Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial

Abstract
:1. Introduction
2. Experimental Section
2.1. Subjects
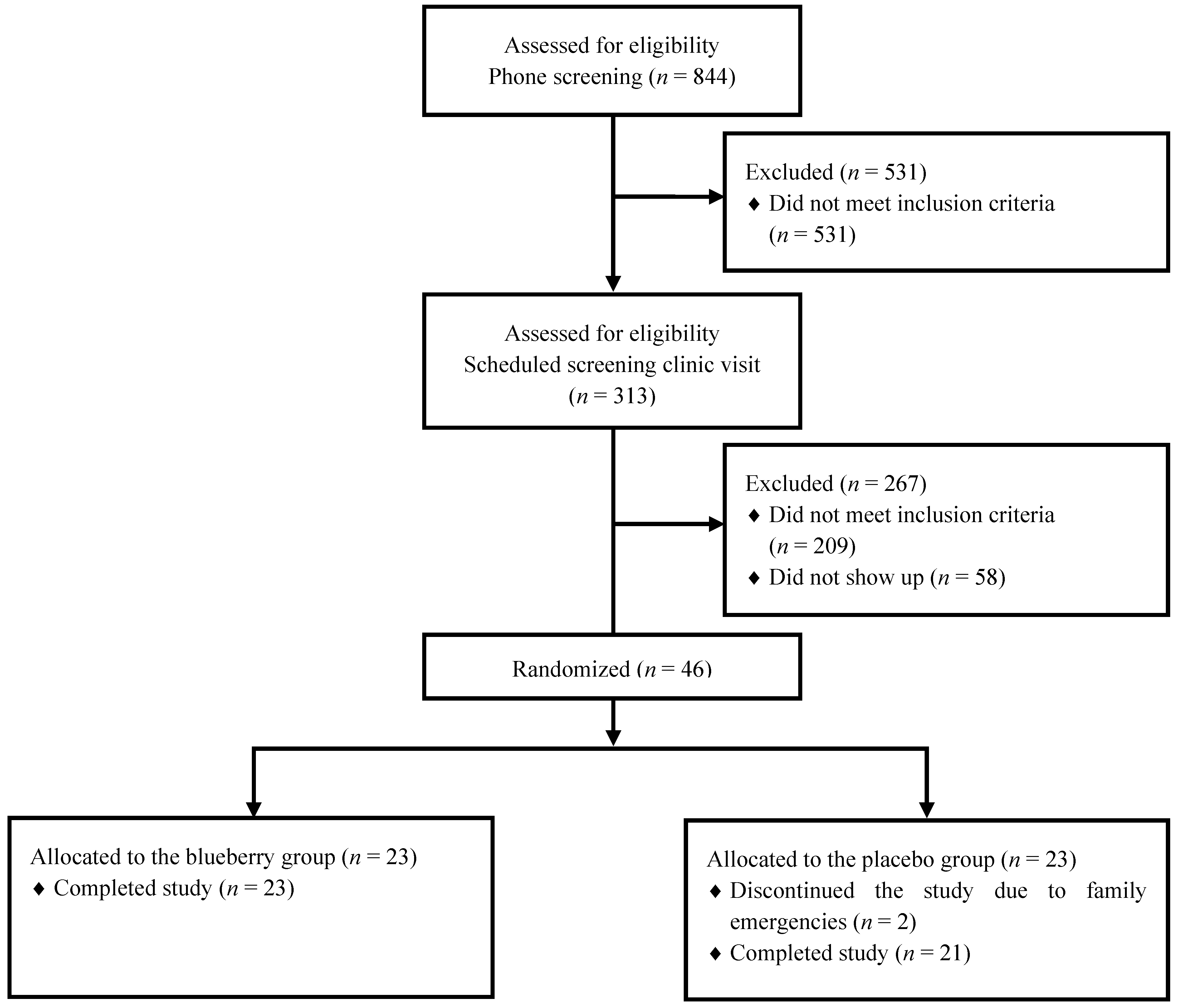
2.2. Study Design

{kind=link}
{kind=link}
| Nutritional Composition | Blueberry | Placebo | Ingredients | Blueberry | Placebo |
|---|---|---|---|---|---|
| Energy, kcal * | 242 | 241 | Yoplait® 99% fat-free creamy vanilla yogurt, g | 125 | 130 |
| Carbohydrate, g | 49.7 | 51 | Skim milk, g | 105 | 115 |
| Fiber, g | 4.5 | 4.5 | Freeze-dried blueberry powder, g | 22.5 | — |
| Protein, g | 8.0 | 7.9 | Imitation vanilla flavor, g | 5 | — |
| Fat, g | 1.1 | 1.0 | Sugar, g | — | 14 |
| Saturated fat, g | 0.6 | 0.6 | Splenda, g | 1 | — |
| Sodium, mg | 110.5 | 114.6 | Benefiber, g | — | 5.2 |
| Vitamin C, mg | 2.7 | 0 | Artificial blueberry flavor (liquid and powder), g | — | 5 |
| Vitamin A, IU | 764.9 | 807.3 | Red food color, g | — | 2.9 |
| Iron, mg | 0.22 | 0.04 | Blue food color, g | — | 1.1 |
| Calcium, mg | 275.3 | 287.5 | Water, g | 23.7 | 9 |
| Antioxidants (ORAC), μmol TE # | 6615 | — | |||
| Total phenolics, mg | 773.6 | — | |||
| Anthocyanins, mg | 290.3 | — | |||
| Total smoothie weight, g | 282.2 | 282.2 |
2.3. Endothelial Function and Blood Pressure
2.4. Body Weight, Body Composition and Insulin Sensitivity
2.5. Biochemical Analyses
2.6. Statistical Analyses
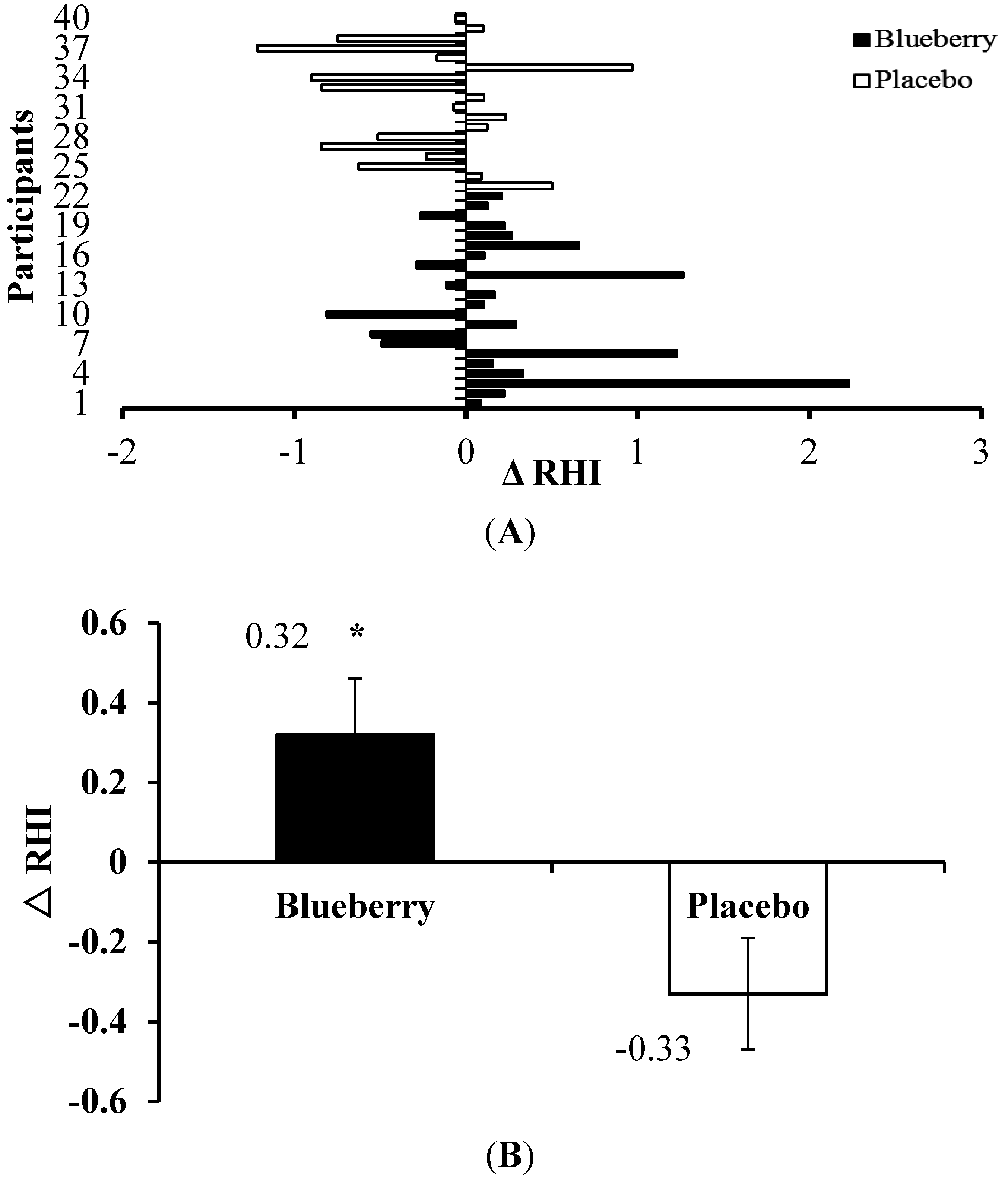
3. Results

| Variables | Blueberry | Placebo |
|---|---|---|
| n = 23 | n = 21 | |
| Race (African American/Caucasian), n/n | 13/10 | 8/13 |
| Gender (male/female), n/n | 11/12 | 5/16 |
| Age, years | 55 ± 2 | 59 ± 2 |
| Body weight, kg | 100.8 ± 3.9 | 98.9 ± 3.0 |
| BMI, kg/m2 | 35.2 ± 0.8 | 36.0 ± 1.1 |
| Body fat, % | 37.8 ± 1.4 * | 42.8 ± 1.6 |
| Fat mass, kg | 38.5 ± 2.0 | 42.7 ± 2.3 |
| Lean mass, kg | 63.4 ± 2.9 | 56.8 ± 2.3 |
| Clinic systolic blood pressure, mmHg | 125.7 ± 2.2 | 125.0 ± 3.2 |
| Clinic diastolic blood pressure, mmHg | 82.7 ± 1.9 | 77.5 ± 1.9 |
| Serum biochemistry | ||
| Glucose, mmol/L | 5.6 ± 0.1 | 5.6 ± 0.1 |
| Insulin, pmol/L | 129.3 ± 16.7 | 108.6 ± 9.1 |
| Triglycerides, mmol/L | 1.8 ± 0.2 | 1.4 ± 0.1 |
| Cholesterol, mmol/L | 5.4 ± 0.2 | 5.1 ± 0.2 |
| LDL, mmol/L | 3.2 ± 0.2 | 3.0 ± 0.2 |
| HDL, mmol/L | 1.3 ± 0.1 | 1.5 ± 0.1 |
| 24-h systolic blood pressure, mmHg # | 123.4 ± 1.9 | 124.7 ± 3.5 |
