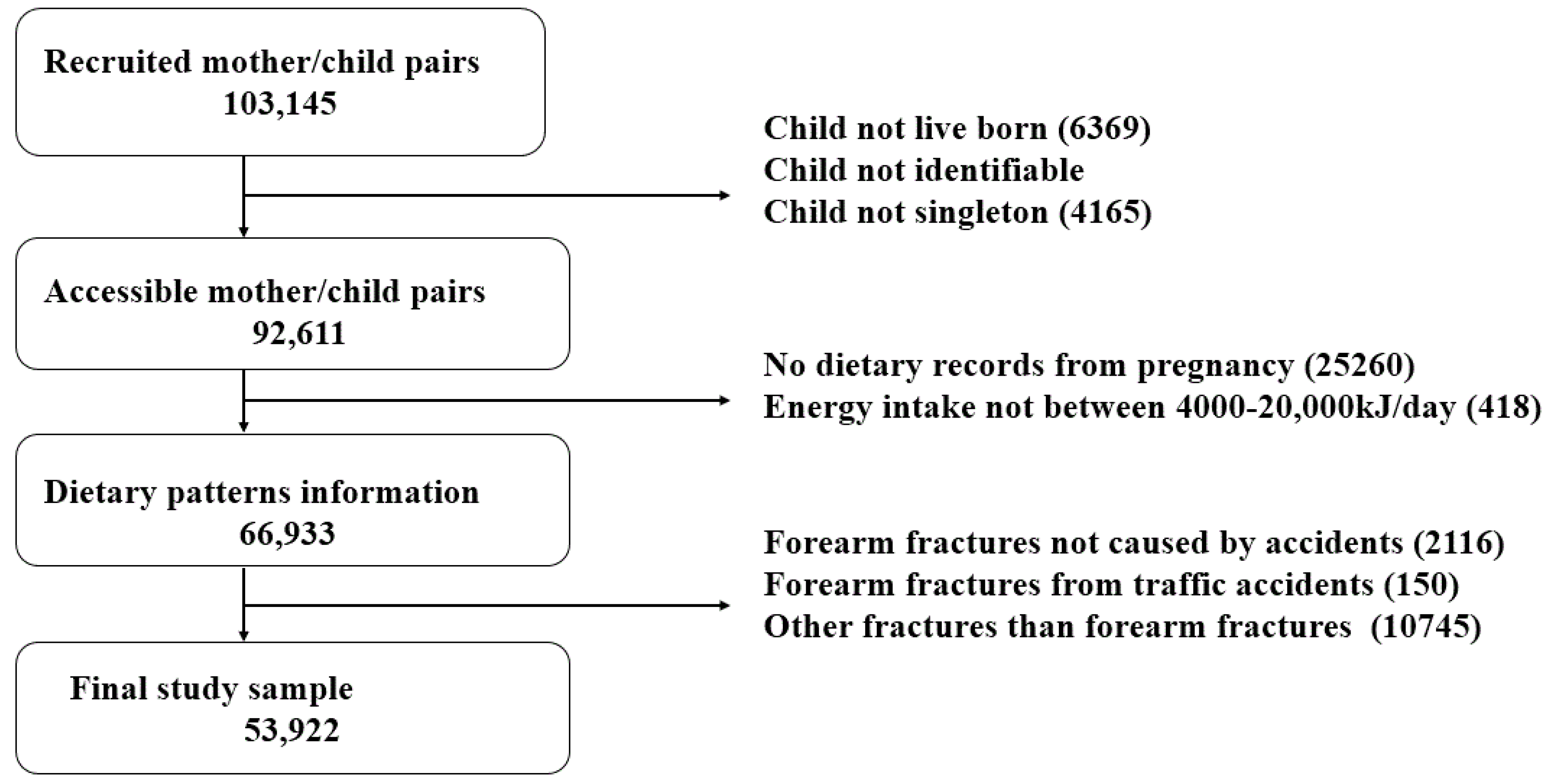
2.1. Study Population
2.2. Exposure
2.2.1. Assessment of Nutrient Intake
2.2.2. Assessment of Dietary Patterns
2.3. Outcome

{kind=link}
{kind=link}
| Prudent | Alcohol | Western | Nordic | Shellfish | Sweets | Traditional | |
|---|---|---|---|---|---|---|---|
| High In | Vegetables | Alcohol | Meat | Dark bread | Fish | White bread | Poultry |
| Legumes | Soy | Potatoes | Nordic fruit | Shellfish | Cakes | Meat | |
| Root | Root | White bread | Cheese | Lamb | Margarine | Low-fat milk | |
| Fruit | Soft drinks | Egg | Banana | Oils | French fries | Meat | |
| Corn | Berries | Margarine | Cakes | Egg | Soft drinks, sugar | Water | |
| Low In | Meat | Pasta/rice | Vegetables | French fries | Soft drinks, diet | Low-fat milk | Full fat milk |
| French Fries | Yogurt | Fruit | Candy/snack | Candy/snack | Cabbage | Coffee | |
| Margarine | Poultry | Breakfast cereals | Soft drinks | Low-fat milk | Fruits | Butter | |
| White bread | Cheese | Nuts | Processed meat | Coffee | Fish | Potatoes | |
| Candy/snack | Bread | Water | Desserts | White bread | Legumes | White bread |
2.4. Statistical Methods

3. Results
| Forearm Fracture | |||
|---|---|---|---|
| Yes n = 4222 | No n = 49,700 | p | |
| Maternal age (mean) | 30.44 | 30.46 | 0.80 a |
| Pre-pregnancy BMI, kg m−2 (mean) | 23.66 | 23.46 | 0.002 a |
| Occupational status (%) | |||
| High | 23.5 | 22.9 | 0.50 b |
| Medium | 34.6 | 35.0 | |
| Skilled | 26.1 | 25.7 | |
| Student | 4.5 | 5.1 | |
| Unskilled | 9.6 | 9.8 | |
| Unemployed | 1.6 | 1.5 | |
| Cohabitation status (%) | |||
| Single | 1.56 | 1.67 | 0.60 b |
| Couple | 98.4 | 98.3 | |
| Smoking (%) | |||
| Non-smoker | 76.5 | 76.1 | 0.83 b |
| Occasional smoker | 12.0 | 12.2 | |
| <15 cigarettes/day | 9.8 | 9.9 | |
| ≥15 cigarettes/day | 1.6 | 1.8 | |
| Parity (%) | |||
| Nulliparous | 48.6 | 51.7 | <0.001 b |
| 1 child | 37.0 | 34.0 | |
| 2 children | 12.4 | 11.7 | |
| 3+ children | 2.0 | 2.6 | |
| Physical activity, minutes week−1 (%) | |||
| 0 | 54.3 | 55.2 | 0.011 b |
| 1–44 | 15.5 | 14.9 | |
| 45–74 | 10.9 | 11.0 | |
| 75–149 | 10.9 | 11.8 | |
| ≥150 | 8.3 | 7.1 | |
| Child sex (%) | |||
| Male | 50.3 | 50.4 | 0.89 b |
| Female | 49.7 | 49.6 | |
