Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study


 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
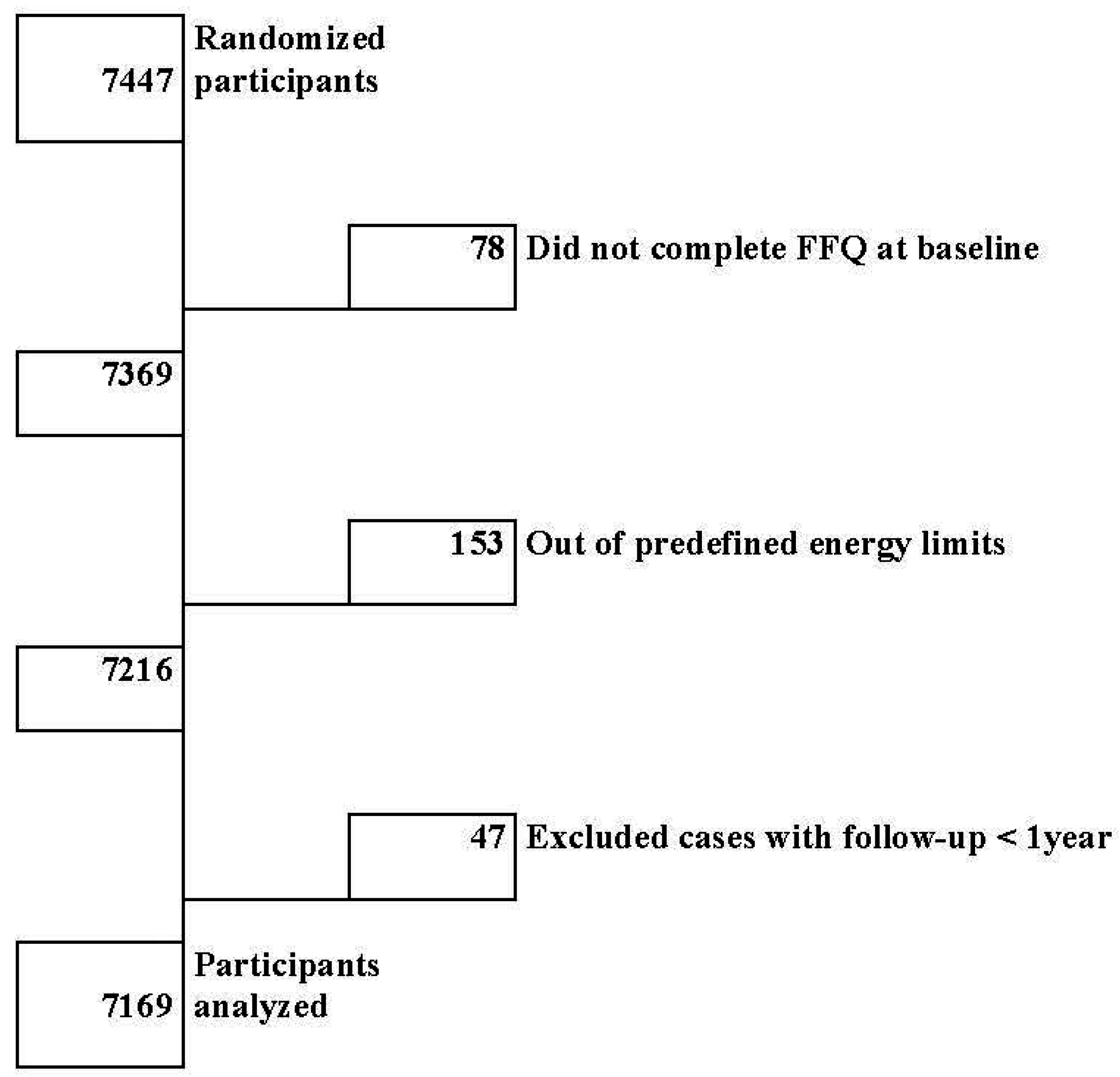
2.1. Participants
2.2. Data Collection and Outcomes
2.3. Statistical Analysis

3. Results

{kind=link}
{kind=link}
{kind=link}
| Variables | Quartiles of Dietary Inflammatory Index (DII) (a Higher Value Implies Higher Inflammatory Potential) | |||
|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |
| DII, median | −2.46 | −1.34 | −0.32 | 1.17 |
| Number | 1804 | 1804 | 1804 | 1804 |
| Age, year | 66 (6) | 67 (6) | 67 (6) | 68 (6) |
| Sex (% Women), | 55 | 57 | 58 | 60 |
| Family history of early CHD, % | 23 | 24 | 22 | 20 |
| Hypertension, % | 81 | 83 | 84 | 83 |
| Dyslipidemia, % | 76 | 72 | 71 | 69 |
| Diabetes, % | 48 | 46 | 49 | 52 |
| Smoking, % | ||||
| Never | 61 | 60 | 62 | 63 |
| Former | 26 | 26 | 24 | 22 |
| Current | 13 | 14 | 14 | 15 |
| Body mass index, kg m−2 | 29.6 (3.9) | 30.0 (3.9) | 30.0 (3.8) | 30.0 (3.8) |
| Waist-to-height ratio | 0.6 (0.1) | 0.6 (0.1) | 0.6 (0.1) | 0.6 (0.1) |
| Physical activity, METS-min day−1 | 270 (279) | 237 (241) | 224 (223) | 194 (199) |
| Marital status, % | ||||
| Single | 4 | 5 | 4 | 5 |
| Married | 81 | 75 | 77 | 72 |
| Widowed | 13 | 18 | 16 | 19 |
| Other | 2 | 3 | 4 | 3 |
| Educational level, % | ||||
| Primary education or less | 74 | 78 | 79 | 80 |
| Secondary education | 17 | 15 | 15 | 14 |
| College or higher | 9 | 7 | 6 | 6 |
| Total energy intake, kcal day−1 | 2542 (535) | 2347 (512) | 2146 (460) | 1909 (450) |
| Alcohol intake, g day−1 | 10 (15) | 8 (14) | 8 (14) | 7 (13) |
| Protein intake, % energy | 16.7 (2.7) | 16.5 (2.7) | 16.7 (2.8) | 16.7 (3.0) |
| Carbohydrate intake, % energy | 42.5 (7.1) | 42.4 (6.9) | 41.8 (7.1) | 40.5 (7.3) |
| Total fat intake, % energy | 38 (7) | 39 (7) | 39 (7) | 40 (7) |
| Saturated, % energy | 9 (2) | 10 (2) | 10 (2) | 11 (2) |
| Monounsaturated, % energy | 18 (5) | 19 (4) | 20 (4) | 21 (5) |
| Polyunsaturated, % energy | 7 (2) | 6 (2) | 6 (2) | 6 (2) |
| Fiber, g day−1 | 34 (9) | 27 (6) | 23 (5) | 17 (4) |