| 24-h diastolic blood pressure, mmHg # | 78.6 ± 1.2 | 76.1 ± 1.8 |
| RHI # | 1.94 ± 0.11 * | 2.34 ± 0.16 |
| Antihypertensive medication users, % | 91% | 95% |
| Variables | Blueberry (n = 23) | Placebo (n = 21) |
|---|---|---|
| Δ | Δ | |
| Body weight, kg | 0.9 ± 0.3 | 0.6 ± 0.3 |
| BMI, kg/m² | 0.3 ± 0.1 | 0.2 ± 0.1 |
| Body fat, % | −0.1 ± 0.2 | 0.2 ± 0.2 |
| Fat mass, kg | 0.1 ± 0.2 | 0.4 ± 0.2 |
| Lean mass, kg | 0.5 ± 0.3 | 0.2 ± 0.3 |
| Clinic systolic blood pressure, mmHg | −5.1 ± 3.0 | −6.5 ± 2.4 |
| Clinic diastolic blood pressure, mmHg | −5.5 ± 2.0 | −7.3 ± 1.7 |
| Serum biochemistry | ||
| Glucose, mmol/L | 0.1 ± 0.1 | 0.2 ± 0.1 |
| Insulin, pmol/L | −6.6 ± 13.9 | −2.9 ± 8.0 |
| Triglycerides, mmol/L | −0.2 ± 0.1 | −0.1 ± 0.1 |
| Cholesterol, mmol/L | −0.9 ± 0.1 | −0.6 ± 0.1 |
| LDL, mmol/L | −0.6 ± 0.1 | −0.3 ± 0.1 |
| HDL, mmol/L | −0.2 ± 0.03 | −0.2 ± 0.1 |
| 24-h systolic blood pressure, mmHg# | −1.1 ± 0.9 | −0.9 ± 1.8 |
| 24-h diastolic blood pressure, mmHg# | −0.5 ± 0.5 | −0.8 ± 0.7 |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the american heart association. Circulation 2014, 129, e28–e292. [Google Scholar]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a who consultation. Diabet. Med. 1998, 15, 539–553. [Google Scholar]
- Yeboah, J.; Crouse, J.R.; Hsu, F.C.; Burke, G.L.; Herrington, D.M. Brachial flow-mediated dilation predicts incident cardiovascular events in older adults: The cardiovascular health study. Circulation 2007, 115, 2390–2397. [Google Scholar] [CrossRef] [PubMed]
- Vita, J.A.; Treasure, C.B.; Nabel, E.G.; McLenachan, J.M.; Fish, R.D.; Yeung, A.C.; Vekshtein, V.I.; Selwyn, A.P.; Ganz, P. Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circulation 1990, 81, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Celermajer, D.S.; Sorensen, K.E.; Bull, C.; Robinson, J.; Deanfield, J.E. Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J. Am. Coll. Cardiol. 1994, 24, 1468–1474. [Google Scholar] [CrossRef]
- Rimm, E.B.; Ascherio, A.; Giovannucci, E.; Spiegelman, D.; Stampfer, M.J.; Willett, W.C. Vegetable, fruit, and cereal fiber intake and risk of coronary heart disease among men. JAMA 1996, 275, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Joshipura, K.J.; Ascherio, A.; Manson, J.E.; Stampfer, M.J.; Rimm, E.B.; Speizer, F.E.; Hennekens, C.H.; Spiegelman, D.; Willett, W.C. Fruit and