| Season of birth (%) | |||
| Mar/Apr/May | 23.3 | 23.4 | 0.023 b |
| Jun/Jul/Aug | 26.0 | 26.5 | |
| Sep/Oct/Nov | 28.5 | 26.5 | |
| Dec/Jan/Feb | 22.2 | 23.6 | |
| Gestational age (mean) | 280.5 | 280.2 | 0.15 a |
| Birth weight (mean) | 3624 | 3583 | <0.001 a |
| Cases | Crude HR (95% CI) | p | Adjusted HR (95% CI) * | p | ||
|---|---|---|---|---|---|---|
| Prudent pattern | Q1 | 860 | 1.00 | 0.81 a | 1.00 | 0.79 a |
| Q2 | 856 | 1.01 (0.92, 1.11) | 0.98 b | 1.01 (0.91, 1.11) | 0.87 b | |
| Q3 | 859 | 1.02 (0.92, 1.12) | 1.01 (0.92, 1.12) | |||
| Q4 | 820 | 0.97 (0.88, 1.07) | 0.97 (0.88, 1.07) | |||
| Q5 | 857 | 1.03 (0.93, 1.13) | 1.03 (0.93, 1.14) | |||
| Alcohol pattern | Q1 | 823 | 1.00 | 0.05 a | 1.00 | 0.05 a |
| Q2 | 806 | 0.95 (0.86, 1.05) | 0.86 b | 0.95 (0.86, 1.05) | 0.79 b | |
| Q3 | 917 | 1.10 (1.00, 1.20) | 1.09 (0.99, 1.20) | |||
| Q4 | 861 | 1.03 (0.93, 1.13) | 1.02 (0.93, 1.13) | |||
| Q5 | 845 | 0.99 (0.90, 1.09) | 0.99 (0.90, 1.09) | |||
| Western pattern | Q1 | 804 | 1.00 | 0.15 a | 1.00 | 0.20 a |
| Q2 | 841 | 1.04 (0.95, 1.15) | 0.06 b | 1.03 (0.94, 1.14) | 0.06 b | |
| Q3 | 828 | 1.04 (0.94, 1.14) | 1.03 (0.93, 1.14) | |||
| Q4 | 903 | 1.12 (1.02, 1.23) | 1.11 (1.01, 1.23) | |||
| Q5 | 876 | 1.09 (0.99, 1.20) | 1.09 (0.98, 1.21) | |||
| Nordic pattern | Q1 | 844 | 1.00 | 0.50 a | 1.00 | 0.47 a |
| Q2 | 850 | 0.98 (0.89, 1.08) | 0.63 b | 0.98 (0.89, 1.08) | 0.59 b | |
| Q3 | 808 | 0.94 (0.85, 1.03) | 0.93 (0.85, 1.03) | |||
| Q4 | 880 | 1.02 (0.93, 1.12) | 1.02 (0.92, 1.12) | |||
| Q5 | 870 | 0.99 (0.90, 1.09) | 1.00 (0.90, 1.10) | |||
| Seafood pattern | Q1 | 860 | 1.00 | 0.20 a | 1.00 | 0.19 a |
| Q2 | 803 | 0.94 (0.85, 1.03) | 0.91 b | 0.94 (0.85, 1.03) | 0.52 b | |
| Q3 | 906 | 1.05 (0.95, 1.15) | 1.05 (0.96, 1.16) | |||
| Q4 | 833 | 0.96 (0.87, 1.06) | 0.97 (0.88, 1.08) | |||
| Q5 | 850 | 0.99 (0.90, 1.09) | 1.01 (0.91, 1.12) | |||
| Sweets pattern | Q1 | 866 | 1.00 | 0.06 a | 1.00 | 0.05 a |
| Q2 | 883 | 1.02 (0.93, 1.12) | 0.79 b | 1.02 (0.93, 1.12) | 0.98 b | |
| Q3 | 814 | 0.94 (0.86, 1.04) | 0.94 (0.86, 1.04) | |||
| Q4 | 793 | 0.92 (0.83, 1.01) | 0.92 (0.84, 1.02) | |||
| Q5 | 896 | 1.04 (0.95, 1.14) | 1.05 (0.96, 1.16) | |||
| Traditional pattern | Q1 | 884 | 1.00 | 0.94 a | 1.00 | 0.85 a |