| Adherence to the Mediterranean diet (0 to 14 points) | 10 (2) | 9 (2) | 8 (2) | 8 (2) |
4. Discussion
| Hazard Ratios (HR) | Quartiles of Adherence to the Dietary Inflammatory Index | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | P for trend | |
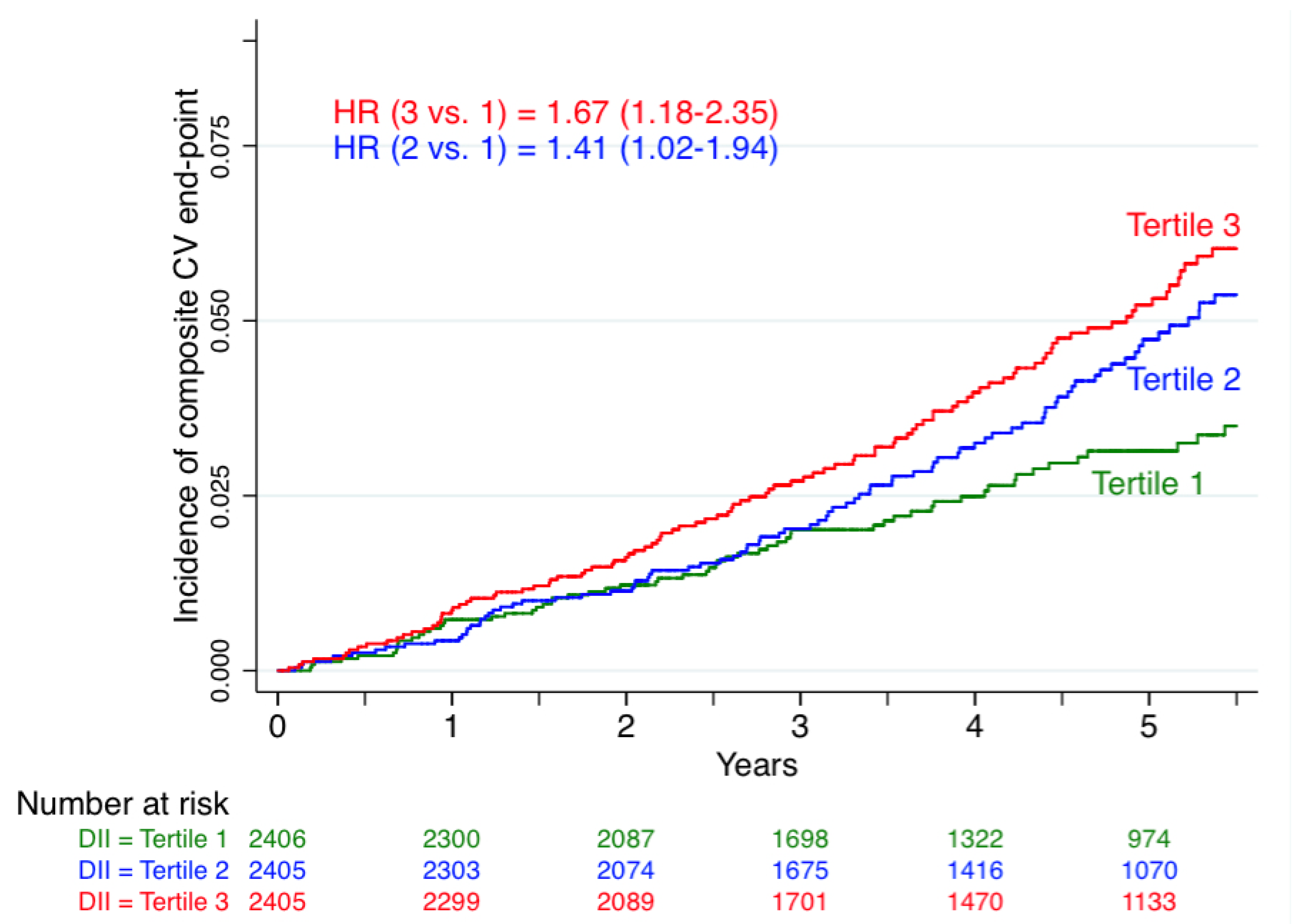
| Cases/person-years | 49/7641 | 64/7755 | 85/7684 | 79/7960 | |
| Crude HR | 1 (ref) | 1.32 (0.91–1.92) | 1.84 (1.29–2.63) | 1.68 (1.16–2.43) | 0.003 |
| Adjusted for age and sex HR | 1 (ref) | 1.41 (0.96–2.06) | 1.87 (1.29–2.69) | 1.76 (1.21–2.57) | 0.002 |
| Multivariable adjusted HR 1 | 1 (ref) | 1.42 (0.97–2.09) | 1.85 (1.27–2.71) | 1.73 (1.15–2.60) | 0.008 |
| After excluding cases with follow-up < 1 year | 36/7633 | 58/7752 | 73/7678 | 63/7951 | |
| Crude HR | 1 (ref) | 1.62 (1.071–2.48) | 2.16 (1.43–3.24) | 1.83 (1.20–2.78) | 0.005 |
| Adjusted for age and sex HR | 1 (ref) | 1.75 (1.14–2.68) | 2.21 (1.46–3.35) | 1.93 (1.26–2.97) | 0.004 |
| Multivariable adjusted HR 1 | 1 (ref.) | 1.76 (1.14–2.70) | 2.22 (1.45–3.41) | 1.90 (1.20–3.01) | 0.012 |


5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Declaration
References
- World Health Organization. World Health Statistics; World Health Organization: Geneva, Switzertland, 2012. [Google Scholar]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Páramo, J.; Rodríguez, J.; Orbe, J. Atherosclerosis in inflammatory diseases. Med. Clin. 2007, 128, 749–756. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Fung, T.T.; Meigs, J.B.; Rifai, N.; Manson, J.E.; Hu, F.B.; Schulze, M. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2004, 80, 1029–1035. [Google Scholar] [PubMed]
- Salas-Salvadó, J.; Garcia-Arellano, A.; Estruch, R.; Marquez-Sandoval, F.; Corella, D.; Fiol, M.; Gómez-Gracia, E.; Viñoles, E.; Arós, F.; Herrera, C.; et al. Components of the Mediterranean-type food pattern and serum inflammatory markers among patients at high risk for cardiovascular disease. Eur. J. Clin. Nutr. 2008, 62, 651–659. [Google Scholar]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Dietary patterns and markers of systemic inflammation among Iranian women. J. Nutr. 2007, 137, 992–998. [Google Scholar] [PubMed]