vegetable intake in relation to risk of ischemic stroke. JAMA 1999, 282, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, A.; Mukamal, K.J.; Liu, L.; Franz, M.; Eliassen, A.H.; Rimm, E.B. High anthocyanin intake is associated with a reduced risk of myocardial infarction in young and middle-aged women. Circulation 2013, 127, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Stull, A.J.; Cash, K.C.; Johnson, W.D.; Champagne, C.M.; Cefalu, W.T. Bioactives in blueberries improve insulin sensitivity in obese, insulin-resistant men and women. J. Nutr. 2010, 140, 1764–1768. [Google Scholar] [CrossRef] [PubMed]
- DeFuria, J.; Bennett, G.; Strissel, K.J.; Perfield, J.W., 2nd; Milbury, P.E.; Greenberg, A.S.; Obin, M.S. Dietary blueberry attenuates whole-body insulin resistance in high fat-fed mice by reducing adipocyte death and its inflammatory sequelae. J. Nutr. 2009, 139, 1510–1516. [Google Scholar]
- Vendrame, S.; Kristo, A.S.; Schuschke, D.A.; Klimis-Zacas, D. Wild blueberry consumption affects aortic vascular function in the obese Zucker rat. Appl. Physiol. Nutr. Metab. 2014, 39, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Norton, C.; Kalea, A.Z.; Harris, P.D.; Klimis-Zacas, D.J. Wild blueberry-rich diets affect the contractile machinery of the vascular smooth muscle in the Sprague-Dawley rat. J. Med. Food 2005, 8, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Kristo, A.S.; Kalea, A.Z.; Schuschke, D.A.; Klimis-Zacas, D.J. A wild blueberry-enriched diet (Vaccinium angustifolium) improves vascular tone in the adult spontaneously hypertensive rat. J. Agric. Food Chem. 2010, 58, 11600–11605. [Google Scholar] [CrossRef] [PubMed]
- Kalea, A.Z.; Clark, K.; Schuschke, D.A.; Kristo, A.S.; Klimis-Zacas, D.J. Dietary enrichment with wild blueberries (Vaccinium angustifolium) affects the vascular reactivity in the aorta of young spontaneously hypertensive rats. J. Nutr. Biochem. 2010, 21, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Kalea, A.Z.; Clark, K.; Schuschke, D.A.; Klimis-Zacas, D.J. Vascular reactivity is affected by dietary consumption of wild blueberries in the Sprague-Dawley rat. J. Med. Food 2009, 12, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, K.S.; Boswall, I.A.; Scanlan, A.P.; Gottschall-Pass, K.T.; Sweeney, M.I. Diets containing blueberry extract lower blood pressure in spontaneously