| Q2 | 876 | 1.01 (0.92, 1.11) | 0.70 b | 1.00 (0.91, 1.09) | 0.41 b | |
| Q3 | 826 | 0.97 (0.88, 1.07) | 0.95 (0.86, 1.05) | |||
| Q4 | 843 | 1.00 (0.91, 1.10) | 0.98 (0.89, 1.08) | |||
| Q5 | 823 | 0.99 (0.90, 1.09) | 0.97 (0.88, 1.07) |
| Estimated intake | Crude HR (95% CI) | Adjusted HR (95% CI) * | Mutually Adj. HR (95% CI) ** |
|---|---|---|---|
| Sugar sweetened soft drinks, grams per day | |||
| Q1 (0–45) | 1.00 | 1.00 | 1.00 |
| Q2 (46–80) | 0.92 (0.84, 1.02) | 0.93 (0.84, 1.02) | 1.08 (0.98, 1.19) |
| Q3 (81–149) | 1.01 (0.92, 1.11) | 1.01 (0.92, 1.11) | 1.10 (1.00, 1.21) |
| Q4 (150–257) | 0.98 (0.89, 1.08) | 0.98 (0.89, 1.08) | 1.07 (0.97, 1.18) |
| Q5 (258–4000) | 0.96 (0.88, 1.06) | 0.97 (0.88, 1.07) | 1.05 (0.95, 1.16) |
| p = 0.42 a; p = 0.71 b | p = 0.43 a; p = 0.80 b | p = 0.38 a; p = 0.81 b | |
| Artificially sweetened soft drinks, grams per day | |||
| 0 | 1.00 | 1.00 | 1.00 |
| >0–10 | 0.98 (0.87, 1.10) | 0.98 (0.87, 1.11) | 0.98 (0.87, 1.10) |
| ≥10–60 | 1.06 (0.98, 1.15) | 1.06 (0.98, 1.15) | 1.06 (0.98, 1.15) |
| ≥60 | 1.14 (1.05, 1.23) | 1.12 (1.04, 1.21) | 1.12 (1.03, 1.21) |
| p = 0.005 a; p = 0.02 b | p = 0.02 a; p = 0.08 b | p = 0.03 a; p = 0.08 b | |
| Carbonated sugar sweetened soft drinks, servings per week | |||
| Never | 1.00 | 1.00 | 1.00 |
| <1 | 0.92 (0.84, 1.02) | 0.93 (0.84, 1.02) | 0.94 (0.86, 1.04) |
| 1–6 | 0.96 (0.88, 1.05) | 0.97 (0.89, 1.05) | 0.97 (0.89, 1.07) |
| ≥7 | 0.93 (0.82, 1.05) | 0.93 (0.82, 1.06) | 0.96 (0.84, 1.11) |
| p = 0.39 a; p = 0.38 b | p = 0.44 a; p = 0.48 b | p = 0.34 a; p = 0.72 b | |
| Carbonated artificially sweetened soft drinks, servings per week | |||
| Never | 1.00 | 1.00 | 1.00 |
| <1 | 1.04 (0.95, 1.14) | 1.03 (0.94, 1.14) | 1.03 (0.94, 1.14) |
| 1–6 | 1.10 (1.01, 1.19) | 1.08 (1.00, 1.18) | 1.07 (0.98, 1.17) |
| ≥7 | 1.02 (0.87, 1.19) | 0.99 (0.84, 1.16) | 0.95 (0.80, 1.14) |
| p = 0.15 a; p = 0.09 b | p =0.28 a; p = 0.26 b | p = 0.34 a; p = 0.50 b | |
| Noncarbonated sugar sweetened soft drinks, servings per week | |||
| Never | 1.00 | 1.00 | 1.00 |
| <1 | 0.91 (0.82, 1.00) | 0.90 (0.82, 1.00) | 0.93 (0.84, 1.02) |
| 1–6 | 0.95 (0.88, 1.02) | 0.94 (0.87, 1.02) | 0.96 (0.89, 1.05) |