- Fung, T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willett, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Dietary patterns, Mediterranean diet, and cardiovascular disease. Curr. Opin. Lipidol. 2014, 25, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Canela, M.; Zazpe, I.; Shivappa, N.; Hébert, J.R.; Sánchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Lamuela-Raventós, R.M.; Fernández-Crehuet, J.; et al. Dietary inflammatory index and anthropometric measures of obesity in a population sample at high cardiovascular risk from the PREDIMED trial. Br. J. Nutr. 2015, 13, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fiol, M.; Wärnberg, J.; Arós, F.; Ruíz-Gutiérrez, V.; Lamuela-Raventós, R.M.; et al. Cohort profile: Design and methods of the PREDIMED study. Int. J. Epidemiol. 2012, 41, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Ros, E.; Martínez-Gonz;lez, M.A.; Estruch, R.; Salas-Salvadó, J.; Fitó, M.; Martínez, J.A.; Corella, D. Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study. Adv. Nutr. 2014, 5, 330S–336S. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schröder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The Predimed study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Caan, B.; Hou, L.; Johnson, K.C.; Mossavar-Rahmani, Y.; Shivappa, N.; et al. The association between dietary inflammatory index and risk of colorectal cancer among postmenopausal women: Results from the Women’s Health Initiative. Cancer Causes Control 2015, 26, 399–408. [Google Scholar]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; de Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.G.; Shivappa, N.; Berthon, B.S.; Gibson, P.G.; Hebert, J.R. Dietary inflammatory index is related to asthma risk, lung function and systemic inflammation in asthma. Clin. Exp. Allergy 2015, 45, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Khymenets, O.; Urpí-Sardà, M.; Tulipani, S.; Garcia-Aloy, M.; Monagas, M.; Mora-Cubillos, X.; Llorach, R.; Andres-Lacueva, C. Cocoa