hypertensive stroke-prone rats. Nutr. Res. 2009, 29, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Elks, C.M.; Reed, S.D.; Mariappan, N.; Shukitt-Hale, B.; Joseph, J.A.; Ingram, D.K.; Francis, J. A blueberry-enriched diet attenuates nephropathy in a rat model of hypertension via reduction in oxidative stress. PLoS ONE 2011, 6, e24028. [Google Scholar] [CrossRef] [PubMed]
- Mykkanen, O.T.; Huotari, A.; Herzig, K.H.; Dunlop, T.W.; Mykkanen, H.; Kirjavainen, P.V. Wild blueberries (Vaccinium myrtillus) alleviate inflammation and hypertension associated with developing obesity in mice fed with a high-fat diet. PLoS ONE 2014, 9, e114790. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xia, M.; Yang, Y.; Liu, F.; Li, Z.; Hao, Y.; Mi, M.; Jin, T.; Ling, W. Purified anthocyanin supplementation improves endothelial function via NO-cGMP activation in hypercholesterolemic individuals. Clin. Chem. 2011, 57, 1524–1533. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mateos, A.; Rendeiro, C.; Bergillos-Meca, T.; Tabatabaee, S.; George, T.W.; Heiss, C.; Spencer, J.P. Intake and time dependence of blueberry flavonoid-induced improvements in vascular function: A randomized, controlled, double-blind, crossover intervention study with mechanistic insights into biological activity. Am. J. Clin. Nutr. 2013, 98, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- Riso, P.; Klimis-Zacas, D.; Del Bo, C.; Martini, D.; Campolo, J.; Vendrame, S.; Moller, P.; Loft, S.; De Maria, R.; Porrini, M. Effect of a wild blueberry (Vaccinium angustifolium) drink intervention on markers of oxidative stress, inflammation and endothelial function in humans with cardiovascular risk factors. Eur. J. Nutr. 2013, 52, 949–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAnulty, S.R.; McAnulty, L.S.; Morrow, J.D.; Khardouni, D.; Shooter, L.; Monk, J.; Gross, S.; Brown, V. Effect of daily fruit ingestion on angiotensin converting enzyme activity, blood pressure, and oxidative stress in chronic smokers. Free Radic. Res. 2005, 39, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.A.; Figueroa, A.; Navaei, N.; Wong, A.; Kalfon, R.; Ormsbee, L.T.; Feresin, R.G.; Elam, M.L.; Hooshmand, S.; Payton, M.E.; et al. Daily blueberry consumption improves blood pressure and arterial stiffness in postmenopausal women with pre- and stage 1-hypertension: A randomized, double-blind, placebo-controlled clinical trial. J. Acad. Nutr. Diet 2015, 115, 369–377. [Google Scholar] [CrossRef]