| ≥7 | 0.98 (0.90, 1.06) | 0.97 (0.89, 1.05) | 1.00 (0.91, 1.09) |
| p = 0.21 a; p = 0.54 b | p = 0.17 a; p = 0.40 b | p = 0.43 a; p = 0.91 b | |
| Noncarbonated artificially sweetened soft drinks, servings per week | |||
| Never | 1.00 | 1.00 | 1.00 |
| <1 | 0.96 (0.85, 1.08) | 0.96 (0.85, 1.08) | 0.95 (0.84, 1.08) |
| 1–6 | 1.05 (0.96, 1.15) | 1.05 (0.56, 1.15) | 1.04 (0.95, 1.15) |
| ≥7 | 1.13 (1.04, 1.24) | 1.13 (1.03, 1.23) | 1.11 (1.01, 1.23) |
| p = 0.02 a; p = 0.005 b | p = 0.04 a; p = 0.009 b | p = 0.10 a; p = 0.03 b | |
| Estimated intake | Crude HR (95% CI) | p | Adjusted HR (95% CI) * | p * |
|---|---|---|---|---|
| Meat | ||||
| Q1 | 0.98 (0.89, 1.08) | 0.35 a | 0.99 (0.90, 1.09) | 0.33 a |
| Q2 | 0.98 (0.94, 1.08) | 0.97 b | 0.99 (0.90, 1.08) | 0.89 b |
| Q3 | 0.91 (0.89, 1.00) | 0.91 (0.83, 1.00) | ||
| Q4 | 0.98 (0.90, 1.08) | 0.98 (0.89, 1.08) | ||
| Q5 | 1.00 | 1.00 | ||
| Protein, total | ||||
| Q1 | 0.97 (0.88, 1.07) | 0.70 a | 0.99 (0.90, 1.09) | 0.70 a |
| Q2 | 1.04 (0.94, 1.14) | 0.49 b | 1.05 (0.95, 1.15) | 0.75 b |
| Q3 | 0.98 (0.89, 1.08) | 0.99 (0.90, 1.08) | ||
| Q4 | 0.99 (0.90, 1.09) | 0.99 (0.90, 1.09) | ||
| Q5 | 1.00 | 1.00 | ||
| Animal protein | ||||
| Q1 | 0.96 (0.88, 1.06) | 0.67 a | 0.96 (0.88, 1.06) | 0.67 a |
| Q2 | 1.00 (0.91, 1.10) | 0.34 b | 1.00 (0.91, 1.10) | 0.41 b |
| Q3 | 0.95 (0.86, 1.04) | 0.95 (0.86, 1.04) | ||
| Q4 | 0.96 (0.87, 1.05) | 0.96 (0.87, 1.05) | ||
| Q5 | 1.00 | 1.00 | ||
| Vegetable protein | ||||
| Q1 | 0.99 (0.90, 1.09) | 0.62 a | 0.99 (0.90, 1.08) | 0.58 a |
| Q2 | 0.95 (0.86, 1.05) | 0.97 b | 0.95 (0.86, 1.04) | 0.87 b |
| Q3 | 0.95 (0.86, 1.04) | 0.95 (0.86, 1.04) | ||
| Q4 | 0.94 (0.85, 1.03) | 0.94 (0.85, 1.03) | ||
| Q5 | 1.00 | 1.00 |

4. Discussion
4.1. Western Diet in Relation to Bone Health
4.2. Our Results in Relation to Existing Knowledge
4.3. Strengths and Limitations
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Heaney, R.P.; Abrams, S.; Dawson-Hughes, B.; Looker, A.; Marcus, R.; Matkovic, V.; Weaver, C. Peak bone mass. Osteoporos. Int. 2000, 11, 985–1009. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Westlake, S.; Harvey, N.; Javaid, K.; Dennison, E.; Hanson, M. Review: Developmental origins of osteoporotic fracture. Osteoporos. Int. 2006, 17, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C. Epidemiology of osteoporotic fracture: Looking to the future. Rheumatology 2005, 44, iv36–iv40. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Crozier, S.R.; Harvey, N.C.; Gale, C.R.; Dennison, E.M.; Boucher, B.J.; Arden, N.K.; Godfrey, K.M.; Cooper, C. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, C.; Javaid, M.K.; Mahon, P.; Yaqub, M.K.; Harvey, N.C.; Godfrey, K.M.; Noble, J.A.; Cooper, C.; Papageorghiou, A.T. The effect of maternal vitamin D concentration on fetal bone. J. Clin. Endocrinol. Metab. 2012, 97, E2070–E2077. [Google Scholar] [CrossRef] [PubMed]
- Sayers, A.; Tobias, J.H. Estimated maternal ultraviolet B exposure levels in pregnancy influence skeletal development of the child. J. Clin. Endocrinol. Metab. 2009, 94, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Wills, A.K.; Fraser, A.; Sayers, A.; Fraser, W.D.; Tobias, J.H. Association of maternal vitamin D status during pregnancy with bone-mineral content in offspring: A prospective cohort study. Lancet 2013, 381, 2176–2183. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Whitehouse, A.J.; Hart, P.; Kusel, M.; Mountain, J.; Lye, S.; Pennell, C.; Walsh, J.P. Maternal vitamin D status during pregnancy and bone mass in offspring at 20 years of age: A prospective cohort study. J. Bone Miner. Res. 2014, 29, 227–233. [Google Scholar]
- Jones, G. Early life nutrition and bone development in children. Nestle Nutr. Workshop Ser. Pediatr. Program. 2011, 68, 227–233. [Google Scholar] [PubMed]
- Jones, G.; Riley, M.D.; Dwyer, T. Maternal diet during pregnancy is associated with bone mineral density in children: A longitudinal study. Eur. J. Clin. Nutr. 2000, 54, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Tobias, J.H.; Steer, C.D.; Emmett, P.M.; Tonkin, R.J.; Cooper, C.; Ness, A.R. Bone mass in childhood is related to maternal diet in pregnancy. Osteoporos. Int. 2005, 16, 1731–1741. [Google Scholar] [CrossRef] [PubMed]