polyphenols and inflammatory markers of cardiovascular disease. Nutrients 2014, 6, 844–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Chun, O.K.; Song, W.O. Plasma and dietary antioxidant status as cardiovascular disease risk factors: A review of human studies. Nutrients 2013, 5, 2969–3004. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Kosanovic, M.; Yasin, J.; El Essa, A. Oxidative damage and inflammation in obese diabetic Emirati subjects. Nutrients 2014, 6, 4872–4880. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorff, H.H.; Zulet, M.Á.; Abete, I.; Martínez, J.A. A legume-based hypocaloric diet reduces proinflammatory status and improves metabolic features in overweight/obese subjects. Eur. J. Nutr. 2011, 50, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Van Woudenbergh, G.; Theofylaktopoulou, D.; Kuijsten, A.; Ferreira, I.; van Greevenbroek, M.M.; van der Kallen, C.J.; Schalkwijk, C.G.; Stehouwer, C.D.; Ocké, M.C.; Nijpels, G.; et al. Adapted dietary inflammatory index and its association with a summary score for low-grade inflammation and markers of glucose metabolism: The Cohort study on Diabetes and Atherosclerosis Maastricht (CODAM) and the Hoorn study. Am. J. Clin. Nutr. 2013, 98, 1533–1542. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Shivappa, N.; Crichton, G.; Hébert, J.R. No significant independent relationships with cardiometabolic biomarkers were detected in the Observation of Cardiovascular Risk Factors in Luxembourg study population. Nutr. Res. 2014, 34, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Urpí-Sardà, M.; Chiva-Blanch, G.; Ros, E.; Martínez-González, M.A.; Covas, M.I.; Lamuela-Raventos, R.M.; Salas-Salvadó, J.; Fiol, M; et al. The effects of the mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS ONE 2014, 9, e100084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulló, M.; Casas, R.; Portillo, M.P.; Basora, J.; Estruch, R.; García-Arellano, A.; Lasa, A.; Juanola-Falgarona, M.; Arós, F.; Salas-Salvadó, J. Dietary glycemic index/load and peripheral adipokines and inflammatory markers in elderly subjects at high cardiovascular risk. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 443–450. [Google Scholar] [CrossRef]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mena, M.; Sacanella, E.; Vazquez-Agell, M.; Morales, M.; Fitó, M.; Escoda, R.; Serrano-Martínez, M.; Salas-Salvadó, J.; Benages, N.; Casas, R.; et al. Inhibition of circulating immune cell activation: A molecular antiinflammatory effect of the Mediterranean diet. Am. J. Clin. Nutr. 2009, 89, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.; Burch, J.; Shivappa, N.; Violanti, J.M.; Burchfiel, C.M.; Fekedulegn, D.; Andrew, M.E.; Hartley, T.A.; Miller, D.B.; Mnatsakanova, A.; et al. Association of a dietary inflammatory index with inflammatory indices and metabolic syndrome among police officers. J. Occup. Environ. Med. 2014, 56, 986–989. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Mediterranean dietary pattern, inflammation and endothelial function: A systematic review and meta-analysis of intervention trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Arellano, A.; Ramallal, R.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Shivappa, N.; Schröder, H.; Hébert, J.R.; Ros, E.; Gómez-Garcia, E.; et al. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study. Nutrients 2015, 7, 4124-4138. https://doi.org/10.3390/nu7064124
Garcia-Arellano A, Ramallal R, Ruiz-Canela M, Salas-Salvadó J, Corella D, Shivappa N, Schröder H, Hébert JR, Ros E, Gómez-Garcia E, et al. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study. Nutrients. 2015; 7(6):4124-4138. https://doi.org/10.3390/nu7064124
Chicago/Turabian StyleGarcia-Arellano, Ana, Raul Ramallal, Miguel Ruiz-Canela, Jordi Salas-Salvadó, Dolores Corella, Nitin Shivappa, Helmut Schröder, James R. Hébert, Emilio Ros, Enrique Gómez-Garcia, and et al. 2015. "Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the PREDIMED Study" Nutrients 7, no. 6: 4124-4138. https://doi.org/10.3390/nu7064124