- Del Bo, C.; Riso, P.; Campolo, J.; Moller, P.; Loft, S.; Klimis-Zacas, D.; Brambilla, A.; Rizzolo, A.; Porrini, M. A single portion of blueberry (Vaccinium corymbosum L) improves protection against DNA damage but not vascular function in healthy male volunteers. Nutr. Res. 2013, 33, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Du, M.; Leyva, M.J.; Sanchez, K.; Betts, N.M.; Wu, M.; Aston, C.E.; Lyons, T.J. Blueberries decrease cardiovascular risk factors in obese men and women with metabolic syndrome. J. Nutr. 2010, 140, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Greenway, F.L.; Cornelissen, G.; Pan, W.; Halberg, F. Prediabetes is associated with abnormal circadian blood pressure variability. J. Hum. Hypertens 2008, 22, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Slinkard, K.; Singleton, V.L. Total phenol analysis—Automation and comparison with manual methods. Am. J. Enol. Viticult. 1977, 28, 49–55. [Google Scholar]
- Cheng, G.W.; Breen, P.J. Activity of phenylalanine ammonia-lyase (PAL) and concentrations of anthocyanins and phenolics in developing strawberry fruit. J. Am. Soc. Hortic. Sci. 1991, 116, 865–869. [Google Scholar]
- Ou, B.X.; Hampsch-Woodill, M.; Prior, R.L. Development and validation of an improved oxygen radical absorbance capacity assay using fluorescein as the fluorescent probe. J. Agric. Food Chem. 2001, 49, 4619–4626. [Google Scholar] [CrossRef] [PubMed]
- Rubinshtein, R.; Kuvin, J.T.; Soffler, M.; Lennon, R.J.; Lavi, S.; Nelson, R.E.; Pumper, G.M.; Lerman, L.O.; Lerman, A. Assessment of endothelial function by non-invasive peripheral arterial tonometry predicts late cardiovascular adverse events. Eur. Heart J. 2010, 31, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Cefalu, W.T.; Werbel, S.; Bell-Farrow, A.D.; Terry, J.G.; Wang, Z.Q.; Opara, E.C.; Morgan, T.; Hinson, W.H.; Crouse, J.R., 3rd. Insulin resistance and fat patterning with aging: Relationship to metabolic risk factors for cardiovascular disease. Metab. Clin. Exp. 1998, 47, 401–408. [Google Scholar] [CrossRef]
- Boston, R.C.; Stefanovski, D.; Moate, P.J.; Sumner, A.E.; Watanabe, R.M.; Bergman, R.N. Minmod millennium: A computer program to calculate glucose effectiveness and insulin sensitivity from the frequently sampled intravenous glucose tolerance test. Diabetes Technol. Ther. 2003, 5, 1003–1015. [Google Scholar] [CrossRef] [PubMed]