- Ganpule, A.; Yajnik, C.S.; Fall, C.H.; Rao, S.; Fisher, D.J.; Kanade, A.; Cooper, C.; Naik, S.; Joshi, N.; Lubree, H.; et al. Bone mass in Indian children—Relationships to maternal nutritional status and diet during pregnancy: The Pune Maternal Nutrition Study. J. Clin. Endocrinol. Metab. 2006, 91, 2994–3001. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.C.; O’Brien, K.O.; Nathanson, M.S.; Caulfield, L.E.; Mancini, J.; Witter, F.R. Fetal femur length is influenced by maternal dairy intake in pregnant African American adolescents. Am. J. Clin. Nutr. 2003, 77, 1248–1254. [Google Scholar] [PubMed]
- Yin, J.; Dwyer, T.; Riley, M.; Cochrane, J.; Jones, G. The association between maternal diet during pregnancy and bone mass of the children at age 16. Eur. J. Clin. Nutr. 2010, 64, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Cole, Z.A.; Gale, C.R.; Javaid, M.K.; Robinson, S.M.; Law, C.; Boucher, B.J.; Crozier, S.R.; Godfrey, K.M.; Dennison, E.M.; Cooper, C. Maternal dietary patterns during pregnancy and childhood bone mass: A longitudinal study. J. Bone Miner. Res. 2009, 24, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Heppe, D.H.; Medina-Gomez, C.; Hofman, A.; Franco, O.H.; Rivadeneira, F.; Jaddoe, V.W. Maternal first-trimester diet and childhood bone mass: The Generation R Study. Am. J. Clin. Nutr. 2013, 98, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Melbye, M.; Olsen, S.F.; Sorensen, T.I.; Aaby, P.; Andersen, A.M.; Taxbol, D.; Hansen, K.D.; Juhl, M.; Schow, T.B.; et al. The Danish National Birth Cohort—Its background, structure and aim. Scand. J. Public Health 2001, 29, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Clark, E.M.; Tobias, J.H.; Ness, A.R. Association between bone density and fractures in children: A systematic review and meta-analysis. Pediatrics 2006, 117, e291–e297. [Google Scholar] [CrossRef] [PubMed]
- Ryan, L.M. Forearm fractures in children and bone health. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.F.; Mikkelsen, T.B.; Knudsen, V.K.; Orozova-Bekkevold, I.; Halldorsson, T.I.; Strøm, M.; Osterdal, M.L. Data collected on maternal dietary exposures in the Danish National Birth Cohort. Paediatr. Perinat. Epidemiol. 2007, 21, 76–86. [Google Scholar] [CrossRef] [PubMed]
- National Food Institute—Technical University of Denmark (DTU). The Official Danish Food Composition Database. Available online: http://www.foodcomp.dk (accessed on 2 March 2009).