- Streppel, M.T.; Arends, L.R.; van’t Veer, P.; Grobbee, D.E.; Geleijnse, J.M. Dietary fiber and blood pressure—A meta-analysis of randomized placebo-controlled trials. Arch. Intern. Med. 2005, 165, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Reverri, E.J.; LaSalle, C.D.; Franke, A.A.; Steinberg, F.M. Soy provides modest benefits on endothelial function without affecting inflammatory biomarkers in adults at cardiometabolic risk. Mol. Nutr. Food Res. 2015, 59, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Nagaya, N.; Yamamoto, H.; Uematsu, M.; Itoh, T.; Nakagawa, K.; Miyazawa, T.; Kangawa, K.; Miyatake, K. Green tea reverses endothelial dysfunction in healthy smokers. Heart 2004, 90, 1485–1486. [Google Scholar] [CrossRef] [PubMed]
- Hermann, F.; Spieker, L.E.; Ruschitzka, F.; Sudano, I.; Hermann, M.; Binggeli, C.; Luscher, T.F.; Riesen, W.; Noll, G.; Corti, R. Dark chocolate improves endothelial and platelet function. Heart 2006, 92, 119–120. [Google Scholar] [CrossRef] [PubMed]
- Heiss, C.; Kleinbongard, P.; Dejam, A.; Perre, S.; Schroeter, H.; Sies, H.; Kelm, M. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J. Am. Coll. Cardiol. 2005, 46, 1276–1283. [Google Scholar] [CrossRef] [PubMed]
- Fisher, N.D.; Hughes, M.; Gerhard-Herman, M.; Hollenberg, N.K. Flavanol-rich cocoa induces nitric-oxide-dependent vasodilation in healthy humans. J. Hypertens. 2003, 21, 2281–2286. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.J.; Keaney, J.F., Jr.; Holbrook, M.; Gokce, N.; Swerdloff, P.L.; Frei, B.; Vita, J.A. Short- and long-term black tea consumption reverses endothelial dysfunction in patients with coronary artery disease. Circulation 2001, 104, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Hausberg, M.; Lang, D.; Barenbrock, M.; Kosch, M. Large artery wall properties—What is relevant for the management of hypertension? Deut. Med. Wochenschr. 2005, 130, 2657–2661. [Google Scholar] [CrossRef] [PubMed]
- Rice, B.H. Dairy and cardiovascular disease: A review of recent observational research. Curr. Nutr. Rep. 2014, 3, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Astrup, A. Yogurt and dairy product consumption to prevent cardiometabolic diseases: Epidemiologic and experimental studies. Am. J. Clin. Nutr. 2014, 99, 1235S–1242S. [Google Scholar] [CrossRef] [PubMed]
- Serafini, M.; Ghiselli, A.; FerroLuzzi, A. In vivo antioxidant effect of green and black tea in man. Eur. J. Clin. Nutr. 1996, 50, 28–32. [Google Scholar] [PubMed]
- Reddy, V.C.; Sagar, G.V.V.; Sreeramulu, D.; Venu, L.; Raghunath, M. Addition of milk does not alter the antioxidant activity of black tea. Ann. Nutr. Metab. 2005, 49, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Leenen, R.; Roodenburg, A.J.C.; Tijburg, L.B.M.; Wiseman, S.A. A single dose of tea with or without milk increases plasma antioxidant activity in humans. Eur. J. Clin. Nutr. 2000, 54, 87–92. [Google Scholar] [CrossRef] [PubMed]
- van het Hof, K.H.; Kivits, G.A.A.; Weststrate, J.A.; Tijburg, L.B.M. Bioavailability of catechins from tea: The effect of milk. Eur. J. Clin. Nutr. 1998, 52, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Cebeci, F.; Sahin-Yesilcubuk, N. The matrix effect of blueberry, oat meal and milk on polyphenols, antioxidant activity and potential bioavailability. Int. J. Food Sci. Nutr. 2014, 65, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Lerman, A.; Burnett, J.C., Jr. Intact and altered endothelium in regulation of vasomotion. Circulation 1992, 86, 12–19. [Google Scholar] [PubMed]
- Forstermann, U.; Munzel, T. Endothelial nitric oxide synthase in vascular disease: From marvel to menace. Circulation 2006, 113, 1708–1714. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stull, A.J.; Cash, K.C.; Champagne, C.M.; Gupta, A.K.; Boston, R.; Beyl, R.A.; Johnson, W.D.; Cefalu, W.T. Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients 2015, 7, 4107-4123. https://doi.org/10.3390/nu7064107
Stull AJ, Cash KC, Champagne CM, Gupta AK, Boston R, Beyl RA, Johnson WD, Cefalu WT. Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nutrients. 2015; 7(6):4107-4123. https://doi.org/10.3390/nu7064107
Chicago/Turabian StyleStull, April J., Katherine C. Cash, Catherine M. Champagne, Alok K. Gupta, Raymond Boston, Robbie A. Beyl, William D. Johnson, and William T. Cefalu. 2015. "Blueberries Improve Endothelial Function, but Not Blood Pressure, in Adults with Metabolic Syndrome: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial" Nutrients 7, no. 6: 4107-4123. https://doi.org/10.3390/nu7064107