- Rasmussen, M.A.; Maslova, E.; Halldorsson, T.I.; Olsen, S.F. Characterization of dietary patterns in the danish national birth cohort in relation to preterm birth. PLoS ONE 2014, 9, e93644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, T.F.; Madsen, M.; Jorgensen, J.; Mellemkjoer, L.; Olsen, J.H. The Danish national hospital register. A valuable source of data for modern health sciences. Dan. Med. Bull. 1999, 46, 263–268. [Google Scholar] [PubMed]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Pedersen, L.; Sorensen, H.T. The Danish Civil Registration System as a tool in epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, P.; Mosekilde, L. Fracture risk in patients with celiac disease, Crohn’s disease, and ulcerative colitis: A nationwide follow-up study of 16,416 patients in Denmark. Am. J. Epidemiol. 2002, 156, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Horiguchi, H.; Oguma, E.; Miyamoto, K.; Hosoi, Y.; Kim, M.K.; Kayama, F. Dietary patterns associated with bone mineral density in premenopausal Japanese farmwomen. Am. J. Clin. Nutr. 2006, 83, 1185–1192. [Google Scholar] [PubMed]
- Hardcastle, A.C.; Aucott, L.; Fraser, W.D.; Reid, D.M.; Macdonald, H.M. Dietary patterns, bone resorption and bone mineral density in early post-menopausal Scottish women. Eur. J. Clin. Nutr. 2011, 65, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Massey, L.K. Dietary animal and plant protein and human bone health: A whole foods approach. J. Nutr. 2003, 133, 862S–865S. [Google Scholar] [PubMed]
- Remer, T.; Krupp, D.; Shi, L. Dietary protein’s and dietary acid load’s influence on bone health. Crit. Rev. Food Sci. Nutr. 2014, 54, 1140–1150. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, S.; Mellstrom, D.; Strandvik, B. Fatty acid pattern in serum is associated with bone mineralisation in healthy 8-year-old children. Br. J. Nutr. 2009, 102, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Kelly, O.J.; Gilman, J.C.; Kim, Y.; Ilich, J.Z. Long-chain polyunsaturated fatty acids may mutually benefit both obesity and osteoporosis. Nutr. Res. 2013, 33, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Prentice, A. Diet, nutrition and the prevention of osteoporosis. Public Health Nutr. 2004, 7, 227–243. [Google Scholar] [CrossRef] [PubMed]
- Wynn, E.; Krieg, M.A.; Lanham-New, S.A.; Burckhardt, P. Postgraduate symposium: Positive influence of nutritional alkalinity on bone health. Proc. Nutr. Soc. 2010, 69, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, R.; McLaren, H.J. The acid-ash hypothesis revisited: A reassessment of the impact of dietary acidity on bone. J. Bone Miner. Metab. 2014, 32, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Adeva, M.M.; Souto, G. Diet-induced metabolic acidosis. Clin. Nutr. 2011, 30, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Hanley, D.A.; Whiting, S.J. Does a high dietary acid content cause bone loss, and can bone loss be prevented with an alkaline diet? J. Clin. Densitom. 2013, 16, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Simpson, M.E.; Duggal, S.; Keiver, K. Prenatal ethanol exposure has differential effects on fetal growth and skeletal ossification. Bone 2005, 36, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Fadel, R.A.; Persaud, T.V. Ossification of the vertebral column in the offspring of rats exposed to alcohol, acetaldehyde and caffeine. Exp. Toxicol. Pathol. 1993, 45, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Libuda, L.; Alexy, U.; Remer, T.; Stehle, P.; Schoenau, E.; Kersting, M. Association between long-term consumption of soft drinks and variables of bone modeling and remodeling in a sample of healthy German children and adolescents. Am. J. Clin. Nutr. 2008, 88, 1670–1677. [Google Scholar] [CrossRef] [PubMed]
- McGartland, C.; Robson, P.J.; Murray, L.; Cran, G.; Savage, M.J.; Watkins, D.; Rooney, M.; Boreham, C. Carbonated soft drink consumption and bone mineral density in adolescence: The Northern Ireland Young Hearts project. J. Bone Miner. Res. 2003, 18, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Wyshak, G. Teenaged girls, carbonated beverage consumption, and bone fractures. Arch. Pediatr. Adolesc. Med. 2000, 154, 610–613. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Jones, G. Soft drink and milk consumption, physical activity, bone mass, and upper limb fractures in children: A population-based case-control study. Calcif. Tissue Int. 2004, 75, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Namgung, R.; Tsang, R.C. Bone in the pregnant mother and newborn at birth. Clin. Chim. Acta 2003, 333, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Weiler, H.A. Long-term effects of gestational diabetes on offspring health are more pronounced in skeletal growth than body composition and glucose tolerance. Br. J. Nutr. 2010, 104, 1641–1649. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.C.; Javaid, M.K.; Arden, N.K.; Poole, J.R.; Crozier, S.R.; Robinson, S.M.; Inskip, H.M.; Godfrey, K.M.; Dennison, E.M.; Cooper, C. Maternal predictors of neonatal bone size and geometry: The Southampton Women’s Survey. J. Dev. Orig. Health Dis. 2010, 1, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Halldorsson, T.I.; Strom, M.; Petersen, S.B.; Olsen, S.F. Intake of artificially sweetened soft drinks and risk of preterm delivery: A prospective cohort study of 59,334 Danish pregnant women. Am. J. Clin. Nutr. 2010, 92, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, C.R.; Boullata, J.; McCauley, L.A. The potential toxicity of artificial sweeteners. AAOHN J. 2008, 56, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.L. Response of male rate to sodium saccharin ingestion: Urine composition and mineral balance. Food Cosmet. Toxicol. 1979, 17, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Friis, S.; Kruger Kjaer, S.; Stripp, C.; Overvad, K. Reproducibility and relative validity of a self-administered semiquantitative food frequency questionnaire applied to younger women. J. Clin. Epidemiol. 1997, 50, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, T.B.; Osler, M.; Olsen, S.F. Validity of protein, retinol, folic acid and n-3 fatty acid intakes estimated from the food-frequency questionnaire used in the Danish National Birth Cohort. Public Health Nutr. 2006, 9, 771–778. [Google Scholar] [PubMed]
- Mikkelsen, T.B.; Olsen, S.F.; Rasmussen, S.E.; Osler, M. Relative validity of fruit and vegetable intake estimated by the food frequency questionnaire used in the Danish National Birth Cohort. Scand. J. Public Health 2007, 35, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M. The role of nutrition on optimizing peak bone mass. Asia Pac. J. Clin. Nutr. 2008, 17, 135–137. [Google Scholar] [PubMed]
- Pitukcheewanont, P.; Austin, J.; Chen, P.; Punyasavatsut, N. Bone health in children and adolescents: Risk factors for low bone density. Pediatr. Endocrinol. Rev. 2013, 10, 318–335. [Google Scholar] [PubMed]
- Mathison, D.J.; Agrawal, D. An update on the epidemiology of pediatric fractures. Pediatr. Emerg. Care. 2010, 26, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petersen, S.B.; Rasmussen, M.A.; Olsen, S.F.; Vestergaard, P.; Mølgaard, C.; Halldorsson, T.I.; Strøm, M. Maternal Dietary Patterns during Pregnancy in Relation to Offspring Forearm Fractures: Prospective Study from the Danish National Birth Cohort. Nutrients 2015, 7, 2382-2400. https://doi.org/10.3390/nu7042382
Petersen SB, Rasmussen MA, Olsen SF, Vestergaard P, Mølgaard C, Halldorsson TI, Strøm M. Maternal Dietary Patterns during Pregnancy in Relation to Offspring Forearm Fractures: Prospective Study from the Danish National Birth Cohort. Nutrients. 2015; 7(4):2382-2400. https://doi.org/10.3390/nu7042382
Chicago/Turabian StylePetersen, Sesilje B., Morten A. Rasmussen, Sjurdur F. Olsen, Peter Vestergaard, Christian Mølgaard, Thorhallur I. Halldorsson, and Marin Strøm. 2015. "Maternal Dietary Patterns during Pregnancy in Relation to Offspring Forearm Fractures: Prospective Study from the Danish National Birth Cohort" Nutrients 7, no. 4: 2382-2400. https://doi.org/10.3390/nu7042382